")
Back to Journals » Clinical Ophthalmology » Volume 11
Uveitis incidence in Jichi Medical University Hospital, Japan, during 2011-2015
Authors Takahashi R, Yoshida A, Inoda S , Okubo A, Kawashima H
Received 11 January 2017
Accepted for publication 29 April 2017
Published 15 June 2017 Volume 2017:11 Pages 1151—1156
DOI https://doi.org/10.2147/OPTH.S132184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ryota Takahashi,1 Atsushi Yoshida,2 Satoru Inoda,3 Akira Okubo,4 Hidetoshi Kawashima5
1Department of Ophthalmology, Jichi Medical University, Shimotsuke, Tochigi, 2Division of Ophthalmology, The Cancer Institute Hospital of JFCR, Koto, Tokyo, 3Department of Ophthalmology, Jichi Medical University, Shimotsuke, Tochigi, 4Okubo Eye Clinic, Tochigi, 5Department of Ophthalmology, Jichi Medical University, Shimotsuke, Tochigi, Japan
Purpose: To investigate uveitis incidence of new patients who visited Jichi Medical University Hospital, Tochigi, north of Tokyo, during 2011–2015, and to compare the results with previously reported data from other facilities.
Methods: We retrospectively analyzed clinical records of new patients with uveitis from April 2011 to March 2015 and compared the uveitis incidence with those from other hospitals.
Results: A total of 502 patients were enrolled in the study; definite diagnoses were made in 262 patients (52.2%). The top 4 diseases were sarcoidosis, 47 patients (9.4%); Vogt–Koyanagi–Harada (VKH) disease, 35 patients (7.0%); herpetic iritis, 29 patients (5.8%); and Behçet’s disease, 21 patients (4.2%).
Conclusion: The most commonly diagnosed diseases in our study were sarcoidosis, VKH disease, herpetic iritis, and Behçet’s disease. Compared with the latest nationwide survey in Japan, our results showed similar trends.
Keywords: uveitis, Behçet’s disease, sarcoidosis, Vogt–Koyanagi–Harada disease, herpetic iritis, etiological analysis
Introduction
Correct diagnoses of patients are essential for adequate and proper therapeutic modalities, thus being one of the crucial factors for obtaining favorable outcomes in many diseases such as uveitis. Regional and updated recognition of uveitis etiologies diagnosed in a given area during a certain period of time is, thus, crucial for desirable prognoses. Together with the information concerning the similarities and differences between regional etiologies as well as trends throughout the era, we can be assured of the overall aptness of the reached diagnoses and provide patients with suitable treatments.
Numerous etiological studies have been conducted and reported either from single institutes1–7 or as nation-wide surveys in Japan,8,9 as well as those from other countries.10–14 Genetic, geographic, social, and environmental factors may impact the distribution of etiologies and frequencies of any given diseases. In Japan, Behçet’s disease, sarcoidosis, and Vogt–Koyanagi–Harada disease (VKH) had traditionally been the top 3 uveitides.1–9 A nation-wide survey in 20099 reported that the rates of Behçet’s disease and bacterial endophthalmitis decreased, whereas those of acute anterior uveitis (AAU) and masquerade syndrome increased when compared with the nation-wide survey conducted in 2002.8
The investigation of current trends in the frequencies of various uveitides is, therefore, essential for establishing proper diagnoses and disease management. Because the current trends of our region (whether different from other institutes or not) are not available, we investigated the etiological facts of the patients with uveitis in our clinic over a 4-year period, 2011–2015.
