")
Back to Journals » Psychology Research and Behavior Management » Volume 11
Validation of the Indonesian version of Champion’s Health Belief Model Scale for breast self-examination
Authors Dewi TK
Received 13 June 2018
Accepted for publication 13 August 2018
Published 4 October 2018 Volume 2018:11 Pages 433—438
DOI https://doi.org/10.2147/PRBM.S177124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Igor Elman
Triana Kesuma Dewi
Department of Clinical Psychology and Mental Health, Faculty of Psychology, Airlangga University, Surabaya, East Java, Indonesia
Purpose: The present study aimed to adapt and determine the psychometric properties of the Indonesian version of the Champion’s Health Belief Model Scale (I-CHBMS) of breast self-examination in the measurement of belief toward breast cancer screening.
Subjects and methods: A convenience sample of 406 Indonesian women aged 19–60 years was recruited. This study was conducted in Surabaya from December 2016 to January 2017. The I-CHBMS applied a “forward–backward” translation procedure to translate from the English version into Indonesian. Validity of the I-CHBMS was assessed using content, face, and construct validity. Confirmatory factor analysis was used to assess the construct validity. Reliability was measured using Cronbach’s alpha coefficient.
Results: The result of confirmatory factor analysis indicated 42 items of I-CHBMS with six-factor solution (susceptibility, severity, benefits, barriers, cues to action and self efficacy) were acceptable as a new instrument. Cronbach’s alpha of the subscale ranged from 0.669 to 0.866, indicating a good range of reliability.
Conclusion: The finding of the study suggested that I-CHBMS of breast self-examination practice has good psychometric properties and could be an appropriate measure for health beliefs related to breast cancer screening.
Keywords: breast cancer, CHBMS, Indonesian version of CHBMS, psychometric properties
Introduction
Breast cancer is the most prevalent cancer in women, both in developed and developing countries. In Indonesia, of all types of cancer, breast cancer is the most prevalent cancer and is the first leading cause of death among women, with an incidence rate of 30.5% and a mortality rate of 21.5%.1–3 The national hospital information system recorded that there were 12,014 (28.7%) cases of breast cancer inpatients in Indonesia.4 Breast cancer in an earlier stage has a better prognosis if treated accurately and adequately and has been shown to decrease the mortality level.5,6 Unfortunately, in Indonesia, almost 70% of breast cancer patients come to the hospital in the late stage of the disease.7 Early detection is thus needed to control the development of breast cancer. It will not decrease the incidence of breast cancer cases, but it will certainly improve the prognosis and treatment outcomes.8
Breast self-examination (BSE) is one of the strategies which can be employed to achieve earlier detection of breast cancer. It is a unique procedure in many ways: it is an inexpensive, noninvasive and non-hazardous technique, is simple, involves little time and physical energy, and does not depend on professional help. In addition, it encourages women to be actively responsible for their own health.2 In countries where (health-related) resources are limited, as it is the case in developing countries such as Indonesia, and where due to sociocultural influences women are hesitant and unfamiliar about sharing health issues about their breasts, empowering women to examine their breasts is an important first step.9
Despite the importance of breast cancer screening, its awareness among women in Indonesia is low,6 due to which there is a low rate of breast cancer screening. Taylor10 noted that the lack of participation in screening behavior could be explained based on Health Belief Model (HBM). HBM was first developed by Rosenstock,11 and it focuses on threat perception and behavioral evaluation as the key aspects representing health behavior.12 Threat perception consists of two beliefs: 1) perceived susceptibility: indicating the level of vulnerability of an individual to an illness or health problem; and 2) perceived severity: representing the degree to which an individual anticipates the seriousness of the consequences of an illness. Behavioral evaluation is constructed of two distinct beliefs: 1) perceived benefits: concerning the positive outcome of a health behavior; and 2) perceived barriers: representing the cost or obstacle to enact the behavior. In addition, the model proposed the fifth component: cues to action, which activate health behavior when appropriate beliefs are apprehended. Cues to action may include individual perceptions of symptoms, social influence or health education. Finally, self-efficacy is added to the model, which indicates the belief of individuals in their capacity to execute a health behavior.
