")
Back to Journals » International Journal of General Medicine » Volume 12
Utilization of cross-matched blood in elective thyroid and parathyroid surgeries: a single-center retrospective study
Authors Alahmari AF , Marzouki HZ, MS Alsallum , Subki AH , Merdad M
Received 9 July 2018
Accepted for publication 9 January 2019
Published 8 February 2019 Volume 2019:12 Pages 87—90
DOI https://doi.org/10.2147/IJGM.S170328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Abdulmajeed Fahad Alahmari, Hani Z Marzouki, Mohammed Saad Alsallum, Ahmed Hussein Subki, Mazin Merdad
Department of Otorhinolaryngology, Head and Neck Surgery, College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Background: Hospital blood banks face the common challenge of maintaining an adequate supply of blood products to serve all potential patients while minimizing the need to discard expired blood products. This study aimed to determine the risk of blood transfusion during elective thyroid and parathyroid surgery and potential factors related to blood loss and risk of transfusion in these cases.
Methods: The study included all thyroid and parathyroid surgeries performed at King Abdulaziz University Hospital between January 2015 and December 2017. After exclusion of patients with incomplete data, 179 patients with complete data who had undergone thyroid and parathyroid surgery were analyzed.
Results: Of the 179 patients included in this study, 33 (18.4%) were male. Overall, patients had a mean age and body-mass index of 44.55±13.67 years and 27.66±5.38 kg/m2, respectively. The mean duration of surgery was 168.48±90.69 minutes. None of the patients had a history of previous radiotherapy, bleeding disorder, or blood transfusion. Benign goiter was the most common finding (n=78, 43.6%), followed by papillary carcinoma (n=49, 27.4%). During surgery, most patients (n=136, 76.0%) experienced minimal blood loss. None of the patients in our cohort (n= 179) required any blood transfusion or products.
Conclusion: In this study, we aimed to audit the surgical blood-ordering and -transfusion practices associated with elective thyroid and parathyroid surgeries at our institution. These practices are intended to balance the availability of blood products with the avoidance of unnecessary wastage. In our study of patients who underwent elective thyroid and parathyroid surgeries, parathyroid surgeries, none required blood transfusion.
Keywords: cross-matched blood, thyroid surgery, parathyroid surgery
Introduction
Hospital blood banks face the common challenge of maintaining an adequate supply of blood products while minimizing the need to discard expired blood products. To reduce workloads and address the current blood-product wastage of approximately 4%,1 maximum surgical blood-ordering schedule has been adopted as a common standard in elective surgeries.2–4 This blood-bank policy aims to limit the amount of blood products reserved for some predefined elective surgeries. It aims to balance as closely as possible the number of cross-matched blood units for an operation with the amount actually used in the operating room, thus ensuring that the cross-match:transfusion ratio remains near the industry standard of 2:1.5 Hospitals that have implemented the maximum surgical blood-ordering schedule have reported cost savings and more efficient utilization of blood products.6
Most head and neck surgeries, including elective thyroid surgeries, have a low cross-match:transfusion ratio,6,7 and previous studies have deemed the risk of blood loss during such surgeries to be too low to necessitate preoperative ordering and reservation of blood units.8 With this study, we aim to determine the risk of blood transfusion during elective thyroid surgery and identify potential factors related to blood loss and transfusion in this setting.
Methods
This retrospective study included all thyroid and parathyroid surgeries performed at King Abdulaziz University Hospital between January 2015 and December 2017. After exclusion patients of incomplete data, 179 patients with complete data who had undergone thyroid surgery were analyzed. Data collected from hospital records for these patients were age, sex, body-mass index, diabetes mellitus status, hypertension status, thyroid-stimulating hormone level, weight of gland, bleeding-disorder status, preoperative hemoglobin level, preoperative prothrombin time, preoperative activated partial thromboplastin time, preoperative international normalized ratio, prior chemotherapy, prior surgery, prior radiotherapy, type of surgery, duration of surgery, estimated blood-loss and blood-transfusion volumes, number of transfused units (if any), and length of postoperative hospital stay. Minimal blood loss is defined as any blood loss of 200 mL or less.
This study received ethical approval prior to data collection. This was attained from the Institutional Review Board of King Abdulaziz University Hospital, Jeddah, Saudi Arabia. Given the nature of our study, consent to review medical records was waived. Patient-data confidentiality was maintained at all times. SPSS version 20 (IBM Corporation, Armonk, NY, USA) was used to analyze data.
Results
Of the 179 patients included in this study, 33 (18.4%) were male. Overall, patients had a mean age and body-mass index of 44.55±13.67 years and 27.66±5.38 kg/m2, respectively. The mean duration of surgery was 168.48±90.69 minutes and mean postoperative hospital stay 3.38±1.17 (2–8) days. Mean values and ranges for thyroid-stimulating hormone level, weight, preoperative hemoglobin, prothrombin time, activated partial thromboplastin time, and international normalized ratio are presented in Table 1.
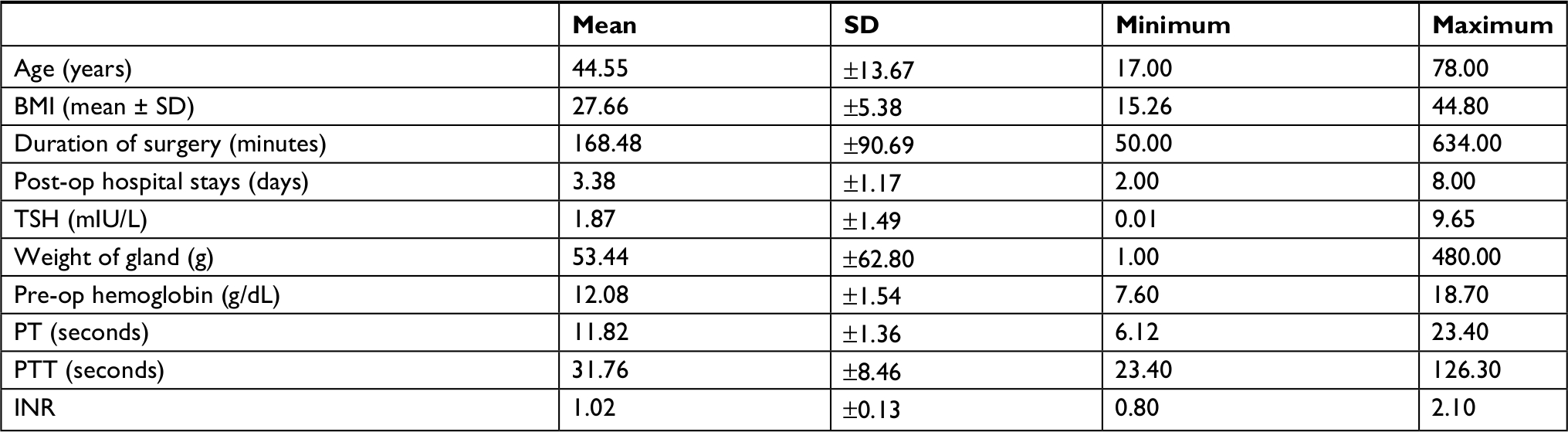 | Table 1 Descriptive statistics of all patients (continuous variables, n=179) Abbreviations: BMI, body-mass index; INR, international normalized ratio; PT, prothrombin; PTT, partial thromboplastin time; TSH, thyroid-stimulating hormone. |
A total of 73 patients (40.8%) had a history of prior surgery, while 24 (13.4%) and 36 (20.1%) had diabetes mellitus and hypertension, respectively. None of the patients had a history of previous radiotherapy, bleeding disorder, or blood transfusion (Table 2). In a histological review, benign goiter was the most common finding (43.6%), followed by papillary thyroid cancer (27.4%). More than two-thirds of patients (68.7%) underwent total thyroidectomy. During surgery, most patients (76.0%) experienced minimal blood loss during surgery, while only one patient lost 1,500–2,000 mL of blood.
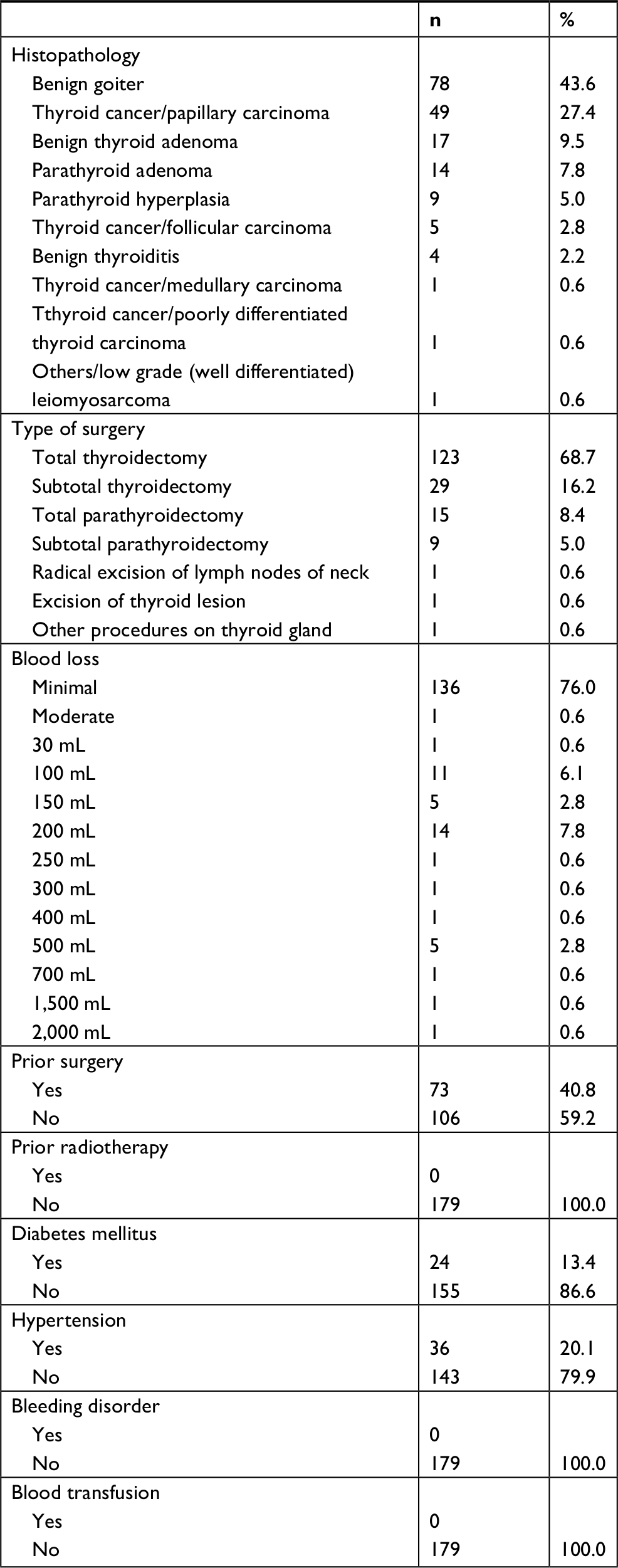 | Table 2 Pathology, type of surgery, and amount of blood loss (n=179) |
Discussion
Despite reports that routine excessive preoperative blood reservation is a source of economic loss and repeated blood wastage, the practice remains prevalent, particularly in the context of elective thyroid surgeries.2–4,9,10 Therefore, a clear transfusion policy that minimizes wastage and maximizes utilization is warranted, particularly in low-risk elective surgeries. In this study, we aimed to audit the surgical blood-ordering and -transfusion practices associated with elective thyroid and parathyroid surgeries at our institution. As noted, these practices are intended to balance the availability of blood products with the avoidance of unnecessary wastage.
In our study of patients who underwent elective thyroid and parathyroid surgeries, we found that none required blood transfusion. The reported blood loss was ≤500 mL in the vast majority of patients (98%).High-volume hospitals or those that perform more than four operations daily11 generally report lower rates of mortality and morbidity associated with thyroidectomy compared to hospitals with a lower surgical volume.12,13 None of the included operations in our study was associated with mortality. Additionally, estimated blood loss in most cases was <30 mL and average operation time <168 minutes. Two patients that underwent total thyroidectomies for papillary cancer and benign thyroiditis required 1,500 mL and 2,000 mL, but no blood transfusion was required. Only two surgeries had a duration of >10 hours, and these were for medullary and anaplastic thyroid cancers requiring concomitant neck dissection.
Our results are supported by multiple studies demonstrating a very low risk of blood transfusion during elective thyroid surgery. Kpolugbo et al reported an average blood loss in thyroid surgery of 334.3 mL and found that only 2.5% of the study population of 80 patients required blood transfusion.8 In a review of 1,122 elective thyroid surgeries, Kalenda et al found that only 0.8% of patients required intraoperative blood transfusion. Additionally, the patients requiring transfusion had predisposing factors, including coagulation issues, systemic comorbidities, preoperative anemia, or prolonged operations.14 Weiss et al reported an association of old age with increased morbidity.11
Patients with large goiters associated with Graves’s disease may be an exception to the generally low risk for blood transfusion during thyroid surgery. Yamanouchi et al assessed the risk of blood loss during elective thyroid goiter surgeries, and found a positive correlation between gland weight (>200 g) and risk of bleeding, which was explained by the potential high vascularity observed in a Graves’s disease-associated goiter.15 Interestingly, in our study histopathological analysis showed that 43.6% of excised glands had thyroid goiter; however, no association between this histology and blood-transfusion requirement was found. We note that in our series, the mean thyroid gland weight was 53.4 g, which was lower than that reported by Yamanouchi et al as associated with a requirement for transfusion.
