")
Back to Journals » International Journal of General Medicine » Volume 15
Utilization of Risk Scores for Coronary Heart Disease Diagnosis in Rural China
Authors Liao H, Chen Q, Liu L, Zhong S, Xiao C
Received 23 December 2021
Accepted for publication 17 February 2022
Published 5 March 2022 Volume 2022:15 Pages 2541—2548
DOI https://doi.org/10.2147/IJGM.S355573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Huocheng Liao, Qiuyue Chen, Lin Liu, Sigan Zhong, Chun Xiao
Department of Cardiology, The Third People’s Hospital of Huizhou and the Affiliated Hospital of Guangzhou Medical University, Huizhou City, Guangdong Province, People’s Republic of China
Correspondence: Chun Xiao, Department of Cardiology, The Third People Hospital of Huizhou, The Affiliated Hospital of Guangzhou Medical University, Huizhou City, Guangdong Province, People’s Republic of China, Email [email protected]
Objective: The current study was to design a cardiovascular risk score for the diagnosis of coronary heart disease (CHD) in the rural area of China and the sensitivity and specificity of this score would be assessed.
Methods: A total of 520 patients were enrolled and based on the results from coronary artery angiography, patients were divided into three groups: CHD group (coronary artery ≥ 50% stenosis), atherosclerosis group (coronary artery < 50% stenosis) and normal groups (without stenosis). Between-group differences were evaluated and the sensitivity and specificity of cardiovascular risk score were evaluated.
Results: Compared to the normal and atherosclerosis groups, patients in the CHD group were older, had higher body mass index, and more likely to be smoking and obese, and had dyslipidemia, hypertension and diabetes, and had higher cardiovascular risk score (4.05 ± 2.15 vs 2.94 ± 1.90 vs 2.54 ± 1.59). Patients in the CHD group were more likely to have cardiovascular risk scores ≥ 2 (90.2% CHD group vs 74.2% atherosclerosis group vs 76.1% normal group, P < 0.05). The area under the ROC was 0.673, with 95% confidence interval was 0.623– 0.722 (P < 0.001), and the sensitivity and specificity were highest when the cardiovascular risk score was 4, indicating that the value of cardiovascular risk score of 4 was a good cutoff point for CHD diagnosis.
Conclusion: Using cardiovascular risk score can improve CHD diagnosis which may help to reduce health disparities between rural and urban area.
Keywords: coronary heart disease, cardiovascular risk score, sensitivity, specificity
Introduction
Coronary heart disease (CHD) is a leading cause of morbidity and mortality in the developed countries.1–3 In the past decades, with increasing prevalence and incidence of hypertension, diabetes, dyslipidemia, as well as endemic of sedentary lifestyle and smoking,4–6 the prevalence and incidence of CHD in China is increased dramatically.7,8 Due to the profound differences in economic development between the urban and rural areas of China, the health resources, diagnostic equipment and therapeutic approaches for CHD are quite different, which result in significantly poorer prognosis and higher mortality rates of CHD in patients of rural area than urban area.9–11
Notably, besides typical clinical symptoms, electrocardiogram (ECG), sensitive cardiac biomarkers such as high-sensitivity cardiac troponin-I (Hs-CTnI), cardiac computed tomography (CT) and angiography are the important avenues for increasing the diagnostic accuracy of CHD.12–14 However, in rural areas of China, other than ECG, the commonly used sensitive diagnostic approaches are not always readily available which lead to delayed diagnosis and missed the timing for reperfusion of occluded coronary artery with fibrinolysis or percutaneous coronary intervention.
Huizhou, a city located in the southeast part of China, is a relatively well-developed urban city, which is surrounded by many rural areas wherein health resources are scarce. In order to improve the managements of suspected CHD patients in the local rural areas of Huizhou city, the Huizhou Institute of Health initiates a program in order to help improve the diagnosis of CHD in these rural areas, and as one of the leading cardiovascular centers in Huizhou, we designed a cardiovascular risk score for CHD diagnosis and then to evaluate the sensitivity and specificity of this score for CHD diagnosis. Our results indicate that this score has a good predictive value for CHD diagnosis in Huizhou rural area. Hopefully, this score derived from our study can be further corroborated in other population groups which in turn can improve prognosis of CHD patients in the rural area.
Methods
Participants’ Enrollment
The current study was approved by the Clinical Research Ethic Committee of the Third People’s Hospital of Huizhou. Informed consent was obtained before participant’s enrollment. All the performances were conducted in accordance with the Declaration of Helsinki. Current study was conducted between January of 2017 to December of 2017. The inclusion criteria were: patients with suspected CHD and underwent coronary angiography; the exclusion criteria were: missed data of clinical risk factors; could not finish ECG, echocardiography or carotid artery ultrasound examination; documented acute heart failure or acute myocardial infarction; or had end stage liver, renal, lung disease or malignancy. A total of 520 patients were enrolled and based on the results from coronary artery angiography, patients were divided into three groups: CHD group (coronary artery ≥50% stenosis), atherosclerosis group (coronary artery <50% stenosis) and normal groups (without stenosis).
Data Collection
The factors including into the cardiovascular risk scores were as follows: 1) presence of any of these risk factors (male ≥45 years old or female ≥55 years old; hypertension or with antihypertensive treatment; dyslipidemia or with statins treatment; smoking; body mass index ≥28 kg/m2, or male waist circumference >90 cm and female waist circumference >85 cm; diabetes or with anti-diabetic treatment or abnormal fasting or postprandial blood glucose level); 2) ECG changes (no ST-T abnormality; ST-T depression and/or T wave flat or inversion); 3) echocardiography change (normal wall motion or focal or diffuse wall motion abnormality); 4) carotid artery ultrasound (normal; carotid intima-media thickness [CIMT] >1.0 cm; presence of carotid plaque; carotid stenosis <50% or ≥50%); 5) clinical symptoms (chest pain, dyspnea, short of breath or palpitation; duration of symptoms; activity related; relieved by rest or nitroglycerin); 6) coronary angiography (coronary artery ≥50% stenosis, <50% stenosis or without stenosis). Based on the presence of these factors, a score from 0 to 4 was signed into each individual variable (Table 1).
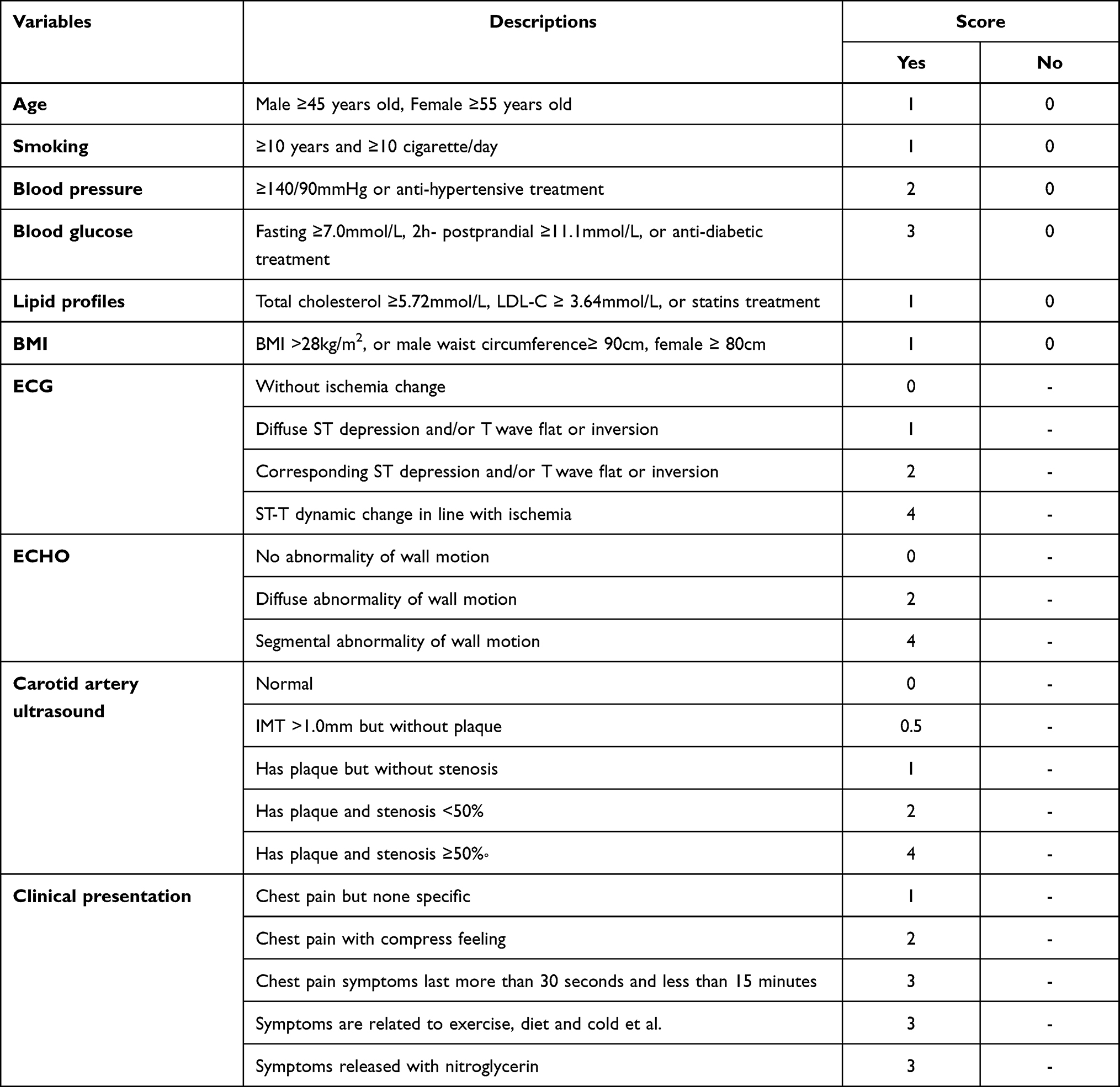 |
Table 1 Variables of Cardiovascular Risk Score |
Statistical Analysis
We used statistical software SPSS24.0 to perform statistical analysis. Using the chi-square test for comparison of categorical variables and analysis of variance for continuous variables. Coronary artery angiography was used as the standard diagnostic criteria and the cardiovascular risk score was compared with the angiography to evaluate the accuracy of the score. The point allocation to each variable was based on the coefficient of the logistic regression analysis which was described previously. In specific, in the first step, univariate regression analysis was performed and factors with P-value <0.1 were entered into multivariable regression models. In the second step, factors independently associated with CHD were selected. In addition, factors which were clinically important were also selected although without statistical significance. In the third step, based on the value of the coefficient, a score from 0 to 4 was assigned.
The receiver operating curve (ROC) was constructed to evaluate the performance of this score for CHD diagnosis; and the sensitivity and specificity of different scores for diagnosing CHD were calculated. P < 0.05 was considered as statistically significant;
Results
Baseline Characteristics Comparisons
As presented in Table 2, compared to the normal and atherosclerosis groups, patients in the CHD group were older (63.8 ± 11.2 vs 61.8 ± 11.7 vs 58.3 ± 12.9 years old), had higher BMI (26.5 ± 5.8 vs 25.8 ± 5.7 vs 25.3 ± 5.2 kg/m2), and more likely to be smoking (58.1% vs 29.9% vs 44.4%) and obese (30.6% vs 17.5% vs 11.1%), and had dyslipidemia (30.6% vs 17.5% vs 11.1%), hypertension (60% vs 48.5% vs 31.7%) and diabetes (30.3% vs 14.4% vs 12.7%), and had higher cardiovascular risk score (4.05 ± 2.15 vs 2.94 ± 1.90 vs 2.54 ± 1.59). In addition, compared to the normal group, patients in the atherosclerosis group were also older, and more likely to be obese, and had dyslipidemia and hypertension and had higher cardiovascular risk score, but less likely to be male and smoking.
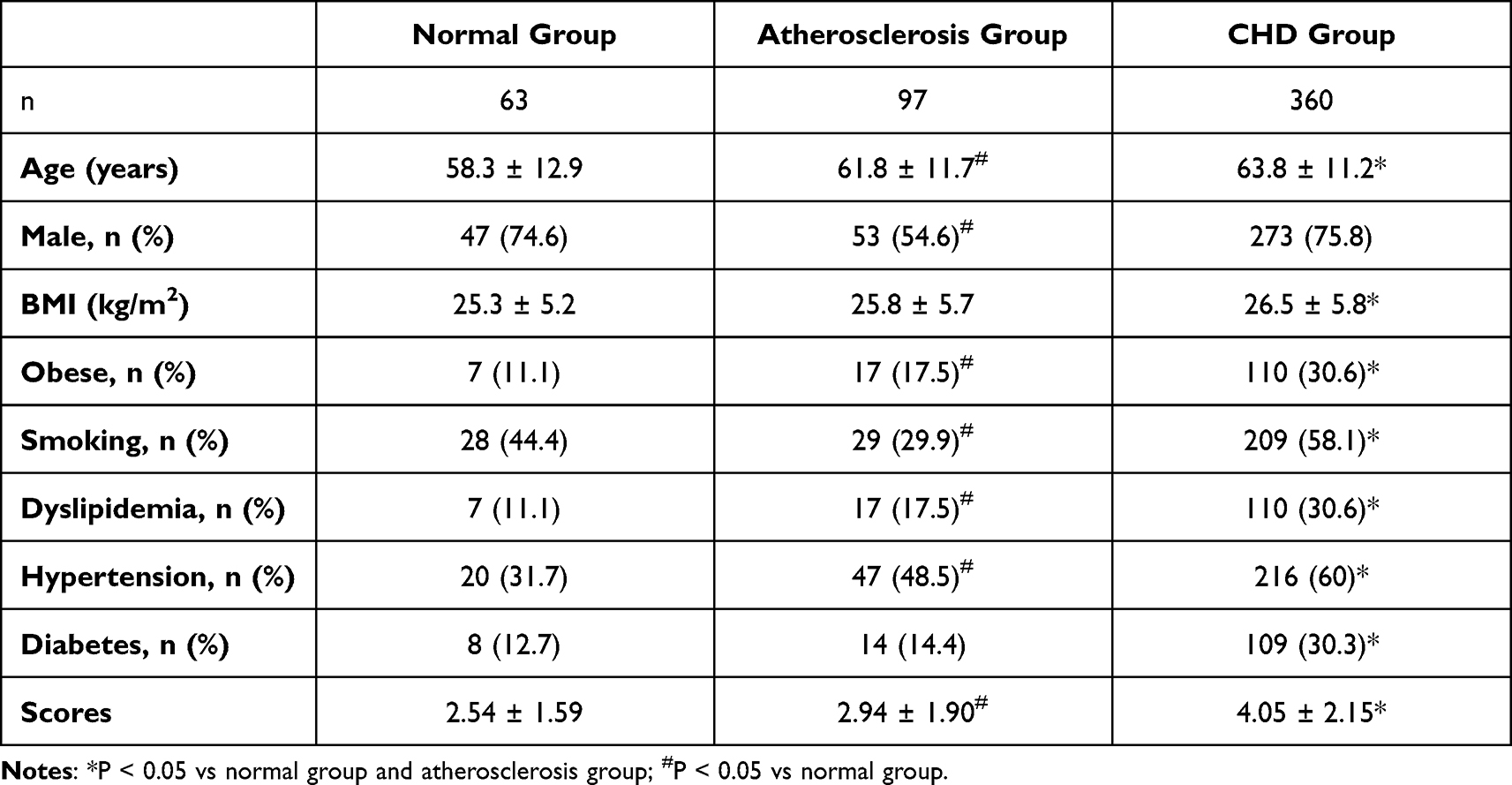 |
Table 2 Baseline Characteristics and Cardiovascular Risk Score Comparisons |
Distribution of Cardiovascular Risk Scores Among Three Groups
As presented in Table 3, compared to the normal and atherosclerosis groups, patients in the CHD group were more likely to have cardiovascular risk scores ≥2 (90.2% CHD group vs 74.2% atherosclerosis group vs 76.1% normal group, P < 0.05) and no significant differences in atherosclerosis group and normal group was observed in patients with cardiovascular risk scores ≥2. However, compared to patients in the normal group, patients in the atherosclerosis group were more likely to have cardiovascular risk scores ≥3 (58.7% vs 42.9%, P < 0.05).