The Champion’s Health Belief Model Scale (CHBMS) was developed and revised by Champion in 1984–1999 to identify beliefs underlying breast cancer screening behaviors based on HBM perspective.13,14 The scale is widely used in different populations, mostly for breast cancer in Western cultures.14 Nevertheless, a valid and reliable instrument to determine beliefs of Indonesian women underlying BSE has not been reported. Therefore, the aim of this study was to adapt and assess the validity and reliability of the Indonesian version of CHBMS (I-CHBMS) in the measurement of beliefs underlying BSE practice.
Subjects and methods
Sample and data collection
This cross-sectional study was conducted in Surabaya, East Java, Indonesia. A convenience sample of 425 individuals aged 19–60 years in nine districts in Surabaya was recruited. The research assistants randomly approached registered families with women aged 19–60 years as a family member in the districts during 2016. Sample size was determined based on Osborne and Costello’s15 participant-to-variable ratio approach, suggesting that a sample size of five to ten subjects per item was important to ensure a conceptually clear factor structure for factor analysis. Based on the 42-item scale of HBM, a minimum of 210–420 participants were required for this study. Thus, 425 participants recruited in this study were considered to be an adequate sample. The inclusion criteria were being female, aged between 19 and 60 years, able to communicate in Indonesian language and consenting to take part in the study.
The data were collected during December 2016 to January 2017. The potential participants were approached and screened for eligibility for the study. Participants who met the inclusion criteria and agreed to participate were invited to complete the 42-item questionnaire, which took about 10–15 minutes to complete. Prior to data collection, participants were explained the study purpose and gave written consent to participate in the study. The study was approved by the Research Ethics Committee, Faculty of Psychology, Universitas Airlangga.
Instruments
To collect the data, we used two sets of questionnaires: 1) a questionnaire to collect sociodemographic information of the participants such as age, education, employment, marital status, family history of cancer, participant’s history of (breast) cancer and the frequency of BSE; and 2) health belief was assessed using the I-CHBMS. It contains 42 items within six subscales: perceived susceptibility (6 items), perceived severity (12 items), perceived benefits (5 items), perceived barriers (8 items), cues to action (8 items) and self-efficacy (3 items). Each item was measured on a 5-point Likert scale.
Instrument development
The items of the new instrument were selected largely from a previously developed scale from the work of Champion.13 Champion developed 39 items of CHBMS, consisting of five dimensions: perceived susceptibility (α=0.78), perceived seriousness (α=0.78), perceived benefits (α=0.61), perceived barriers (α=0.76) and motivation (α=0.602), measuring health beliefs of breast cancer and screening behavior. Once Victoria Champion granted the permission to modify and use CHBMS, translation of the scales was started. The questionnaire was translated using forward and backward translation. The questionnaire was first translated from English to Indonesian by two professional translators and the I-CHBMS was developed based on the comparison of the two translations. Next, the I-CHBMS was back translated to English by two other professional translators. Back translations and each item of the original CHBMS were compared and a final Indonesian version of the questionnaire was obtained. To be updated with the recent revision of HBM, which includes cues to action and self-efficacy, we added items representing those two dimensions in the I-CHBMS and removed the motivation dimension in the scale.
To test the content validity of the I-CHBMS, a panel consisting of two health psychologists and two lecturers of Health Behavior subject was created. The panel assessed and commented the suitability, reasonability and logical sequence of each item. Furthermore, the panel also discussed the conciseness and comprehensiveness of the items.
Data analysis
All data analyses were performed by using the SPSS (version 22) and LISREL. Demographic characteristics of the participants were analyzed by using descriptive statistics. Confirmatory factor analysis (CFA) was used to examine the construct validity of I-CHBMS. The reliability of the scale was measured using internal consistency methods.
Results
Sample characteristics
Four hundred and twenty-five participants joined the study; 19 of them were excluded from the analysis due to incomplete response(s), and thus, there were 406 data included in the analysis. Mean and SD of the participants’ age was 32.74±11.65 years. Majority of the sample graduated from Senior High School (56.2%), were married (58.6%) and had been never diagnosed with either breast cancer (97%) or any other type of cancer (96.3%). Details of demographic characteristics are presented in Table 1.
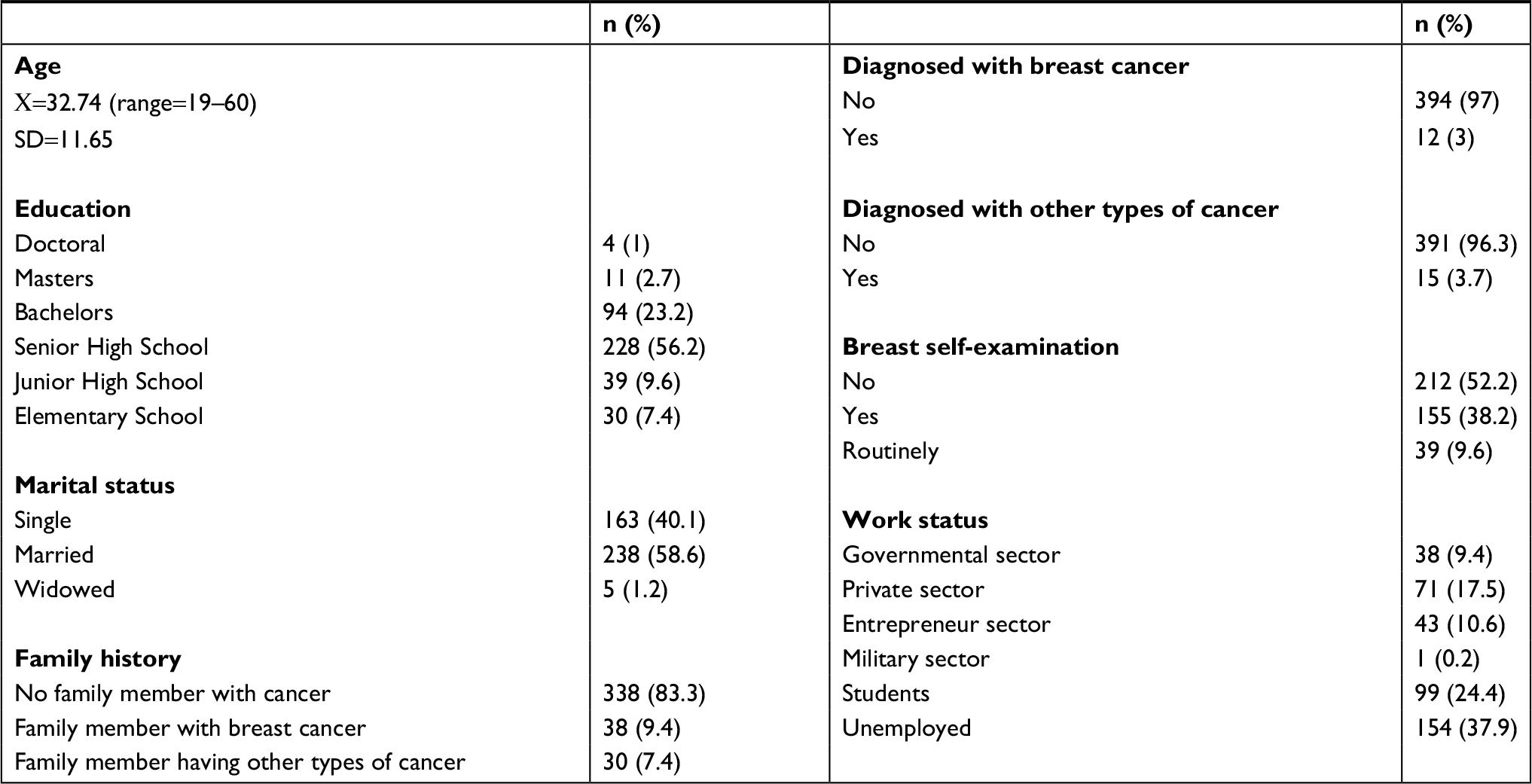 | Table 1 Demographic characteristics |
Validity
CFA was run to examine the construct validity of the six factor models of HBM. Initially, 42 predictors (items) were used to test the model using LISREL program. Data from individual items for perceived susceptibility, perceived severity, perceived barriers, perceived benefits, cues to action and self-efficacy in BSE were submitted to the PRELIS program to develop a continuous covariance matrix. This matrix was then used in the CFA. The fit indices for the 42-item model were χ2=2,071.2, degrees of freedom=804, P=0.000, GFI=0.80, CFI=0.92, AGFI=0.78, RMSEα=0.06 and SRMR=0.064. The model fit is acceptable, indicated by the CFI value of 0.092 or greater and the RMSEA value of 0.06 or less.16
Reliability
Cronbach’s alpha coefficients were estimated separately for all six factors, ranging between 0.669 and 0.866. Cronbach’s alpha is an index indicating the degree to which a scale is internally reliable and is the most commonly used.17 A reliability coefficient of 0.70 or above is considered as suitable for ability tests, a minimum value of 0.80 is appropriate for cognitive tests, while for scales of psychological constructs, value below 0.70 is realistically expected.18 Thus, I-CHBMS is considered as having an acceptable value of alpha coefficient. In this study, item 8 had the lowest total item correlation value of 0.368. Other items had a value ranging from 0.413 to 0.780.
Six items of perceived susceptibility had Cronbach’s alpha 0.844 with the item-total correlation ranging from 0.422 to 0.780. The 12 items of perceived severity had Cronbach’s alpha 0.815 and corrected item-total correlation 0.368–0.656. Perceived benefits consisted of five items, which had Cronbach’s alpha 0.815 and corrected item-total correlation ranging from 0.531 to 0.701. Perceived barriers included eight items, which had Cronbach’s alpha 0.825 and corrected item-total correlation 0.480–0.661. The eight items related to cues to action had Cronbach’s alpha 0.809 and corrected item-total correlation ranging from 0.430–0.592. The last component, self-efficacy, consisted of three items with Cronbach’s alpha 0.669 and corrected item-total correlation ranging from 0.424 to 5.14. Table 2 provides a summary of Cronbach’s alpha coefficient and description of each item.
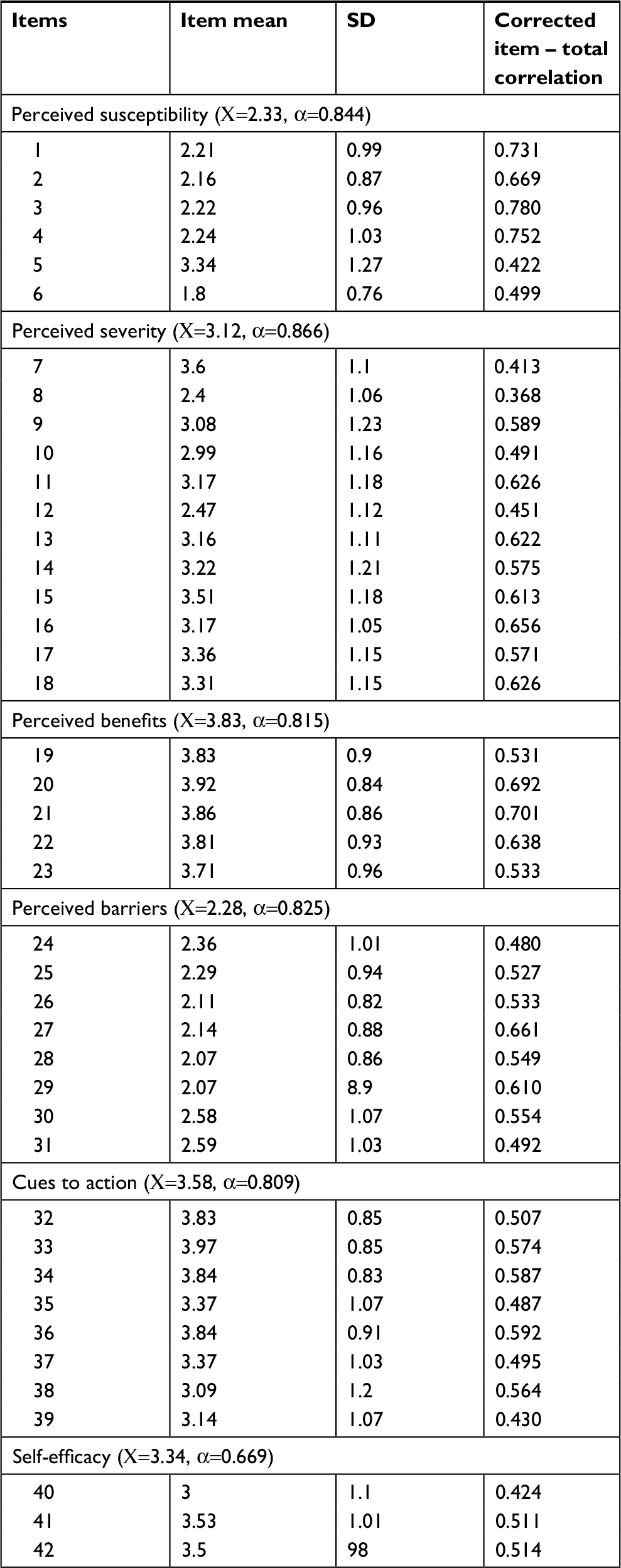 | Table 2 Summary of Cronbach’s alpha and item-total correlation value |
Discussion
Breast cancer is the most prevalent type of cancer in Indonesian women. Early detection of breast cancer, which results in early treatment, has been shown to decrease the mortality level.5 Although some literature suggested that BSE was not effective in reducing mortality level, studies in developing countries indicate that regular BSE is applicable to identify breast cancer in its early stage and reduce the mortality level.19,20 Indonesian women need to improve their breast awareness, especially given the limited