")
Back to Journals » Open Access Emergency Medicine » Volume 13
USER Protocol as a Guide to Resuscitation of the Patient with Septic Shock in the Emergency Department
Authors Devia Jaramillo G , Menendez Ramirez S
Received 29 October 2020
Accepted for publication 14 December 2020
Published 12 February 2021 Volume 2021:13 Pages 33—43
DOI https://doi.org/10.2147/OAEM.S289148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
German Devia Jaramillo,1 Salvador Menendez Ramirez2
1Resuscitation Unit, Hospital Universitario Mayor Méderi; Department of Emergency Medicine-Internal Medicine, School of Medicine and Health Sciences, Universidad del Rosario, Bogotá, Colombia; 2Department of Emergency Medicine, School of Medicine and Health Sciences, Universidad del Rosario, Bogotá, Colombia
Correspondence: German Devia Jaramillo
Hospital Universitario Mayor Méderi, Cra. 24 No. 29-45 Research Office, Bogota, 111411, Colombia
Tel +571 5600520 ext 3961-3987
Email [email protected]
Introduction: Sepsis is a disease that is still associated with high mortality, in which timely interventions are related to better results.
Objective: To determine if there is a difference in in-hospital mortality, fluid balances, norepinephrine initiation and recovery time of blood pressure, when comparing the resuscitation of the patient who is admitted to the emergency room in septic shock by applying the ultrasound protocol (USER) versus the standard of care.
Patients and Methods: This is a prospective, cohort study conducted in the emergency room of a highly complex hospital of patients with septic shock.
Results: 83 patients recruited in total. The groups were comparable in demographics, mean baseline blood pressure, disease severity given by the SOFA value, and arterial lactate. A statistically significant difference was documented in the fluid balances at 4 hours, median 1325mL (IQR:451– 2455mL) in Group C versus 900mL (IQR:440– 1292) in Group U (p=0.048) and at 6 hours, median 1658mL (IQR:610– 2925mL) versus 1107mL (IQR:600– 1500mL), p=0.026, as well as in the total fluid balance of hospital stay, median 14,564mL (IQR:8660– 18,705mL) versus 8660mL (IQR:5309– 16,974mL), p=0.049. On the other hand, in the USER Group, the mean blood pressure ≥ 65mmHg was achieved in 97.4% of the patients 4 hours after the start of the protocol versus 50% in Group C (p=< 0.001). Mortality with the use of the protocol compared with conventional therapy was (56.4% vs 61.36%, p=0.647).
Conclusion: The use of the USER protocol in patients with septic shock in the emergency room showed lower fluid balances at 4 and 6 hours, and of the total hospital stay, as well as earlier initiation of norepinephrine and statistically significant faster improvement in blood pressure. Although a statistically significant difference was not found in the days of ICU stay, hospitalization and in-hospital mortality, a trend was observed in the reduction of these parameters.
Keywords: septic shock, emergency medicine, resuscitation, bedside ultrasound, fluid responsiveness, passive leg raising, goal-directed therapy, Doppler snuffbox resistance index
Introduction
Sepsis is a disease of high mortality that varies according to some studies between 18%1,2 and 55%.3 In the emergency room, the delay in adequate and timely care of these patients is related to the increase in mortality.4
Since the protocol was carried out “Early Goal-Directed Therapy in The Treatment of Severe Sepsis and Septic Shock”5 to date, there is no protocol that has conclusively demonstrated reduced mortality in patients with septic shock in the emergency room, and even one goal-driven strategy has not been shown to be superior to another.6 However, what is clear is that, since resuscitation protocols have been developed, their application has shown reduced mortality.7
Bedside ultrasound in the emergency room has proven to be a useful tool in the assessment of critically ill patients8 and it is even of great help in pathologies such as dyspnea,9,10 shock of unclear etiology11 and cardiac arrest,12 among others. Specifically, in resuscitation of the patient with septic shock, there is literature showing that ultrasound may be used to help search for the possible site of infection, guide fluid administration, document cardiac dysfunction, help monitoring some treatments, and may even be helpful as support in bedside procedures.13
Current guidelines recommend the initial administration of 30 cc per kg of bolus crystalloid fluids in order to improve organ perfusion.14 However, unnecessary fluid loads may have an association with the development of disorders such as non-cardiogenic pulmonary edema (ARDS).15 Additionally, abnormally high fluid balances are related to increased patient mortality.16 For this reason, strategies should be created for the administration of fluids, individualized to the patients´ needs using predictors of response to fluids,17 some of these with applicability in the emergency room, but others less so.18,19 In general, predictors using bedside ultrasound as a key tool may be useful in the emergency room,20 since they are relatively easy and quick to use. Passive leg rising with ultrasound cardiac output measurement may be an option for predicting volume response in the emergency room.21 This measurement may be done using several techniques,22,23 among them, the indirect cardiac output calculation using the Doppler carotid artery flow, which is attractive due to the comfort and relative ease.22,24–26
On the other hand, the administration of vasopressors should be timely. The current recommendation is that they should be initiated in the event that there is no response to fluid volume to improve blood pressure.27 However, according to some studies, the early administration of vasopressors seems to have better results in terms of mortality.28,29 This leads to an imperative question: When should vasopressors be initiated, and even when should fluids only be administered? Even, why not to administer fluids and vasopressors simultaneously from the beginning?. Recently, the relationship between the Doppler measurement of the radial artery at the level of the anatomic snuffbox and the systemic vascular resistance has been demonstrated,30,31 which means that, in the emergency room, the measurement of the resistance index of the radial artery at the level of the anatomic snuffbox may be used as an indicator of the need to start vasopressor support early, since it could reflect a deterioration of the systemic vascular resistance as an explanation for the patient’s arterial hypotension.
