")
Back to Journals » Open Access Journal of Contraception » Volume 11
Utilization of Maternity Services and Its Relationship with Postpartum Use of Modern Contraceptives Among Women of Reproductive Age Group in Nigeria
Received 9 August 2019
Accepted for publication 21 November 2019
Published 6 January 2020 Volume 2020:11 Pages 1—13
DOI https://doi.org/10.2147/OAJC.S215619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Innocent Anayochukwu Ugwu,1 Imose Itua2
1Department of Obstetrics & Gynecology, College of Medicine, Enugu State University of Science & Technology (ESUT) and ESUT Teaching Hospital, Enugu, Nigeria; 2Department of Public Health and Healthcare Management, University of Liverpool/Laureate Online Education, Liverpool, UK
Correspondence: Innocent Anayochukwu Ugwu
Department of Obstetrics & Gynecology, College of Medicine, Enugu State University of Science & Technology (ESUT) and ESUT Teaching Hospital, Parklane, Enugu, Nigeria
Tel +234 8034749789
Email [email protected]
Background: Utilization of maternity services (UMS) exposes mothers to family planning (FP) counseling and other FP promotional activities. Uptake of postpartum modern contraceptives (PPMC) reduces both infant and maternal mortalities by reducing unwanted pregnancies and promoting good child spacing. Understanding the relationship between UMS and uptake of PPMC was therefore very important.
Purpose: To determine the association between UMS and uptake of PPMC among women of the reproductive age group in Nigeria taking into consideration the influence of the place of access to the maternity services.
Patients and Methods: This study was a descriptive epidemiological study design. Secondary data obtained from the 2013 Nigerian Demographic Health Survey (NDHS) was analyzed to achieve the above aim. The uptake of PPMC was the dependent variable (DV). The independent variables (IDV) selected were the number of antenatal care (ANC) visits, place of access of ANC, place of delivery, timing of postnatal care (PNC) and place of access of PNC. Other control variables include socio-demographic factors. Descriptive statistics, chi-square testing, and logistic regression analyses were conducted to determine the association between the PPMC uptake and the IDV/other control variables. Statistical significance was claimed at p<0.05.
Results: Utilization of maternity services was associated with higher uptake of PPMC among the women (>/= 4 ANC visits OR = 2.08, 95% CI=1.65–2.62, P<0.001; public facility delivery OR= 1.80, 95% CI= 1.54–2.10, P< 0.001; private facility delivery OR =1.54, 95% CI 1.28–1.85, P< 0.001; PNC OR=1.21, 95% CI= 1.02–1.43, P=0.029). Accessing postnatal care in private health facilities was associated with increased uptake of PPMC (OR= 1.46, 95% CI =1.05–2.02, P= 0.024). The number of children alive, educational attainment, wealth index and having information about FP remained significant predictors of PPMC uptake.
Conclusion: The utilization of maternity services was positively associated with postpartum use of modern contraceptives among women of reproductive age in Nigeria. There was increased uptake of PPMC among women who utilized maternity service compared to their counterparts who did not. Regarding the place of access, accessing antenatal care as well as delivering in either private or public health facilities was not a significant predictor of PPMC use. However, accessing postnatal care in private facilities was associated with higher uptake of PPMC.
Keywords: maternity services, postpartum contraception, family planning, Nigeria
Introduction
Family planning (FP) offers people the opportunity to space their pregnancies and have their preferred number of children and this is accomplished through the utilization of various methods of contraception.1 Control of fertility through effective contraceptive use offers social and health benefits to individuals, the families as well as society.2 It prevents pregnancy-associated health problems, reduces abortions, unintended/unwanted pregnancies, and infants’ death, slows rapid growth in population, improves women’s economic and social status and enables their full participation in the society.3
Postpartum contraception/FP is the commencement of the use of contraceptives within 12 months after childbirth.4 The use of contraception during the period after delivery has since been demonstrated as a vital element of reproductive health care (RHC).5 Health care workers through their contact with mothers during pregnancy and delivery have been noted as an important information source on postpartum contraceptive use.6
Justification for the need for postpartum contraceptive uptake is that increased use of modern FP methods in the period after delivery reduces both infant and maternal mortalities by reducing unwanted pregnancies and by promoting adequate child spacing in between births.7 It has been noted that women are more inspired to prevent pregnancies and most “receptive to” the discussions on contraception during pregnancy and after childbirth – thus they are more likely to adopt a contraceptive method postpartum.8
Theoretical reasons exist to anticipate an association between maternity and “child health” (MCH) services utilization and uptake of contraception.9 First, utilization of maternity services (UMS) exposes mothers to family planning (FP) counseling and other FP promotional activities. Second, integration of MCH with FP services as is often done in the majority of settings may decrease the time-associated cost of uptake of contraception.9
Making FP services and information more available increases the acceptability and the desirability of the use of contraceptives by the members of a community, thereby stimulating further uptake of contraception.10 It has been shown that use of contraception by women is really shaped by the presence and accessibility of family planning services as well as by the perceived service quality.11 Investigators have also shown that after controlling for women’s household and individual characteristics, increased uptake of postpartum contraception is related to the availability of a close-by public health care center and the quality of contraceptive services rendered in that community.12
Health care services including FP services could be delivered through private and public providers. Public health care service is typically delivered by governments through their national health systems. The private health care is delivered via private practitioners and “for profit” institutions/hospitals and other nongovernmental nonprofit providers including the “faith-based” institutions.13 Where a woman access maternity services (public or private health facility) is likely to have an impact on subsequent use of contraceptives.
Nigeria remains Africa’s most populous nation with a population of 177,155,754 and contraceptive prevalence rate (CPR) of 14% in 2014.14 This is low when compared with the worldwide CPR of 63.3% in 2010.15 However, Adeyemi et al revealed an unmet need for contraception as high as 59.4% at 10 months after delivery in Nigeria.16 The result of this high level of unmet need for contraception and low prevalence for modern contraceptive methods after the delivery period include increased rate of unintended and/or unwanted pregnancies, abortions, short interval between pregnancies and resultant high child (128/1000 live births) and maternal (576/100,000 live birth) mortalities.17 These pregnancy-associated complications and mortalities constitute massive “public health” challenges to stakeholders and policymakers at every level in Nigeria.18
Studies have shown that there is a positive relationship between the utilization of maternity services and subsequent uptake of modern contraceptives.5,9,19,20 Despite this body of evidence, in Nigeria, most studies are local ones that investigated contraceptive use among young people, adolescents, and undergraduates and women in general. Only one, using the 2008 NDHS data examined the postpartum modern contraceptive (PPMC) determinants and use in the contexts of contacts of women with other reproductive health care delivery system5 but none examined the influence of place of access (government or private) of the maternity services on the uptake of PPMC. This study, therefore, aimed to determine whether there is an association between utilization of maternity services and postpartum use of modern contraceptives among women of reproductive age between 2009 and 2013 in Nigeria taking into consideration the influence of the place of access of the maternity services in the country.