accessibility to health-related resources compared to Western population. Thus, it is reasonable to empower Indonesian woman to practice BSE. The main purpose of this study was to examine the psychometric properties of I-CHBMS. The findings indicate that the 42-item I-CHBMS is a valid and reliable scale to measure health belief underlying BSE practice among Indonesian women.
We performed a validity and reliability study to confirm that I-CHBMS could produce appropriate information as expected. The validity of the questionnaire structure was tested after a translation procedure and the final version of the I-CHBMS was obtained. We translated the CHBMS using forward and backward translation. The validity of the I-CHBMS was confirmed after assessment of suitability, reasonability, logical sequence, conciseness, and comprehensiveness of each item with minor revisions.
We employed CFA to assess the construct validity of the 42 items representing six-factor model of HBM: perceived susceptibility, perceived severity, perceived barriers, perceived benefits, cues to action and self efficacy. CFA is a deductive mode of structural equation modeling dealing specifically with measurement of latent variable responsible for the commonality among a set of scores.21,22 According to Hu and Bentle,16 fit index value is considered applicable when CFI value is 0.092 and greater and RMSEA value is 0.06 or less. In this study, the χ2 value, GFI value, CFI value, AGFI value, RMSEA value and SRMR value were determined consecutively as 2,071.2, 0.08, 0.92, 0.78, 0.06 and 0.064, respectively. The results indicated that the data comply with the theoretical structure, leading to the conclusion that the factor structure of I-CHBMS may provide an applicable scale.
The most widely applicable method to examine internal consistency reliability is coefficient alpha (Cronbach’s alpha). The normal value of Cronbach’s alpha ranges from 0 to 1, in which higher value indicates higher internal consistency reliability.23 The coefficients of Cronbach’s alpha in all six factors of I-CHBMS were 0.844, 0.866, 0.815, 0.825, 0.809, and 0.669 for perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action and self-efficacy, respectively. The result indicated that internal consistency of self-efficacy factor is considered moderate and internal consistencies of other five remaining factors are deemed as showing high level of reliability.
Item analysis is another method to examine the internal consistency of a scale. In this study, total item correlation scores of I-CHBMS were calculated and it was found that the value ranged from 0.368 to 0.780. Item-total correlations of 0.40 or higher values are considered as highly distinguishing items, and those with values lower than 0.30 are indicated as statistically insignificant and are recommended to be excluded from the scale.24 To conclude, as indicated by Cronbach’s alpha and total item correlation, I-CHBMS has an acceptable value of internal consistency for a new instrument applicable for a heterogeneous population among Indonesian women.
It is interesting to compare the findings in Indonesian population to the original scales for a heterogeneous but predominantly middle-class white population.13 It seems that the reliability for I-CHBMS was higher than that in the original version. The Cronbach’s alpha values for perceived susceptibility, perceived severity, perceived benefits and perceived barriers in the original scale were 0.77, 0.78, 0.61 and 0.76, respectively. CHBMS was widely used to study breast cancer screening behavior using HBM perspective. Some studies in Middle East and Far East have indicated that CHBMS had a good reliability. Persian CHBMS,25 which is developed for applying to Iranian women, noted the Cronbach’s alpha values of perceived susceptibility, perceived severity, perceived benefits and perceived barriers were 0.72, 0.75, 0.82 and 0.76, respectively. The Turkish version of CHBMS recorded that the Cronbach’s alpha values of perceived susceptibility, perceived severity, perceived benefits and perceived barriers were 0.77, 0.79, 0.87 and 0.76, respectively.26 The populations of both studies were predominantly with a low education background, married, and unemployed. But the study in Taiwan indicated a higher reliability score, given the Cronbach’s alpha values of perceived susceptibility, perceived severity, perceived benefits and perceived barriers as 0.921, 0.832, 0.915, and 0.874, respectively.27 The population of the study was predominantly educated up to junior high school and below, with a low income and with no employment.
Conclusion
The data from this study lead to the conclusion that I-CHBMS is a valid and reliable measurement tool in all statistical operations. This newly developed scale has the qualities that may be useful in assisting health professionals to measure the health beliefs of individuals in participating in screening behavior, especially in breast cancer early detection using BSE. This information will provide the health professionals with significant information for need assessment, and will help them further to design strategies to improve participation in breast cancer early detection behavior. The use of the scale should be based on the demographic characteristics of the sample in this study; therefore, application to different sample groups should be re-evaluated. This scale was tested in a sample group in Surabaya, East Java with Javanese and Madurese cultural background, and therefore, it should be evaluated in different cultures. It will be beneficial to test validity and reliability to further develop the scale, especially in the cues to action component, which has a moderate level of reliability.
Acknowledgments
The researcher expresses her gratitude to Prof Victoria Champion for the permission to use CHBMS in the research, Dr Rahkman Ardi and Rizqy Amelia Zein, MSc for fruitful statistical discussion, and all the participants in the study. The article was funded by RKAT 2017, Faculty of Psychology, Universitas Airlangga.
Disclosure
The author reports no conflicts of interest in this work.