Based on these observations, this study proposes an ultrasound-based protocol to determine the amount of fluids to be administered and the time to initiate vasopressor support in the patient with septic shock in the emergency room.
The objective of this study is to determine if there is a difference in in-hospital mortality, when comparing the resuscitation of the patient who is admitted to the emergency room in septic shock using the ultrasound protocol (USER), compared to the standard of care (C). Additionally, to evaluate if there is a difference in the recovery time of mean blood pressure, fluid balances, time of initiation of vasopressor support, days of ICU stay, and hospital stay, when the resuscitation of the patient entering the emergency room in septic shock is compared according to the sepsis-3 definition, using the ultrasound protocol (USER), compared to the standard of care (C).
Patients and Methods
Research Design Type and Study Site
This is a prospective, cohort study conducted in the emergency room of the Hospital Universitario Mayor Méderi. This highly complex university institution attends 238,000 consultations annually in its adult emergency department, who are treated in 110 observation beds, of which 15 correspond to the adult resuscitation room.
Data Source and Participants
Inclusion Criteria
The inclusion criteria were adult patients aged over 18 years assisted at the hospital resuscitation service during the period between August 2019 and January 2020, with a diagnosis of septic shock, including patients with chronic liver and kidney disease. Patients referred to other institutions or who had incomplete data in medical records were excluded. During the above-mentioned study period, the sample was selected in a continuous sequential manner.
Based on the sepsis-3 consensus,32 confirmation of the diagnosis of septic shock was made in patients who had suspected or confirmed infection plus organ dysfunction documented by a SOFA score (sequential organ failure assessment score) ≥ 2, mean blood pressure less than 65 mmHg with arterial lactate ≥ 2 mmol/L and required vasopressor support to improve blood pressure.32
The variables used were demographics (age, gender), site of infection; mean blood pressure, fluid balance, initiation time and days of use of norepinephrine, vasopressin, dopamine, dobutamine, epinephrine; hydrocortisone use, antibiotic start time, surgical pathology, SOFA score, and arterial lactate; days of hospital stay, days of ICU stay, and in-hospital mortality.
USER Protocol
The protocol Bedside Ultrasound in Septic shock for Emergency department Resuscitation (USER) [Bedside Ultrasound in Septic Shock for Emergency Department Resuscitation], consists of using tools based on bedside ultrasound findings with septic shock, in order to determine the strategy to improve blood pressure using or not using fluids and associating them or not with vasopressors. The main objective of this protocol is to determine the most appropriate initiation time for vasopressor support, regardless the amount of fluids administered to the patient.
The protocol is described in Figure 1. Patients who entered the resuscitation room in shock were initially given an initial bolus of 30 cc/kg body weight of crystalloid fluids, and during this period, patients were monitored in a minimally invasive way with blood pressure control, continuous electrocardiographic activity, oxygen saturation, urinary output, and central venous line. Additionally, routine paraclinical evaluations were taken. Patients who recovered blood pressure with the initial bolus were excluded from the study because they did not meet the definition of septic shock. If the patient persisted with arterial hypotension, the first USER protocol ultrasound was performed, a passive leg rising (PLR) test by Doppler-guided carotid flow test (PLRcD) was carried out and, if positive, another dose of 500 cc of liquids was scheduled. In parallel, a measurement of Doppler snuffbox resistance index (DSIR) was performed and, if the value was less than 0.9, it was considered positive and vasopressor support was started immediately with low-dose norepinephrine (initially 0.05 µg/kg/min, but that would be titrated as found in the protocol). The protocol was repeated every two hours for the first 6 hours or until a goal of mean blood pressure ≥ 65 mmHg was achieved. Subsequently, all patients received standard of care, many of them in the ICU.
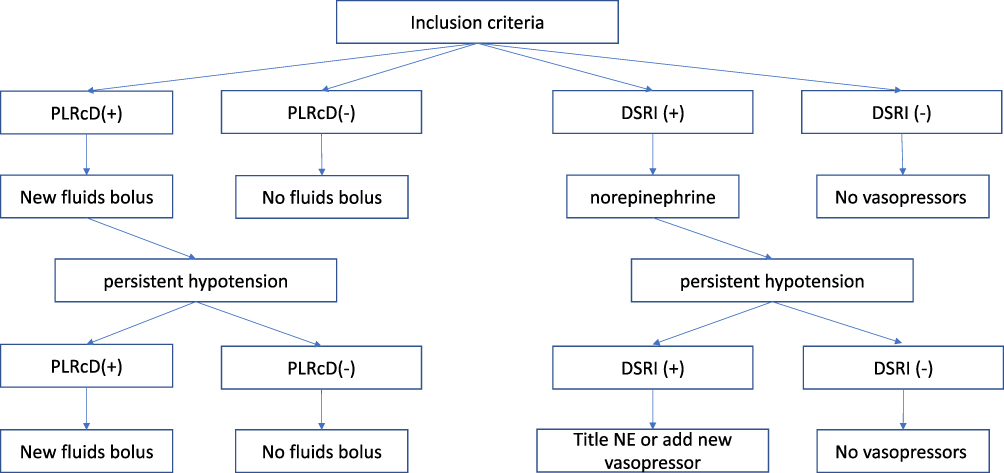 |
Figure 1 U.S.E.R protocol. U.S.E.R: Bedside Ultrasound in Septic Shock for Emergency department Resuscitation. Abbreviations: PLRcD, passive leg raising for carotid Doppler; DSRI, Doppler snuffbox resistive index; NE, norepinephrine. |
Ultrasound Measurements
All measurements were made with a 7.5 MHz linear array transducer probe connected to a real-time ultrasound scanner (Sonosite M-Turbo P08792/P09823).
Passive Leg Rising by Doppler-Guided Carotid Flow Technique
The PLRcD was performed similarly as published in previous articles.25 PLRcD was considered positive for response to fluids if the carotid flow improved 20% with respect to the baseline value after 90 seconds of lower limb elevation (Figure 2A).