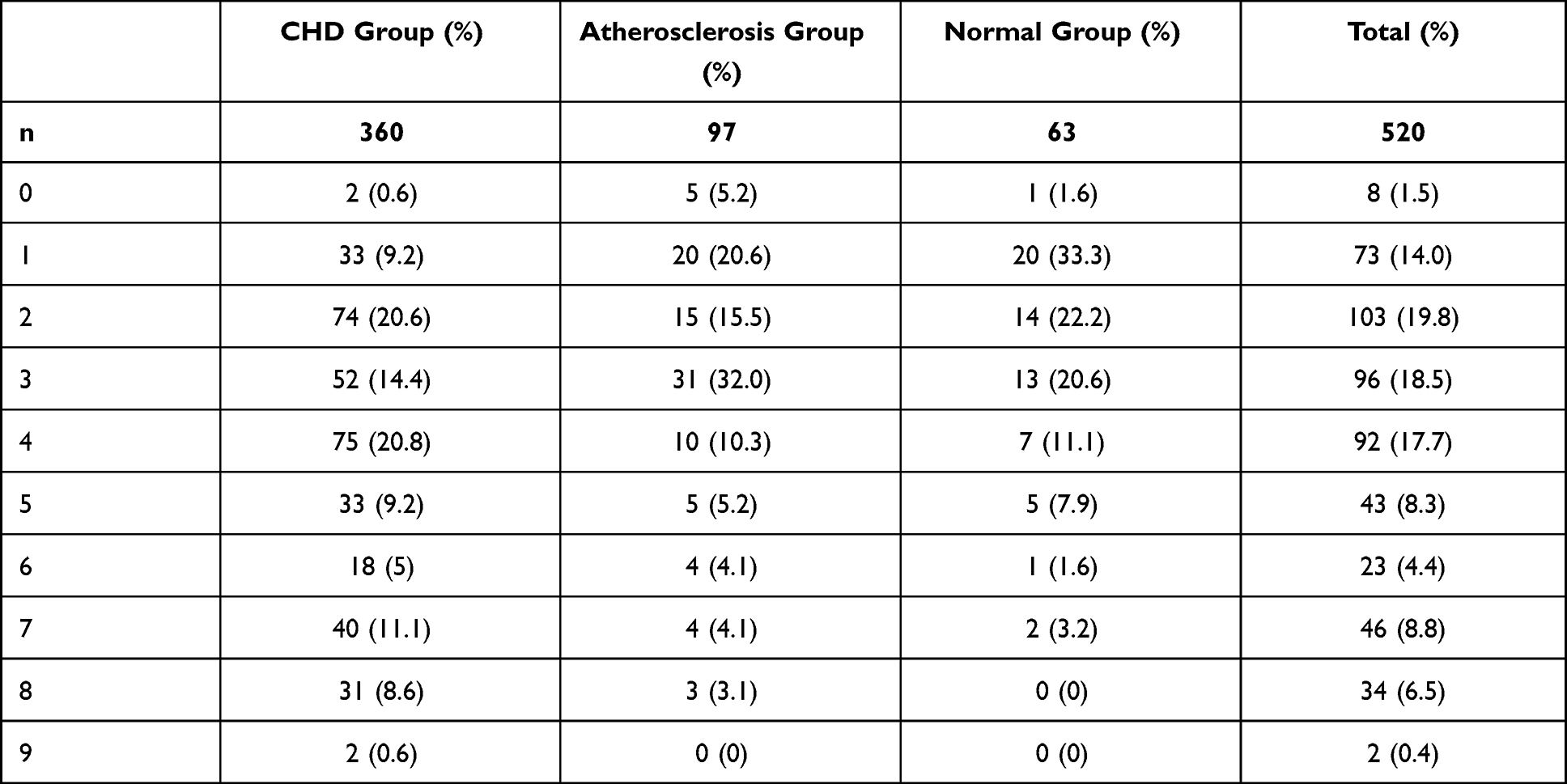 |
Table 3 Distribution of Cardiovascular Risk Scores Among Three Groups |
Sensitivity and Specificity of Cardiovascular Risk Score to Predict CHD
Using coronary angiography as standard diagnostic criteria, the sensitivity and specificity of cardiovascular risk score were evaluated by the ROC. As presented in Figure 1, the area under the ROC was 0.673, with 95% confidence interval was 0.623–0.722 (P < 0.001), and as presented in Table 4, the sensitivity and specificity was highest when the cardiovascular risk score was 4, indicating that the value of cardiovascular risk score of 4 was a good cutoff point for CHD diagnosis.
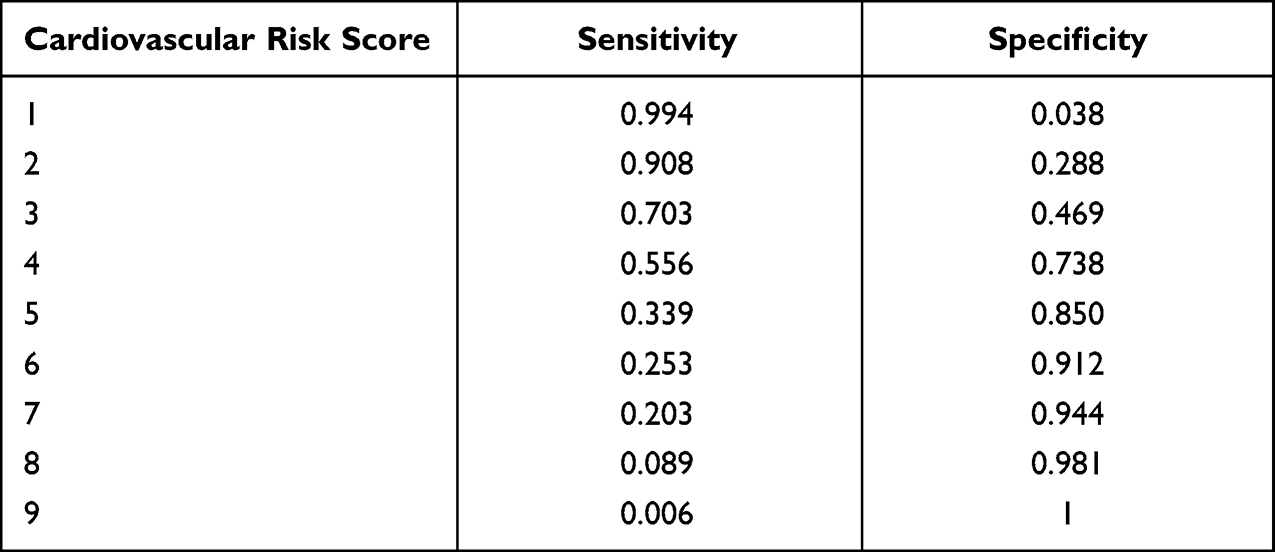 |
Table 4 Sensitivity and Specificity of Cardiovascular Risk Score for CHD Diagnosis |
 |
Figure 1 Performance of risk score. The area under the ROC was 0.673, with 95% confidence interval was 0.623–0.722 (P < 0.001). |
Discussion
To our knowledge, our current study for the first time shows that in the rural area of China, cardiovascular risk scores, which include parameters of clinical symptoms, comorbidities, ECG, echocardiography and carotid artery ultrasound, can be used to diagnose CHD. When compared to coronary artery angiography, cardiovascular risk scores of four have the best sensitivity and specificity for CHD diagnosis. Further studies of other geographic areas and population groups should be conducted to corroborate our findings.
Major and profound growth of economy have occurred in China in the past decades. Unfortunately, the risk factors (eg, diabetes) and unhealthy lifestyle (eg, smoking) also concurrently increase,15,16 which result in dramatic increase in atherosclerotic cardiovascular disease.17,18 In the last decade, the treatment of CHD has improved in China especially in the urban area.8 However, national survey indicates that the diagnosis and treatment of CHD in the rural area are still poor and the underlying mechanisms are multifactorial and can be attributed to the lacking of health resources such as coronary artery computed tomography and coronary angiography.19,20 For example, Yan et al19 conducted an epidemiological study recruiting participants from high-, medium- and low-income regions of China, and their study indicates that there was an inverse trend between risk-factor burden and cardiovascular disease prevalence in urban and rural communities. They concluded that such asymmetry might be attributed to the interregional differences in residents’ awareness, quality of healthcare, and availability and affordability of medical services. Wan et al21 conducted a study to evaluate the mortality trend of ischemic heart disease (IDH) in China from 1991 to 2009. They reported that in rural areas, the mortality rate with annual percentage change increasing from 3.52% in 1991–2000 to 9.02% in 2000–2009, which was much higher than in urban areas (1.05%). These results collectively indicate that it is a priority to improve the management of CHD in the rural areas of China otherwise the health and economic expenditure could not be reduced despite improvement of CHD prognosis has been achieved in urban area of China.
As a cardiovascular health improvement initiative of Huizhou City, our center conducted a pilot study to evaluate whether combining traditional risk factors can improve CHD diagnosis in rural area of Huizhou. Our study demonstrated that when combining risk factors, ECG change and clinical symptoms, the diagnostic sensitivity and specificity of cardiovascular risk score could be as high as 55.6% and 73.8%, respectively. These findings have several significant clinical implications, especially in rural area of China. First of all, our results stress the importance of collecting basic clinical information in terms of the features of patients’ clinical symptoms and ECG. Second, using cardiovascular risk score can help physicians to evaluate a suspected CHD in a comprehensive and integrated pattern. Third, with a high specificity, our current cardiovascular risk score can help local physician to better rule out CHD which result in reduced unnecessary economic expenditure. Last but not the least, our study indicates that despite less well developed than urban area, the prevalence of cardiovascular risk factors and comorbidities remained high in these rural areas. Further studies are needed to evaluate the underlying mechanisms so as to improve the overall health for the people in these rural areas.
Notably, ECG remains an irreplaceable tool in the management of the patients with CHD. Among these ECG parameters, ST-segment change has been commonly used to identify CHD. Nevertheless, in recent decades, accumulative evidence has suggested that other than ST-segment change, other parameters such as QTc and Tp-e can also be used to screen and identify the possibility of CHD22. In the current study, we only used the ST-segment change which has also shown a good predictive value. However, it is clinically relevant to evaluate whether other ECG parameters can improve CHD diagnosis in the absence of ST-segment change in the future.
The impacts of this risk score in daily clinical practice can be depicted in three aspects. First, in rural areas where health resources and specialists are limited, using this risk score can help improve the diagnosis of CHD. Second, this risk score can help to rule out those with unlikely to have CHD, which in turn can avoid unnecessary further examination and expenditure. Third, this risk score can facilitate general practitioner to screen those with suspected CHD and determine whether prevention therapy is needed.
Strength and Limitation
The strength of current study is that this should be the first study to use the easily available parameters to construct the risk score for predicting CHD in rural China. In addition, several parameters with detailed information were recorded, which help to improve the discriminative performance of the risk score. There are also some limitations of our current study needed to be addressed. First, since current study was conducted only in Huizhou area and findings from our study may not be extrapolated to other areas. However, our study provides insight into the usefulness of cardiovascular risk score for CHD diagnosis in areas without advanced diagnostic instrument (eg, cardiac CT). Second, since this was a cross-sectional study and we do not know whether using this cardiovascular risk score can improve patients’ long-term outcome or not. Further studies are needed to answer this question. Third, we only recorded ST change and other ECG parameters (QTc and Tp-e) were unavailable. Further studies are needed to collect these parameters and to evaluate whether adding these parameters would improve the predictive value. Lastly, in the cardiovascular risk score, we have only included several traditional risk factors and whether including cardiac biomarker such as Hs-CTnI or cardiac kinase-MB can further improve the diagnostic accuracy deserves evaluation in the future.
Conclusion
In conclusion, our study for the first time shows that using cardiovascular risk score can improve CHD diagnosis in rural area of China which may help to reduce health disparities between rural and urban area. Future studies are warranted whether this score can improve patients’ outcome.
Abbreviation
CHD, Coronary heart disease; ECG, Electrocardiogram; Hs-CTnI, High-sensitivity cardiac troponin-I; CT, Computer tomography; CIMT, Carotid intima-media thickness.
