")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Using Participatory Methods to Engage Multidisciplinary Clinical Staff in the Embedding of Trauma-Informed Care and Practice Principles in a Sub-Acute Mental Health Inpatient Unit
Authors Walsh K , Benjamin R
Received 27 November 2019
Accepted for publication 1 April 2020
Published 26 May 2020 Volume 2020:13 Pages 485—494
DOI https://doi.org/10.2147/JMDH.S240240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kenneth Walsh,1 Richard Benjamin2
1School of Nursing, University of Tasmania, Hobart, Tasmania, Australia; 2Clarence and Eastern Districts Adult Community Health Service, Rosny Park, Tasmania, Australia
Correspondence: Richard Benjamin
Clarence and Eastern Districts Adult Community Mental Health Service, c/- Clarence Integrated Care Centre, 16-22 Bayfield St, Rosny Park, Tasmania 7018, Australia
Email [email protected]
Abstract: Changing multidisciplinary team practice is difficult, even in circumstances where the staff support such change. This methodology paper describes the successful use of respectful and participatory methods and processes to engage multidisciplinary clinical staff in practice change. These methods are described and discussed in relation to a clinical practice change project that sought to embed trauma-informed care and practice (TICP) in a sub-acute mental health unit. TICP is a critical new paradigm for multidisciplinary mental health services that involves the recognition of the high rates of abuse and trauma suffered by those with mental illness and the need to both understand the effects of this abuse and trauma and to respond to them appropriately. The principles of the paradigm need to be introduced throughout mental health services, but especially in inpatient units where a predominantly biomedical perspective can preclude a more holistic approach. This paper outlines the background of TICP and describes in detail the four TICP-compatible, participatory methods and processes used to engage staff in the embedding of TICP principles in their everyday practice. The participatory approaches employed reflected TICP principles and addressed issues including the engagement of staff in the change project, the identification of TICP-compatible care practices currently used in the unit, the identification of issues related to the further embedding of TICP in everyday care, and the generation of solutions to the issues raised. The processes undertaken were underpinned by a heuristic framework to maintain staff engagement. This paper is not intended to be a recipe for TICP change. However, the methods and processes described may be adapted to be of practical use in the design of TICP and other practice change initiatives in multidisciplinary clinical settings.
Keywords: engagement, practice development, solution-focused approaches, mental health, trauma-informed care and practice
Introduction and Aims
The aim of this paper is to describe the use of four interrelated practice change methods and processes to engage multidisciplinary staff in practice change. These are described and discussed in relation to their use in a clinical practice change project to embed trauma-informed care and practice (TICP) in a sub-acute mental health unit.
Trauma-informed care and practice (TICP) is a critical new paradigm in mental health services involving an understanding of the high prevalence of abuse and trauma in those who attend mental health services, and of the significant neurological, biological, psychological and social effects of such experiences. The key or guiding principles of TICP are safety, trustworthiness, choice, collaboration and empowerment.1
The change project sought to engage multidisciplinary staff with the paradigm of TICP, to gather staff perceptions about what TICP practices were already in place, and to consider how to build upon these practices to further embed TICP in the everyday life of a sub-acute mental health inpatient unit.
For the project team, it was vitally important that the methods and processes used to achieve the project aims engaged staff and were, in themselves, safe, trustworthy, provided choice, and fostered collaboration and empowerment. That is, it was important that they were TICP-compatible. This paper outlines the background of TICP and describes in detail the TICP-compatible participatory methods and processes adopted and their use in achieving the change project’s aims. We hope our experience may be useful to other teams interested in TICP or wanting to use respectful and participatory methods and processes to engage staff to plan and implement person-centred practice change.
Background to Trauma-Informed Care and Practice and the Sub-Acute Mental Health Unit
Before describing the project and the four interrelated change methods and processes used, it is important to situate the project within the current mental health care context and outline the background and principles of TICP. The current mental health landscape in Australia, although diverse, is dominated by the “bio-medical” paradigm of psychiatry, particularly in public settings. This paradigm promotes the “diagnosis” of mental illness primarily by the clustering together of symptoms, and the “treatment” of mental illness, frequently by psychopharmacological means, and/or by brief, structured psychological interventions. Over recent years, another focus for those with significant mental illness has been the addition of psychosocial support within the community. These approaches often fail to take into account the sometimes profound effect that the environment can have upon individuals, particularly as a result of abuse and trauma, including sexual abuse, physical abuse, emotional abuse and neglect. Over the last several decades it has been found, for example, that by far the majority of adults with severe mental illness have been exposed to trauma, and that many have undiagnosed Posttraumatic Stress Disorder.2–4 A history of childhood abuse has also been described in connection with almost all the severe mental illnesses, including psychosis, although the relationship is frequently overlooked.5,6 This type of misunderstanding may lead to the provision of inappropriate treatment, sometimes over many years. TICP approaches include the recognition, understanding and responding to those suffering the effects of many different types of abuse and trauma.