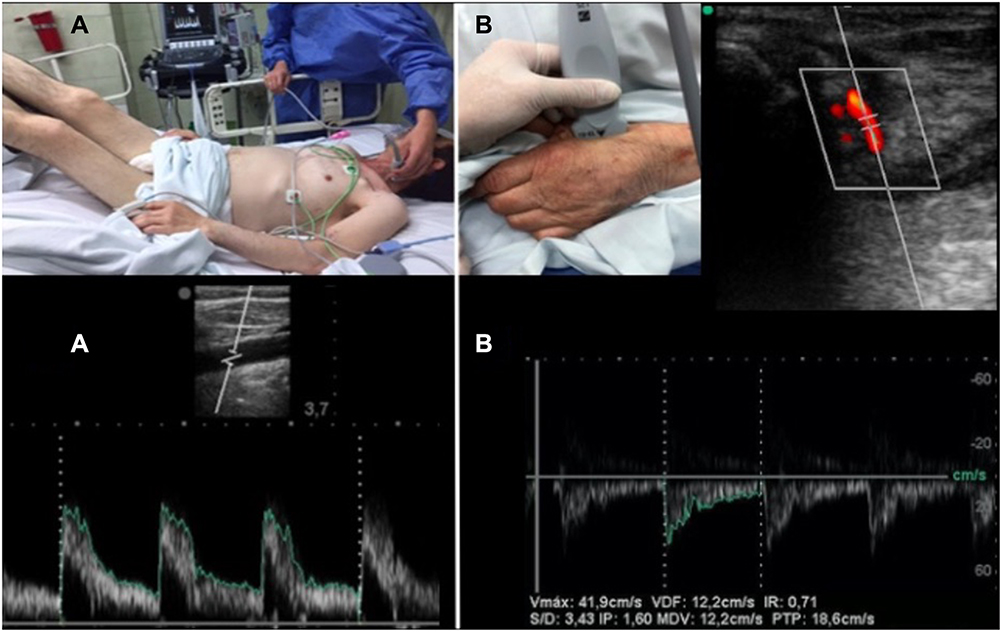 |
Figure 2 The U.S.E.R, ultrasound measurements. Notes: (A) Passive leg raising for carotid Doppler flow technique. (B) Doppler snuffbox resistive index technique. |
The carotid images were performed by a team of emergency medicine specialists with training in ultrasound. To measure the Doppler flow of the carotid artery, an image of the common carotid artery was initially taken in a short axis, then the transducer was rotated 90 ° until a long axis was achieved, the image of the artery was followed up to the carotid bulb and Approximately one centimeter from the bulb, the diameter of the intima of the artery was measured in centimeters, once an adequate visualization of the vessel was obtained, the pulsed Doppler was run in the middle of the artery perpendicular to the flow (Figure 2A) and the velocity-time integral in centimeters was automatically determined through digitized Doppler spectral envelopes, with the sample obtained in the middle of the artery. The blood flow per minute was automatically determined by software included in the ultrasound equipment.
Doppler Snuffbox Resistance Index Technique
For DSRI, the technique described in previous articles was applied.30,31 During the limb elevation time, the DSRI was calculated and considered positive as an indicator of low systemic vascular resistance when its value was less than 0.9 (Figure 2B).
Conventional Treatment
Patients who were not resuscitated according to protocol U were treated by emergency room physicians according to current institutional guidelines adapted from the international recommendations set forth in “Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012”.
Cohort Collection Method
Patients who consulted the emergency room during the study period were admitted to the study group (case) depending on whether the team that knew the protocol was available at the time of septic shock identification upon admission to the emergency room. If not available, the patient would be managed according to the standard of care and would be part of the control group. The sample collection period was terminated earlier than expected due to the difficulty in collecting patients secondary to the pandemic that started in 2019.
Statistical Analysis
The information recorded in the collection tool was reviewed to avoid inconsistencies or duplications, it was verified that the data recorded corresponded to each type of variable. Inclusion and exclusion criteria were applied.
It began with a descriptive analysis of the variables under study. For categorical variables, frequency distribution was performed, and for continuous variables, measurements of central tendency and dispersion were made according to the type of distribution (mean and standard deviation versus median and interquartile ranges [IQR] for normal or non-normal distribution, respectively), for which a normality test was applied (Shapiro Wilk). For the analysis of the collected sample, contrast testing hypothesis was applied according to the characteristics and distribution of the variables (T test, Kolmogorov Smirnov, X2).
All statistical calculations were performed using the STATA program, version 15, educational license from the Universidad del Rosario (StataCorp. 2009. College station, TX: StataCorp LP).
Ethical Aspects
The study was conducted in accordance with the Ethical Principles for Medical Research in Humans according to the Declaration of Helsinki - 59th General Assembly, Seoul, Korea, October 2008.
The local regulations of the Colombian Ministry of Health were taken into account according to Resolution 8430/1993, regarding Chapter I “On the Ethical Aspects of Research in Humans”.
This research is classified within the category “no risk”. Access to research instruments was limited only to investigators according to Article 8 of Resolution 008430/1993 by the Ministry of Health.
All patients admitted to emergency department signed a generic form (patient consent F-CME-22 V.0). They accepted and gave their written informed consent for the use and publication of their medical records for academic and research purposes.
It was the responsibility of the investigators to keep the information contained in the medical records with absolute confidentiality, and to comply with current regulations regarding its management, regulated by the following legislation: Law 100/1993, Law 23/1981, Decree 3380/1981, Resolution 008430/1993, and Decree 1995/1999.
All the members of the research group were ready to give information about the study to organized, approved and interested entities in knowing it, as long as they were academic and scientific in nature, preserving the accuracy of the results and referring to global data, and not to particular patients or institutions.
Absolute confidentiality will be maintained and the good professional institutional name will be preserved.
The study was carried out with impartial and responsible statistical management. The study design was reviewed and approved by the Hospital Research Committee.
Results
During the study period, a total of 83 patients were included, 44 of which were managed with the standard of care, and 39 with the USER protocol. No statistically significant differences were found in terms of age and sex. The patients’ disease severity was similar as found in the SOFA score and lactate at admission. Additionally, no difference in antibiotic initiation time or steroid use was found. In particular, there was no statistically significant difference in mean blood pressure at patient admission. The most frequent sources of infection were pulmonary, urinary, and gastrointestinal (Table 1).
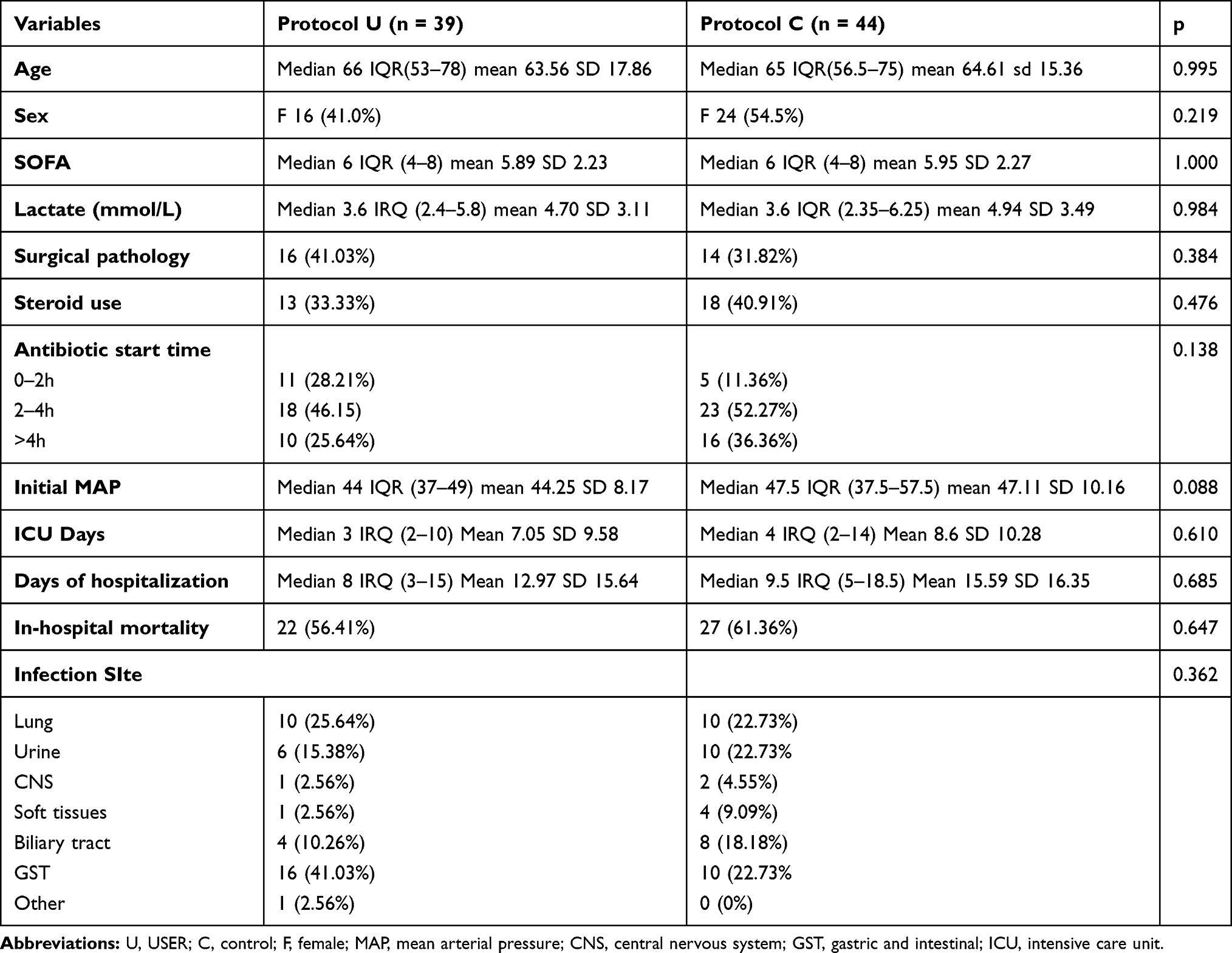 |
Table 1 Population Characteristics |
Regarding the fluid balances, statistically significant differences could be documented at 4 and 6 hours, and in the total hospital stay (Table 2). No statistically significant difference was found in the fluid balances of the groups in the first hour (p = 0.110) and at 2 hours (p = 0.07). After 12 hours, no significant difference was documented in the fluid balance (p = 0.110), as well as at 24 hours (p = 0.255), 48 hours (p = 0.493) and 72 hours (p = 0.264).
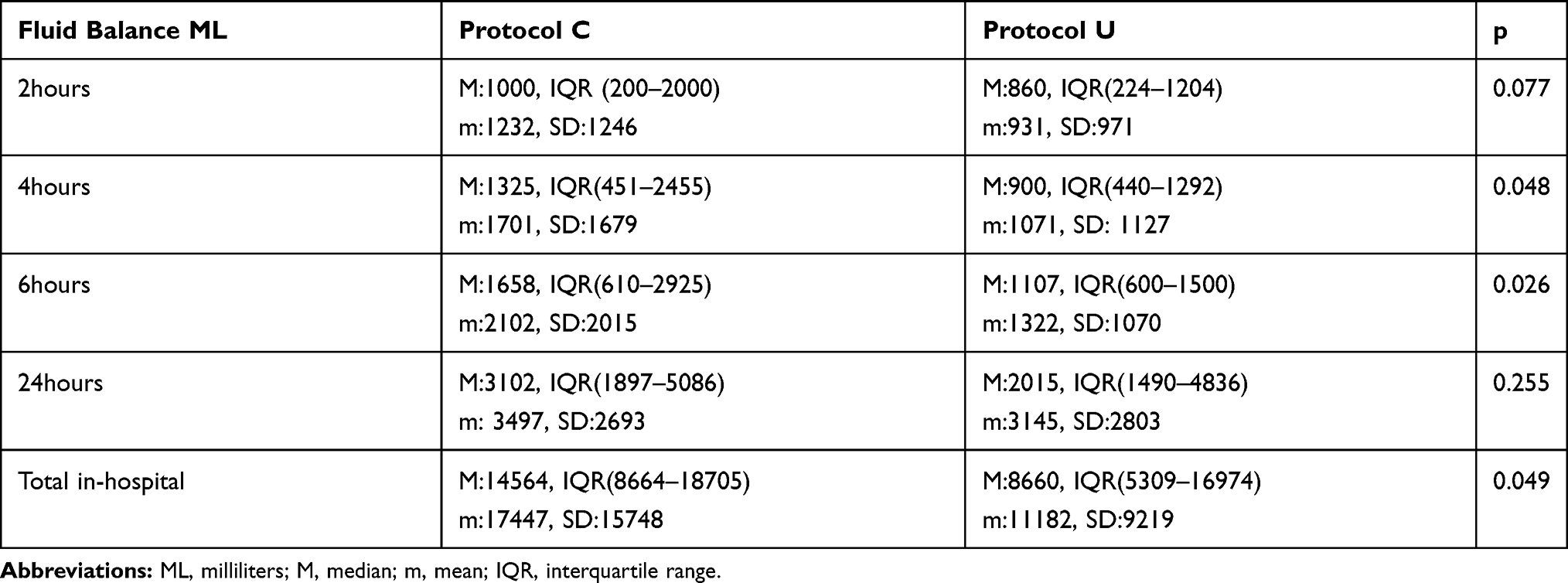 |
Table 2 Relevant Fluid Balance |
Likewise, when reviewing the behavior of the use of vasopressors, it was documented that there is a significant difference in the initiation time of norepinephrine, thus an earlier onset could be established in the USER group. When compared to the control group (p = < 0.001), it was documented that, 3 hours after onset of resuscitation in the study group, 53.3% of patients already had norepinephrine started compared to 18.8% of the control group. Similarly, at 6 hours, 100% of the patients in the USER group was on norepinephrine, while 90.9% of the control group were on that vasopressor support. However, no significant difference was found in the number of days of norepinephrine use (p = 0.99), nor was there a difference in the initiation time of vasopressin (p = 0.170), nor in the days of vasopressin use (p = 0.527). Only in one patient during the study, dopamine was used, thus no significant difference was found in the groups (p = 0.285). Additionally, no difference was found in dobutamine initiation time between the groups (p = 0.264), nor in the days of use of this inotropic drug (p = 1000). There was also no statistically significant difference in epinephrine initiation time (p = 0.402), and epinephrine use time (p = 0.964).
A statistically significant difference was found in terms of time to achieve control of mean blood pressure. It was established that in the USER group it was possible to achieve the objective more quickly (≥ 65 mmHg), faster than in the control group, there was a difference in mean blood pressure of the groups at two hours (p = 0.02), four hours (p = <0.001), and six hours (p = 0.001) (Table 3).
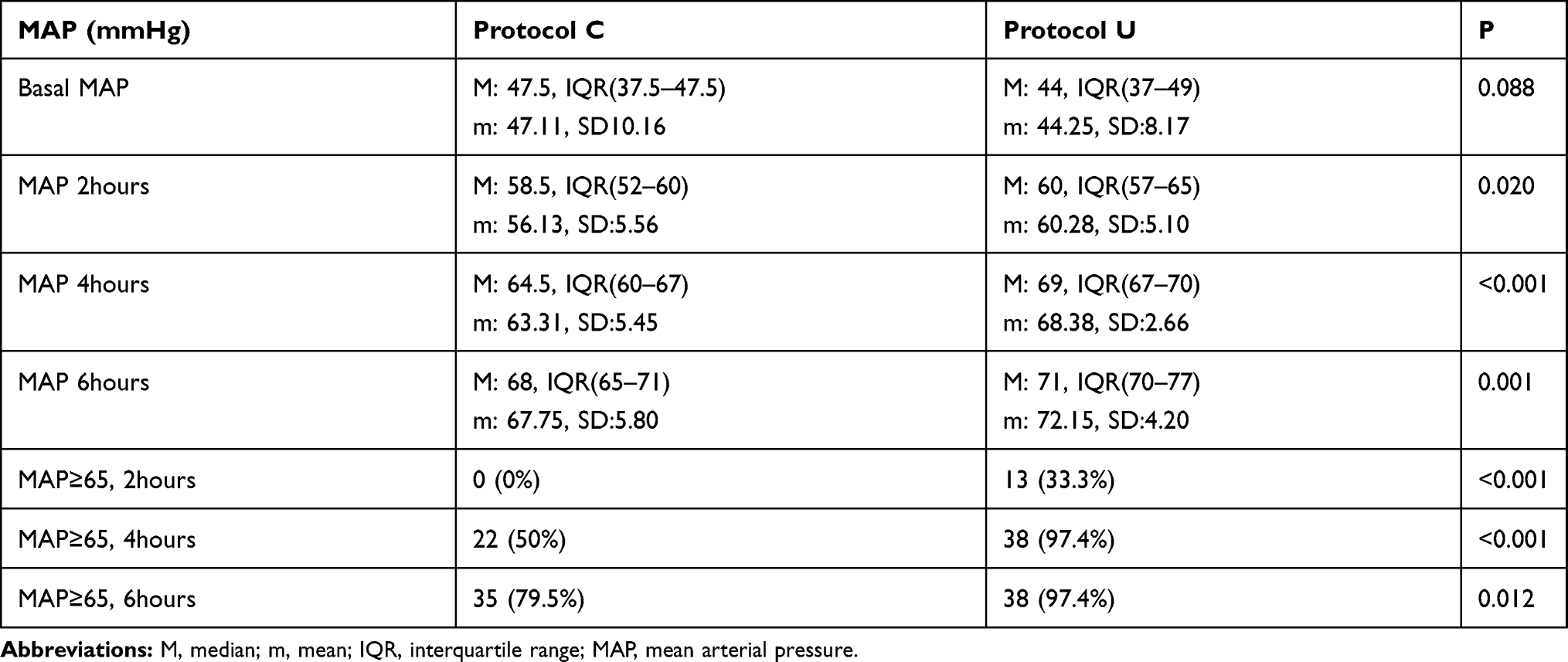 |
Table 3 Behavior of Mean Arterial Pressure According to Each Protocol |
Finally, regarding the days of ICU stay, no significant difference was found between the groups (p = 0.610), nor in the days of hospital stay (p = 0.685), and especially, a statistically significant difference in mortality of the two groups could not be documented (p = 0.647) (Table 1).
Discussion
Managing arterial hypotension of the patient with septic shock in the emergency room is challenging. This work aims to provide a tool using ultrasound so that the clinician can use either fluid administration or vasopressors or both, in a more objective and non-empirical manner, in order to alleviate arterial hypotension in a timely manner and without increased side effects.
The number of patients recruited in the study was 83. The inclusion of patients had to be terminated early due to the pandemic that started in February in the country, since the usual routes of admission were affected and this could confuse the inclusion variables. Having said that, 39 patients were recruited in the study group, and were compared to 44 patients who formed the control group. However, it was possible to document that groups were comparable in terms of the severity of the condition indicated by the SOFA score and arterial lactate measured upon admission to the emergency room. Likewise, it was possible to determine that they were comparable in terms of age, sex and focus of infection, and it was also documented that there was no difference in the groups in terms of patients with surgical pathology and, additionally, the foci of infection between the groups were similar, consequently cases and controls could be compared.
Early antibiotic initiation in the emergency room when treating septic patients has been shown to decrease mortality.33 Hence, it is important to note that the speed in the administration of antibiotics in the study group was not the best, since it was documented that only approximately half of the group started antibiotics in the first 4 hours. This could have affected the mortality outcome of the entire population, and could have been a confounding factor. However, this factor did not affect the comparison of the two study groups, since no differences in the antibiotic administration time were found between cases and controls.
The use of steroids in patients with septic shock is a widely discussed subject, and so far, there is no definitive conclusion. However, it seems that it is a good idea in patients with suspected refractory shock, since it could help in the quicker resolution of arterial hypotension.34 The use of hydrocortisone in the study group was around 40%, which apparently may be related to the severity of shock of the patients in the analysis, which may also be related to the high mortality found. However, it was not considered a confounding factor between the groups, since no differences were found between cases and controls analyzed in this study.
One of the study objectives was to determine which patient benefited from the administration of fluids, in order to improve blood pressure, and secondarily, cell perfusion without harm, since it is known that abnormally positive fluid balances are related to adverse outcomes and increased mortality.15,16 Therefore, there are studies that seek to determine if the use of dynamic variables of response to fluids in critically ill patients may help to reduce the administration of unnecessary fluids significantly.35 There are multiple dynamic variables to determine the response to fluids18 in the emergency room, based on the conditions of the service, the inferior cava vein compliance or collapse index may be used, or the PLR test may also be used. However, in a recent meta-analysis,36 it was determined that the variation with respiration of the inferior cava vein has a poor prognostic performance. Thus, the PLR test was considered to predict fluid response in the study group.
There are several ways to assess the change in cardiac output with PLR,37 the most widely used is by minimally invasive monitoring of direct measurement of cardiac output. However, this is difficult in the emergency department, since it requires specific monitoring and is usually not available in emergency rooms. Thus, bedside ultrasound may be used: one way is the PLR test guided by changes in cardiac output, minimally invasively assessing changes in the velocity time integral of the left ventricular outflow tract with proper results.17 However, it was also possible to determine that the PLR may be guided by changes in the peak velocity of the carotid,25 finding acceptable predictive indexes. However, there is literature that does not support the latter method;38 nevertheless, this last study has many limitations, since it is a study with few patients, and the measurements were not very easy to perform, apparently due to the characteristics of the population. In the studied population, it was technically easier to visualize the flow of the carotid than left ventricular flow. Hence, it was decided to use PLR guided by changes in the peak velocity in the carotid as a predictor of response to fluids.
The findings of this study regarding the prediction of response to fluids were interesting: It was possible to document a significant difference in the fluid balances at 4 and 6 hours of stay in the emergency room, thus probably preventing the unnecessary administration of fluids. Initially, both groups received similar volume loads with a balance of approximately 1 liter in both groups. However, it was determined that, at 4 hours, the study group had around 300 to 700 mL less fluid balance, constituting a significant difference between the two groups. Additionally, at 6 hours it was shown that the study group had around 500 to 1000 mL less positive fluid balance compared to the control group, constituting a significant difference and probably avoiding exposure to dangerously positive fluid balances. Finally, it was documented that, in the total hospital stay, the study group had significantly lower fluid balances than the control group, which is probably due to the more conservative administration of fluids during the first 6 hours of resuscitation. This demonstrates that having an objective strategy of fluid administration in resuscitation allows lower fluid balances and probably less risk of fluid overload.
The initiation of vasopressor support is decisive for the control of arterial hypotension of the patient with septic shock. The most commonly used vasopressor for this purpose is currently norepinephrine.27 However, the timing of norepinephrine initiation during the resuscitation process of the patient with septic shock is not entirely clear yet, and there is literature suggesting that early initiation of norepinephrine may be associated with lower fluid requirements and a faster recovery of blood pressure, probably contributing to the improvement of clinical outcomes.39
In general, in the patient with septic shock, vasopressors improves the systemic vascular resistance that is presumed to be decreased. It would be ideal to be able to directly measure this variable. However, in emergency rooms, this monitoring is not routinely available. Thus, alternatives to measuring vascular resistance in a minimally invasive manner should be found. An alternative is the one described in several articles in which an association could be determined by measuring the resistance index of the snuffbox by Doppler and systemic vascular resistance.30,31 Therefore, our study used this variable to decide on the initiation of norepinephrine support. By applying the technique of measuring the resistance index of the snuffbox by Doppler, a statistically significant difference could be found at the beginning of norepinephrine support in the study group compared to the control group. It was documented that all patients who were included in the USER group had been administered norepinephrine within 6 hours of admission to the emergency department, and even within 2 hours, 30.7% of the group had already started this support. This, then, might improve the perfusion pressure of the organs, probably faster than in the control group. The use of norepinephrine early in critically ill patients shows to be a safe intervention with the benefits of achieving an improvement in blood pressure.39
The use of vasopressin is recommended in the resuscitation guidelines of the patient with septic shock that does not improve with the initial administration of norepinephrine.40 During the study, it was documented that some patients in both groups required the use of vasopressin. However, no significant difference was found, probably secondary to the small sample (12 patients in the control group and 14 patients in the USER group), and also, because probably both groups of treating physicians considered using vasopressin only in case the patient was in shock refractory to the use of norepinephrine.
Furthermore, dopamine was not used during the study, probably due to the recommendations in the literature.40 Only 4 patients in the population required the use of epinephrine as adjuvant therapy, which did not allow a comparison analysis between cases and controls. Thus no differences were found in the use or duration of this vasopressor.
The initiation of inotropic therapy is recommended when documenting cardiac dysfunction as a cause of poor cell perfusion, despite recovery of blood pressure.41 During the study, it was possible to document that 9 patients of the USER protocol required this medication compared to 6 patients in the control group. However, no differences were found in the initiation time or in the duration of therapy. This data is interesting, given that the USER protocol does not contemplate the use of inotropic drugs, since it does not include the assessment of cardiac function for the improvement of blood pressure. It is probably interesting to include in a future study the early assessment of cardiac function at bedside, to define the early onset of inotropic drugs. However, this discussion is beyond the scope of this paper.
An interesting fact provided by this study was that, when the USER protocol is applied, a faster improvement in blood pressure is achieved. It was determined that 97.4% of the study group had a mean blood pressure ≥ 65 mmHg 4 hours after the start of resuscitation, while only 50% of the control group had achieved this goal, and only up to 6 hours, 79.5% of the control group had achieved a statistically significant difference. This data is worthwhile noting, since it has been shown that the delay in the improvement of blood pressure is related to the increase in mortality in patients with septic shock.42,43
Finally, regarding the outcome of the patients when they are resuscitated in the first 6 hours with the USER protocol compared to the standard of care, it was possible to document that the patients to whom the study protocol was applied had fewer days of ICU stay, as well as fewer days of hospital stay. However, these data were not statistically significant. Additionally, it was possible to document a difference in mortality of the two groups: 56.4% for the USER protocol and 61.3% for the control group. This difference was not statistically significant, although it does establish that there is a tendency to decrease mortality when following a protocol that, using objective measurement variables, allows the clinician to decide with a better physiological basis on the use of fluids and/or vasopressors for the management of arterial hypotension in the patient with sepsis. It is likely that the difference was not statistically significant due to the small number of study participants, so a study with a larger sample was left open.
Limitations
Sample size calculation was not performed, which could alter the statistical validity of the study. However, the results in the analyzed population justify a study with a better epidemiological design.
As it was an observational study, the USER protocol was not randomized. It was only performed at certain times of the day, since the protocol is known only to a group of doctors and is not a protocol that is routinely performed in the hospital. However, there were no significant differences between the patients in both groups, which made them comparable. Additionally, performing the protocol requires ultrasound training and Doppler techniques that, although simple, not all ultrasound personnel are used to do.
Conclusion
The use of the USER protocol in patients with septic shock in the emergency room showed lower fluid balances at 4 and 6 hours and the total hospital stay, as well as earlier initiation of norepinephrine and faster improvement in blood pressure in a statistically significant manner. Likewise, a trend was shown in the reduction of the days of ICU stay, hospitalization and in-hospital mortality. This shows that patients with septic shock should be resuscitated in the emergency room on a case-by-case basis and as objectively as possible.
However, a study with a larger sample and with a better epidemiological design is needed to conclusively demonstrate the benefit of this protocol over the standard of care.
Acknowledgment
To Zai and Tato for their patience and inspiration.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Peake SL, Delaney A, Bailey M, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371(16):1496–1506.
2. Yealy DM, Kellum JA, Huang DT, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683–1693.
3. Machado FR, Cavalcanti AB, Bozza FA, et al. The epidemiology of sepsis in Brazilian intensive care units (the Sepsis PREvalence Assessment Database, SPREAD): an observational study. Lancet Infect Dis. 2017;17(11):1180–1189.
4. Angus DC, van der Poll T. van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369(9):840–851. doi:10.1056/NEJMra1208623
5. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377. doi:10.1056/NEJMoa010307
6. Nguyen HB, Jaehne AK, Jayaprakash N, et al. Early goal-directed therapy in severe sepsis and septic shock: insights and comparisons to ProCESS, ProMISe, and ARISE. Crit Care. 2016;20(1):160.
7. Wira CR, Dodge K, Sather J, Dziura J. Meta-analysis of protocolized goal-directed hemodynamic optimization for the management of severe sepsis and septic shock in the Emergency Department. West J Emerg Med. 2014;15(1):51–59.
8. Whitson MR, Mayo PH. Ultrasonography in the emergency department. Crit Care. 2016;20(1):227.
9. Bekgoz B, Kilicaslan I, Bildik F, et al. BLUE protocol ultrasonography in Emergency Department patients presenting with acute dyspnea. Am J Emerg Med. 2019.
10. Lichtenstein DA. BLUE-protocol and FALLS-protocol: two applications of lung ultrasound in the critically ill. Chest. 2015;147(6):1659–1670. doi:10.1378/chest.14-1313
11. Bagheri-Hariri S, Yekesadat M, Farahmand S, et al. The impact of using RUSH protocol for diagnosing the type of unknown shock in the emergency department. Emergency Radiology. 2015;22(5):517–520. doi:10.1007/s10140-015-1311-z
12. Lalande E, Burwash-Brennan T, Burns K, et al. Is point-of-care ultrasound a reliable predictor of outcome during atraumatic, non-shockable cardiac arrest? A systematic review and meta-analysis from the SHoC Investigators. Resuscitation. 2019;139:159–166. doi:10.1016/j.resuscitation.2019.03.027
13. Shrestha GS, Srinivasan S. Role of Point-of-Care Ultrasonography for the Management of Sepsis and Septic Shock. Rev Recent Clin Trials. 2018;13(4):243–251. doi:10.2174/1574887113666180412165405
14. Seymour CW, Rosengart MR. Septic Shock: advances in Diagnosis and Treatment. JAMA. 2015;314(7):708–717. doi:10.1001/jama.2015.7885
15. Chang DW, Huynh R, Sandoval E, Han N, Coil CJ, Spellberg BJ. Volume of fluids administered during resuscitation for severe sepsis and septic shock and the development of the acute respiratory distress syndrome. J Crit Care. 2014;29(6):1011–1015. doi:10.1016/j.jcrc.2014.06.005
16. Boyd JH, Forbes J, Nakada T-A, Walley KR, Russell JA. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011;39(2):259–265. doi:10.1097/CCM.0b013e3181feeb15
17. Monnet X, Marik PE, Teboul J-L. Prediction of fluid responsiveness: an update. Ann Intensive Care. 2016;6(1):111. doi:10.1186/s13613-016-0216-7
18. Monnet X, Teboul J-L. Assessment of fluid responsiveness: recent advances. Curr Opin Crit Care. 2018;24(3):190–195. doi:10.1097/MCC.0000000000000501
19. Monnet X, Teboul J-L. Volume responsiveness. Curr Opin Crit Care. 2007;13(5):549–553. doi:10.1097/MCC.0b013e3282ec68b2
20. Maurer C, Wagner JY, Schmid RM, Saugel B. Die Bestimmung des Volumenstatus und der Volumenreagibilität in der Notaufnahme – ein systematischer Ansatz. Medizinische Klinik Intensivmedizin und Notfallmedizin. 2017;112(4):326–333. doi:10.1007/s00063-015-0124-x
21. Thiel SW, Kollef MH, Isakow W. Non-invasive stroke volume measurement and passive leg raising predict volume responsiveness in medical ICU patients: an observational cohort study. Crit Care. 2009;13(4):R111. doi:10.1186/cc7955
22. Peng Q-Y, Zhang L-N, Ai M-L, et al. Common Carotid Artery Sonography Versus Transthoracic Echocardiography for Cardiac Output Measurements in Intensive Care Unit Patients. J Ultrasound Med. 2017;36(9):1793–1799. doi:10.1002/jum.14214
23. Tan HL, Pinder M, Parsons R, Roberts B, van Heerden PV. Clinical evaluation of USCOM ultrasonic cardiac output monitor in cardiac surgical patients in intensive care unit. Br J Anaesth. 2005;94(3):287–291. doi:10.1093/bja/aei054
24. Gassner M, Killu K, Bauman Z, Coba V, Rosso K, Blyden D. Feasibility of common carotid artery point of care ultrasound in cardiac output measurements compared to invasive methods. J Ultrasound. 2015;18(2):127–133. doi:10.1007/s40477-014-0139-9
25. Marik PE, Levitov A, Young A, Andrews L. The use of bioreactance and carotid Doppler to determine volume responsiveness and blood flow redistribution following passive leg raising in hemodynamically unstable patients. Chest. 2013;143(2):364–370. doi:10.1378/chest.12-1274
26. Jalil B, Thompson P, Cavallazzi R, et al. Comparing Changes in Carotid Flow Time and Stroke Volume Induced by Passive Leg Raising. Am J Med Sci. 2018;355(2):168–173. doi:10.1016/j.amjms.2017.09.006
27. Scheeren TWL, Bakker J, De Backer D, et al. Current use of vasopressors in septic shock. Ann Intensive Care. 2019;9(1):20. doi:10.1186/s13613-019-0498-7
28. Bai X, Yu W, Ji W, et al. Early versus delayed administration of norepinephrine in patients with septic shock. Crit Care. 2014;18(5):532. doi:10.1186/s13054-014-0532-y
29. Sennoun N, Montemont C, Gibot S, Lacolley P, Levy B. Comparative effects of early versus delayed use of norepinephrine in resuscitated endotoxic shock. Crit Care Med. 2007;35(7):1736–1740. doi:10.1097/01.CCM.0000269028.28521.08
30. Ban K, Kochi K, