")
Back to Journals » Patient Preference and Adherence » Volume 16
Valid and Convenient Questionnaire Assessment of Chinese Body Constitution: Item Characteristics, Reliability, and Construct Validation
Authors Lu T, Yan J, Chang J, Cai J, Yin L, Yuan J, Huang L, Li Y, Bai M, Hau KT, Wu D, Yang Z
Received 5 May 2022
Accepted for publication 15 July 2022
Published 2 August 2022 Volume 2022:16 Pages 1875—1884
DOI https://doi.org/10.2147/PPA.S373512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Taoying Lu,1– 3 Jingwen Yan,4 Jianfang Chang,5 Jianxiong Cai,1– 3 Lingjia Yin,1,3,6 Jiamin Yuan,1,7 Li Huang,1,7 Yingshuai Li,8 Minghua Bai,9 Kit-Tai Hau,5 Darong Wu,1– 3 Zhimin Yang1,7
1State Key Laboratory of Dampness Syndrome of Chinese Medicine, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 2Guangdong Provincial Key Laboratory of Clinical Research on Traditional Chinese Medicine Syndrome, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 3Program for Outcome Assessment in TCM, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, People’s Republic of China; 4The Second Clinical Medical College of Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 5Department of Education Psychology, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 6Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden; 7Health Construction Administration Center, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, People’s Republic of China; 8National Institute of TCM Constitution and Preventive Medicine, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 9School of Traditional Chinese Medicine/National Institute of TCM Constitution and Preventive Medicine, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
Correspondence: Darong Wu; Zhimin Yang, State Key Laboratory of Dampness Syndrome of Chinese Medicine, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, 111 Dade Road, Guangzhou, 510120, People’s Republic of China, Tel +86 13808869436 ; +86 13822296363, Email [email protected]; [email protected]
Background: Body constitution is a fundamental concept in traditional Chinese medicine (TCM) for clinical diagnosis, treatment of illness, and community-based health promotion. Clinical assessment of patients’ body constitutions, however, has never been easy and consistent, even by well-trained clinicians and TCM practitioners. Therefore, questionnaires such as the popular Constitution in Chinese Medicine Questionnaire (CCMQ) can be an appealing and convenient assessment alternative. The present research borrowed advanced methodologies for questionnaire development in psychology and other social sciences to examine the performance of the CCMQ in terms of (i) the strength of relations of each item with its designated constitution, (ii) the reliabilities of each constitution, and (iii) the overall 9-constitution structure. This research provided empirical evidence to support the use of the CCMQ and proposed directions for refinement in future revisions of the CCMQ or similar measures.
Methods: A total of 1571 volunteers from three villages in southern China participated in the CCMQ survey. The item characteristics, reliabilities, interconstitution correlations, and confirmatory factor analysis of the 9-body-constitution structure were examined.
Results: The results generally supported the appropriateness of the clinical observations (the questionnaire items) and the CCMQ 9-constitution classification structure. Nevertheless, some relatively weaker items, item pairs with similar meanings, and highly overlapping constitutions were identified for future CCMQ revisions.
Conclusion: The CCMQ measured the 9 constitutions efficiently and with reasonably good reliability and construct validity. Given the various challenges to assessing TCM body constitutions even by experienced clinicians, the CCMQ provides an appealing alternative to measure the Chinese body constitutions of healthy participants in large-scale research or community health promotion programs. The present study also demonstrated how advanced methodologies in social sciences can help validate and refine the CCMQ and similar complementary medicine measures.
Keywords: Chinese constitution, body constitution, CCMQ, Constitution in Chinese Medicine Questionnaire, reliability, construct validity
Introduction
Body constitution, an ancient concept of traditional Chinese medicine (TCM), postulates that people have relatively stable unique morphological structures and physiological, psychological, and functional activities due to genetic disposition, acquired factors, and self-regulation.1 People can be classified, therefore, by these similarities and differences in body constitution into many different “types”.2–4 The determination of body constitution helps the effective treatment of illness, health maintenance, and disease prevention. Given that our body constitutions are partly determined from birth through heredity, the knowledge of our constitutions greatly facilitates health maintenance and disease prevention.
Accurately identifying body constitution has never been easy, even for experienced clinicians. Interrater consistency was a major concern,5,6 and people tried to standardize and develop structured TCM interviews.7 Even for 5-year or more experienced acupuncturists, for example, 4 to 6 of them were needed to obtain reliable yin and yang deficiency ratings.8 Training helped improve interrater reliability from 0.11 to 0.62 after three rounds of discussion and training.9 Reviews by Brien and Birch10 also showed that the reliabilities of pulse diagnosis were low to very good, while those of tongue and other diagnoses varied.
Obviously, more training and having several clinicians diagnose each patient or research participant is time-consuming, resource-demanding, and impractical for large-scale empirical research or community health promotion programs. A high-quality questionnaire, therefore, becomes an appealing alternative. Despite such a demand, constructing a valid and reliable instrument is also challenging, particularly in developing an assessment for the healthy general population. It is difficult for clinicians to accurately assess patients with observable illness symptoms, so developing a questionnaire applicable to the nonsymptomatic healthy general population will be even more difficult. Such attempts included the questionnaires on cold, heat, complex, and phlegm.11,12 Among them,13–17 the Constitution in Chinese Medicine Questionnaire (CCMQ)18–20 was probably the most comprehensive and widely used.
The CCMQ by Wang et al was developed in China18–20 but also has been translated and used in Canada, Japan, Korea, and the USA, among other countries.21–23 It consists of 60 items with 9 subscales, each measuring one Chinese body constitution. The items (clinical observations; eg, “Did you get tired easily?”) measure participants’ feelings or symptoms in the last year. It has been shown to have reasonably good psychometric properties24,25 in various medical settings.26–30 Versions of 60, 41, and 30 items in Chinese, English, and Japanese23,31 have been developed and evaluated,32 with over 2277 papers, 55% of which are journal articles published between 2006 and 2016.33
Despite its popularity, challenges to its use included34 (i) difficulty for people with limited education to understand some items, (ii) questionable classification of some items, (iii) many items classified as mixed body constitution, (iv) some items cross-linked to multiple body constitutions,34–36 (v) the originally proposed structure could not be reproduced with empirical data (eg, 8 factors found in research despite the 9 originally proposed in CCMQ),32,37 and (vi) items not allocated to their intended constitutions (many items in some constitutions, but few items in others).32,37 The interrelations among the original items (indicators) were not carefully examined in the previous factor analyses. The more appropriate confirmatory factor analysis was used with patients only in Hong Kong SAR to confirm its original constitution structure.38 However, the results were dubious, with 5 items with standardized loadings larger than 1, 7 items in the unexpected direction (negative instead), and 1 item with extremely low loading (−0.01), suggesting likely inappropriate modeling and the misclassification of items.
The present study contributed academically by adopting advanced methodologies commonly used in psychology and other social sciences questionnaire development.39 Importantly, the traditional exploratory factor analysis used in earlier studies32,37 was replaced by the more appropriate confirmatory factor analysis in this study. The more commonly used exploratory factor analysis can help researchers group items with an unknown structure into factors.39,40 In contrast, confirmatory factor analysis works with items with a known grouping (factors) and provides statistics (fit indices) to inform researchers whether such a grouping is supported or not. Thus, as the grouping (structure) of the CCMQ items was provided by Wang et al,18–20 confirmatory factor analysis was the proper method to examine the correctness of the original item classifications.
Specifically, this study provides empirical evidence on the construct validation and reliability information of the CCMQ. The objectives were to examine (i) the appropriateness of each item (clinical observations of the constitutions) as a measure of its original intended constitutions, (ii) the internal consistency reliability of each constitution, and (iii) the convergent (coherent)/divergent (discriminating) relations among the constitutions. The study not only evaluated the overall fit of the original 9-constitution structure but also examined the suitability of each individual item in the instrument. The information is essential to support the use of this important CCMQ in large-scale research or community health promotion programs when a high-quality and convenient Chinese body constitution instrument is needed.
Materials and Methods
Participants
The 1571 voluntary participants, who individually provided their consent, were residents from three villages in Foshan, a city in Guangdong Province in the southern part of China with a population of approximately 5000. The survey was conducted at local clinics, but only their first-visit responses were used in the analyses, even if they made further visits for other purposes. There were more females than males, and there were more older (older than 40) than younger participants (Table 1).
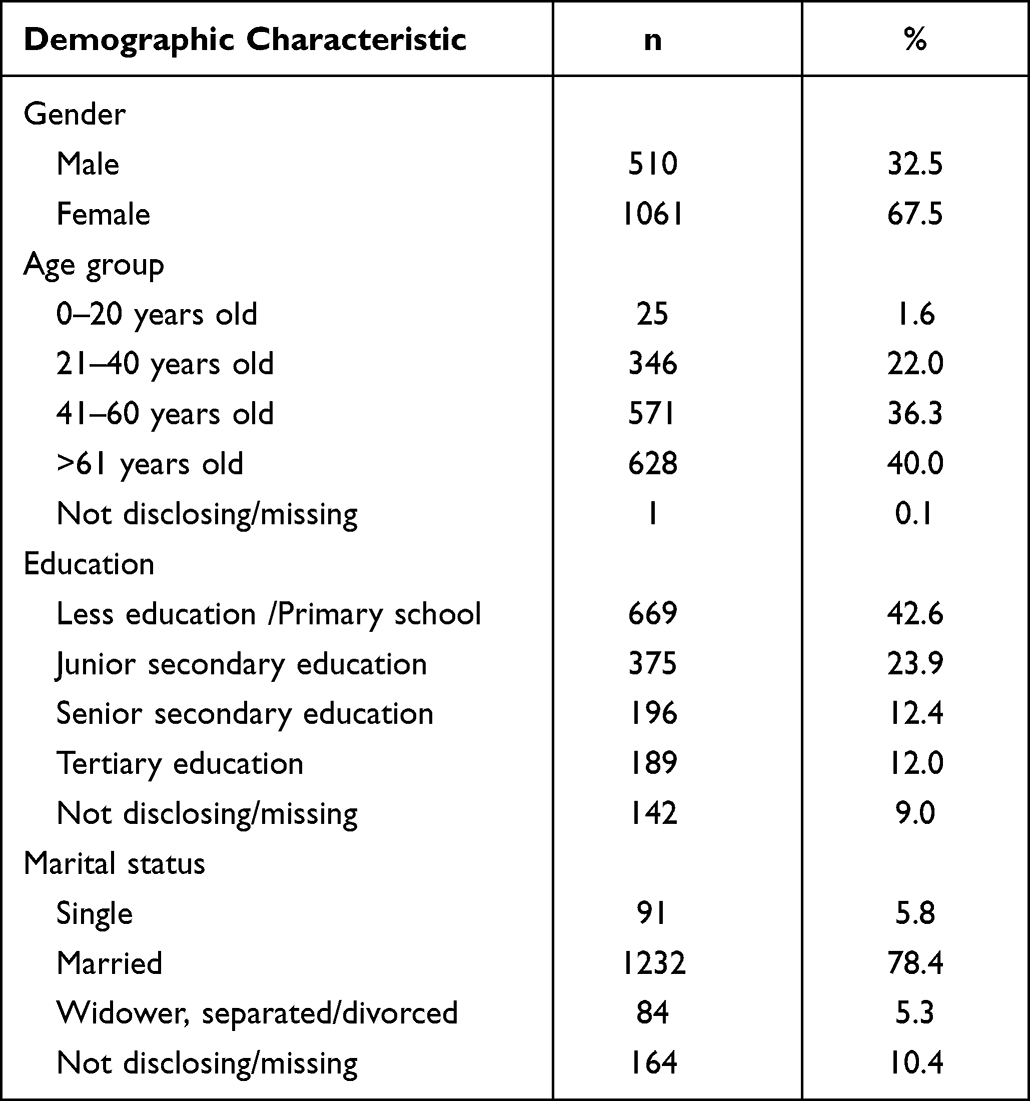 |
Table 1 Demographic Characteristics of Participants (n = 1571) |
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained for this project from the Research Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine (Reference No: B2013-009-01/B2017-150-01). The participants provided written informed consent before answering the survey questionnaire.