Materials and Methods
Study Design
This was a descriptive epidemiological study that involved the analysis of secondary data from the 2013 Nigerian Demographic Health Survey (NDHS).
Study Setting
Nigeria remains the most populous country in the African continent with a population of 177,155,754.14 Presently Nigeria is geopolitically grouped into six zones with a total of thirty-six states, 774 local government areas (LGA) and a Federal Capital Territory.
Sample Size
This study involved secondary analyses of an already existing set of data from the 2013 NDHS in which a study sample of 38,948 women aged 15–49 years were interviewed all over the country. A total of 13,066 data was analyzed after applying the exclusion and inclusion criteria.
Inclusion and Exclusion Criteria
All women within the age group 15–49 who had at least one delivery within the past 5 years were included. Women whose most recent birth did not fall within 5 years prior to the survey were excluded from the sample (use of contraception after most recent birth was considered, and this must be between 2009 −2013). Also, all the women who delivered less than 12 months prior to the date of the 2013 NDHS were also excluded – so as to make sure that all women analyzed completed a one-year post-delivery period.
Ethics
The data for this study were made readily available by request from the ICF macro USA and the details of the proposed use of the data made known to them. Permission was granted for use of the data. Also, data were in aggregated form, the initial participants were not individually recognizable or identifiable in any form. Therefore, the issue of anonymity, confidentiality, and informed consent never arose.
Data Source
The source of data for this study was the women’s questionnaire of the 2013 NDHS. It provided recent information on health indicators including family planning as well as other demographic characteristics of women of reproductive age group 15–49 years. It also provided information on health indicators for Federal Capital Territory (FCT), the thirty-six states, the six geopolitical divisions of the country as well as national estimates. The 2013 NDHS sample was a national representative sample that covered the whole population living in residential units in Nigeria. The sampling frame of the survey was the enumeration area (EA) list which was put together during the 2006 national population census. The sample for the survey was obtained using a stratified three-stage cluster design. Stratification was done by splitting every state in the country into rural and urban areas.
Postpartum modern contraceptive (PPMC) use was the dependent variable (DV). This was defined as the use of any of the following modern contraceptives from at least 12 months after the last delivery.5 The methods included sterilization (female or male), intrauterine device (IUD), injectables, implants, pills, condoms, female condoms, diaphragm, and foam/Jelly. The independent variables (IDV) selected that depict utilization of maternity services included; the number of antenatal care (ANC) visits, place of access of ANC, place of delivery, timing of postnatal care (PNC) and place of access of PNC.
Other control variables selected based on the literature review findings and on the factors associated with utilization of contraception were; age group of mother at last delivery, educational status of the woman, wealth index, place of residence (urban or rural), region of residence, marital status, religion, exposure to FP information in health facility, and number of children alive.
Data Analysis
A set of data (13,066) which was needed to address the research question of this study was extracted from the above-mentioned source after applying the inclusion and exclusion criteria. Statistical analysis was done using Statistical Package for Social Science (SPSS) version 21. There was some missing data for ANC, PNC, and place of delivery. For this analysis, only those respondents with responses for the variables of interest were included in cross-tabulation (chi-square test) and in logistic regression. Hence, all cases with missing data were excluded using a complete case analysis method.21 Also in order to address the “differences in the probability of selection” and produce appropriate representation; weighting was applied in the tabulation. The “weight cases” option in SPSS was selected for all the cross-tabulations and logistic regression analyses.
Descriptive analysis was used to present the socio-demographic characteristics (SDC) of the participants. Frequency tables were used to show the percentages of SDC, the percentage utilization of the selected maternity services as well as the percentage uptake of postpartum modern contraceptive. Furthermore, the Chi-square test was used to test for the association between the selected independent variables indicating maternity services utilization (ANC, place of delivery, PNC, place of access of the maternity services) and the dependent (outcome) variable (uptake of PPMC).
Finally, the relationship existing between the dependent and the independent variables as well as other socio-demographic variables was tested using multiple logistic regression (MLR) models to address confounders. The MLR analysis was applied in situations where there existed a single variable with dichotomous outcomes (use or no use of PPMC) and greater than one independent or control variables.22 It permitted the estimation of the odds ratio “for a putative factor” independent of the influence of confounders and other existing explanatory variables.23 Statistical significance was claimed at p<0.05 for all the analyses.
Result
The final data of women aged 15–49 years analyzed were 13,066. Figure 1 depicted how the final data were obtained.
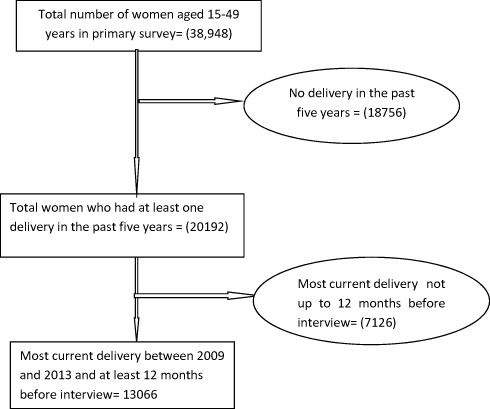 |
Figure 1 The flow chart showing the data selection procedure. |
Descriptive Statistics
Socio-Demographic Characteristics (SDC) of the Respondents
Table 1 shows the frequency distribution of the SDC of women. About two-thirds (63.4%) of the women were aged 20–34 years at the time of the last delivery. This was followed by those aged 35 years and above (32%). Women less than 20 years of age constituted (4.7%) of the respondents. Concerning the number of children alive, slightly above one-third of the women had 1–2 children (36.8%), while those that had 3–4 children alive were about 32.2%. There were more women from rural areas (66%), and a greater proportion of the participants was from the northwest part of the country. The majority of women (45.8%) had no formal education. Islam was the most commonly reported religion (56.8%) while the majority of the women were married (93.5%).
