")
Back to Journals » OncoTargets and Therapy » Volume 8
Utility of gonadotropin-releasing hormone agonists for prevention of chemotherapy-induced ovarian damage in premenopausal women with breast cancer: a systematic review and meta-analysis
Authors Shen Y, Zhang X, Lv M, Chen L, Qin TJ, Wang F, Yang J, Liu PJ, Yang J
Received 7 September 2015
Accepted for publication 15 October 2015
Published 13 November 2015 Volume 2015:8 Pages 3349—3359
DOI https://doi.org/10.2147/OTT.S95936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Yan-Wei Shen,1 Xiao-Man Zhang,1 Meng Lv,1 Ling Chen,1 Tian-Jie Qin,1 Fan Wang,1 Jiao Yang,1 Pei-Jun Liu,2 Jin Yang1
1Department of Medical Oncology, 2Center for Translational Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China
Background: Premature ovarian failure and infertility following chemotherapy are major concerns for premenopausal women with breast cancer. A potential ovarian function preservation strategy is administration of gonadotropin-releasing hormone (GnRH) agonists during adjuvant chemotherapy; however, studies of the clinical efficacy of GnRH agonists to protect chemotherapy-induced ovarian damage have shown mixed results.
Objective: This meta-analysis study was designed to estimate the efficacy of GnRH agonists administered concurrently with chemotherapy to prevent chemotherapy-induced ovarian damage in premenopausal women with breast cancer.
Methods: Electronic literature databases (PubMed, EMBASE, MEDLINE, Cochrane Library databases searching, China National Knowledge Infrastructure, Web of Science, and the Wanfang Data) were searched for relevant randomized controlled trials (RCTs) published until September 2015. Only RCTs that examined the effect of GnRH agonists for chemotherapy-induced ovarian failure in premenopausal women with breast cancer were selected. The rate of spontaneous resumption of menses and spontaneous pregnancy were collected. All data were analyzed by RevMan 5.3 (Cochrane Collaboration, Copenhagen, Denmark) and Stata 12.0 (StataCorp, College Station, TX, USA).
Results: Eleven RCTs with a total of 1,062 participants (GnRH agonists administered concurrently with chemotherapy, n=541; chemotherapy alone, n=521) were included in the meta-analysis. A significantly greater number of women treated with GnRH agonist experienced spontaneous resumption of menses after the adjuvant chemotherapy, yielding a pooled odds ratio of 2.57 (versus chemotherapy alone, 95% confidence interval (CI)=1.65, 4.01; P<0.0001). A subgroup analysis showed that addition of GnRH agonists significantly improved the resumption of menses rate in patients who were hormone-insensitive. However, the two treatment groups experienced similar spontaneous pregnancy (odds ratio =0.177; 95% CI=0.92, 1.40; P=0.09).
Conclusion: GnRH agonists cotreatment with chemotherapy in premenopausal women with breast cancer plays a beneficial role in resumption of ovarian function, with a higher rate of resumption of menses. However, treatment with GnRH agonists does not appear to exhibit its protective effects in fertility.
Keywords: GnRH agonists, ovarian damage, breast cancer, chemotherapy, meta-analysis
Introduction
Breast cancer is one of the most frequently diagnosed malignancies in women worldwide, and the probability of developing breast cancer before the age 40 years is approximately 1 for every 200 women.1 In the reproductive-age women with malignant disease, breast cancer patient’s accounts for more than 40%.2 Breast cancer in young women is characterized by generally aggressive disease, including higher incidence of undifferentiated, hormone-insensitive, and human epidermal growth factor receptor-2 overexpressing tumors.3 In addition, it may represent a unique biologic entity driven by specific oncogenic signaling pathways.4 Adjuvant chemotherapy has significantly improved disease free and overall survival in young women with breast cancer, particularly in those with hormone-insensitive breast cancer.5 However, a considerable number of these young patients eventually develop premature ovarian failure (POF) and delayed attempts at conception. The incidence of POF depends on the type and intensity of chemotherapy, age at diagnosis, and use of tamoxifen.6–8 POF has major consequences, including sexual dysfunction and loss of fertility; furthermore, it also leads to subjective (hot flashes, sweats, sleep disturbance, loss of libido) and objective (osteoporosis, cardiovascular incidents, genital atrophy, loss of mental efficiency, cognitive dysfunction, mood swings, dyspareunia, loss of vitality) menopausal symptoms,9 which may be of great concern to younger patients with breast cancer and have a strong negative impact on the quality of life.
Currently, there are no standard strategies for preventing chemotherapy-induced POF. Reproductive technology, such as cryopreservation of embryos or oocytes, has provided certain fertility preservation methods. However, the cost and feasibility of these methods are unsuitable for all patients. Ovarian protection using gonadotropin-releasing hormone (GnRH) agonist during adjuvant chemotherapy has been proposed as a potential fertility preservation strategy to prevent POF after cytotoxic chemotherapy.10 In the 1980s, the effectiveness of GnRH agonist during chemotherapy for ovarian function preservation was first demonstrated in rodents and monkeys.11,12 Later, the efficacy of GnRH agonist for ovarian function preservation in chemotherapy-treated patients with early breast cancer has been reported in many studies. While single-arm and retrospective studies demonstrated encouraging results,13–17 randomized trial data have shown mixed results.18–28 Several factors contributing to the conflicting results include heterogeneity of both study populations and procedures, treatment regimens, and lack of a proven mechanism of action for ovarian protection with GnRH agonist, which make interpretation of results more challenging.
Based on the previous clinical trials, meta-analyses of the coadministration of GnRH agonist with adjuvant chemotherapy for the preservation of ovarian function in premenopausal women with breast cancer have shown mixed results. A meta-analysis published in 2013 determined that GnRH agonists treatment during chemotherapy significantly benefited spontaneous resumption of menses in premenopausal women.29 However, a subsequent meta-analysis showed that concurrent GnRH agonists with chemotherapy may not preserve ovarian function in women with breast cancer.30 Recently, another meta-analysis provided evidence that the GnRH treatment with chemotherapy did not preserve both ovarian function and fertility. In this meta-analysis, however, there was substantial heterogeneity in the types of disease, including lymphoma, ovarian cancer, and breast cancer.31 Thus, the strength of association between GnRH-related preservation of chemotherapy-induced ovarian damage in premenopausal women with breast cancer remains controversial and unproven.
Taking into consideration the importance of ovarian function preservation for premenopausal women with breast cancer, and the controversial data on the true incidence of amenorrhea induced by contemporary chemotherapy, an improved understanding of GnRH efficacy is necessary. Therefore, we conducted a meta-analysis of up-to-date published clinical data to quantitatively evaluate the efficacy of GnRH agonists to protect against chemotherapy-induced ovarian damage in premenopausal women with breast cancer.
Materials and methods
Search strategy
To identify all the articles that reported the association of GnRH agonists for ovarian protection during adjuvant chemotherapy for breast cancer, we searched for published literature in the electronic databases, including PubMed, EMBASE, MEDLINE, Cochrane Library databases searching, China National Knowledge Infrastructure, Web of Science, and the Wanfang Data using the terms: “gonadotropin-releasing hormone agonists”, “luteinizing hormone (LH)-releasing hormone agonists”, “chemotherapy”, “ovarian preservation”, “ovarian failure”, and “breast cancer” without any restriction on language or publication year. In addition, by means of online retrieval and literature review, references obtained using the aforementioned databases were reviewed again to identify any additional eligible trials.
Inclusion and exclusion criteria
All the included studies for the meta-analysis had to meet the following inclusion criteria: 1) the patient group consisted of premenopausal women with a pathological diagnosis of breast cancer and a detailed description of patients’ basic characteristics; 2) intervention included the GnRH agonists plus chemotherapy and compared with patients treated with chemotherapy alone, with no limit to the chemotherapy scheme and the GnRH agonists treatment; 3) GnRH agonists interventions were administered concurrently with chemotherapy. For trials with more than two treatment arms, each valid pairwise comparison was considered separately; and 4) the type of study must be a randomized controlled clinical trial. Trials were excluded from the meta-analysis based on the following criteria: 1) the studies contained women with locally advanced or metastatic disease; 2) controlled trials that were not randomized; or 3) trials presented in abstract form, with relevant data not being available or no related outcome measured.
Two investigators (YWS and JY) were independently involved in citations search and identified trials that met the inclusion criteria. Inclusion and exclusion decisions were made by two investigators after evaluating the manuscripts; if views diverged, the differences were resolved through consulting with a third investigators (ML).
Data extraction and quality assessment
Two authors (YWS and JY) independently extracted the data from each trial using predefined data extraction sheet to obtain the following information: 1) baseline demographics: author, country, and year of publication; 2) study population: age of patients, sample size, characteristics of breast cancer, and types of chemotherapy; 3) GnRH agonist and chemotherapy intervention: type, schedule of administration, and duration; 4) outcome measures: resumption of menses and spontaneous pregnancy at various time intervals after the completion of chemotherapy; and 5) adverse effects. When multiple publications of the same trial were identified, only the latest publication was included. Discrepancies were resolved by consensus, if necessary, we contacted the corresponding author to obtain the data.
The methodological quality of each study was assessed independently by two researchers (YWS and JY) using the modified Jadad scale.32 The scale evaluated the study quality based on the following evaluation criteria: randomization, blinding, withdrawals, dropouts, inclusion/exclusion criteria, adverse effects, and statistical analysis (Table 1). The total score for each study ranged from 0 to 8 points, and using the eight items, the trials was divided into two levels. Trials were considered to be of low quality if they wielded 0–3 points, and of high quality if they achieved 4–8 points.
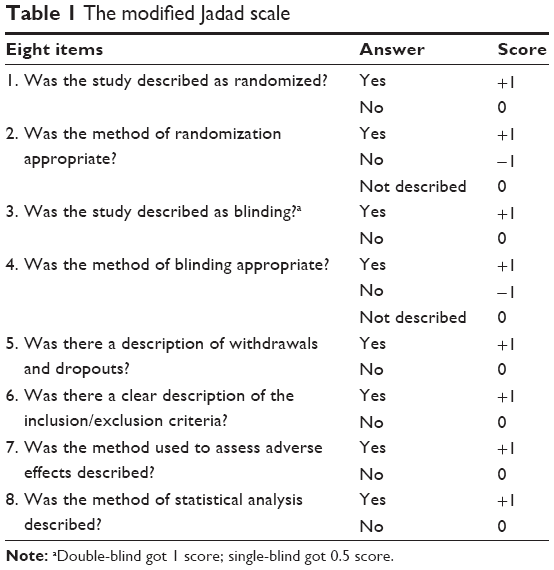 | Table 1 The modified Jadad scale |
Statistical analysis
Data management and statistical analysis were performed utilizing RevMan version 5.3 (Cochrane Collaboration, Copenhagen, Denmark) and the meta-analysis module included in Stata 12.0 (StataCorp, College Station, TX, USA). Both Q-test and I2 test were used to assess the statistical heterogeneity of the included studies. An I2 value greater than 50% indicated significant heterogeneity across studies. This research used the analytical statistics of odds ratio (OR) and 95% confidence interval (CI) to determine the effect size. The significance of the pooled OR was determined by the Z-test (P<0.05 was considered statistically significant). A random- or fixed-effects model was used to calculate pooled effect estimates in the presence (P<0.10) or absence (P>0.10) of heterogeneity, respectively. To assess the degree of potential publication bias both graphically and statistically, funnel plots and Egger’s test were performed. An asymmetric plot suggested a possible existence of publication bias and P<0.05 indicated a statistically significant publication bias.
Results
Study selection and exclusion
Overall, a total of 721 potentially relevant citations were identified at the initial search stage, and 174 duplicates removed by EndNote; 504 studies were excluded by reading the titles and abstracts. Through detailed literature sorting and reading, a total of 43 trials were considered for inclusion in the meta-analysis by preliminary analysis, but 32 studies were eliminated from the meta-analysis given that they were not randomized or presented in abstract form only. Finally, eleven trials,18–28 involving 1,062 patients, of which 541 and 521 patients were divided into GnRH agonists with chemotherapy and chemotherapy alone, respectively, were included in the meta-analysis. The flow diagram of the literature retrieval and selection is shown in Figure 1.
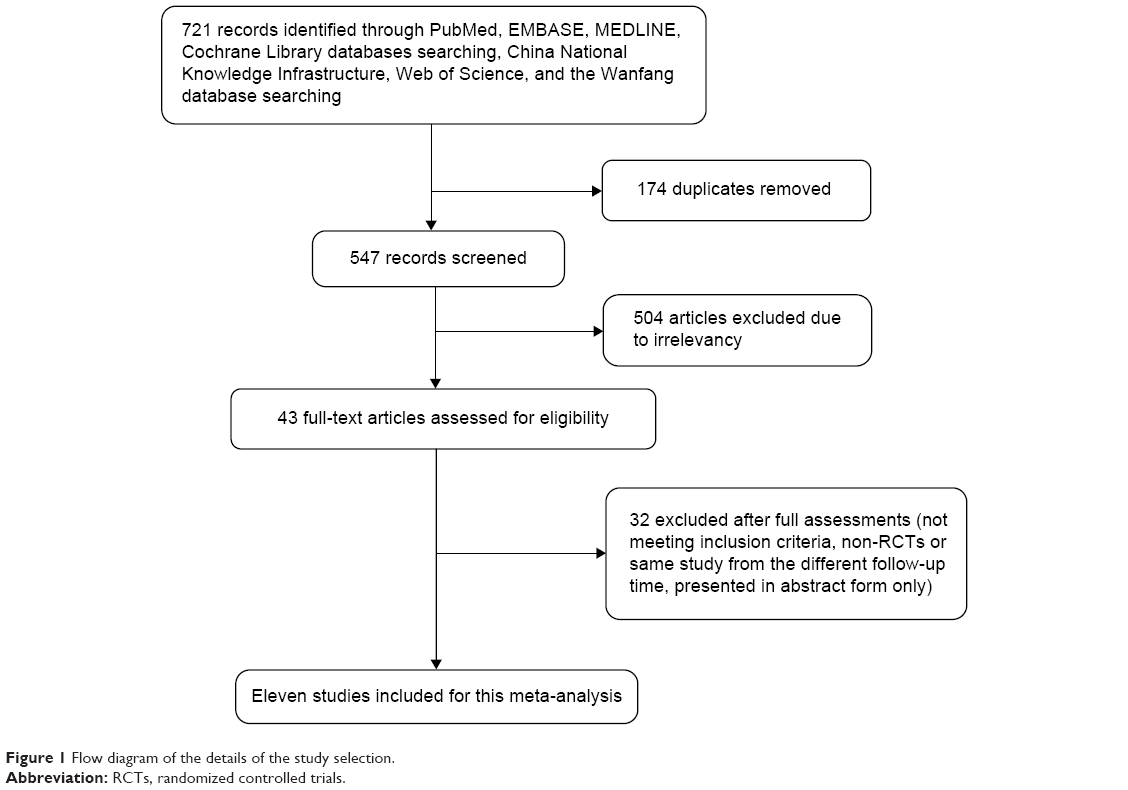 | Figure 1 Flow diagram of the details of the study selection. |
General study characteristics
The general characteristics of the all eligible trials are shown in Table 2. All of these studies included an assessment of the randomized addition of GnRH agonists to adjuvant chemotherapy. No imbalance between treatment arms for any of baseline factors (age, tumor size, nodal status, estrogen-receptor status, and progesterone-receptor status) was found. In these trials, GnRH agonists were administered once every 4 weeks throughout the chemotherapy treatment period, including goserelin, triptorelin, cetrorelix, or leuprolide. Among the eleven studies, one of them21 had more than two treatment arms, and the relevant groups were combined to create a single pair-wise comparison.
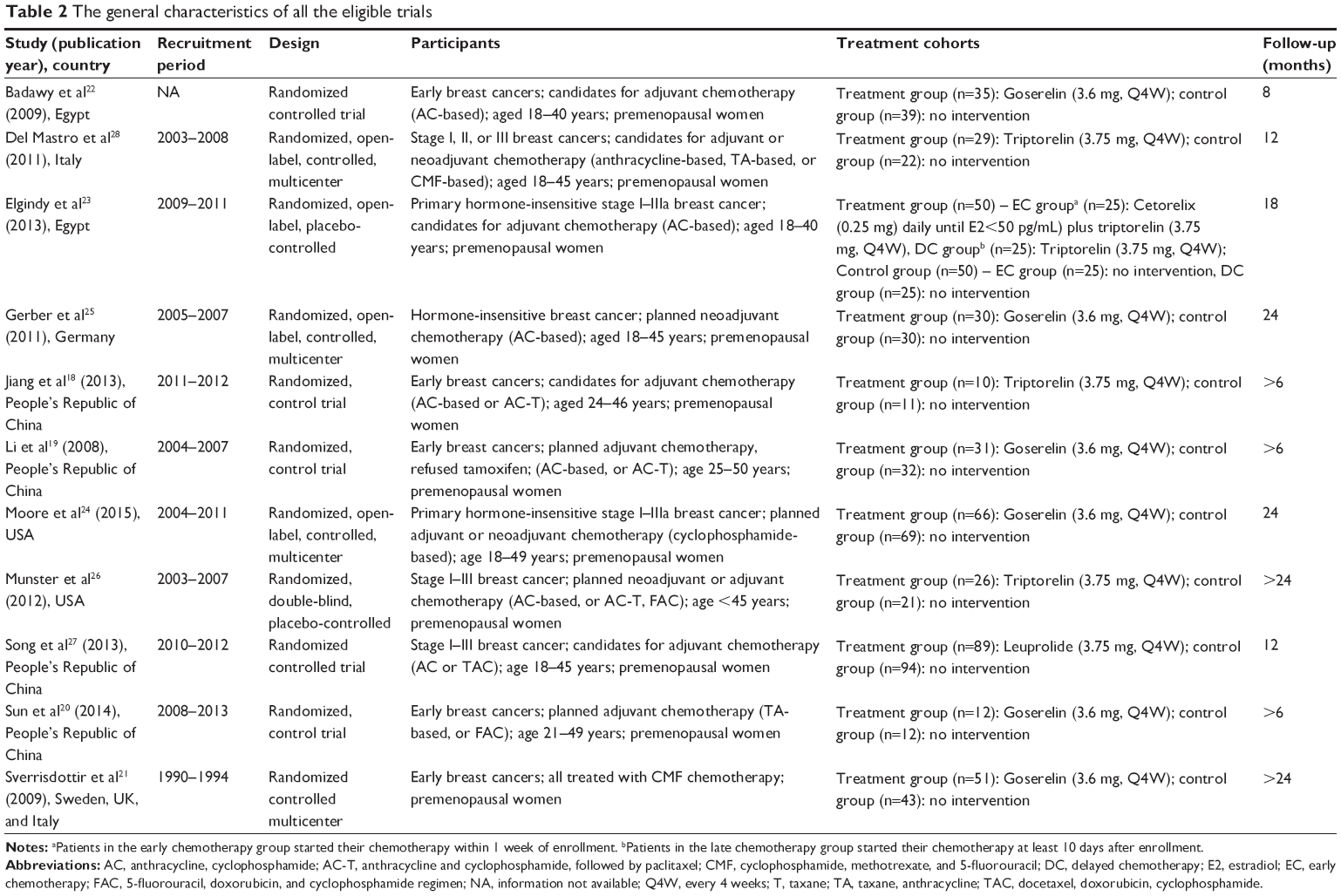 | Table 2 The general characteristics of all the eligible trials |
Assessment of the methodological quality of the included trials
The validity of the eleven studies were evaluated using the modified Jadad scale that we previously described. By evaluating every study, the mean modified Jadad scale score was 5.6 with a standard deviation of 0.4. The modified Jadad scale scores of included studies are shown in Table 3.
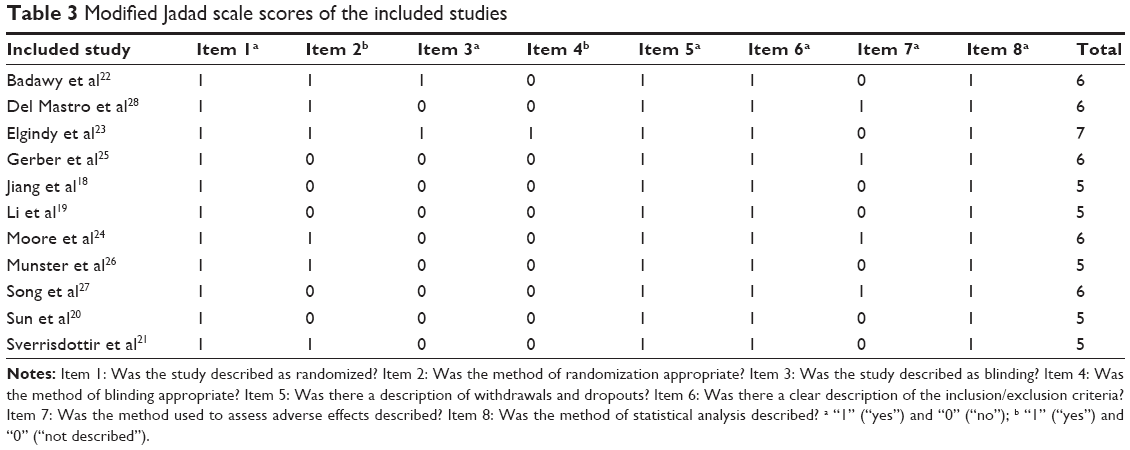 | Table 3 Modified Jadad scale scores of the included studies |
Resumption of menses rate
All the eleven randomized controlled trials evaluated the resumption of menses in relation to GnRH agonist treatment during the longest follow-up. The resumption of menses rate in the GnRH agonist plus chemotherapy arm ranged from 19.6% to 100% and the rate in the chemotherapy alone arm ranged from 11.6% to 96.5% at 6–24 months after treatment. The heterogeneity test indicated that the heterogeneity among the eleven trials was moderate (I2=43%, P=0.06). Based on heterogeneous across the studies, we used the DerSimonian and Laird33 random-effects model for analyses. The meta-analysis showed that the pooled OR was 2.57 (95% CI=1.65, 4.01; P<0.0001) and statistical significance was identified in terms of GnRH agonist plus chemotherapy relative to chemotherapy alone (Figure 2). In general, GnRH agonist administered concurrently with chemotherapy for young women with breast cancer may increase the resumption of menses rate.
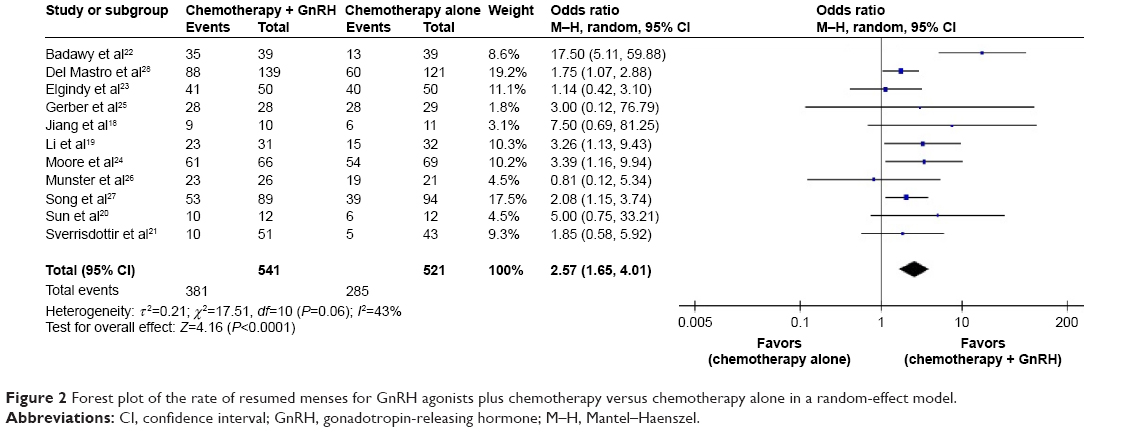 | Figure 2 Forest plot of the rate of resumed menses for GnRH agonists plus chemotherapy versus chemotherapy alone in a random-effect model. |
Spontaneous pregnancy rate
A total of four trials,24–26,28 regarding the spontaneous pregnancy rate in relation to GnRH agonist treatment during the longest follow-up, were incorporated into this meta-analysis. The heterogeneity test indicated that a fixed-effect model could be selected (I2=3%, P=0.38). The pooled results showed that the rates of spontaneous pregnancy were not significantly different between the GnRH agonist-treated patients and the patients treated with chemotherapy alone (OR=0.177; 95% CI=0.92, 1.40; P=0.09) (Figure 3).
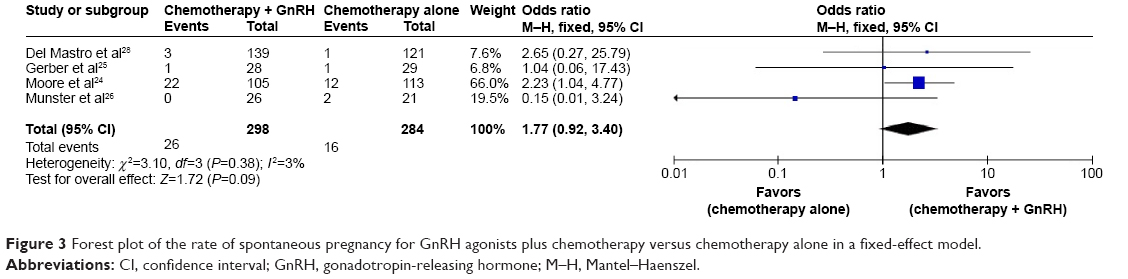 | Figure 3 Forest plot of the rate of spontaneous pregnancy for GnRH agonists plus chemotherapy versus chemotherapy alone in a fixed-effect model. |
Incidence of adverse effects
Three trials24,25,28 reported adverse events experienced by patients in the two treatment groups. Considering the existence of clinical heterogeneity, we used the random-effect model method. Compared with chemotherapy alone, the addition of GnRH agonists significantly increased the hot flushes rate (OR=1.92, 95% CI=1.26, 2.93; P=0.002). However, the pooled OR for mood modification, vaginal dryness was 1.23 (95% CI=0.71, 2.13) and 1.46 (95% CI=0.69, 3.10), respectively; the difference between the two treatment groups was not statistically significant (P=0.45 and 0.32, respectively) (Figure 4).
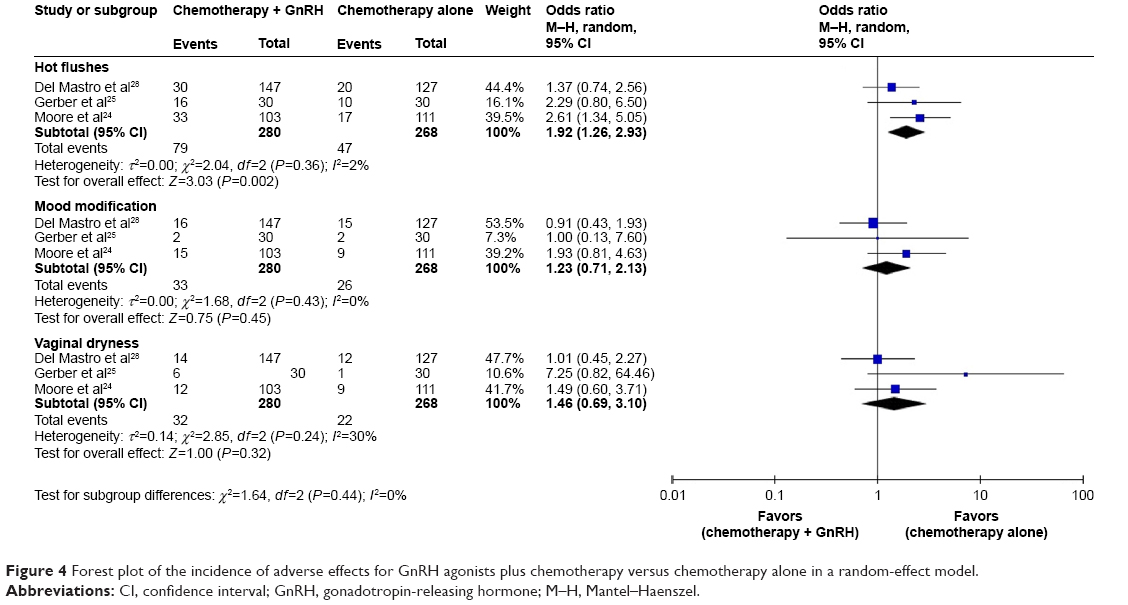 | Figure 4 Forest plot of the incidence of adverse effects for GnRH agonists plus chemotherapy versus chemotherapy alone in a random-effect model. |
Subgroup analyses of resumed menses rate
Although no significant heterogeneity was found among included studies, we still conducted subgroup analysis based on our clinical practice. Accordingly, subgroup analyses were performed after stratifications of the data by hormone receptor status (use of tamoxifen or not) and age (<35 or >35 years). In the tamoxifen (-) group, the addition of GnRH agonists significantly increased the resumed menses rate (OR=2.83, 95% CI=1.68, 4.74; P<0.0001). Nevertheless, the rate of resumption of menses was not significantly different between the GnRH agonist-treated patients and the patients treated with chemotherapy alone in the tamoxifen (+) group (OR=1.52, 95% CI=1.91, 2.54; P=0.11). Additionally, when stratified by age, the rate of spontaneous menstruation in women who were >35 years was statistically greater when GnRH agonist was used (OR=7.35; 95% CI=1.92, 28.16; P=0.004). In terms of young women with breast cancer aged <35 years, the rate of resumed menses was not statistically different between the two treatment groups (OR=3.38; 95% CI=0.32, 35.98; P=0.31) (Figure 5).
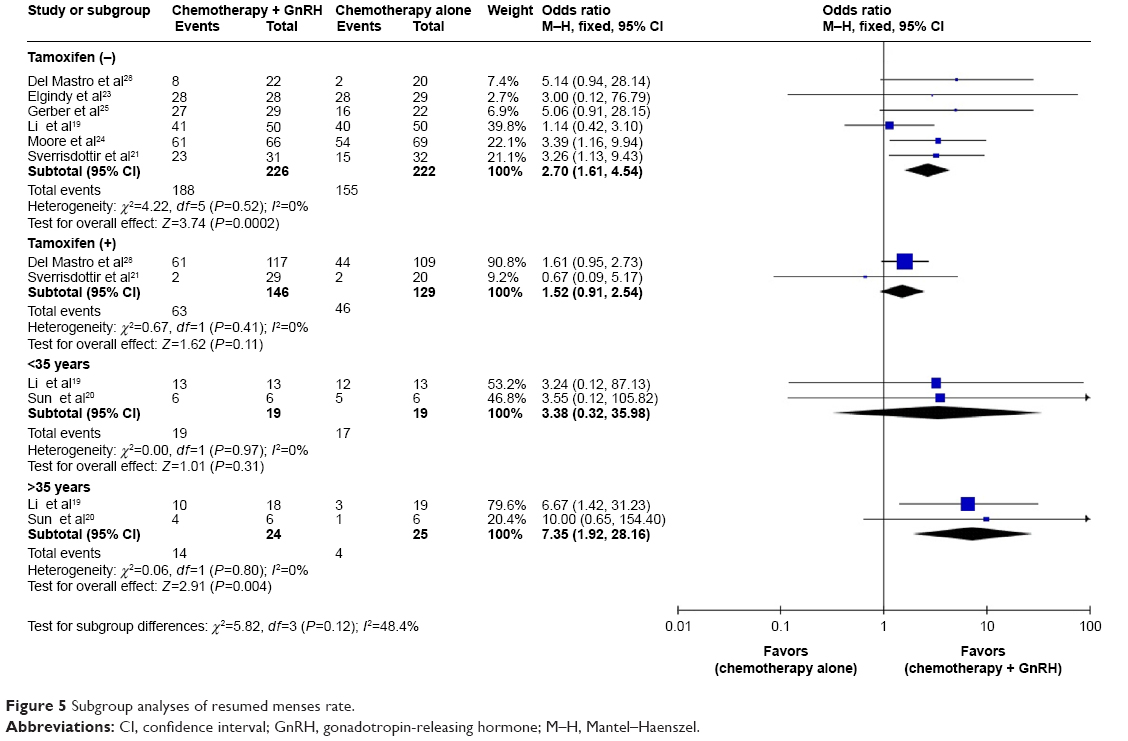 | Figure 5 Subgroup analyses of resumed menses rate. |
Publication bias
To assess the publication bias of the literature, funnel plot and Egger’s test were performed. The shape of the funnel plots seemed visually symmetrical, suggesting that there were no significant publication bias, which was further confirmed by Egger’s test (t=1.06, P=0.316) (Figure 6).
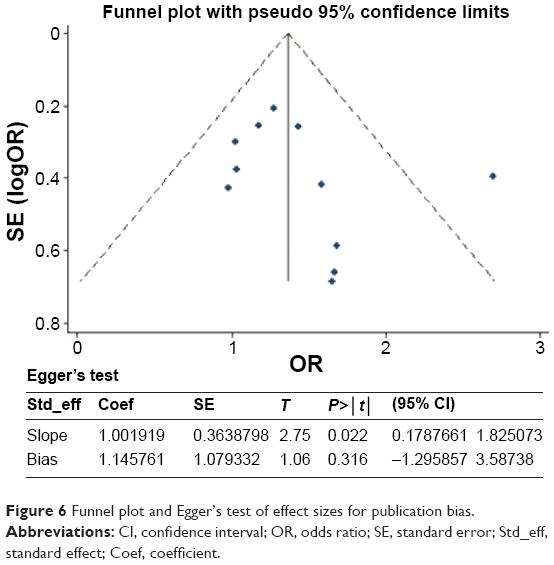 | Figure 6 Funnel plot and Egger’s test of effect sizes for publication bias. |
Discussion
The fundamental reason for treatment with GnRH agonists for ovarian protection was based on an occasional observation that prepubescent children had different rates of infertility after treatment with chemotherapy, where the prepubescent state seemed to confer some preservation to female gonads, but not male.34 Therefore, induction during the prepubescent state with GnRH agonists may mitigate chemotherapy-induced ovarian damage. The mechanism of action for ovarian protection with GnRH agonists has not been elucidated completely, though various hypotheses have been proposed. It had some possible mechanism: 1) GnRH agonists-induced hypoestrogenic state decreases ovarian perfusion; 2) GnRH agonists-induced hypogonadotropic milieu decreases the number of primordial follicles entering the differentiation stage; 3) decreased ovarian cell apoptosis, through either activation of the GnRH receptors or upregulation of intragonadal antiapoptotic molecules; and 4) GnRH agonist may have certain protective effect on ovarian germline stem cells.34 Since the early 1980s, there were some studies on the effectiveness of GnRH agonist in the preservation of chemotherapy-induced ovarian damage. However, not all studies had the same results; possible reasons include heterogeneity of the studied populations and procedures, different follow-up periods, various definitions of POF, type, and intensity of chemotherapy.
To the best of our knowledge, this is the first meta-analysis of up-to-date published clinical data to separately analyze the rate of resumption of menses with GnRH agonists administration during the course of chemotherapy among women with breast cancer in hormone receptor status and age (categorized as use of tamoxifen or not and <35 years or >35 years, respectively). In the general premenopausal women with breast cancer, regardless of their hormone receptor status, the results of this meta-analysis show that GnRH agonists during chemotherapy significantly increases the resumption of menses rate after the end of chemotherapy. However, subgroup analyses found that the advantage of GnRH agonists for ovarian protection was obvious in the either tamoxifen (-) or >35 years group, but not obvious in the tamoxifen (+) or <35 years group. Consequently, our results should be more relevant to clinical practice as they reflect the resumed menses rate among appropriate patients rather than in the general population.
It is well known that the menstruation alone may not be an accurate marker to reflect ovarian function,35 and other hormone markers such as follicle-stimulating hormone, anti-Mullerian hormone, luteinizing hormone, E2, and inhibin-A and B have been implicated with the preferred determination of ovarian functions. Monitoring the role of these hormone indicators will help in detecting chemotherapy-induced ovarian damage prior to the absence of menstruation. Measurement of anti-Mullerian hormone along with ultrasound-guided antral follicle counting has been suggested as an effective means for determining the residual ovarian function after adjuvant chemotherapy for breast cancer.36 Unfortunately, owing to the insufficiency of data, we were not able to carry out an analysis of the hormone markers to more accurately evaluate ovarian reserve in the pooled patients from the trials in this meta-analysis. Thus, the finding of this meta-analysis must be interpreted carefully.
Infertility is another potential long-term toxicity of adjuvant chemotherapy that is experienced by some reproductive-age women. As a result, occurrence of pregnancy was also used to evaluate the residual ovarian function.37,38 In the current meta-analysis, four randomized controlled trials24–26,28 evaluated the spontaneous pregnancy rate after chemotherapy. The pooled results revealed that no statistically significant increase in spontaneous pregnancies was found for GnRH agonist treatment. However, the follow-up duration of included studies was too short to really evaluate the influence on pregnancy rate. To further investigate this problem, more high-quality homogeneous prospective randomized controlled clinical studies with large sample size and long duration follow-up are required in the future.
The potential side effects of the GnRH agonists is a major concern in both young patients and treating physicians, even though the GnRH agonist treatment has a certain protective effect of preserving ovarian function in premenopausal women treated with chemotherapy. GnRH agonists suppression of the reproductive axis results in typical menopausal symptoms, including hot flushes, headaches, mood changes, sweating, and dry skin; additionally, it also decreased bone density and possible predisposition to osteoporosis or bone fracture. However, the current meta-analysis indicates that there were no statistically significant differences on mood modification and vaginal dryness between the two treatment groups. It is noteworthy that the incidence of hot flushes were significantly increased in the GnRH agonists-treated patients.
Compared with the previous meta-analyses,29–31 to a large degree, the current meta-analysis further strengthened the statistical power of the pooled results. First, all the included studies were confined to randomized controlled clinical studies with a mean score of 5.6. Moreover, this meta-analysis substantially enlarged the number of included studies and added subgroup analysis on hormone receptor status and age. Furthermore, we performed a pooled analysis on spontaneous pregnancy and adverse effects rate, so as to provide a more reliable estimation of the efficacy and safety of GnRH agonists for prevention of chemotherapy-induced ovarian damage in premenopausal women with breast cancer. Although only relatively high-quality randomized controlled clinical studies were included in the meta-analysis, several potential limitations still need to be elucidated. First, although no language restrictions were applied to our search strategy, trials in languages other than English and Chinese were not included, which might have overlooked some relevant clinical data published in other languages. Second, there was moderate heterogeneity among all included studies. The lack of uniform chemotherapy regimens, follow-up duration, use of tamoxifen, and age may be the source of heterogeneity. Third, the number of patients in the subgroup analysis according to age was inadequate, thus we may not have had enough statistical power to provide an accurate evaluation. Fourth, the outcome measurements were single as all included trials only adopted resumed menses and spontaneous pregnancy as clinical indicators to monitor the ovarian function. It would be best to assess more comprehensively by the determination of hormone markers and ovarian ultrasonography. Finally, the limited length of follow-up in the included studies restricted our evaluating power to determine the long-term effect of GnRH agonists for prevention of ovarian damage.
Conclusion
Based on the results of the present meta-analysis, GnRH agonists administered concurrently with chemotherapy in premenopausal women with breast cancer provides a potential benefit for ovarian function resumption, with higher resumed menses rates. The patients with hormone-insensitive breast cancer might benefit from the addition of GnRH agonists for prevention of chemotherapy-induced menopause. However, the benefit of GnRH agonists for fertility preservation after chemotherapy was not proved. Additional well-designed trials with larger and more diverse populations and more sensitive marker of ovarian reserve are highly needed to confirm the protective effects of GnRH agonists for chemotherapy-induced ovarian damage.
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277–300. | ||
Anders CK, Johnson R, Litton J, Phillips M, Bleyer A. Breast cancer before age 40 years. Semin Oncol. 2009;36(3):237–249. | ||
Keegan TH, DeRouen MC, Press DJ, Kurian AW, Clarke CA. Occurrence of breast cancer subtypes in adolescent and young adult women. Breast Cancer Res. 2012;14(2):R55. | ||
Anders CK, Hsu DS, Broadwater G, et al. Young age at diagnosis correlates with worse prognosis and defines a subset of breast cancers with shared patterns of gene expression. J Clin Oncol. 2008;26(20):3324–3330. | ||
Clarke M, Coates AS, Darby SC, et al. Adjuvant chemotherapy in oestrogen-receptor-poor breast cancer: patient-level meta-analysis of randomised trials. Lancet. 2008;371(9606):29–40. | ||
Walshe JM, Denduluri N, Swain SM. Amenorrhea in premenopausal women after adjuvant chemotherapy for breast cancer. J Clin Oncol. 2006;24(36):5769–5779. | ||
Goodwin PJ, Ennis M, Pritchard KI, et al. Adjuvant treatment and onset of menopause predict weight gain after breast cancer diagnosis. J Clin Oncol. 1999;17(1):120–129. | ||
Sonmezer M, Oktay K. Fertility preservation in female patients. Hum Reprod Update. 2004;10(3):251–266. | ||
Schover LR. Premature ovarian failure and its consequences: vasomotor symptoms, sexuality, and fertility. J Clin Oncol. 2008;26(5):753–758. | ||
Recchia F, Sica G, De Filippis S, Saggio G, Rosselli M, Rea S. Goserelin as ovarian protection in the adjuvant treatment of premenopausal breast cancer: a phase II pilot study. Anti-Cancer Drugs. 2002;13(4):417–424. | ||
Ataya K, Ramahi-Ataya A. Reproductive performance of female rats treated with cyclophosphamide and/or LHRH agonist. Reprod Toxicol. 1993;7(3):229–235. | ||
Bokser L, Szende B, Schally AV. Protective effects of D-Trp6-luteinising hormone-releasing hormone microcapsules against cyclophosphamide-induced gonadotoxicity in female rats. Br J Cancer. 1990;61(6):861–865. | ||
Urruticoechea A, Arnedos M, Walsh G, Dowsett M, Smith IE. Ovarian protection with goserelin during adjuvant chemotherapy for pre-menopausal women with early breast cancer (EBC). Breast Cancer Res Treat. 2008;110(3):411–416. | ||
Wong M, O’Neill S, Walsh G, Smith IE. Goserelin with chemotherapy to preserve ovarian function in pre-menopausal women with early breast cancer: menstruation and pregnancy outcomes. Ann Oncol. 2013;24(1):133–138. | ||
Maisano R, Caristi N, Mare M, et al. Protective effect of leuprolide on ovarian function in young women treated with adjuvant chemotherapy for early breast cancer: a multicenter phase II study. J Chemother. 2008;20(6):740–743. | ||
Recchia F, Saggio G, Amiconi G, et al. Gonadotropin-releasing hormone analogues added to adjuvant chemotherapy protect ovarian function and improve clinical outcomes in young women with early breast carcinoma. Cancer. 2006;106(3):514–523. | ||
Park HJ, Koo YA, Im YH, Yoon BK, Choi D. GnRH agonist therapy to protect ovarian function in young Korean breast cancer patients. J Korean Med Sci. 2010;25(1):110–116. | ||
Jiang FY, Zhang QQ, Zeng J. Protective effect of GnRHa on chemotherapy induced ovarian damage in breast cancer patients. Shandong Med J. 2013;53(8):16–18. | ||
Li MY, Huang H, Liang Y, Tan JM, Lin DR. Effect of zoladex administered before chemotherapy on menstruation of patients with breast cancer. Chin J Oncol. 2008;35(16):905–907. | ||
Sun JB, Jiang B, Yang L, Li WQ, Ren YH. Effect of the goserelin on the occurrence of chemotherapy-induced early menopause in premenopausal women with breast cancer. J Qiqihar Univ Med. 2014;35(2):224–225. | ||
Sverrisdottir A, Nystedt M, Johansson H, Fornander T. Adjuvant goserelin and ovarian preservation in chemotherapy treated patients with early breast cancer: results from a randomized trial. Breast Cancer Res Treat. 2009;117(3):561–567. | ||
Badawy A, Elnashar A, El-Ashry M, Shahat M. Gonadotropin-releasing hormone agonists for prevention of chemotherapy-induced ovarian damage: prospective randomized study. Fertil Steril. 2009;91(3):694–697. | ||
Elgindy EA, El-Haieg DO, Khorshid OM, et al. Gonadatrophin suppression to prevent chemotherapy-induced ovarian damage: a randomized controlled trial. Obstet Gynecol. 2013;121(1):78–86. | ||
Moore HC, Unger JM, Phillips KA, et al. Goserelin for ovarian protection during breast-cancer adjuvant chemotherapy. N Engl J Med. 2015;372(10):923–932. | ||
Gerber B, von Minckwitz G, Stehle H, et al. Effect of luteinizing hormone-releasing hormone agonist on ovarian function after modern adjuvant breast cancer chemotherapy: the GBG 37 ZORO study. J Clin Oncol. 2011;29(17):2334–2341. | ||
Munster PN, Moore AP, Ismail-Khan R, et al. Randomized trial using gonadotropin-releasing hormone agonist triptorelin for the preservation of ovarian function during (neo) adjuvant chemotherapy for breast cancer. J Clin Oncol. 2012;30(5):533–538. | ||
Song G, Gao H, Yuan Z. Effect of leuprolide acetate on ovarian function after cyclophosphamide-doxorubicin-based chemotherapy in premenopausal patients with breast cancer: results from a phase II randomized trial. Med Oncol. 2013;30(3):667. | ||
Del Mastro L, Boni L, Michelotti A, et al. Effect of the gonadotropin-releasing hormone analogue triptorelin on the occurrence of chemotherapy-induced early menopause in premenopausal women with breast cancer: a randomized trial. JAMA. 2011;306(3):269–276. | ||
Wang C, Chen M, Fu F, Huang M. Gonadotropin-releasing hormone analog cotreatment for the preservation of ovarian function during gonadotoxic chemotherapy for breast cancer: a meta-analysis. PloS One. 2013;8(6):e66360. | ||
Vitek WS, Shayne M, Hoeger K, Han Y, Messing S, Fung C. Gonadotropin-releasing hormone agonists for the preservation of ovarian function among women with breast cancer who did not use tamoxifen after chemotherapy: a systematic review and meta-analysis. Fertil Steril. 2014;102(3):808–815. | ||
Elgindy E, Sibai H, Abdelghani A, Mostafa M. Protecting ovaries during chemotherapy through gonad suppression: a systematic review and meta-analysis. Obstet Gynecol. 2015;126(1):187–195. | ||
Oremus M, Wolfson C, Perrault A, Demers L, Momoli F, Moride Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement Geriatr Cogn Disord. 2001;12(3):232–236. | ||
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. | ||
Blumenfeld Z. How to preserve fertility in young women exposed to chemotherapy? The role of GnRH agonist cotreatment in addition to cryopreservation of embrya, oocytes, or ovaries. Oncologist. 2007;12(9):1044–1054. | ||
Bukman A, Heineman MJ. Ovarian reserve testing and the use of prognostic models in patients with subfertility. Hum Reprod Update. 2001;7(6):581–590. | ||
Anderson RA, Themmen AP, Al-Qahtani A, Groome NP, Cameron DA. The effects of chemotherapy and long-term gonadotrophin suppression on the ovarian reserve in premenopausal women with breast cancer. Hum Reprod. 2006;21(10):2583–2592. | ||
Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update. 2006;12(6):685–718. | ||
Broer SL, van Disseldorp J, Broeze KA, et al. Added value of ovarian reserve testing on patient characteristics in the prediction of ovarian response and ongoing pregnancy: an individual patient data approach. Hum Reprod Update. 2013;19(1):26–36. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.