The importance of recognising the effects of trauma is especially relevant to care provided in inpatient units, where those suffering from mental illness often present in extremis, and power differentials between staff and consumers may be very high; this is particularly relevant with respect to the use of involuntary treatment, including psychotropic medication, and the use of seclusion and restraint. When consumers present, and their trauma histories go unrecognised, they may be re-traumatised by many of the regular ward practices. One of the fundamental practice concepts of TICP is the institution of “universal precautions” with respect to trauma: that is, treating all consumers as if they have been traumatised. This involves careful reception processes, the process of sensitively taking thorough histories, responding to trauma issues, as well as careful and sensitive approaches to personal possessions, personal space, accommodation options, gender, and so on. An example of staff being responsive to a patient’s possible trauma history using TICP principles is illustrated in the following scenario.
“Sally”* is a 58-year-old single primary school teacher. She originally presented with acute suicidal ideation and depressive symptoms, and at transfer to the sub-acute unit was still thought to present some risk to herself. The receiving staff almost immediately noted that Sally appeared to be frightened of any men in her environment. They discussed this issue in clinical review, and with heightened awareness of trauma, and of the TICP principles of safety and trustworthiness, speculated that a history of trauma might have been important for Sally and that issues other than depressive symptoms might benefit from consideration. It was agreed that the unit psychologist, “Jane”**would see her. Sally met Jane the day after transfer.
Sally confided in Jane that a male patient had been sexually inappropriate toward her in the acute unit, trying to touch her and to kiss her. She said that she thought that she might not be believed if she told anybody, and that she did not feel that she could speak freely in the doctor’s round; there were just too many people there and the space was just too overwhelming. With Sally’s permission, Jane discussed this issue with her treating doctor and the other unit staff, and Sally was moved to a room that was closer to the nurse’s station, where she might feel safer. Staff as a group also volunteered that they would be more aware of Sally’s concerns regarding other people in her environment, and the potential relevance of other trauma-related factors in her presentation.
Jane met with Sally every other day and Sally came to trust her a little more each time. She told Jane that she had for many years suffered anxiety, nightmares and insomnia. At their fourth meeting, just before the session was about to end, Sally burst into tears and told Jane that she had been sexually assaulted by an uncle on many occasions when she was between about six and eight years of age. Sally had never shared this information with anybody previously.
Although they were never able to work out the trigger for her recent suicidal ideation, Sally wanted to keep talking about her past to see what more she could make sense of. She was now sure, however, that she chose to work with children because she thought they were “safe”. She also wondered what her looming retirement might mean for her.
Sally was discharged two weeks after transfer, feeling much more settled. She discussed her follow-up with Jane and they agreed she should attend the local sexual assault service. Sally also gave her consent for Jane to discuss her history with her General Practitioner.
After Sally left, the unit staff discussed her admission. Almost all said that they felt that, because of the trauma training that they had received, they understood Sally as more of an individual person with her own trauma history. Trauma training also helped them look after Sally more compassionately and helped them to be more thoughtful generally regarding the backgrounds of people coming into their care.
*“Sally” is a fictional patient, based on the experience of one of the authors (RB). **“Jane” is a fictional psychologist.
The setting for this project was a 10-bed public sub-acute mental health inpatient unit in Hobart, Tasmania. When this work was undertaken, in 2016 and 2017, the unit functioned as a “step-down” facility for the local general hospital acute mental health unit, and a “step-up” facility for the local adult community mental health teams. The unit at that time had a model of care that involved two to four-week admissions, with multidisciplinary input from community psychiatrists, nurses and allied health. The unit is physically easy to navigate, with a central dining, TV and socialisation area. The nursing staff work 12-hour shifts, have mental health qualifications, and most have been in their positions for many years. As a result of the above combination of factors, the unit is well organised and psychologically very “containing”.
A number of staff expressed an interest in embedding TICP in everyday practice and contacted the local university for assistance and a multidisciplinary project team was formed. The project team consisted of nursing, medical and allied health staff of the unit and a nursing academic from the local university. Prior to this project, it had been recognised that some of the unit’s medical, nursing, and allied health staff were either familiar or somewhat familiar with the principles of TICP, so that it seemed like an appropriate unit in which to attempt to further embed the principles. As part of the process, all staff also underwent a one-day training course in TICP prior to the commencement of the change project.
Methodology and Methods
Tasmania Health and Medical Human Research Ethics Committee approval for the project was obtained and collaborative, inclusive and participatory practice development methodology and methods were employed. Practice development has been defined by Manley et al (2008)7 as:
… a continuous process of developing person-centred cultures. It is enabled by facilitators who authentically engage with individuals and teams to blend personal qualities and creative imagination with practice skills and practice wisdom. The learning that occurs brings about transformations of individual and team practices.
As mentioned earlier, the overall aim of the change project was to embed trauma-informed care and practice (TICP) in a sub-acute mental health unit. The practice development methodology employed by the project team to meet the project aim involved using a structured engagement tool and semi-structured group interviews with all staff in order to understand the strengths of current practices and the issues of concern to be addressed in embedding the new paradigm in the unit. Following the identification of strengths and issues, staff were engaged in a modified “World Café” group event to formulate feasible, appropriate, meaningful and effective solutions to the puzzle of embedding TICP practices in everyday care in the unit. These methods, described in detail later, were chosen on the basis that they were TICP-compatible, would engage staff, and would be solution, rather than blame, focused.
Facilitating Change and Choosing TICP-Compatible Methods and Processes
Changing practice, even in circumstances where staff are motivated, can be difficult. Change comes with many underlying and often unspoken assumptions. For there to be a need for change, something currently happening must be considered less than optimal, or even “bad”, and this has further implications for those currently carrying out this work; they may, by association, be seen as “bad”. This situation is potentially further exacerbated by the problem-focused approach usually applied to change.8–10 This problem focus is reflected in everyday language, “you have a problem”, “that’s not my problem, that’s your problem”, or, “who caused the problem in the first place?”.9 In this way, problems (things that need changing) have negativity, blame and ownership attached to them. This may have the effect of disengaging the very people needed to bring about change.11 Coupled with the frequent lack of a structured process of engagement as a precursor to change, it is not surprising that change is almost universally seen as a difficult thing to bring about.
Much has been written about the importance of collaboration in change processes, but much less attention has been paid to engagement as a precursor to collaboration.12 In light of this, it was believed that those involved in embedding TICP principles in the sub-acute unit needed to develop a robust engagement plan and use participatory change methods for the project. It was also evident that any such method should be compatible with the principles of TICP,1,13 so that the project mirrored the principles of safety, trustworthiness, choice, collaboration and empowerment that the project team wanted to embed.
To this end, the project team employed two stakeholder engagement methods to engage staff in the project: the “Building Effective Engagement Techniques Tool” (BEET),12 and a modified Fourth Generation stakeholder evaluation method known as “Claims, Concerns and Issues”, or CCI.14,15 This was followed by a World Café group session and underpinned by a heuristic engagement framework known as SCARF.16,17
These four methods and processes were designed to:
- Engage staff in the project (BEET tool),
- Identify current TICP-compatible care practices currently used in the unit (CCI),
- Take a non-blame approach to identify issues related to further embedding TICP in everyday care (CCI),
- Generate feasible, meaningful solutions to these issues (World Café), and
- Be underpinned by a heuristic framework (SCARF)17 designed to maintain engagement throughout the project.
As this methodology paper is about using respectful and engaging methods and processes to assist in planning and implementing participatory person-centred practice change, the four methods that were employed and examples of their process outcomes are considered “results” and will be described in detail in this section.
Results
Engaging Staff in the Project Using the BEET Tool
The first step in the process of embedding TICP in the unit was to engage the staff. This was assisted by using the BEET tool (the complete tool is available on request). The BEET tool is designed to engage teams in change by developing an engagement statement that avoids blame while clearly outlining the practice “puzzle” to be solved or the issue to be addressed, the evidence on which the need for change is based and the outcomes that are sought. It deliberately uses inclusive non-problem focused language, in order to minimise the threat response often associated with change and to keep staff engaged.9,17 For example, the main engagement statement is written as a puzzle to be solved collaboratively, rather than a problem, and is framed as, “How can we work together to … ?”.
The outcome of the BEET tool is a one-page statement that is used as a script for project teams to engage others and as a guide to keep the project on track. Once the draft engagement statement is developed using the tool, it must pass a test called the PUG-Q test, or the Positive, Unconditional, Generative, Question test.12 The engagement statement should be positively stated with no actual or implied blame attached. It should be unconditional in that it should not have a preconceived solution in it; the solution should come out of the engagement with the stakeholders. This also guards against the “Why don’t you … yes but” phenomenon,18 where people will argue against a preconceived solution that they have not been a part of developing. The statement should be generative, in that it lends itself to more than one solution and, finally, it should be a genuine question around which genuine engagement is wanted, rather than a statement with a question mark attached.
The statement should also include the evidence that indicated the change was needed, framed as “currently we know … ” and the broad outcomes which could be achieved, framed as, “We think that, if we could solve this puzzle, our clients would … our staff would … and our organisation would … ”.The engagement statement the project team developed is depicted in Box 1.
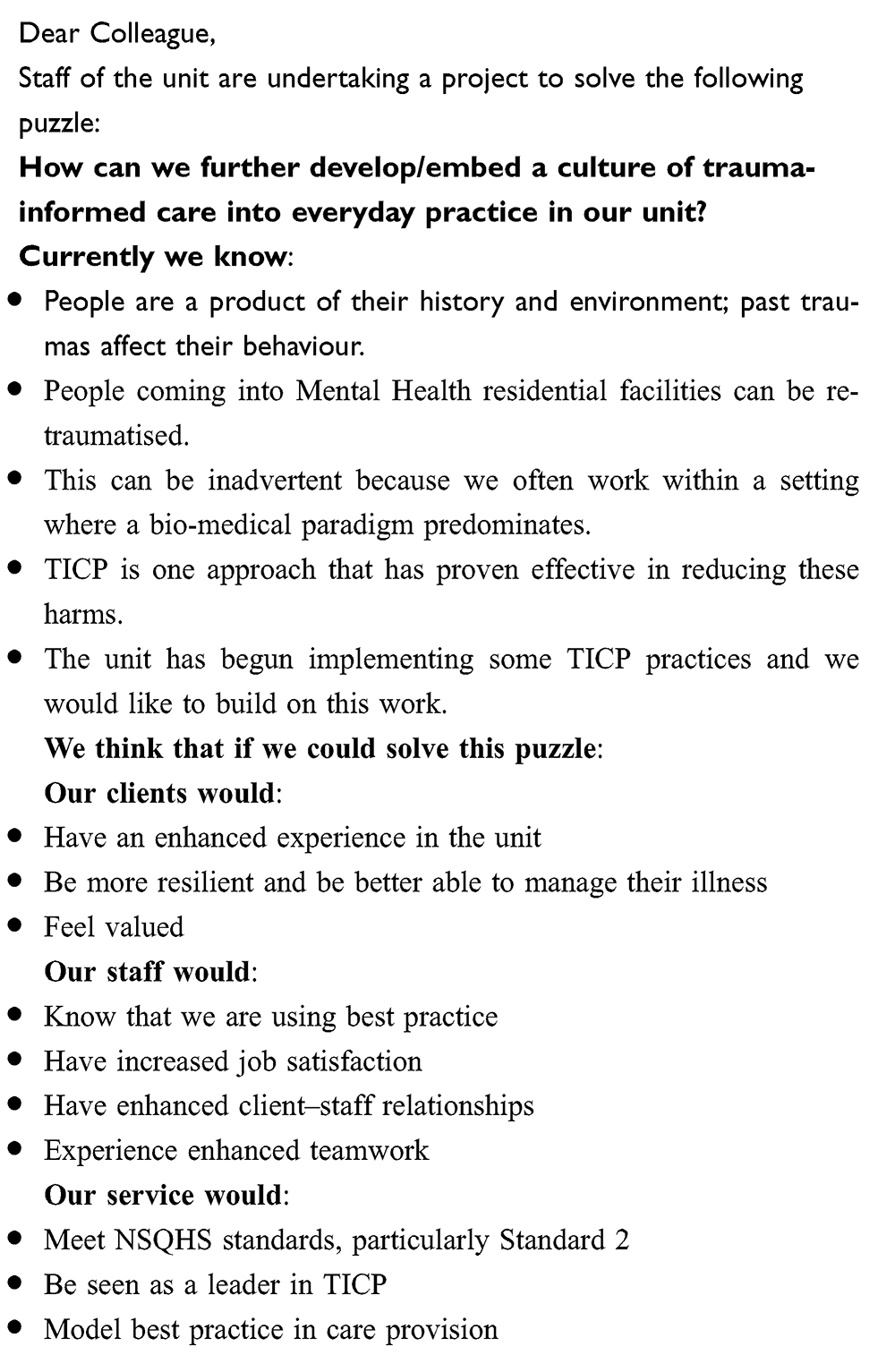 |
Box 1 Engagement statement |
Once the statement had been developed, it was used by the project team as a script to engage staff in the project. Wherever possible this was done face-to-face. The temptation to send out group emails to staff was resisted as it was believed that engaging staff face-to-face better conveyed the importance of the staff members to the project. This was based on the belief that such face-to-face interaction imparts a psychological status reward which enhances engagement.17,19 This was based on the use of a heuristic framework named SCARF (described later)17 for staff engagement which underpinned the facilitation of the methods and processes used.
It is noteworthy that following the engagement process, all staff, excluding those who were on leave, voluntarily elected to participate in the Claims, Concerns and Issues groups which followed.
Identifying Current and Future Trauma-Informed Care Practices in the Unit Using Claims, Concerns and Issues Group Sessions
The Claims, Concerns and Issues (CCI) group process was adapted from Fourth Generation Evaluation processes.14,15 Fourth Generation Evaluation is an approach that adopts a constructivist paradigm that takes a negotiated approach to evaluation.20 It is used to engage team members in evaluating an issue specific to the context and culture; in this case, evaluating the extent to which TICP was evident in the ward environment and identifying the issues that if addressed, might lead to it being further embedded.
The CCI process consisted of four group sessions where multidisciplinary team members were asked to reflect on their claims, concerns and issues in relation to a question. In this case, the question was, “How can we further develop/embed a culture of trauma-informed care (TICP) into everyday practice in the sub-acute unit?” (see Box 1) which was developed using the BEET tool discussed earlier. All sessions were held face-to-face on the ward and included sessions for staff on night shift. Once again, face-to-face was the preferred mode of communication as the project team believed this conveyed respect for the staff and their contribution to the project. The CCI sessions lasted from 30–45 minutes. Staff responses to the claims, concerns and issues were captured on a whiteboard so that staff could clearly see their responses and build upon or challenge these if they wished. A total of 24 staff attended the CCI sessions.
Participants were first asked to consider what claims they could make in relation to the puzzle question identified in the engagement statement (“How can we further develop/embed a culture of trauma-informed care (TICP) into everyday practice in the sub-acute unit?). “Claims” in the context of CCI are the good things that are already happening in the unit regarding TICP, the strengths the staff possess which would assist them and the features of the context which would contribute to further embedding TICP in everyday practice. Beginning with the “claims” was deliberate in that it began the engagement from a positive, strengths-based position and avoided leading with a negative narrative. Following the claims, the participants were then asked to consider the concerns they may have about the puzzle question. These concerns were then transformed by the participants into issues to be addressed together, in the form of a question, “How can we … ?”. The issues were later used to form a plan of action to develop solutions and evaluate the initiative (see World Café below). Table 1 (below) contains examples of some of the claims, concerns and issues identified by the staff in relation to the puzzle identified in Box 1 (see above).
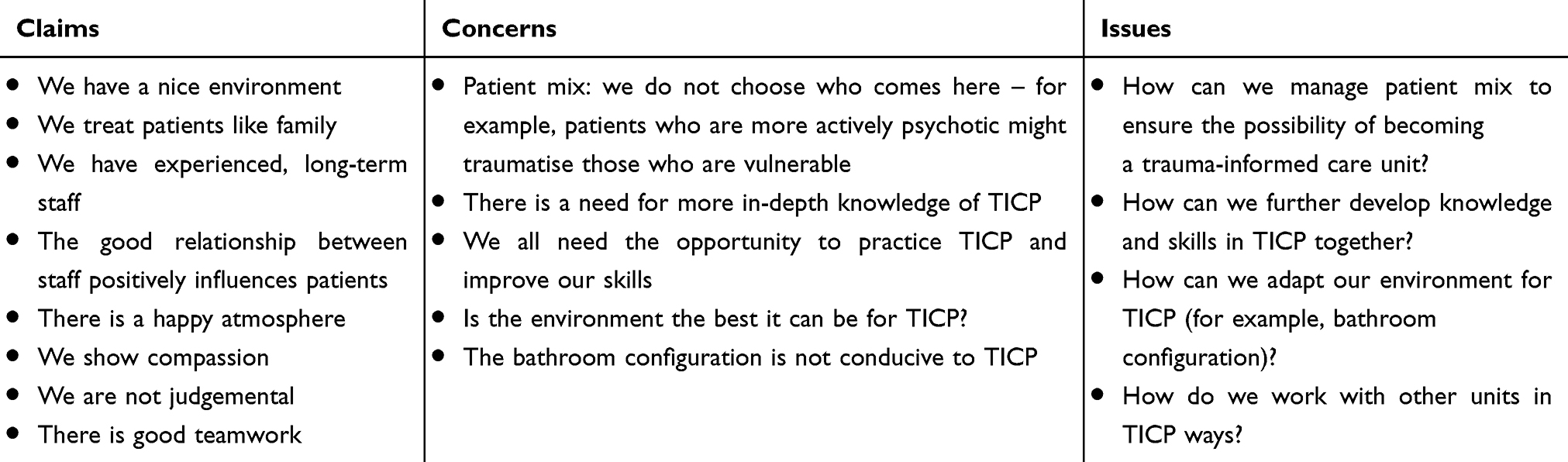 |
Table 1 Claims, Concerns and Issues Identified by Staff |
As can be seen from the examples given in Table 1, staff claims tended to focus upon positive staff-staff and staff-consumer relationships as well as staff mental health knowledge, clinical experience and compassion. They had concerns about gaps in their knowledge of TICP, the physical environment and its compatibility with TICP as well as consumer mix, policies and procedures. The concerns were translated by the group into issues to be addressed which included management, policy and governance issues, educational needs including TICP skill development, and meeting consumer needs in TICP appropriate ways.
Following the CCI sessions, the project team reviewed the CCI data. Common issues identified across the four CCI group sessions were summarised into four main issues to be the focus of the World Café event.
Generating Solutions to TICP Related Issues Using the World Café Process
The World Café session was used to collaboratively develop solutions to solve these issues. World Café methodology was developed by Juanita Brown and is based around seven principles:16
- Set the context
- Create hospitable space
- Explore questions that matter
- Explore everyone’s contribution
- Cross-pollinate and connect diverse perspectives
- Listen together for patterns, insights and deeper questions
- Harvest and share collective discoveries
Brown noted that people naturally engage with each other in informal settings such as cafés. The World Café methodology seeks to engage small groups to generate answers to important questions. Tan and Brown16 state that:
In a World Café dialogue, intimate conversations at small café-style tables or in small conversation clusters link and build on each other as people move between groups, cross-pollinate ideas, and make new connections around questions that really matter to their life, work, or community.
Fifteen staff of the sub-acute unit volunteered to participate in a 180-minute World Café event. Following an explanation of the purpose of the exercise and a light-hearted ice breaker, participants were asked to seat themselves at one of four tables. Each table was “hosted” by a facilitator who was a member of the project team. Each table had a “menu” in the form of a question to be discussed by the table participants. The “menu” questions were derived from the summarised issues stemming from the CCI sessions (see Table 1) and were:
- How can we be more sensitive to consumer issues?
- How can we adapt our physical and social environment to cater to consumer needs?
- How can we ensure that staff are up to date with TIC practice and feel supported in their work?
- How can we manage the challenging consumer mix?
The participants on each table discussed the question on their table and the host captured and summarised the key points on the paper tablecloth. After 15 minutes the participants rotated to a new table with a different question. The table host shared the results of the previous participants’ deliberations and facilitated the new participants to link to and build on the previous participants’ ideas. This was repeated until all the participants had the opportunity to engage with each “table menu” or question.
Following this, the table facilitators “harvested” the solutions generated to each question and these were displayed on the wall for all participants to see. Participants were then given four adhesive-backed coloured paper dots and asked to vote for the solutions they believed were the most feasible, appropriate, meaningful and effective by placing one or more of the dots beside their favoured solutions.
For example, in response to question one, “How can we be more sensitive to the consumers’ issues?”, the most favoured solution was
Through recognition of our own issues and personal biases, and how we can more effectively deal with ourselves, and with our consumers; we need further education on this.
Other solutions included being mindful of the power of the language when interacting with consumers and each other, recognising the importance of listening to the consumers’ story, providing further skills development in therapeutic communication, and consciously embedding TICP in all aspects of the unit functioning, including management practices and policy. In response to question two, “How can we adapt our physical and social environment to cater to consumer needs?”, staff spoke of the reality of the limitations of the unit’s physical design but suggested feasible improvements which could be made related to caring for the unit and keeping it clean and tidy as well as practical suggestions to make the space more inviting, comfortable and safe for everyone.
In relation to question three, “How can we ensure that staff are up to date with TIC practice and feel supported in their work?”, staff suggested education and skill development as well as working empathically with consumers and each other, in order to keep up to date with TICP practice and be supported to work in TICP compatible ways.
In response to question four, “How can we manage the challenging consumer mix?”, staff discussed the issues related to consumer mix and suggested solutions such as meeting with new consumers prior to admission, having clear guidance for everyone on the rights and responsibilities when living and working in the unit, and clarifying as much as possible what a person-centred model of care (underpinned by TICP) actually looks like.
The World Café event generated practical and feasible, context-specific solutions to the issues identified. These solutions were then used by the project team to form the basis of an action plan to embed TICP into the sub-acute unit. This work is ongoing. Although the unit has been partially re-purposed since this work was done, and some of the project team members are no longer involved with the unit, staff are still engaged in implementing the solutions identified by this project.
Keeping Staff Engaged Throughout the Project Using the SCARF Framework
The aims of this project were to engage staff about TICP, gather staff perceptions about what TIC practices were already in place and how to build upon these to further embed TICP in the everyday life of a sub-acute mental health inpatient unit. In addition, the project team set out to use processes that were compatible with TICP principles to achieve the aims. It was assumed that staff would have encountered change processes in the past that were driven from the “top down”, with preconceived solutions derived from problem-based reasoning and situated within a culture of blame. In contrast, the processes the project team used were designed to facilitate open staff engagement from a strengths-based perspective and tap into the social and intellectual capital of the staff to meet the shared aims of the project.
In addition to using the processes of the BEET Tool, Claims, Concerns and Issues and the World Café, the project team facilitated these processes using a heuristic framework designed to maximise staff engagement. The framework, developed by David Rock called the SCARF framework.17 SCARF is an acronym for the five social domains, which, according to Rock, can activate the primary reward or primary threat circuitry of the brain (that is, fight or flight).
According to Rock,17 each of these domains, when rewarded, can promote engagement and a psychological “towards state”, and when threatened can trigger a psychological “away state”, or disengagement. Table 2 lists the five domains and their descriptions.