Measures
The CCMQ consisted of 60 items (clinical observations, indicators of constitutions, Table 2) categorized into 9 subscales, each measuring one of the 9 different body constitutions, namely, Yang-deficient (7 items), Yin-deficient (8 items), Qi-deficient (8 items), Phlegm-dampness (8 items), Damp-heat (6 items), Stagnant Blood (7 items), Inherited Special (7 items), Stagnant Qi (7 items), and Balanced (8 items). The items were on a 5-point Likert scale, with high scores indicating a higher likelihood of having the given constitution. Usually, a threshold of 30 or higher points on a subscale was used to classify a person as having that body constitution.
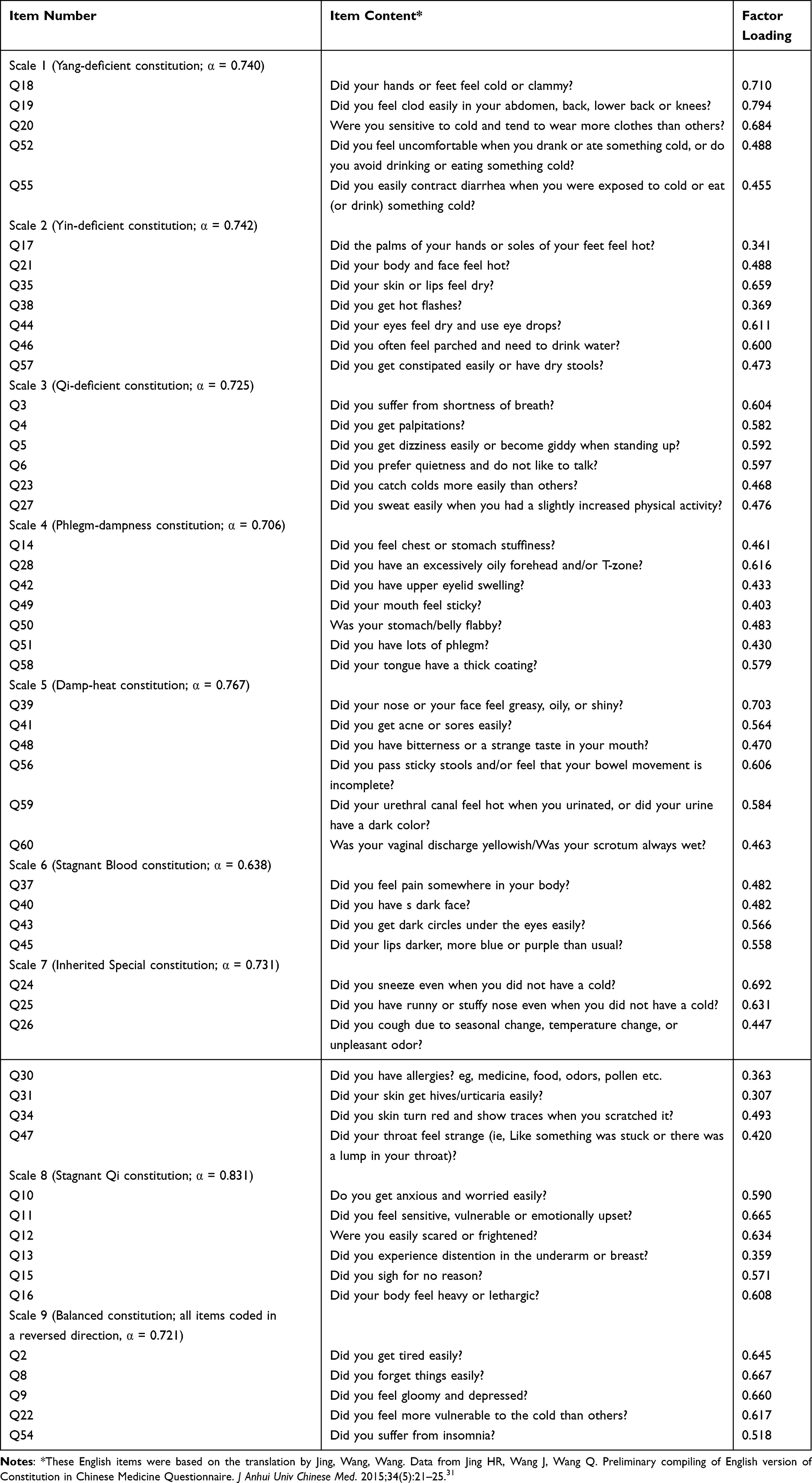 |
Table 2 Reliabilities of 9 Subscales, Item Content, and Standardized Loadings |
Analyses
As there were more females and older participants, a weight (inverse to the group ratio) was added so that all analyses were based on a weighted sample with equal representation of the gender and age groups. In this study, the original structure and classifications of the CCMQ items were known. Thus, confirmatory factor analysis was more appropriately used to assess the suitability of this 9-constitution classification.