Funding
Current study was supported by the Technology Project of Huizhou City (20190401).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):e240–327. doi:10.1161/CIR.0b013e31829e8776
2. Bonneux L, Barendregt JJ, Meeter K, Bonsel GJ, van der Maas PJ. Estimating clinical morbidity due to ischemic heart disease and congestive heart failure: the future rise of heart failure. Am J Public Health. 1994;84(1):20–28. doi:10.2105/AJPH.84.1.20
3. Jankowski P, Czarnecka D, Badacz L, et al. Practice setting and secondary prevention of coronary artery disease. Arch Med Sci. 2018;14(5):979–987. doi:10.5114/aoms.2017.65236
4. Liang Y, Liu R, Du S, Qiu C. Trends in incidence of hypertension in Chinese adults, 1991-2009: the China Health and Nutrition Survey. Int J Cardiol. 2014;175(1):96–101. doi:10.1016/j.ijcard.2014.04.258
5. Wang F, Ye P, Hu D, et al. Lipid-lowering therapy and lipid goal attainment in patients with metabolic syndrome in China: subgroup analysis of the Dyslipidemia International Study-China (DYSIS-China). Atherosclerosis. 2014;237(1):99–105. doi:10.1016/j.atherosclerosis.2014.08.023
6. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
7. Xie W, Li G, Zhao D, et al. Relationship between fine particulate air pollution and ischaemic heart disease morbidity and mortality. Heart. 2015;101(4):257–263. doi:10.1136/heartjnl-2014-306165
8. Li J, Li X, Wang Q, et al. ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): a retrospective analysis of Hospital data. Lancet. 2015;385(9966):441–451. doi:10.1016/S0140-6736(14)60921-1
9. Wu H, Lau ES, Kong AP, et al. Association between educational level and cardiovascular disease and all-cause mortality in patients with type 2 diabetes: a prospective study in the Joint Asia Diabetes Evaluation Program. Clin Epidemiol. 2018;10:1561–1571. doi:10.2147/CLEP.S177437
10. Zhang N. Trends in urban/rural inequalities in cardiovascular risk bio-markers among Chinese adolescents in two decades of urbanisation: 1991-2011. Int J Equity Health. 2018;17(1):101. doi:10.1186/s12939-018-0813-1
11. Zhao Q, Yang Y, Chen Z, Yu H, Xu H. Changes in characteristics, risk factors, and in-hospital mortality among patients with acute myocardial infarction in the capital of China over 40 years. Int J Cardiol. 2018;265:30–34. doi:10.1016/j.ijcard.2018.04.134
12. Driessen RS, Danad I, Stuijfzand WJ, et al. Comparison of coronary computed tomography angiography, fractional flow reserve, and perfusion imaging for ischemia diagnosis. J Am Coll Cardiol. 2019;73(2):161–173. doi:10.1016/j.jacc.2018.10.056
13. Januzzi JL, Suchindran S, Coles A, et al. High-Sensitivity Troponin I and Coronary Computed Tomography in Symptomatic Outpatients With Suspected Coronary Artery Disease: insights From the PROMISE Trial. JACC Cardiovasc Imaging. 2018;1:24.
14. Lubbers M, Coenen A, Kofflard M, et al. Comprehensive Cardiac CT With Myocardial Perfusion Imaging Versus Functional Testing in Suspected Coronary Artery Disease: the Multicenter, Randomized CRESCENT-II Trial. JACC Cardiovasc Imaging. 2018;11(11):1625–1636. doi:10.1016/j.jcmg.2017.10.010
15. Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA. 2015;314(10):1021–1029. doi:10.1001/jama.2015.10029
16. Zhang M, Liu S, Yang L, et al. Prevalence of smoking and knowledge about the smoking hazards among 170,000 Chinese adults: a nationally representative survey in 2013-2014. Nicotine Tob Res. 2019;21(12):1644–1651. doi:10.1093/ntr/ntz020
17. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013;381(9882):1987–2015. doi:10.1016/S0140-6736(13)61097-1
18. Downing NS, Li J. Ischaemic heart disease in China: the time to address rising mortality rates. Eur Heart J Qual Care Clin Outcomes. 2017;3(1):4–5. doi:10.1093/ehjqcco/qcw049
19. Yan R, Li W, Yin L, Wang Y, Cardiovascular Diseases BJ. and Risk-factor burden in urban and rural communities in high-, middle-, and low-income regions of China: a large community-based epidemiological study. J Am Heart Assoc. 2017;6:2. doi:10.1161/JAHA.116.004445
20. Chen WW, Gao RL, Liu LS, et al. China cardiovascular diseases report 2015: a summary. J Geriatr Cardiol. 2017;14(1):1–10. doi:10.11909/j.issn.1671-5411.2017.01.012
21. Wan X, Ren H, Ma E, Yang G. Mortality trends for ischemic heart disease in China: an analysis of 102 continuous disease surveillance points from 1991 to 2009. BMC Public Health. 2017;18(1):52. doi:10.1186/s12889-017-4558-3
22. Hayıroğlu M, Lakhani I, Tse G, Çınar T, Çinier G, Tekkeşin A. In-hospital prognostic value of electrocardiographic parameters other than ST-segment changes in acute myocardial infarction: literature review and future perspectives. Heart Lung Circ. 2020;29(11):1603–1612. doi:10.1016/j.hlc.2020.04.011
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.