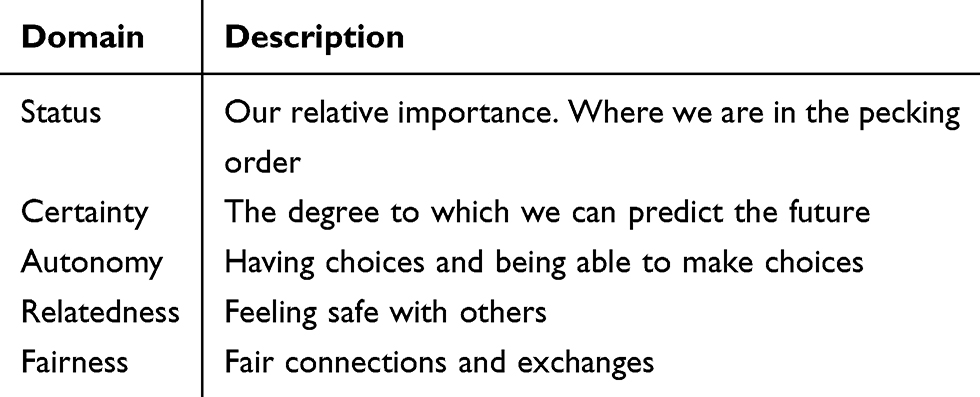 |
Table 2 SCARF Framework |
It is not the intention of the authors to examine the framework in detail or offer a review of its validity. However, the project team found this framework offered an easy to use, intuitive and practical heuristic for the facilitation of the work done.
Some simple examples of the way the project team incorporated SCARF into the project included: wherever possible staff were spoken to face-to-face rather than via email or telephone. All staff were greeted individually as they attended a group session. In this way, the message was conveyed, “We believe you are an important colleague in this project and we want talk to you personally” (Status and Relatedness rewards). Staff were also given prior notice of meetings and group sessions and what was hoped to be achieved was clearly outlined, with limitations clearly spelt out (we could not redesign the physical environment of the unit, for example). The project team was also careful to outline the program so that staff knew what to expect (Certainty reward) and could choose to attend or not without any repercussions (Autonomy reward). Staff were also given the opportunity to comment upon, alter and add to, the group processes (CCI and World Café) used (Autonomy reward). Every group session began with an introductory exercise, in order to promote a sense of us being more similar to each other than different (Relatedness reward). The degree to which each group member participated was up to them (Autonomy reward). Finally, processes were put in place to ensure the contributions of all staff, regardless of rank or role, were treated equally (Fairness reward).
Having trialled the SCARF framework while facilitating the group processes described above, the project team felt that SCARF also provided a potential heuristic framework for the day-to-day encounters between staff and staff, and staff and consumers, which would assist in the relational elements of these daily interactions and be compatible with TICP principles.
Discussion
As research into the link between the prevalence of exposure to trauma and negative long-term mental health outcomes becomes stronger, it is important for mental health services to become more trauma-informed.21 This project was based on the premise that any initiative to change practice to be more trauma-informed needed to use processes that in themselves reflected the principles of trauma-informed care.8 Using such a parallel process conveyed our commitment to TICP and the principles of safety, trustworthiness, choice, collaboration and empowerment.
However, designing an effective project that also reflected these principles required more than the simple use of the principles as a template. It required the application of processes that were, first and foremost, designed to bring about collaborative, inclusive, participatory and effective practice changes that were also TICP-compatible.
The positively framed, no-blame design of the BEET tool assisted the staff to engage collaboratively in the project.12 The application of the Claims, Concerns and Issues (CCI) focus groups empowered the staff to identify strengths as well as issues of concern.14 The World Café16 assisted staff to have a choice in identifying the issues to be address and the solutions to be implemented. The heuristic framework of SCARF17 used in the facilitation of the group processes, engendered ongoing engagement throughout the project. Overall, the application of these person-centred practice change methods and processes instilled a sense of safety and trustworthiness in the project as evidenced by the high level of staff engagement in all the elements of the project.
This paper is not intended to be a recipe for TICP practice change. It is offered here, however, in the hope that the methods, frameworks and processes described may be adapted to be of practical use in the design of TICP and other practice change initiatives in other mental health settings. The project generated practical solutions to the identified issues. Whilst examples of these have been highlighted in this paper, the solutions generated are, understandably, context-specific. They are not necessarily transferable to other contexts. However, we believe the methods, processes and frameworks used in the project are. The emphasis of this paper has therefore been on the processes rather than the solutions. This is in keeping with the adage “ … solutions do not solve problems, people do. Even the best solutions cannot work if the people involved do not support them”.12 One final outcome of this project has been that the project team feel confident that some of the same processes can be used in the next part of the project; to engage with consumers about trauma-informed care.
Conclusion
Histories of abuse and trauma are very common in those who experience mental illness, and staff working in the sector must be able to understand the effects of abuse and trauma and be able to respond to them appropriately.11,19 This approach is especially important in inpatient mental health units where the biomedical paradigm tends to dominate, where power imbalances are high, and where the risk of re-traumatisation is also high.2–5 The principles of TICP can be successfully introduced into inpatient units using methods that reflect TICP principles, particularly the active involvement of staff, with respect to engagement, and the identification of both relevant issues and solutions. All processes used should mirror the five principles of TICP: safety, trustworthiness, choice, collaboration and empowerment. Organisational support is necessary with respect to the necessary culture and the training required, and with respect to resource provision.