To assess whether the items (clinical observations) consistently assessed the respective constitutions, internal consistency reliability measured by Cronbach’s alpha was computed for each of the 9 constitutions (Table 2). In the confirmatory factor analysis, (i) the strength of the relationship of each item to the constitution (ie, factor loading) showing possible misclassified items, (ii) the overall success in measuring the 9 constitutions (ie, model fit), and (iii) the possible weak items measuring more than one constitution (ie, correlated uniqueness in confirmatory factor analysis terminology) were examined with the commercial software Mplus 8.1.40
Results
Preliminary Analyses—Identification of Misclassified Items
In the first stage of the analyses, weak items unrelated to their originally intended and other constitutions were identified and removed. This was based on (i) Cronbach’s alpha (Table 2), (ii) Cronbach’s alpha if-item-deleted, and (iii) corrected item-total correlations. Unless there were strong face-validity reasons, items were potentially removed if (i) they had low corrected item-total correlations, (ii) Cronbach’s alpha was substantially improved when they were deleted, (iii) they had low correlations with other items in the same scale, and (iv) they had low correlations with other constitutions (ie, impossible to reassign to another constitution). Seven items were removed using these criteria (Q1, Q7, Q29, Q32, Q33, Q36, and Q53).
Strength of Relations with Respective constitutions—reliability and Factor Loadings
This study showed that items within each constitution were consistently correlated, with the reliabilities of the constitutions ranging from 0.638 to 0.831 (see Table 2); the lowest reliability, 0.638, was associated with the shortest scale with only 4 items. Confirmatory factor analysis of the 9 factors (Table 2) was conducted on the remaining 53 items, with items grouped under their respective constitutions, and all constitutions were allowed to be correlated. Items were reasonably related to their respective constitutions, with standardized factor loadings ranging from 0.307 to 0.793. Only 5 items had loadings less than 0.4, suggesting that they were weaker items less related to their constitutions and required closer examination in future CCMQ revisions. They were Q17 (Did the palms of your hands or soles of your feet feel hot?), Q38 (Did you get hot flashes?), Q30 [Did you have allergies (eg, medicine, food, odors, pollen, etc.?)], Q31 (Did your skin get hives/urticaria easily?), and Q13 (Did you experience distention in the underarm or breast?).
Overall Appropriateness of the 9-Constitutions Structure—Model Fit
The assessment of the overall 9 constitution structures with confirmatory factor analysis showed that Phlegm-dampness (Factor 4, F4) was extremely highly correlated with the Damp-heat constitution (F5), resulting in an improper (mathematically nonpositive definite) solution. This suggested that Phlegm-dampness and Damp-heat cannot be effectively differentiated from the present set of items. Consequently, they were grouped as a new Dampness factor (a second-order factor F10). Furthermore, some of these clinical observations (the 53 items) in the same or different constitutions were very similar and strongly related (see next section; correlated uniquenesses in the confirmatory factor analysis terminology). The overall fit of the 53 items to the eventual model was acceptable; various indices of model fit were χ2 (1263) = 4516.27, RMSEA = 0.040 (90% CI, 0.039–0.042), Prob. (RMSEA ≤.05) = 1.000, CFI = 0.90, TLI = 0.89. Using the criteria generally adopted,41,42 the fit indices reaffirmed that the data collected fit the originally intended 9-constitution structure reasonably well.
Items (Clinical Observations) Related to More Than One Constitution (Correlated Items)
As discussed above, it was reasonable to postulate before assessing the model fit that some clinical observations (the items) in the same or different constitutions captured similar clinical characteristics and were thus highly correlated. For example, Q24 (Did you sneeze even when you did not have a cold?) and Q25 (Did you have a runny or stuffy nose even when you did not have a cold?), both in the Inherited Special constitution (F7), were strongly related (standardized correlated uniqueness = 0.39). This showed that Q24 and Q25 had commonality over and above (statistically a correlated uniqueness) that captured by their common Inherited Special constitution (F7). Similarly, Q31 and Q30 (both in F7; correlated uniqueness = 0.20) and Q39 and Q41 (both in F5, correlated uniqueness = 0.20) had similarly substantial correlations. As these item pairs came from the same constitutions, one of the two items can be removed, or the two items can be combined in future CCMQ revisions.
There were also pairs of clinical observations coming from two different constitutions. They included, for example, Q20 (F1) and Q22 (F9; correlated uniqueness = 0.37); Q39 (F5) and Q28 (F4; 0.33); Q57 (F2) and Q56 (F5; 0.21); Q22 (F9) and Q19 (F1; 0.23); Q48 (F5) and Q46 (F2; 0.20); and Q51 (F4) and Q47 (F7; 0.20), which came from two constitutions and were correlated. For these item pairs from different constitutions, (i) one or both items in the item pair can be revised so that they focus on one constitution only, or (ii) one or both items in the item pair can be removed if they have double and confusing meanings.
Relations Among Constitutions
The correlations among the constitutions (Table 3) showed moderate to strong relations, supporting their commonality in measuring the individuals’ TCM body characteristics. It was also noted that the Balanced constitution (F9) was negatively correlated with all other scales, which suggested it was measuring body constitution from an opposite perspective to those of the other eight constitutions. In general, it was understandable that the Phlegm-dampness constitution (F4) and Damp-heat constitution (F5), both measuring “dampness”, were highly correlated. Similarly, the Yang-deficient constitution (F1), Yin-deficient constitution (F2), and Qi-deficient constitution (F3) were also moderately to highly correlated, measuring “deficiency”. The Stagnant Qi constitution (F8) and Balanced constitution (F9) were closely but negatively related. The Stagnant Blood constitution (F6) and Inherited Special constitution (F7) were two constitutions much less associated with the remaining constitutions (F1, F2, F3, F4, F5, F8, F9).
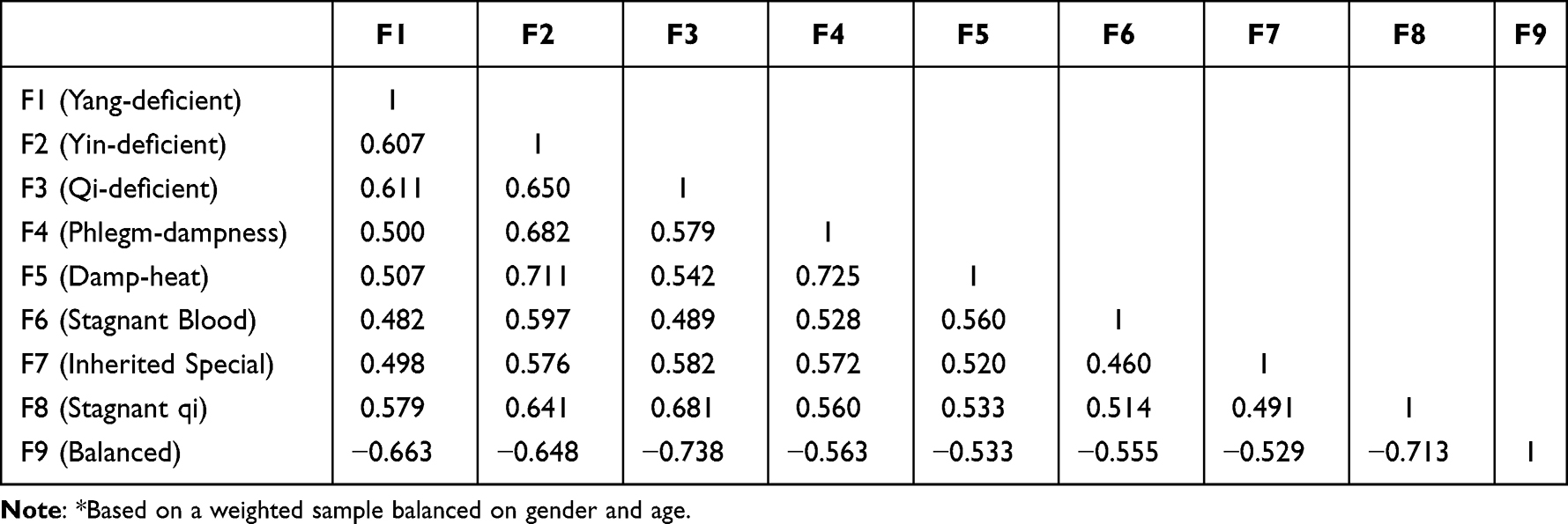 |
Table 3 Correlations Among the Constitutions Scores* |
Discussion
The quality and usefulness of the CCMQ were assessed comprehensively from a wide range of psychometric properties. Specifically, (a) the reliability of each constitution was reasonably high (0.638–0.831), (b) most item-constitution relations (ie, factor loading) were high, and five items with weaker loadings were identified, and (c) confirmatory factor analysis showed good fit of data to the model, broadly supporting the appropriateness of the clinical observations (the questionnaire items) as measures of their intended 9 constitutions. That is, the CCMQ instrument successfully captured the general construct of Chinese body constitutions, while the 9 (eventually combined into 8) separate scales also appropriately differentiated the body constitutions.
At this juncture, we would like to point out that our findings on the performance of CCMQ constitutions and items have direct implications on CTM clinical diagnosis, prognosis, and treatment in general. Thus, for example, our results showed that the Phlegm-dampness and Damp-heat scales were highly correlated. This suggested that in clinical assessment and treatment, clinicians would find great difficulties in differentiating these two constitutions. Clinicians and instrument developers must identify new items to better differentiate these two constitutions. Similarly, for the weak items we identified below, clinicians are also alerted that clinical observations on these symptoms may have to be adjusted accordingly (see Table 4).
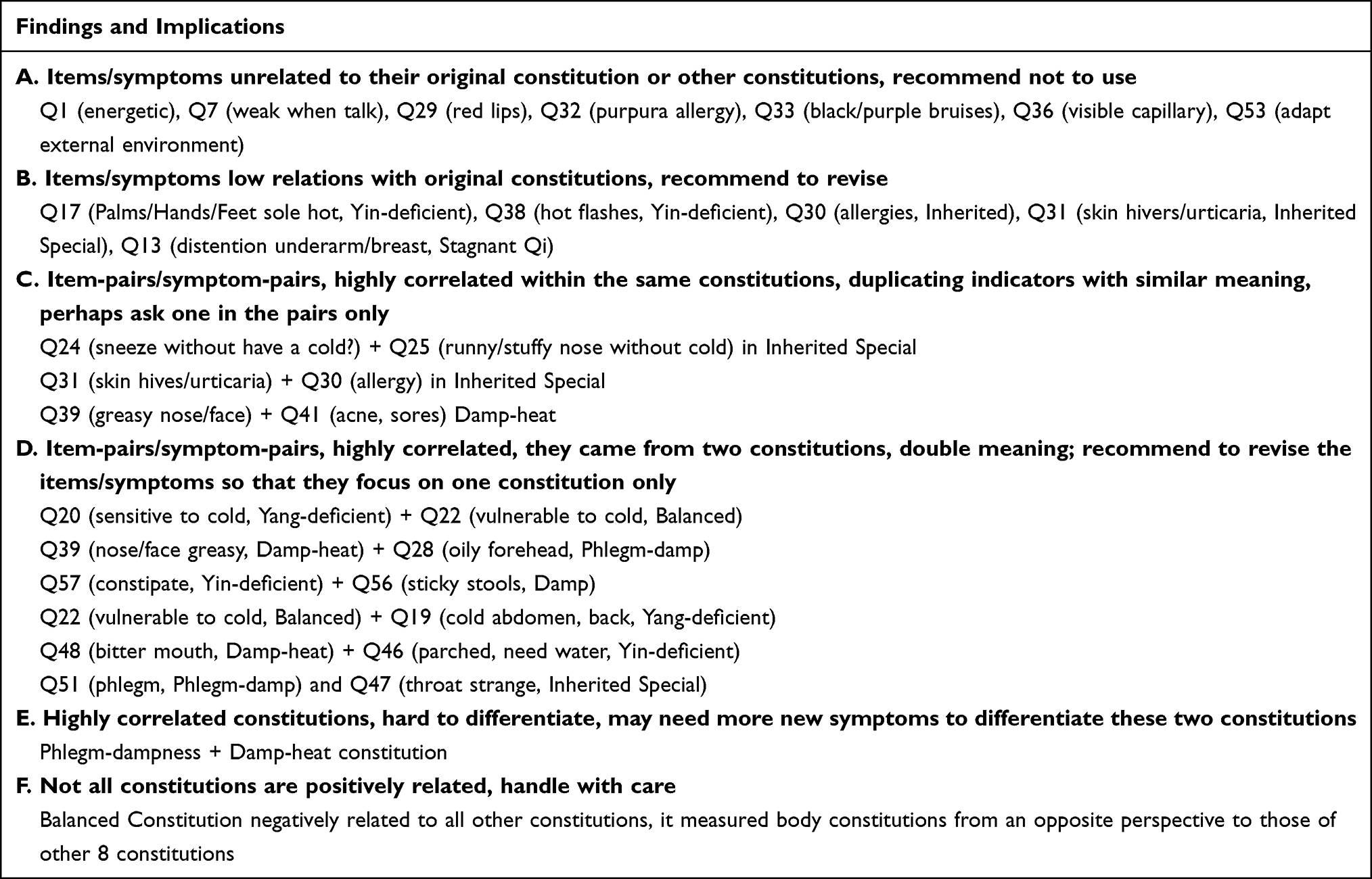 |
Table 4 Summary of Findings and Implications to Clinicians and Instrument Construction |
Based on the reliability analyses, 7 items (Q1, Q7, Q29, Q32, Q33, Q36, and Q53) were removed from this study. In a previous study,43 these items (except Q29) were also deleted based on their psychometric properties (eg, Cronbach’s alpha, item response theory) and expert panel opinion (face validity). The results and recommendations in this study were, therefore, generally consistent with a previous study.43 Contentwise, Q29 (Were your lips redder than others?) in the Yin-deficient constitution (F2) seemed essential for identifying the Yin-deficient constitution. While it is true that some people’s lips with Yin-deficient constitution might be redder than others, it is also possible that some people with Damp-heat constitution might also have similar characteristics. Such items may not discriminate well in the identification of the constitution. It could be one of the potential items, therefore, for deletion in future CCMQ revisions.
This study showed that 5 items (Q13, Q17, Q30, Q31, and Q38) were weaker measures of their respective constitutions (loading less than 0.4). In previous studies,43,44 Q38 and Q31 were also recommended to be removed based on psychometric properties and expert panel opinion (face validity). Relatively, Q17, Q30, and Q13 also had weaker relations with their constitutions. However, they appeared to be important indicators in body constitution identification in clinical diagnosis and can be retained. Nevertheless, these items can still be revisited and polished in future CCMQ revisions. For example, in Q17, “Do the palms of your hands or soles of your feet feel hot?”, some people might have hot palms but cold soles (rather than both hot) and would have difficulty answering this item. Importantly, this study helped identify items that should be carefully examined and further polished.
Although the study started with a 9-constitution structure, the results suggested that some constitutions (eg, Phlegm-dampness constitution, Damp-heat constitution) were highly correlated and hard to differentiate by the participants using the present set of items. Furthermore, the differentiation of other constitutions can also be revisited and improved. For example, high correlations were observed between Q24 and Q25, Q31 and Q30, and Q39 and Q41. These results suggested that the items in these item pairs can be less discriminating, confusing, or similar for many patients. Notably, again, this study identified items or item pairs that can be revised or removed in future CCMQ revisions.
The conclusions drawn from the present study were limited by the participants being recruited from three villages in southern China. Future replications with participants from other geographic regions in China or other countries would provide information on how generalizable the results in this study are for future CCMQ revisions.
Conclusions
In this study, the items and structure of a popular TCM body constitution questionnaire were carefully assessed with a sufficiently large sample size of healthy participants. Generally, the results showed that the CCMQ had reasonably good reliability, differentiating constitution structure, and construct validity to support its use as a valid and convenient Chinese body constitution assessment instrument. Nonetheless, through the analyses of its reliabilities, correlations of items to their respective constitutions, relations among the constitutions, and correlations among item pairs, various issues with the items or constitutions have been identified to facilitate future CCMQ revisions or enhancements. This agrees with the CCMQ’s original authors’ recommendation that accumulated experience would help our timely revisions of the original instruments.34 Indirectly, this study also provided an exemplary practical approach based on advanced methodologies used in psychology and other social sciences to analyze and refine the CCMQ and other TCM questionnaires. Our results have similar critical applications for CTM clinicians using various symptoms as measures of Chinese constitutions in assessment, treatment, and health promotion (see Table 4).
Acknowledgments
We would like to thank all the participants from the three villages, namely, Shilian Village, Xiangang Village, and Songtang Village. We also extend our thanks to all the staff and the village heads for their support and work, especially Dr. Xiaoming Ma from the 8th People’s Hospital of Nanhai District, Foshan, Guangdong, Dr. Weitong from the Fourth People’s Hospital of Nanhai District, Foshan, Guangdong, and Dr. Peixia Lu from Xiqiao Town Community Health Service Center of Nanhai District, Foshan, Guangdong.
Funding
This study was funded by the National Key R&D Program of China (No.2019YFC1709800/ No. 2019YFC1709802); the State Key Laboratory of Dampness Syndrome of Chinese Medicine (No.SZ2021ZZ03/No.SZ2021ZZ0302/No.SZ2021ZZ30/No.SZ2020ZZ10/No.SZ2020ZZ09/ No.SZ2021ZZ32); the Guangdong Provincial Key Laboratory of Clinical Research on Traditional Chinese Medicine Syndrome (No. ZH2019ZZ04); the Science and Technology Planning Project of Guangdong Province (No. 2017B030314166). The funders did not participate in the design, data collection, management, analysis, approval of the manuscript, and decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wang Q. Constitution of Traditional Chinese Medicine.
2. Wang Q. The Discovery of Nine Constitutions of Chinese People. Beijing: Science Press; 2011:8–9.
3. Yang XG, Li XZ, Ren Y, et al. Classification of traditional Chinese medicine constitution and questionnaire: application and research. Chin J of Integr Trad & West Med. 2017;37(8):1003–1007.
4. Zhang C. Modern research progress in TCM constitution identification. Chin J Informat TCM. 2000;27(9):1–4.
5. Brien KA, Abbas E, Zhang J, et al. An investigation into the reliability of Chinese medicine diagnosis according to eight guiding principles and Zang-Fu theory in Australians with hypercholesterolemia. J Altern Complement Med. 2009;15(3):259–266. doi:10.1089/acm.2008.0204
6. Brien KA, Abbas E, Zhang J, et al. Understanding the reliability of diagnostic variables in a Chinese medicine examination. J Altern Complement Med. 2009;15(7):727–734. doi:10.1089/acm.2008.0554
7. Schnyer RN, Conboy LA, Jacobson E, et al. Development of a Chinese medicine assessment measure: an interdisciplinary approach using the Delphi method. J Altern Complement Med. 2005;11(6):1005–1013. doi:10.1089/acm.2005.11.1005
8. Langevin HM, Badger GJ, Povolny BK, et al. Yin scores and Yang scores: a new method for quantitative diagnostic evaluation in Traditional Chinese Medicine Research. J Altern Complement Med. 2004;10(2):389–395. doi:10.1089/107555304323062392
9. Mist S, Ritenbaugh C, Aickin M. Effects of questionnaire-based diagnosis and training on inter-rater reliability among practitioners of traditional Chinese medicine. J Altern Complement Med. 2009;15(7):703–709. doi:10.1089/acm.2008.0488
10. Brien KA, Birch S. A review of the reliability of traditional East Asian medicine diagnoses. J Altern Complement Med. 2009;15(4):353–366. doi:10.1089/acm.2008.0455
11. Ryu H, Lee H, Kim H, Kim J. Reliability and validity of a cold-heat pattern questionnaire for traditional Chinese medicine. J Altern Complement Med. 2010;16(6):663–667. doi:10.1089/acm.2009.0331
12. Park YJ, Park JS, Kim MY, et al. Development of a valid and reliable phlegm pattern questionnaire. J Altern Complement Med. 2010;17(9):851–858. doi:10.1089/acm.2010.0504
13. Lin JD, Chen LL, Lin JS, et al. BCQ-: a body constitution questionnaire to assess Yin-Xu. Part I: establishment of a provisional version through a Delphi process. Forsch Komplementmed. 2012;19(5):234–241. doi:10.1159/000343580
14. Lin JS, Chen LL, Lin JD, et al. BCQ-: a body constitution questionnaire to assess Yin-Xu. Part II: evaluation of reliability and validity. Forsch Komplementmed. 2012;19(6):285–292.
15. Lin JD, Lin JS, Chen LL, et al. BCQs: a body constitution questionnaire to assess stasis in traditional Chinese medicine. Eur J Integr Med. 2012;4(4):e379–e391. doi:10.1016/j.eujim.2012.05.001
16. Zheng SS, Li JX, Wang YL, et al. Study on TCM syndrome elements identification scale for chronic gastritis. China Medical Herald. 2018;15(18):120–123.
17. Su YC, Chen LL, Lin JD, et al. BCQ+: a body constitution questionnaire to assess Yang-Xu. Part I: establishment of a first final version through a Delphi process. Forsch Komplementmed. 2008;15(6):327–334. doi:10.1159/000175938
18. Wang Q. The foundation of the classification and diagnosis standards for the constitutions of TCM. Chin Standardization. 2009;32:16–26.
19. Wang Q, Zhu YB, Xue HS, et al. Primary compiling of Constitution in Chinese Medicine Questionnaire. Chin J Clin Rehabil. 2006;10(3):12–14.
20. Wang Q. Classification and diagnosis basis of nine basic constitutions in Chinese medicine. J Beijing Univ Tradit Chin Med. 2005;28(4):1–8.