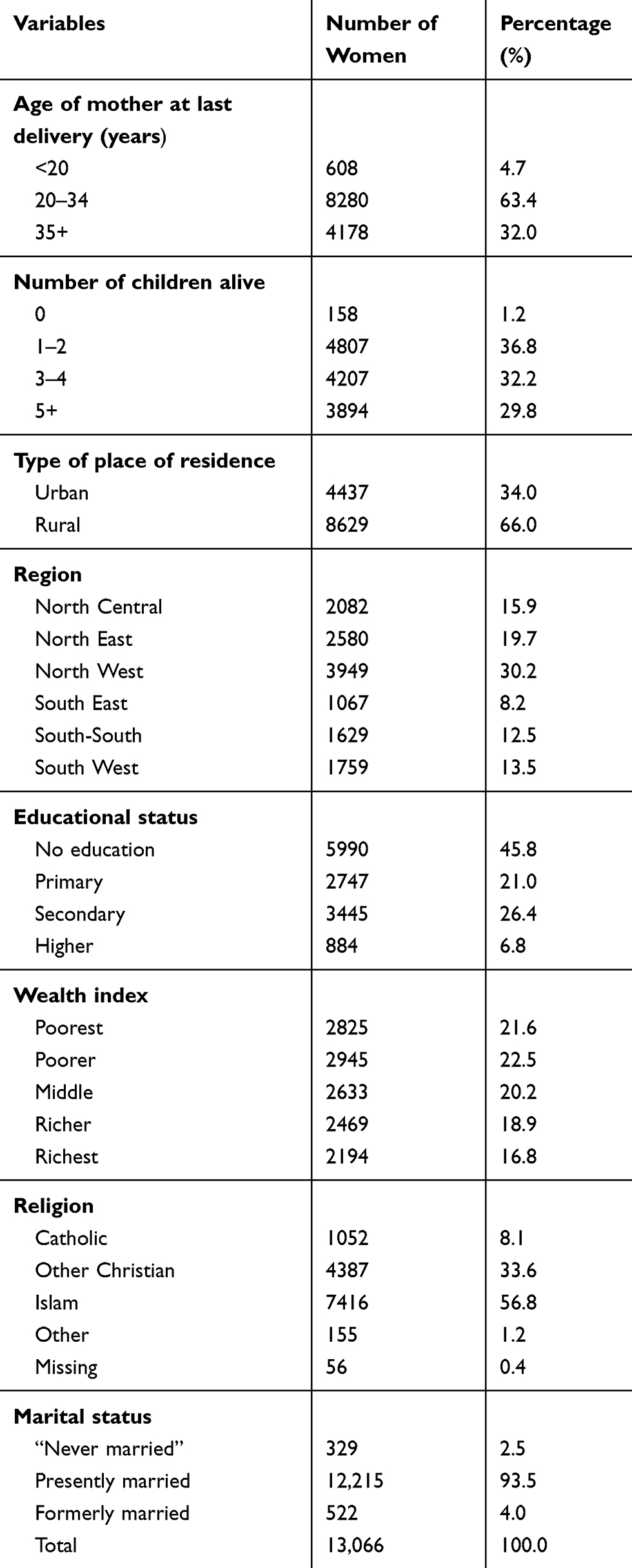 |
Table 1 Frequency Distribution of the Socio-Demographic Characteristics of Women in the Study |
Utilization and Place of Access of Maternity Services
Table 2 shows the frequency distribution of utilization of various maternity services and the place of access to the services. Percentages with and without missing data were presented but the latter reported as the result was not significantly affected by the missing data. The majority of the women (53.2%) attended more than four antenatal care (ANC) visits; however, slightly above one-third (35.4%) did not attend any ANC. Antenatal care was most commonly received in public/government facilities (50.4%) compared with private facilities (14.5%). Most women delivered at home (61.4%), however a higher proportion of the women delivered in public/government sector facilities (25.3%) compared to (13.3%) that delivered in private sector facilities. Similar proportions of women attended postnatal care (PNC) at day 2 or less (14.7%) and between 3 and 6 weeks (14.2%); however, the majority did not attend PNC (71.2%). Among those that attended PNC, a higher proportion of women accessed care in public sector facilities (19.0%) compared with private sector facilities (6.2%).
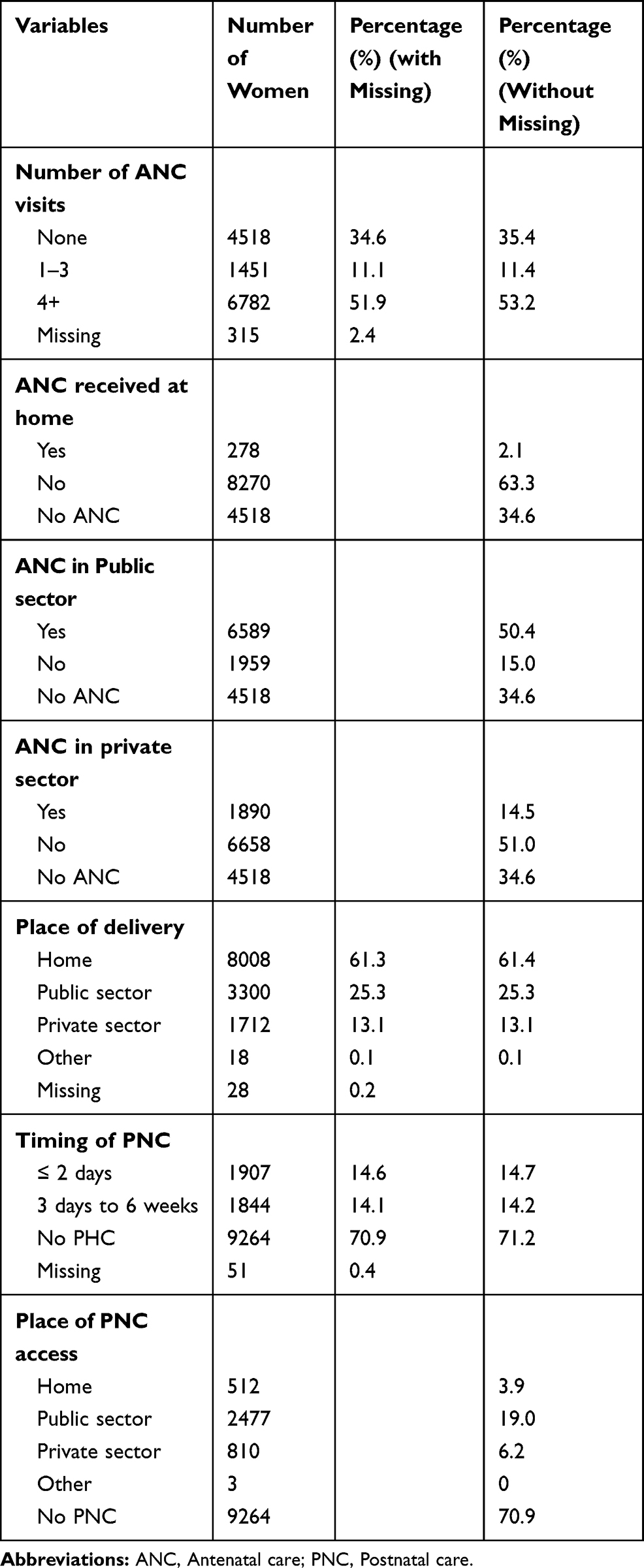 |
Table 2 Frequency Distribution of Utilization of Various Maternity Services (ANC, Place of Delivery, and PNC) and the Place of Access of the Services |
Prevalence of Postpartum Modern Contraceptive (PPMC) Use, Methods, and Information About Family Planning (FP)
A total of 1499 women used PPMC out of 13,066, giving a prevalence rate of 11.5%. The commonest PPMC/FP method used by the women was injectables (4.3%) followed by a condom (2.7%) and pills (2.6%). Diaphram was not used while the least used method was female sterilization. Concerning information about FP, only about one-tenth of the women (11.3%) were informed about FP in health facilities while a greater percentage of the women (88.3%) were not informed.
Bivariate Result
Relationship Between the Socio-Demographic Variables and PPMC Uptake Using the Chi-Square Test
The association between the socio-demographic variables and postpartum modern contraceptive (PPMC) uptake is presented in Table 3. The uptake of PPMC was significantly higher among the women of older age group (X2=58.34, P < 0.001) those that have higher number of children alive (X2 = 41.52, P <0.001) urban dwellers (X2= 474.30, P <0.001) and women from the Southwestern part of the nation (X2 1080.00, P < 0.001). Similarly, significantly higher proportion of women in the postpartum period reporting PPMC use was noted among those with higher education (X2= 1200.00, P <0.001) the richest in the society (X2=1158.30, P < 0.001) Christians (X2= 854.60, P < 0.001) those not married (X2 =78.08, P < 0.001) and women who were informed about family planning in health facilities (X2 522.50, P < 0.001). This infers that the higher use of PPMC by subgroups of those women in each category was not by chance.
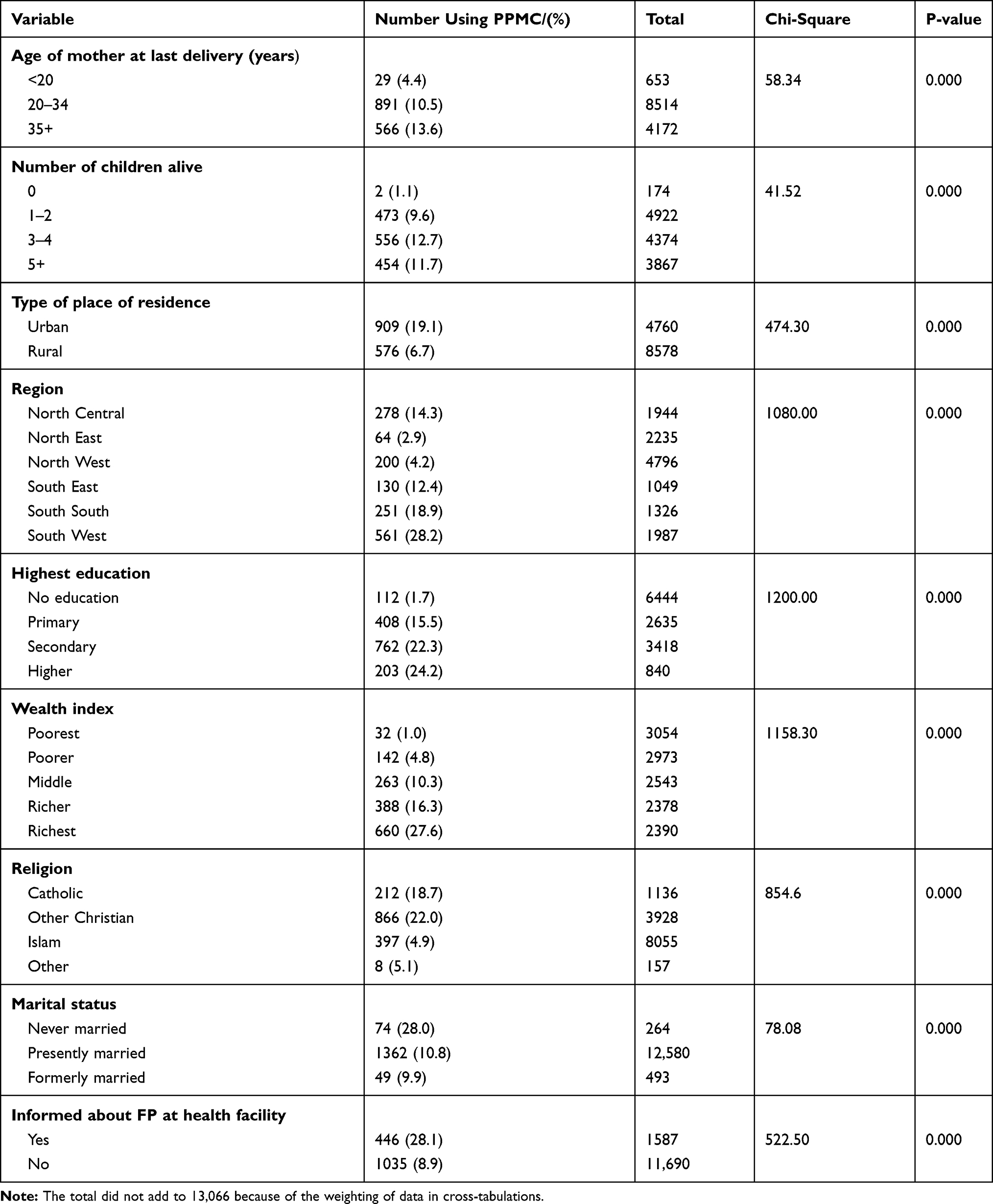 |
Table 3 Association Between the Socio-Demographic Variables and Post-Partum Modern Contraceptive (PPMC) Uptake |
The Relationship Between the Utilization of Maternity Services/Place of Access of Services and Postpartum Modern Contraceptive (PPMC) Use
Table 4 shows the relationship between utilization of maternity services/place of access to services and PPMC use. It was noted that the proportion of women using PPMC increases with an increase in the number of ANC visits. There was a higher use of PPMC among women who had 1–3 visits (6.5%) but the highest use of PPMC was noted among women who had 4 or greater than 4 visits (17.9%). Only 2.3% of women who had no ANC visit prior to their last delivery used PPMC. There was a significant association between the number of ANC visits and the use of PPMC (X2=734.5, P <0.001).
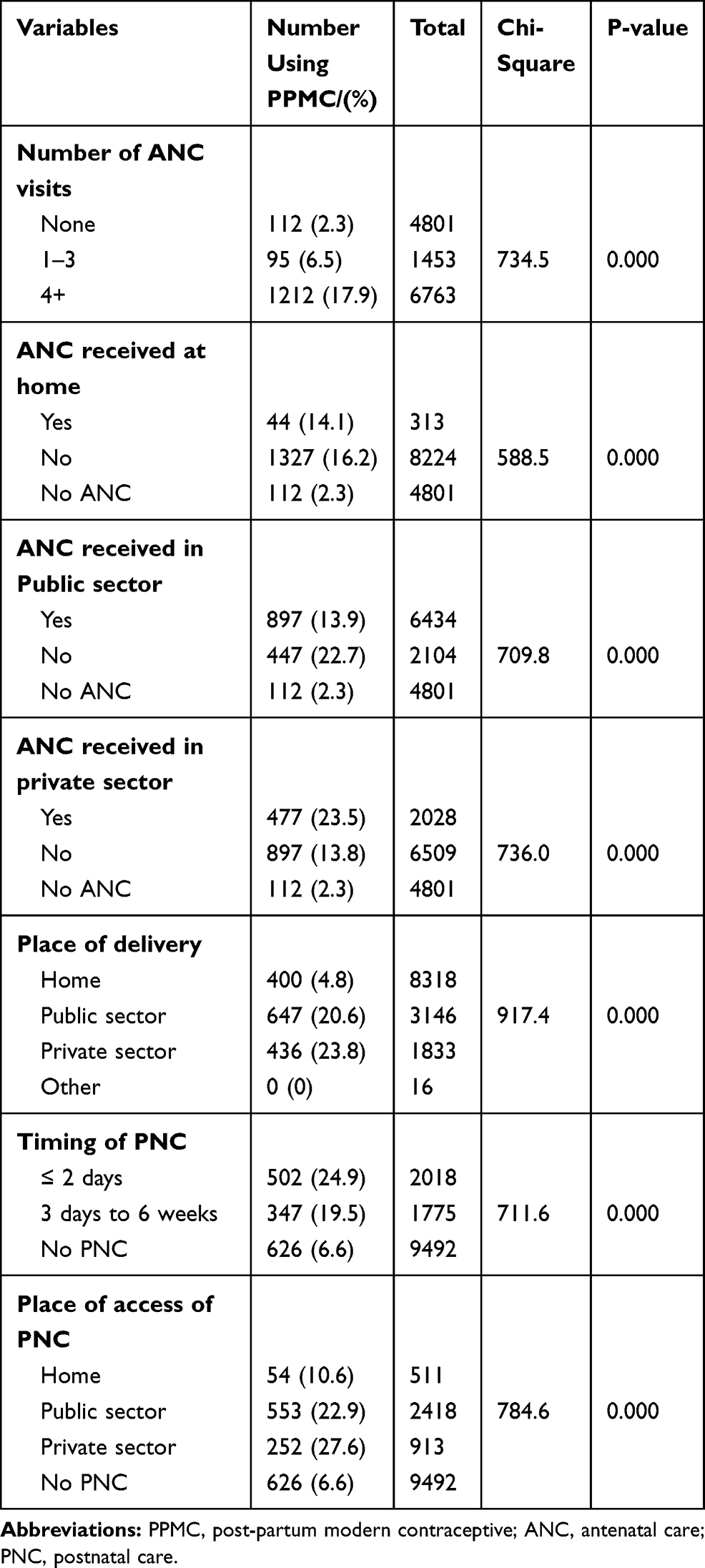 |
Table 4 Relationship Between the Utilization of Maternity Services/Place of Access of Services and PPMC Uptake |
Concerning the place of access of ANC, uptake of PPMC was significantly associated with access to ANC care in a health facility (private or public sector facility) (P<0.001). More women (23.5%) who accessed ANC in private facilities used PPMC compared to those who had care in public facilities (13.9%). The use of PPMC was significantly associated with health facility delivery (X2= 917.4, P< 0.001). Women who delivered in the private health facility had higher use of PPMC (23.8%) compared to those who delivered in a public health facility (20.6%).
The utilization and timing of PNC was also significantly associated with uptake of PPMC (X2= 711.6, P < 0.001). Only 6.6% of the women who did not attend PNC after the last childbirth used PPMC. More women (24.9%) who had their PNC within 48 hrs used PPMC compared to those who had their PNC visits between 3 days and 6 weeks post-delivery (19.5%).
Use of PPMC was also significantly associated with place of PNC access (X2= 784.6, P < 0.001) More women (27.6%) who accessed PNC in private health facilities used PPMC methods after their childbirth compared to those who accessed care in public health facilities (22.9%). Those who attended PNC in a health facility (Public or private) used modern family planning method compared to use by women who had no PNC (6.6%) and use by those who had PNC at home (10.6%).
Logistic Regression
Univariate logistic regression analysis (presented in prose) was done for PPMC use and each of the main independent variables to generate unadjusted odds ratios (OR) and 95% confidence intervals (CI). This was followed by multivariable logistic. All control variables were included in the model producing the adjusted odds ratio (Table 5).
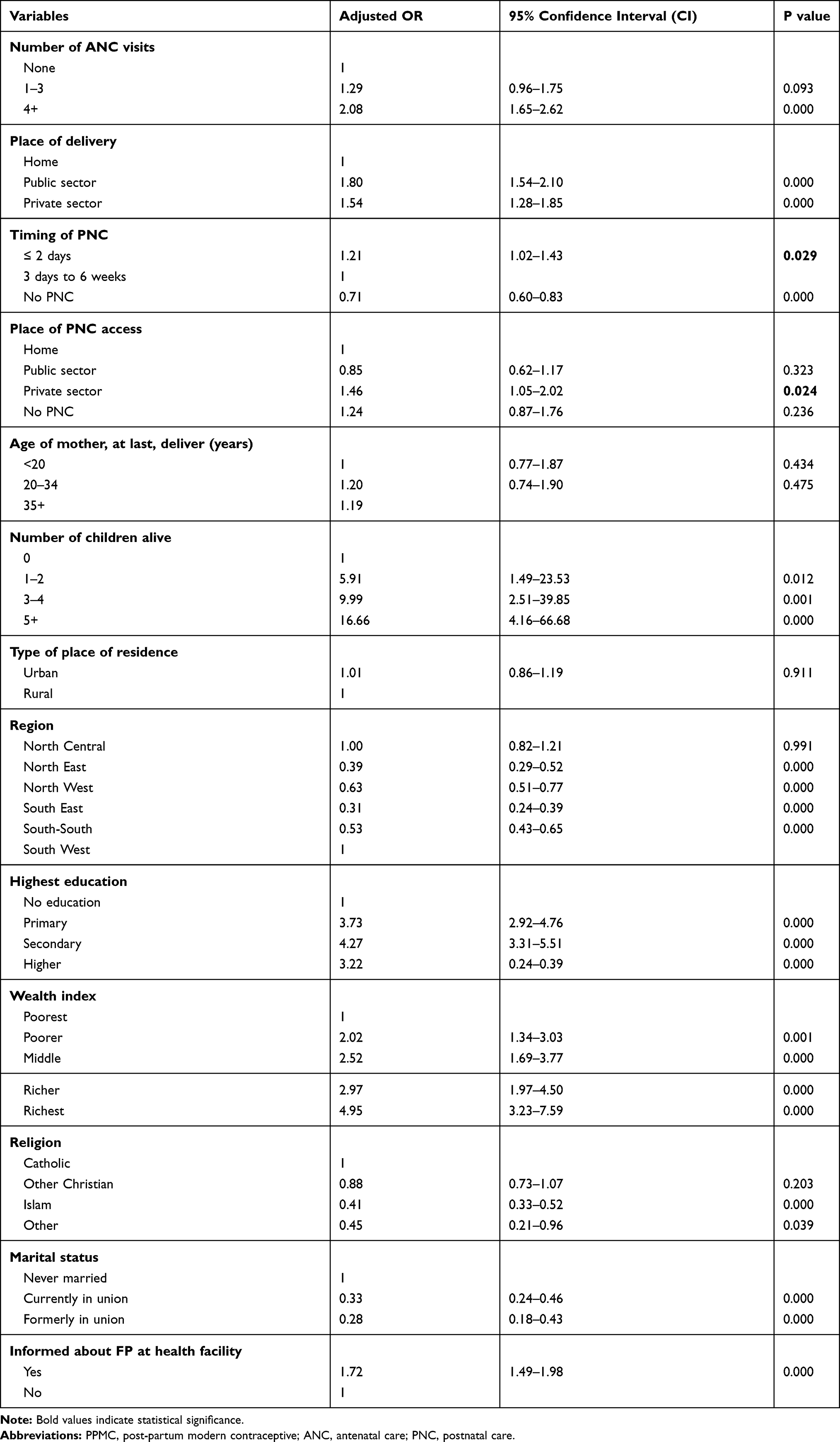 |
Table 5 The Odds of Use of Postpartum Modern Contraception (PPMC) by Number of ANC Visits, Place of Delivery, Timing of Postnatal Care (PNC) Visit, Place of Access of PNC Visit, and Other Control Variables |
Number of Antenatal Care Visits
The crude odds ratio from the regression of PPMC use on the number of ANC visits showed significant associations. The odds of using PPMC among women who had 1–3 visits was 2.94 (95% CI 2.22–3.89, P < 0.001) while the odds of use increased to 9.16 (95% CI 7.51–11.16, P <0.001) for women who had four or more ANC visits. This signified that women who had at least a visit and those that had four or more visits were 3 times and 9 times more likely to have used PPMC, respectively, when compared to women who did not attend ANC. However, after adjusting for the control variables (Table 5), only the comparison between 4 or more visits remained significant (OR = 2.08, 95% CI 1.65–2.62, P < 0.001).
Place of Delivery
The unadjusted OR of use of PPMC was statistically significant among women who delivered in public/government facilities (OR=5.13, 95% CI=4.49–5.85, P < 0.001) and private health facilities (OR= 6.18, 95% CI=5.34–7.16, P < 0.001) compared to home delivery. Delivering in public/private facility (institutional delivery) remained statistically significant after adjusting for other control variables (Table 5).
Timing of Postnatal Care
The use of PPMC was significantly higher among women accessing PNC within 2 days of childbirth (Unadjusted OR=1.36, 95% CI= 1.17–1.59, P < 0.001). This remained statistically significant after adjusting for other variables (OR= 1.21, 95% CI=1.02–1.43. P= 0.029). Note that significance was set at (P< 0.05). Use of PPMC is significantly lower in women who did not attend PNC (OR = 0.71, 95% CI= 0.60–0.83, P < 0.001).
Place of Access of Postnatal Care
The unadjusted OR for use of PPMC was statistically significant for accessing postnatal care (PNC) in public (OR=2.49, 95% CI-1.85–3.36, P < 0.001) as well as private (OR= 3.21, 95% CI 2.34–4.40. P< 0.001) health facilities. However, after adjusting for other variables, accessing PNC in private facility remained statistically significant (OR= 1.46, 95% CI =1.05–2.02, P= 0.024). Therefore, having postnatal care in the private health sector facility was an independent predictor of the use of postpartum modern contraceptives.
Other Variables
The number of children significantly predicted the use of postpartum modern contraceptive (PPMC). As the number of living children increased, the odds of use of contraception in the period after delivery also increased. Women who had 5 or more children were sixteen times more likely to have used postpartum modern contraception (OR= 16.66, 95% CI = 4.16–66.8, P <0.001) compared to the reference group who had no child alive. Similarly, education remained a significant predictor of PPMC use. Odd of use increased with an increase in educational attainment up to secondary education. Women who had secondary education were 4 times more likely to have used modern family planning (FP) method after delivery (OR = 4.27, 95% CI= 3.31–5.51, P < 0.001) compared to the women who had no education. The use of PPMC also increased with an increase in the wealth index. The richest women were 5 times more likely to have used PPMC (OR=4.95, 95% CI= 3.23–7.59, P < 0.001) compared to the reference group (poorest women). Finally, having information about FP in health facility significantly predicted use of PPMC (OR=1.72, 95% CI= 1.49–1.98, P < 0.001).
Discussion
Integrating contraceptive services with maternity and other reproductive health services (RHS) could be one of the approaches needed in order to expand access to contraceptive services and enable women to space or limit their number of children.24 In order to provide further evidence for integration, this analysis investigated the utilization of maternity services and its relationship with postpartum use of modern contraceptives among women of the reproductive age group in Nigeria. It also investigated the influence of place of access of these maternity services (private or public) on the uptake of the postpartum modern contraceptive (PPMC). The implications of the result were discussed under the following headings.
Utilization of Maternity Services and Postpartum Modern Contraceptive (PPMC) Use
The findings showed that utilization of maternity services (attending four or more ANC visits, health facility delivery, and timing of PNC) were significantly associated with increased uptake of PPMC among women of the reproductive age group in Nigeria. This significance remained after controlling for confounders. The findings were in keeping with the results of other related studies that found a significant positive relationship between the utilization of maternity services and the uptake of PPMC.5,19,20 Another important finding of this study was that having information about FP remained a significant predictor of PPMC uptake and there was more uptake of PPMC among women who had FP information. Other studies have also shown similar results.5,25,26 These findings have some vital policy implications apart from its theoretical significance. It suggests that the availability of contraceptive counseling during antenatal care (ANC) visits, delivery, and postnatal care visits provides women with more opportunity and knowledge to make an informed choice about contraception. Offering the contraceptive service during the PNC visit has an additional advantage of allowing women to have postnatal care and contraceptive services in the same visit thereby reducing both financial and time costs. This indicates that promoting and providing counseling on family planning during the ANC attendance may possibly enhance service quality as well as client satisfaction.
Contrary to the findings of the current study, Do and Hotchkiss noted that there was no significant relationship between postnatal care utilization and uptake of contraception during the postpartum period.19 Though the study was a secondary data analysis from the primary DHS survey, the difference in findings might be due to smaller sample sizes they used (3667 and 3587 participants in Zambia and Kenya, respectively) compared to 13,066 participants in this present study. Again, women analyzed in this study included those who had used any form of modern contraception from at least 12 months after last delivery compared to their study that analyzed women who had only 2 months.
Place of Access of Maternity Services and Postpartum Modern Contraceptive (PPMC) Use
The result of this study showed that accessing antenatal care as well as delivering in either private or public health facilities was not a significant predictor of PPMC use. However, it showed that accessing postnatal care in private facilities significantly predicted the use of PPMC. Women who accessed postnatal care in private facilities had a higher uptake of PPMC than those who accessed care in the public/government health facility, and this was still significant after addressing confounders. It is worth to note that contraception becomes an essential need during the postnatal care period and not during antenatal or delivery. This finding was in keeping with the findings of other similar studies in Nigeria where the private health facilities were noted as the commonest source of modern contraception during the postnatal period.27,28 The Nigerian government approved the delivery of free contraceptives in the public/government health facilities without much interest in the private sector.29 The policy implication of this finding is that there is a need for more recognition of the private health sector in the delivery of modern contraceptive methods. It has been noted that the collaboration of the government with the private health sectors in the delivery of contraceptive services would lead to decreased cost, improved affordability, and accessibility of contraceptives.30
Other Socio-Demographic Factors and PPMC Use
This study found that other significant independent predictors of postpartum modern contraceptive (PPMC) use include the number of children alive, educational attainment, and wealth index and having information about family planning. These findings are not new and are similar to the findings of other studies.19,31 The use of PPMC increased with an increase in educational attainment. Also, the wealthy women and those that heard about FP messages used PPMC more than other less privileged counterparts.
Study Strengths
The data for this study were from the Nigerian demographic health survey which used multistage probability sampling techniques in selecting clusters as well as households from a sampling frame that covered the Nigerian territory. Again, the large sample size used for this analysis, the high rate of response and participation, the standard method of collection of data as well as the trained interviewers used in primary survey ensured the reliability of the data and also showed that the estimates from the survey data truly represent national estimate. The span of the data collected (social, demographic, health, wealth, contraception, maternity services, fertility, etc.) allowed a deep analysis that went beyond counting prevalence but enabled the determination of a complex relationship between maternity services and uptake of contraception. Therefore, the result of this study truly reflects how maternity services relate to postpartum modern contraceptive use in the nation as a whole and can be generalized to populations that have the same characteristics as the population studied.
Again, during analysis, the weighting of data was applied to correct for the effect of non-proportional sample allocation to different states and their rural and urban areas and to correct the differences in the response rate in the different states. This also ensured representativeness. This research work has also added to the currently limited evidence on the relationship between utilization of maternity services and postpartum modern contraceptive uptake especially with respect to the influence of place of access of the services among women of the reproductive age group in Nigeria.
Study Limitations
Causality could not be determined as this was a secondary analysis of a primary survey. One of the limitations of survey data is that it measures associations but not very reliable in determining causality.32 The utilization of maternity in this study was significantly associated with the use of PPMC. However, it was impossible to make a conclusion of a cause–effect relationship.
Again, the place of PNC visit was not specifically asked in the DHS and was assumed to be the place where the last baby’s check was done. This may have introduced bias as the woman may have taken the baby for a checkup in other places apart from where she had ANC or where she delivered. However, a postnatal visit to the pediatricians provides another opportunity for mothers to have referrals for babies’ vaccination as well as other services which include family planning.33 Only the respondents with responses for the variables of interest were included in the cross-tabulations chi-square test and multiple logistic regression (MLR). Hence, all cases with missing data were excluded using the “complete cases analysis method”.21 Though an acceptable method during analysis, this method may lead to loss of power and bias and questions the reliability of the result obtained. However, bias often is very minimal when using this method most especially during MLR models.
Conclusion
Utilization of maternity services (ANC, health facility delivery and attending PNC) was positively associated with postpartum use of modern contraceptives among women of reproductive age in Nigeria. There was increased uptake of PPMC among women who utilized maternity service compared to their counterparts who did not. Accessing antenatal care as well as delivering in either private or public health facilities was not a significant predictor of PPMC use. However, accessing postnatal care in private facilities was associated with higher uptake of PPMC.
Acknowledgments
The authors wish to express their appreciation to the MEASURE DHS program and the ICF macro USA for granting access to 2013 Nigeria Demographic and Health Survey data.
Disclosure
The authors declare that they have no conflicts of interest. No funding was received for this research.
References
1. World Health Organization. Family planning/contraception fact sheet; 2015. Available from: http://www.who.int/mediacentre/factsheets/fs351/en/.
2. United Nations Population Funds. A new study shows the benefits of family planning to the well-being of women, families, and economies; 2013. Available from: http://www.unfpa.org/news/new-study-shows-benefits-family-planning-well-being-women-families-and-economies#sthash.URf5MTLF.dpuf.
3. World Health Organization. Maternal mortality ratio (per 100 000 live births); 2015. Available from: http://www.who.int/healthinfo/statistics/indmaternalmortality/en/.
4. World Health Organization. Programming strategies for postpartum family planning; 2013. Available from: http://apps.who.int/iris/bitstream/10665/93680/1/9789241506496_eng.pdf.
5. Akinlo A, Bisiriyu A, Esimai O. Use of maternal health care as a predictor of postpartum contraception in Nigeria. Afr Popul Stud. 2014;27(2):288. doi:10.11564/27-2-475.
6. Duong DV, Lee AH, Binns CW. Contraception within six-month postpartum in rural Vietnam: implications on family planning and maternity services. Eur J Contracept Reprod Health Care. 2005;10(2):111–118. doi:10.1080/13625180500131527
7. Vernon R. Meeting the family planning need of postpartum women. Stud Fam Plann. 2009;40(3):235–245. doi:10.1111/j.1728-4465.2009.00206.x
8. Cwiak C, Gellasch T, Zieman M. Peripartum contraceptive attitude and practices. Contraception. 2004;70:383–386. doi:10.1016/j.contraception.2004.05.010
9. Seiber EE, Hotchkiss DR, Rous JJ, Berruti AA. Maternal and child health and family planning service utilization in Guatemala: implications for service integration. Social Sci Med. 2005;61:279–291. doi:10.1016/j.socscimed.2004.11.068
10. Wang W, Alva S, Winter R, Burgert C. Contextual influences of modern contraceptive use among rural women in Rwanda and Nepal. DHS Analytical Studies No. 41. Calverton, Maryland, USA: ICF International. Available from: http://pdf.usaid.gov/pdf_docs/pnaec676.pdf.
11. Magnani RJ, Hotchkiss DR, Florence CS, Shafer LA. The impact of the family planning supply environment on contraceptive intentions and use in Morocco. Stud Fam Plann. 1999;30(2):120–132. doi:10.1111/sifp.1999.30.issue-2
12. Mensch B, Arends-Kuenning M, Jain A. The impact of the quality of family planning services on contraceptive use in Peru. Stud Fam Plann. 1996;27(2):59–75. doi:10.2307/2138134
13. Basu S, Andrews J, Kishore S, Panjabi R, Stuckler D. Comparative performance of private and public healthcare systems in low- and middle-income countries: a systematic review. PLoS Med. 2012;9(6):e1001244.
14. Central Intelligence Agency (CIA). The world factbook; 2015. Available from: http://www.theodora.com/wfbcurrent/nigeria/nigeria_people.html.
15. Alkema L, Kantorova MC, Biddlecom A. National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: a systematic and comprehensive analysis; 2013. Available from: http://www.healthynewbornnetwork.org/sites/default/files/resources/planning.pdf.
16. Adeyemi AB, Ijadunola KT, Orji EO, Kuti O, Alabi MM. The unmet need for contraception among Nigerian women in the first year post-partum. Eur J Contracept Reprod Health Care. 2005;10(4):229–234. doi:10.1080/13625180500279763.
17. National Population Commission (NPC). [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2014. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International; 2014.
18. USAID. Maternal and child health; 2015. Available from: https://www.usaid.gov/nigeria/global-health.
19. Do M, Hotchkiss D. Relationships between maternal health care and postpartum modern contraceptive use in Kenya and Zambia. Measure Evaluation PRH working paper series; 2011. Available from: http://www.cpc.unc.edu/measure/publications/wp-10-120.
20. Ahmed S, Mosley WH. Simultaneity in the use of maternal-child health care and contraceptives: evidence from developing countries. Demography. 2002;39(1):75–93. doi:10.1353/dem.2002.0001.
21. Graham JW. Missing data analysis: making it work in the real world. Annu Rev Psychol. 2009;60:549–576. doi:10.1146/annurev.psych.58.110405.085530
22. Multivariate Analysis. Multiple logistic regression analysis; 2015. Available from: http://sphweb.bumc.bu.edu/otlt/MPHModules/BS/BS704_Multivariable/BS704_Multivariable8.html.
23. Bruce N, Pope D, Stranistreet D, editors. Chapter 6. Case-control studies. In: Quantitative Research Methods for Health Research: A Practical Interactive Guide to Epidemiology and Statistics. Chichester, UK: J Wiley & Sons Ltd; 2008:297.
24. Kuhlmann AS, Gavin L, Galavotti C. The integration of family planning with other health services: a literature review. Int Perspect Sex Reprod Health. 2010;36(4):189–196. doi:10.1363/3618910
25. Adegbola O, Okunowo A. Intended postpartum contraceptive use among pregnant and puerperal women at a university teaching hospital. Arch Gynecol Obstet. 2009;280:987–992.:. doi:10.1007/s00404-009-1056-6
26. Adanikin AI, Onwudiegwu U, Loto OM. Influence of multiple antenatal counseling sessions on modern contraceptive uptake in Nigeria. Eur J Contracept Reprod Health Care. 2013;18(5):381–387. doi:10.3109/13625187.2013.816672
27. Oye-Adeniran BA, Adewole IF, Umoh AV, et al. Sources of contraceptive commodities for users in Nigeria. PLoS Med. 2005;2(11):e306. doi:10.1371/journal.pmed.0020306
28. Onwujekwe OE, Enemuoh JC, Ogbonna C, et al. Are modern contraceptives acceptable to people and where do they source them from across Nigeria? BMC Int Health Hum Rights. 2013;2013(13):7. doi:10.1186/1472-698X-13-7
29. Federal Ministry of Health [Nigeria]. National Reproductive Health Working Group Meeting Report. Abuja, Nigeria: Federal Ministry of Health; 2013a.
30. Fache M, Ameh N, Daniyan G, Wada I Can public and private synergy improve uptake of family planning services in Nigeria? 2015. Available from: http://dribrahimwada.com/2015/08/06/can-public-and-private-synergy-improve-uptake-of-family-planning-services-in-nigeria/.
31. Igbodekwe FC, Oladimeji O, Oladimeji KE, Adeoye AI, Akpa OM, Lawson L. Utilization of modern contraceptive among women of childbearing age in resource constraint setting: evidence from 2008 National Demographic and Health Survey in Nigeria (2014). J Health Sci. 2014;4(3):72–78.
32. Bruce N, Pope D, Stranistreet D, editors. Chapter 2. Routine data sources and descriptive epidemiology. In: Quantitative Research Methods for Health Research: A Practical Interactive Guide to Epidemiology and Statistics. Chichester, UK: J Wiley & Sons Ltd; 2008:208.
33. Unumeri G, Ishaku S. Delivering Contraceptive Vaginal Rings: Review of Postpartum and Postnatal Care Programs in Nigeria. Abuja: Population Council; 2015. http://www.popcouncil.org/uploads/pdfs/2015RH_NigeriaPPFP.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.