This project was borne out of a desire of a group of multidisciplinary staff to embed TICP principles in everyday practice. It was obvious to the team that the commonly used “top down” approach to practice change9,12 would be incongruent with the five principles of TICP: safety, trustworthiness, choice, collaboration and empowerment. However, practice development methodology, methods and processes described here mirrored trauma-informed care practice principles and were successful in maintaining a high degree of staff engagement and provided practical person-centered processes which generated collaboratively derived solutions to practical issues.
The principles of TICP can be successfully introduced into inpatient units using methods and processes that reflect TICP principles, particularly the active involvement of staff, with respect to engagement, and the identification of both relevant issues and solutions. We hope that by detailing the methods and processes we used, other clinical teams may be able to adapt these methods for other clinical practice change puzzles in other contexts.
Acknowledgments
The authors would like to acknowledge the Tasmanian Health Service for providing funding for the trauma-informed care training, and the Blue Knot organisation for providing the training. We would also like to thank the multidisciplinary staff for their participation and the project team. In particular, we would like to acknowledge Deb Hewson whose energy and commitment helped drive the project forward.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Blue Knot Foundation (2019) Trauma informed practice: blue knot foundation factsheet for workers in diverse service settings. Available from: blueknot.org.au
2. Mueser KT, Goodman LB, Trumbetta SL, et al. Trauma and post-traumatic stress disorder in severe mental illness. J Consult Clin Psychol. 1998;66(3):493–499. doi:10.1037/0022-006X.66.3.493
3. Zammit S, Lewis C, Dawson S, et al. Undetected post-traumatic stress disorder in secondary-care mental health services: systematic review. Br Psychiatry. 2018;212(1):11–18. doi:10.1192/bjp.2017.8
4. Cusack KJ, Grubaugh AL, Knapp RG, et al. Unrecognised trauma and PTSD among public mental health consumers with chronic and severe mental illness. Community Ment Health J. 2006;42(5):487–500. doi:10.1007/s10597-006-9049-4
5. Read J, Goodman L, Morrison AP, et al. Childhood trauma, loss and stress. In: Read J, Mosher LR, Bentall RP, editors. Models of Madness: Psychological, Social and Biological Approaches to Schizophrenia. East Sussex, UK: Routledge; 2004:223–252.
6. Moskowitz A, Schafer I, Dorahy MJ. Psychosis, Trauma and Dissociation: Emerging Perspectives on Psychopathology. West Sussex, UK: Wiley-Blackwell; 2019.
7. Manley K, McCormack B, Wilson V. Introduction. In: Manley K, McCormack B, Wilson V, editors. Practice Development in Nursing: International Perspectives. Oxford: Blackwell; 2008:1–16.
8. McAllister M. Solution Focused Nursing: Rethinking Practice. Gordonsville, VA: Palgrave Macmillan; 2006.
9. Walsh KD, Moss C, Lawless J, et al. Puzzling practice: A strategy for working with clinical practice issues. Int J Nurs Pract. 2008;14(2):94–100. doi:10.1111/j.1440-172X.2008.00671.x
10. Walsh K, Ford K, Morley C, et al. The development and implementation of a participatory and solution-focused framework for clinical research: a case example. Collegian. 2017;24(4):331–338. doi:10.1016/j.colegn.2016.06.003
11. Walsh KD, Crisp J, Moss C. Psychodynamic perspectives on organisational change and their relevance to transformational practice development. Int J Nurs Pract. 2011;17(2):205–212. doi:10.1111/j.1440-172X.2011.01926.x
12. Walsh KD, Lawless J, Moss C, et al. The development of an engagement tool for practice development. Pract Devel Health Care. 2005;4(3):124–130. doi:10.1002/pdh.7
13. Benjamin R, Haliburn J, King S. Humanising Mental Health Care in Australia: A Guide to Trauma-Informed Approaches. London, UK: Routledge; 2019.
14. Guba EG, Lincoln YS. Fourth Generation Evaluation. Newbury Park, CA: Sage; 1989.
15. Walsh KD, Moss C and FitzGerald M. Solution-focused approaches and their relevance to practice development. Pract Devel Health Care. 2006;5(3):145–155. doi:10.1002/pdh.192
16. Tan S, Brown J. The world Café in Singapore: creating a learning culture through dialogue. J Appl Behav Sci. 2005;41(1):83–90. doi:10.1177/0021886304272851
17. Rock D. SCARF: A brain-based model for collaborating with and influencing others. NeuroLeadershipJournal. 2008;1:1–7.
18. Berne E. Games People Play: The Psychology of Human Relationships. New York, NY: Ballantine; 1964.
19. Rock D, Cox C. SCARF in 2012: updating the social neuroscience of collaborating with others. Neuro Leadership J. 2012;4:1–14.
20. Cucuzzella C. Why is fourth generation evaluation essential for sustainable design? Design Principles Pract. 2011;1(5):239–251. doi:10.18848/1833-1874/CGP/v05i01/38014
21. Muskett C. Trauma-informed care in inpatient mental health settings: a review of the literature. Int J Ment Health Nurs. 2014;23:51–59. doi:10.1111/inm.12012
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.