21. Jing HR, Wang J, Wang Q, et al. Applying Constitution in Chinese Medicine Questionnaire (English version) to survey TCM constitutions of the American and Canadian Caucasian in Beijing. Chin J Tradit Chin Med Pharm. 2012;27(9):2417–2419.
22. Li BM, Cao HJ, Tian EH, et al. A cross-sectional study of a Korean population using The Standardized Constitution in Chinese Medicine Questionnaire (Korean Version). J Anhui Univ Chin Med. 2015;34(4):25–28.
23. Zhu YB, Origasa H, Uebaba K, et al. Development and validation of the Japanese version of the Constitution in Chinese Medicine Questionnaire (CCMQ). Kampo Med. 2008;59(6):783–792. doi:10.3937/kampomed.59.783
24. Zhu YB, Wang Q, Xue HS, et al. Preliminary assessment on performance of Constitution in Chinese Medicine Questionnaire. Chin J Clin Rehabil. 2006;10(3):15–17.
25. Zhu YB, Wang Q, Hideki O. Evaluation on reliability and validity of the Constitution in Chinese Medicine Questionnaire (CCMQ). Chin J Behav Med Sci. 2007;16(7):651–654.
26. Yeh MH, Chao CH, Koo M, et al. Association of traditional Chinese medicine body constitution and moderate-to-severe cancer-related fatigue in cancer patients. Complement Ther Med. 2019;43:44–48. doi:10.1016/j.ctim.2019.01.004
27. Tang YC, Zhao T, Huang N, et al. Identification of traditional Chinese medicine constitutions and physiological indexes risk factors in metabolic syndrome: a data mining approach. Evid Based Complement Alternat Med. 2019;2019:1686205. doi:10.1155/2019/1686205
28. Kanazawa S, Zhu YB, Wang Q. Correlation between Chinese medicine constitution and skin types: a study on 187 Japanese women. Chin J Integr Med. 2020;26(3):174–179. doi:10.1007/s11655-019-2709-3
29. Mou X, Zhou DY, Liu WH, et al. Study on the relationship between Chinese medicine constitutive susceptibility and diversity of syndrome in diabetic nephropathy. Chin J Integr Med. 2013;19(9):656–662. doi:10.1007/s11655-013-1411-0
30. Mou X, Liu WH, Zhou DY, et al. Association of Chinese medicine constitution susceptibility to diabetic nephropathy and transforming growth factor-β1 (T869C) gene polymorphism. Chin J Integr Med. 2011;17(9):680–684. doi:10.1007/s11655-011-0845-5
31. Jing HR, Wang J, Wang Q. Preliminary compiling of English version of Constitution in Chinese Medicine Questionnaire. J Anhui Univ Chinese Med. 2015;34(5):21–25.
32. Zhu YB, Shi HM, Yu XH. Comparison of the performance of three versions of constitution of Chinese medicine questionnaire for healthy populations. Chin Gen Pract. 2019;22(35):4381–4387.
33. Zhu LB, Wang J, Zheng YF, et al. Bibliometrics analysis of traditional Chinese Medicine Constitution Scale from 2006 to 2016. Guangming Zhongyi. 2018;33(20):2939–2944.
34. Zhu LB, Wang J, Li YS, et al. Discussion on revision of constitution in Chinese medicine questionnaire. J Anhui Univ Chinese Med. 2016;35(4):6–9.
35. Li YS, Yang Y, Li LR, et al. Interpretation on the difficult problems in application of traditional Chinese Medicine Constitution Scale. J Tradit Chin Med. 2015;56(10):844–846.
36. Xin H, Wu JK, Guo X, et al. Discussion on the problems of nine traditional Chinese medicine constitutional types scale in clinical application. Chin J Tradit Chin Med Pharm. 2014;29(6):1841–1843.
37. Zhu YB, Wang Q, Yu XH, et al. Construct validity and responsiveness of the 41- item short version of Constitution in Chinese Medicine Questionnaire. Chin Gen Pract. 2017;20(26):3282–3286.
38. Wong W, Lam CL, Wong VT, et al. Validation of the Constitution in Chinese Medicine Questionnaire: does the traditional Chinese medicine concept of body constitution exist? Evid Based Complement Alternat Med. 2013;2013:481–491. doi:10.1155/2013/481491
39. Marsh HW, Hau KT. Applications of latent-variable models in educational psychology: the need for methodological-substantive synergies. Contemp Educ Psychol. 2007;32(1):151–170. doi:10.1016/j.cedpsych.2006.10.008
40. Muthén LK, Muthén BO. Mplus User’s Guide.
41. Marsh HW, Balla JR, Hau KT. An evaluation of incremental fit indexes: a clarification of mathematical and empirical properties. In: Marcoulides GA, Schumacker RE, eds. Advanced Structural Equation Modeling Techniques. Mahwah (NJ): Lawrence Erlbaum; 1996: 315–353
42. Marsh HW, Hau KT, Wen ZL. In search of golden rules: comment on hypothesis testing approaches to setting cutoff values for fit indexes and dangers in over generalising Hu & Bentler (1999) findings. Struct Equ Modeling. 2004;11:320–341. doi:10.1207/s15328007sem1103_2
43. Zhu YB, Yu XH, Wang Q, et al. Preliminary development and evaluation of the short- version Constitution in Chinese Medicine Questionnaire. Chin Gen Pract. 2017;20(7):879–885.
44. Zhu YB, Wang Q, Shi HM, et al. Formulation and evaluation on short version of Chinese Medical Constitution Questionnaire with 30 items. J Tradit Chin Med. 2018;59(18):1554–1559.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.