Limitations
Our study has some limitations. First, the analysis was limited by the retrospective nature of the study. A prospective study would better enable an analysis of the potential factors affecting the risk of bleeding during elective surgeries. Second, the study was limited by the lack of specific data, such as the method of discarding unused blood.
Conclusion
This study revealed minimal blood loss and no cases requiring blood transfusion during elective thyroid and parathyroid surgeries. Additionally, we found that comorbidities, thyroid gland size, and coagulation parameters had no effect on the need for blood transfusion. Based on our results and global blood-bank standards, we recommend discontinuing the routine blood cross-matching process in routine thyroid and parathyroid surgeries.
Disclosure
The authors report no conflicts of interest in this work.
References
Zoric L, Daurat G, Demattei C, et al. Blood wastage reduction: a 10-year observational evaluation in a large teaching institution in France. Eur J Anaesthesiol. 2013;30(5):250–255. | ||
Friedman BA, Oberman HA, Chadwick AR, Kingdon KI. The maximum surgical blood order schedule and surgical blood use in the United States. Transfusion. 1976;16(4):380–387. | ||
Hall TC, Pattenden C, Hollobone C, Pollard C, Dennison AR. Blood transfusion policies in elective general surgery: how to optimise Cross-Match-to-Transfusion ratios. Transfus Med Hemother. 2013;40(1):27–31. | ||
Hardy NM, Bolen FH, Shatney CH. Maximum surgical blood order schedule reduces hospital costs. Am Surg. 1987;53(4):223–225. | ||
Thomas RAB, Daniels H, Duncan J. Blood transfusion in general surgery: MSBOS guidelines are accurate and can decrease blood wastage. Int J Surg. 2010;8(7):559. | ||
Lim EJ, Lopez CG, Veera SN, Menaka N, Aminah A. Efficiency of blood usage for elective surgery in the university hospital Kuala Lumpur. Malays J Pathol. 1996;18(2):107–112. | ||
Faridi S, Ahmad A, Beg MA, Siddiqui F, Edhi MM, Khan M. Arranging blood for elective thyroid surgeries: dilemma continues in the developing world. BMC Res Notes. 2017;10(1):49. | ||
Kpolugbo J, Uhumwangho O, Obasikene G, Alili U. Blood transfusion, antibiotics use, and surgery outcome in thyroid surgery: experience from a suburban center in Nigeria. Niger J Clin Pract. 2012;15(4):458–461. | ||
Vibhute M, Kamath SK, Shetty A. Blood utilisation in elective general surgery cases: requirements, ordering and transfusion practices. J Postgrad Med. 2000;46(1):13–17. | ||
Jayaranee S, Prathiba R, Vasanthi N, Lopez CG. An analysis of blood utilization for elective surgery in a tertiary medical centre in Malaysia. Malays J Pathol. 2002;24(1):59–66. | ||
Weiss A, Parina RP, Tang JA, Brumund KT, Chang DC, Bouvet M. Outcomes of thyroidectomy from a large California state database. Am J Surg. 2015;210(6):1170–1176; discussion 1176–1177 | ||
Pieracci FM, Fahey TJ 3rd. Effect of hospital volume of thyroidectomies on outcomes following substernal thyroidectomy. World J Surg. 2008;32(5):740–746. | ||
Efremidou EI, Papageorgiou MS, Liratzopoulos N, Manolas KJ. The efficacy and safety of total thyroidectomy in the management of benign thyroid disease: a review of 932 cases. Can J Surg. 2009;52(1):39–44. | ||
Kalenda E, Eichfeld U, Schonfelder M. [Demand for and use of blood supply for elective surgical procedures]. ZentralblChir. 1999;124(12):1091–1096; discussion 1096–1097. German. | ||
Yamanouchi K, Minami S, Hayashida N, Sakimura C, Kuroki T, Eguchi S. Predictive factors for intraoperative excessive bleeding in Graves’ disease. Asian J Surg. 2015;38(1):1–5. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.