Methods
We retrospectively investigated the records of all patients with uveitis who visited our uveitis clinic for the first time in Jichi Medical University Hospital, Tochigi north of Tokyo, during the 4-year period between April 2011 and March 2015. Clinical data collected in this study included age, gender, diagnosis through ophthalmic examination, and medical evaluation (all clinical records were handled carefully in a confidential manner). Ophthalmic evaluation included best-corrected visual acuity, applanation tonometry, slit-lamp examination, and ophthalmoscopy. Fluorescein angiography and optical coherence tomography were conducted whenever necessary. Patients received medical evaluation of a series of laboratory blood tests (peripheral blood count, calcium, sodium, potassium, chloride, elevated sedimentation rate, C-reactive protein, glucose, serum angiotensin-converting enzyme, rheumatoid factor, antinuclear antibody, single-stranded deoxyribonucleic acid [DNA], double-stranded deoxyribonucleic DNA, total protein, albumin, lactate dehydrogenase, alanine aminotransferase, aspartate aminotransferase, blood urea nitrogen, creatinine, creatine kinase, β-D-glucan, treponema pallidum latex agglutination, antihuman T-cell lymphotropic virus type I antibody, immunoglobulin M [IgM] and immunoglobulin G [IgG] of toxoplasma, IgM and IgG of herpes simplex virus [HSV], IgM and IgG of varicella zoster virus [VZV], IgM and IgG of cytomegalovirus [CMV]), urine tests (urine protein, glucose, ketone body, occult blood, white blood cell, α1-microglobulin), chest X-ray, and purified protein derivative of tuberculin reaction (Mantoux reaction test). Further physical checkups were given by physician(s) whenever necessary.
In our study, we primarily adopted the categories used in the most recent nationwide survey in Japan, 2009.9 Several diagnostic procedures are described hereafter. For sarcoidosis, the diagnosis established by the Diffuse Pulmonary Disease Research Committee of Japan was adopted.15 For VKH, we adopted criteria previously reported.16
Herpetic iritis was diagnosed in patients with skin lesions of herpes zoster ophthalmicus. Patients without skin lesions received polymerase chain reaction (PCR) assay. Ocular fluid samples were collected and sent to a commercially available laboratory company (Special Reference Laboratory, Tokyo, Japan) for qualitative PCR assay to detect VZV, HSV, and CMV. Even without positive results of PCR, diagnosis was conferred after the development of iris atrophy or good responses to the antiviral therapy.
Diagnosis of Behçet’s disease was based on the criteria presented by the Behçet’s Disease Research Committee of Japan.17 As for AAU, systemic diseases such as ankylosing spondylitis (AS), inflammatory bowel disease (IBD), and psoriasis were carefully examined by physician(s) when anterior uveitis was present.18,19 Human leukocyte antigen (HLA)-B27 was examined as well when available. When observed together with AS, IBD, psoriasis, or HLA-B27, patients were listed as stated in the definite group. When AAU patients were without any of these systemic diseases nor HLA-B27, they were categorized as AAU patients of unknown origin in the undefined group.
The diagnoses of fungal infection and bacterial endophthalmitis were reached together with ocular symptoms, laboratory tests (blood culture and serum β-D-glucan), PCR detection of bacterial and fungal DNA in ocular fluid samples by broad range PCR (samples sent to Department of Ophthalmology, University of Tokyo and analyzed, courtesy of Dr Kaburaki),20,21 and response to antibiotics and antifungal drugs.
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis was also investigated by physician(s) when intraocular inflammation was present together with increased p-ANCA or c-ANCA.22
The most common and second most common uveitides were investigated in various age ranges, that is, age range 0–19 years (n=14), 20–39 years (n=63), 40–59 years (n=84), and ≥60 years (n=127), respectively. In addition, the trends of the top 4 uveitides (TOP4) of our study in various age ranges were investigated. Furthermore, TOP4 were compared for the frequencies in other reports, that is, from nation-wide survey in Japan, single institutes, other parts of Asia, Europe, or North America.
This study was approved by the ethical committee of Jichi University Hospital. Patient consent to review their clinical records was not required in accordance with the ethical guideline regarding epidemiologic studies by the Ministry of Education, Culture, Sports, Science, and Technology, as well as the Ministry of Health, Labor, and Welfare, Japan.
Results
Our clinic receives ~2,500 new patients per year from other institutes in the Kanto area north of Tokyo. Approximately 5% of the annual newly arrived patients during the period were diagnosed with uveitis.
The distribution of the ages of newly arrived patients with uveitis during the 4-year period is shown in Figure 1. The mean age ± SD of the whole patients was 53.5±18.0 years (range 5–90), whereas that of male (210 patients) was 52.8±18.0 years (range 6–84) and that of female (292 patients) was 54.1±18.0 years (range 5–90), respectively.
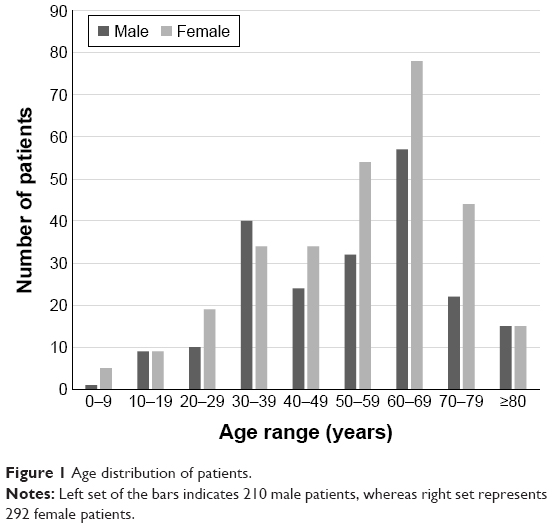 | Figure 1 Age distribution of patients. |
Definite diagnoses were reached in 262 cases (52.2%), and are shown in Table 1. TOP4 of our current study were sarcoidosis, 47 patients (9.4%); VKH disease, 35 patients (7.0%); herpetic iritis, 29 patients (5.8%); and Behçet’s disease, 21 patients (4.2%). These TOP4 in our study accounted for approximately half of the patients with definite diagnoses. The remaining patients with definite diseases and the patients with undefined diseases (as a whole) are listed in Table 1.
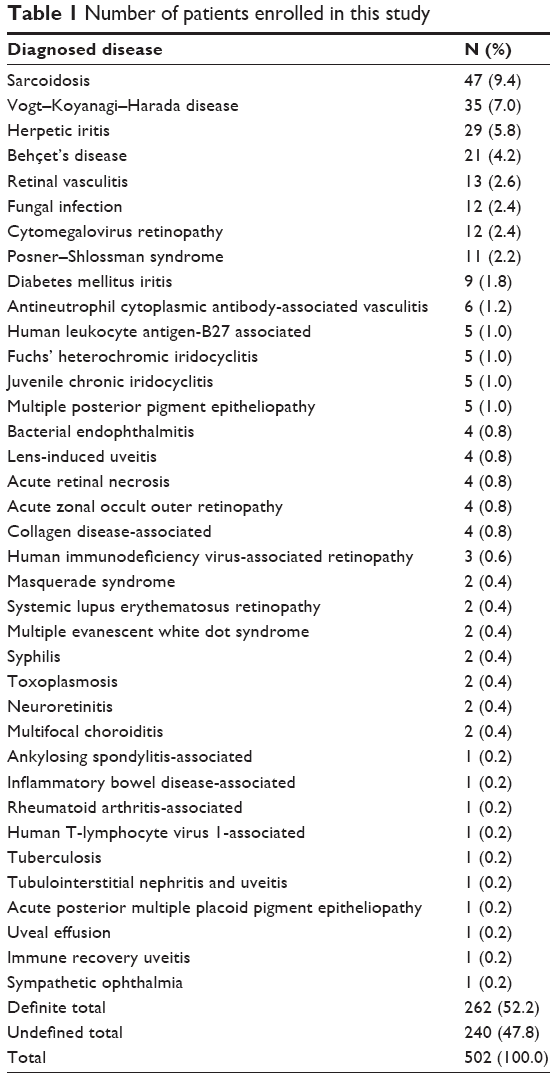 | Table 1 Number of patients enrolled in this study |
In detail, sarcoidosis was diagnosed by histological examination in 22 patients (47%), whereas 25 patients (53%) were clinically diagnosed. VKH disease was accompanied with whitening of hair in 3 patients (9%). Neurologic signs and symptoms were evident in 26 patients (74%), meanwhile the other cases were unquestionably typical in ocular findings.
Herpetic iritis was confirmed by positive PCR result in 5 patients (HSV in 1, VZV in 2, and CMV in 2), whereas extraocular symptoms were evident in 8 patients. The diagnoses were reached following the development of ocular lesions such as iris atrophy in 15 patients.
Six patients (29%) were diagnosed as complete-type Behçet’s disease, whereas 15 patients (71%) were incomplete-type Behçet’s disease. HLA-B27-associated uveitis was found in 5 patients. AS was evident in 1 patient, while 1 patient suffered IBD. The rest of the patients (n=26) were AAU of unknown origin and categorized in the undefined group.
Table 2 shows the most common and second most common uveitides in a given age range, respectively. In the age range of 0–19 years, Juvenile chronic iridocyclitis was the most common disease that accounted for some 36%, whereas VKH disease was tied with retinal vasculitis (14% each). In the age range of 20–39 years, Behçet’s disease was diagnosed in 18% of the patients, whereas VKH disease accounted for another 14%. In the age range of 40–59 and ≥60 years, sarcoidosis was the most common disease that accounted for 17% and 20%, respectively. The second most common disease in the age range of 40–59 years was VKH disease, while that in the age range of ≥60 years was herpetic iritis. TOP4 appeared either as the most common disease or as the second most common disease in each age range.
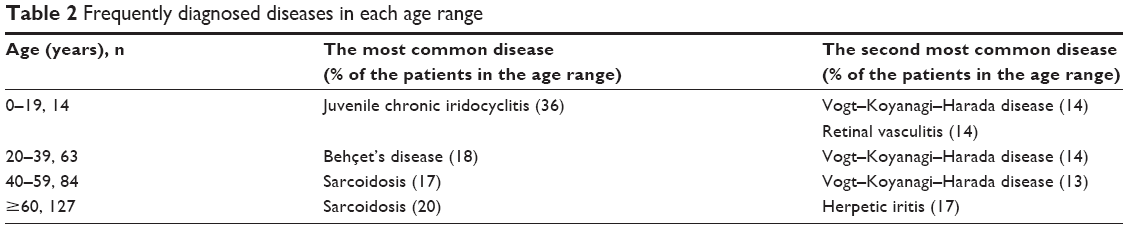 | Table 2 Frequently diagnosed diseases in each age range |
Figure 2 shows the percentages of TOP4 of our report in each age range. The patients with sarcoidosis accounted for 17% in the age range of 40–59 years, whereas 20% in the age range of ≥60 years was diagnosed as sarcoidosis. Behçet’s disease accounted for 17% in the age range of 20–39 years and 7% in the age range of 40–59 years. VKH disease accounted for 14% in the age range of 0–19 and 20–39 years, whereas 13% in the age range of 40–59 years, respectively.
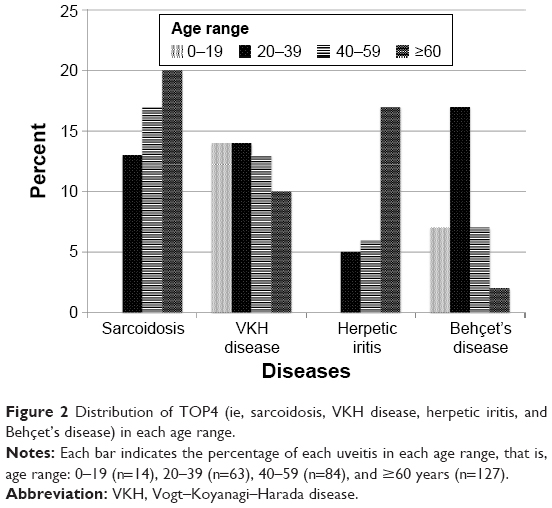 | Figure 2 Distribution of TOP4 (ie, sarcoidosis, VKH disease, herpetic iritis, and Behçet’s disease) in each age range. |
Table 3 shows the frequencies of TOP4 as percentages and order in the reports from other facilities.5,7,9,10–14 Several reports from Japan, as well as from other parts of Asia, and from Europe and North America are shown. Our current data concerning TOP4 showed similar results to other reports from Japan. Sarcoidosis was diagnosed prevalently in many areas except for Korea and North America. VKH disease and Behçet’s disease were not encountered frequently in Europe and North America. Herpetic iritis was also diagnosed more frequently in Saudi Arabia, Europe, and North America.
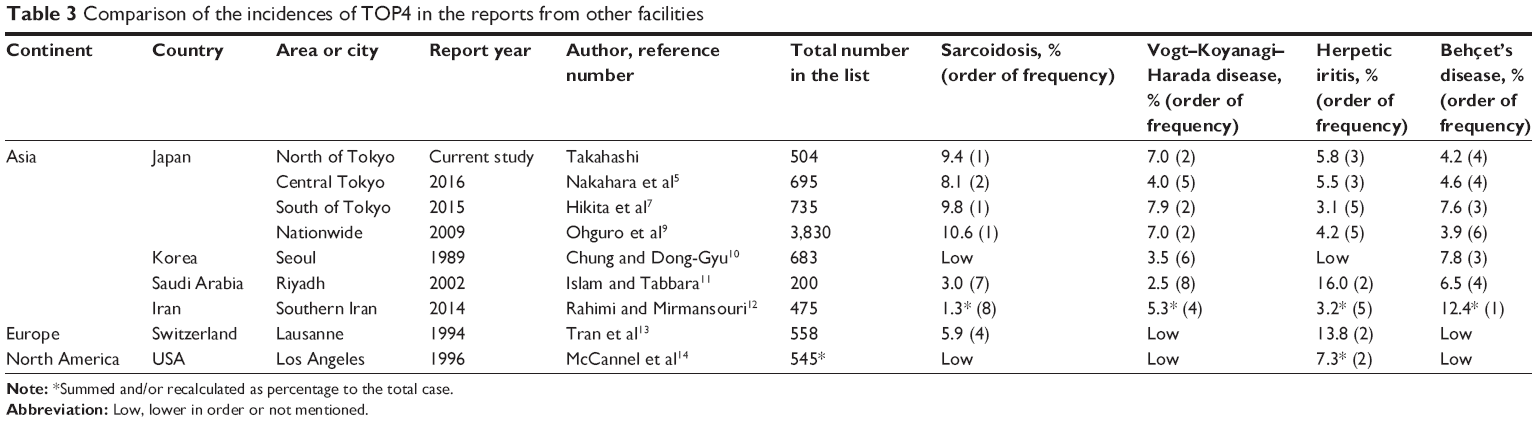 | Table 3 Comparison of the incidences of TOP4 in the reports from other facilities |
Discussion
Uveitis, or intraocular inflammation, consists of a variety of diseases that may threaten vision. Especially when etiology of uveitis remains undefined, patients’ visual prognoses might be challenged. Information concerning the patterns of etiologies in a given area during a certain period of time is one of the essential keys to help doctors treat patients with uveitis properly and efficiently. Since our institute is a tertiary, referral-based university hospital in the area north of Tokyo, Japan, there is an imminent need to know the current trends of these referred patients.
In the present study, we retrospectively examined newly arrived patients with uveitis who visited Jichi Medical University Hospital, between April 2011 and March 2015. The number of patients, either male or female, was fewer among those ≤30 years of age (Figure 1). As there is no general population-based survey of uveitis of any kind, exact reasons for this dissociation cannot be investigated. Yet, it may be either that the real frequency of uveitis patients in the younger generation is actually smaller or that those patients simply do not visit hospitals. The ratio of the definite diagnoses reached in the current study was 52.2% (Table 1), comparable to other reports.1–14 Our data showed similar trends to those of the nation-wide survey in Japan, 2009.9
Almost half of the patients with sarcoidosis received histologic examination in our study. This rate is comparable to other reports.6 Sarcoidosis is one of the most prevalent, thus, important uveitis in Japan. The number of the patients with herpetic iritis was also notable and this disease should be considered as important as the traditional top 3 uveitides in Japan. According to a report from another institute, 21.4% of the patients were clinically diagnosed without PCR assays.4 Nevertheless, a wide usage of PCR assay is beneficial for clinicians to obtain definite diagnoses of many infectious diseases. Fewer patients were diagnosed as complete-type Behçet’s disease. Forty-eight percent of the patients were diagnosed as complete-type in 1980,23 whereas only 29% were complete-type in our study. The tendency of fewer patients of Behçet’s disease for both whole patients and complete-type patients may be one of the current trends in Japan.
In the nation-wide survey in Japan, 2009,9 approximately one third of the patients with AAU were HLA-B27-positive, another one third were negative, and the remaining one third did not receive HLA testing. HLA-B27 was not found frequently among AAU patients. We found 5 patients with HLA-B27-associated AAU and the rest (26 patients) were AAU without unknown systemic diseases.
Table 2 and Figure 2 show additional interesting aspects. In each age range, at least one uveitis was listed as the most or second most common uveitides from the traditional top 3 uveitides in Japan (ie, sarcoidosis, VKH disease, and Behçet’s disease),1–9 and from TOP4, in each age range (Table 2). According to the distribution of TOP4 in each age range (Figure 2), sarcoidosis was found more frequently in older age ranges than in younger age ranges. At the same time, VKH disease was diagnosed almost equally in each age range. Herpetic iritis was more prevalent in older age ranges. The patients with Behçet’s disease were more frequently found in the age range of 20–39 years. Previously, the mean age of ocular onset in the patients in 1980s was reported as 34.5 years, while that of 1990s was 32.1.23
Table 3 shows distinct differences in the incidences of TOP4 in the reports from other institutes.5,7,9,10–14 Similarities in the reports from Japan were expected and noted.1–9 Sarcoidosis was reported to be prevalent in many areas except for Korea and North America.1–14 VKH disease and Behçet’s disease were not encountered frequently in Europe or in North America.13,14 More than 10% of the patients in Iran were found with Behçet’s disease.12 Herpetic iritis was not encountered in Korea,10 whereas it was more prevalent in Saudi Arabia,11 Europe,13 and North America.14 Clearly, these etiologic patterns were quite distinct in various countries in the world. At this point, we can acknowledge the importance of conducting etiology investigations of uveitis patients such as ours.
Conclusion
The present results revealed that the most frequent types of uveitis in Jichi Medical University Hospital, Tochigi north of Tokyo, Japan, during the 4-year period (2011–2015) were sarcoidosis, followed by VKH disease, herpetic iritis, and Behçet’s disease. Herpetic iritis was as frequently diagnosed as Japan’s traditional top 3 uveitides. Overall, the incidences of various uveitides were quite similar to that of the nationwide survey in Japan, 2009.9 We believe that conducting periodic surveys such as ours will provide us with essential and useful knowledge for obtaining the correct diagnoses of uveitis and proper medical modalities.
Acknowledgment
The authors thank Ms Katsue Aramaki for her secretarial assistance throughout the study.
Disclosure
The authors report no conflicts of interest in this work.
References
Akiyama K, Numaga J, Yoshida A, Kawashima H, Kaburaki T, Fujino Y. Statistical analysis of endogenous uveitis at Tokyo University Hospital (1998–2000). Jpn J Ophthalmol. 2006;50(1):69–71. | ||
Tamashima J, Kaburaki T, Takamoto M, et al. Review of endogenous uveitis at the University of Tokyo Hospital (2004–2006). Rinsho Ganka (Jpn J Clin Ophthalmol). 2010;64:85–90. Japanese. | ||
Kawashima H, Fujishiro T, Obata R, Mayama C, Ishii K, Kojima T. Statistical analyses of ocular inflammatory diseases at Saitama Red Cross Hospital (2003–2007). Jpn J Ophthalmol. 2010;54(1):96–97. | ||
Nakahara H, Kaburaki T, Takamoto M, et al. Statistical analyses of Endogenous Uveitis patients (2007–2009) in central Tokyo area and comparison with previous studies (1963–2006). Ocul Immunol Inflamm. 2014;25:1–6. | ||
Nakahara H, Kaburaki T, Tanaka R, et al. Frequency of uveitis in the central Tokyo area (2010–2012). Ocul Immunol Inflamm. 2016:1–7. | ||
Miyanaga M, Takase H, Kawaguchi T, et al. Clinical Survey of Uveitis in Tokyo Medical and Dental University – Comparison between the periods of 1998–2001 and 2007–2011. Nippon Ganka Gakkai Zasshi. 2015;119(10):678–685. | ||
Hikita S, Sonoda KH, Hijioka E, et al. Incidence of uveitis in the northern Kyushu region of Japan – comparison between the periods of 1996–2001 and 2003–2008. Nippon Ganka Gakkai Zasshi. 2012;116(9):847–855. | ||
Goto H, Mochizuki M, Yamaki K, Kotake S, Usui M, Ohno S. Epidemiological survey of intraocular inflammation in Japan. Jpn J Ophthalmol. 2007;51(1):41–44. | ||
Ohguro N, Sonoda KH, Takeuchi M, Matsumura M, Mochizuki M. The 2009 prospective multi-center epidemiologic survey of uveitis in Japan. Jpn J Ophthalmol. 2012;56(5):432–435. | ||
Chung H, Dong-Gyu C. Clinical analysis of uveitis. Kor J Ophthalmol. 1989;3:33–37. | ||
Islam SM, Tabbara KF. Causes of uveitis at The Eye Center in Saudi Arabia: a retrospective review. Ophthalmic Epidemiol. 2002;9(4):239–249. | ||
Rahimi M, Mirmansouri G. Patterns of Uveitis at a Tertiary Referral Center in Southern Iran. J Ophthalmic Vis Res. 2014;9(1):54–59. | ||
Tran VT, Auer C, Guex-Crosier Y, Pittet N, Herbort CP. Epidemiology of uveitis in Switzerland. Ocul Immunol Inflamm. 1994;2(3):169–176. | ||
McCannel CA, Holland GN, Helm CJ, Cornell PJ, Winston JV, Rimmer TG. Causes of uveitis in the general practice of ophthalmology. Am J Ophthalmol. 1996;121(1):35–46. | ||
Kawaguchi T, Hanada A, Horie S, Sugamoto Y, Sugita S, Mochizuki M. Evaluation of characteristic ocular signs and systemic investigations in ocular sarcoidosis patients. Jpn J Ophthalmol. 2007;51(2):121–126. | ||
Read RW, Holland GN, Rao NA, et al. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: report of an International Committee on Nomenclature. Am J Ophthalmol. 2001;131(5):647–652. | ||
Suzuki Kurokawa M, Suzuki N. Behçet’s disease. Clin Exp Med. 2004;4(1):10–20. | ||
Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. | ||
Trusko B, Thorne J, Jabs D, et al. The standardization of uveitis nomenclature (SUN) project. Development of a clinical evidence base utilizing informatics tools and techniques. Methods Inf Med. 2013;52(3):259–265. | ||
Ogawa M, Sugita S, Shimizu N, Watanabe K, Nakagawa I, Mochizuki M. Broad-range real-time PCR assay for detection of bacterial DNA in ocular samples from infectious endophthalmitis. Jpn J Ophthalmol. 2012;56(6):529–535. | ||
Ogawa M, Sugita S, Watanabe K, Shimizu N, Mochizuki M. Novel diagnosis of fungal endophthalmitis by broad-range real-time PCR detection of fungal 28S ribosomal DNA. Graefes Arch Clin Exp Ophthalmol. 2012;250(12):1877–1883. | ||
Generali E, Cantarini L, Selmi C. Ocular involvement in systemic autoimmune diseases. Clin Rev Allergy Immunol. 2015;49(3):263–270. | ||
Yoshida A, Kawashima H, Motoyama Y, et al. Comparison of patients with Behçet’s disease in the 1980s and 1990s. Ophthalmol. 2004;111(4):810–815. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.