References
Depkes RI. Riset Kesehatan Dasar (Riskesdas) 2013. Jakarta: Badan Litbang Kemenkes RI; 2013. | ||
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. | ||
Pusdatin Kemenkes RI. Stop Kanker. Jakarta: Kemenkes RI; 2015. | ||
Kementerian Kesehatan RI. Panduan Program Nasional Gerakan Pencegahan Dan Deteksi Dini Kanker Leher Rahim dan Kanker Payudara. Jakarta: Kementerian Kesehatan RI; 2015. | ||
Xiong Q, Valero V, Kau V, et al. Female patients with breast carcinoma age 30 years and younger have a poor prognosis: the M.D. Anderson Cancer Center Experience. Cancer. 2001;92(10):2523–2528. | ||
Erniyati S. Perilaku SADARI wanita pedesaan dan wanita perkotaan. Jurnal Keperawatan Rufaidah Sumatera Utara. 2005;1:1–9. | ||
Oemiyati R, Rahajeng E, Kristanto A. Prevalensi tumor dan beberapa faktor yang mempengaruhinya di Indonesia. Buletin Penelitian Kesehatan. 2011;39(4):190–204. | ||
Mcpherson K, Steel CM, Dixon JM. ABC of breast diseases. Breast cancer-epidemiology, risk factors, and genetics. BMJ. 2000;321(7261):624–628. | ||
Khokhar A. View point: how to make women familiar with their breasts? Asian Pac J Cancer Prev. 2013;14(9):5539–5542. | ||
Taylor SE. Health Psychology. London: McGraw-Hill; 1999. | ||
Rosenstock IM. The health belief model and preventive health behavior. Health Educ Monogr. 1974;2(4):354–386. | ||
Sheeran P, Abraham C. Health belief model. In: Conner M, Norman P, editors. Behavior Predicting Health. London: McGraw Hill; 2005:28–80. | ||
Champion VL. Instrument development for health belief model constructs. ANS Adv Nurs Sci. 1984;6(3):73–85. | ||
Champion VL. Revised susceptibility, benefits, and barriers scale for mammography screening. Res Nurs Health. 1999;22(4):341–348. | ||
Osborne JW, Costello AB. Sample size and subject to item ratio in principal components analysis. Pract Assess Res Eval. 2004;9(11):8–16. | ||
Hu Li-tze, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. | ||
Field A. Discovering Statistics Using SPSS. 3rd ed. London: SAGE; 2009. | ||
Kline P. The Handbook of Psychological Testing. 2nd ed. London: Routledge; 1999. | ||
Lam WW, Chan CP, Chan CF, et al. Factors affecting the palpability of breast lesion by self-examination. Singapore Med J. 2008;49(3):228–232. | ||
Miller AB, Baines CJ. The role of clinical breast examination and breast self-examination. Prev Med. 2011;53(3):118–120. | ||
Brown TA, Moore MT. Confirmatory factor analysis. Handbook of Structural Equation Modeling. 2012:361–379. | ||
Hoyle RH. Confirmatory factor analysis. In: Handbook of Applied Multivariate Statistics and Mathematical Modeling. 2000:465–497. | ||
Gliem JA, Gliem RR. Calculating, interpreting, and reporting Cronbach’s alpha reliability coefficient for Likert-type scales. Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education; 2003. | ||
Polit D, Beck C. Nursing Research: Principles and Methods. 7th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2003. | ||
Hashemian M, Shokravi FA, Lamyian M, Hassanpour K, Akaberi A. Reliability and validity of the Champion’s Health Belief Model Scale for mammography among Iranian women with family history of breast cancer. Health Education and Health Promotion. 2013;1:19–31. | ||
Erbil N, Bölükbas¸ N. Beliefs, attitudes, and behavior of Turkish women about breast cancer and breast self-examination according to a Turkish version of the Champion Health Belief Model Scale. Asian Pac J Cancer Prev. 2012;13(11):5823–5828. | ||
Wang W-L, Hsu S-D, Wang J-H, Huang L-C, Hsu W-L. Survey of breast cancer mammography screening behaviors in Eastern Taiwan based on a health belief model. Kaousiung J Med Sci. 2014;30:422–427. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.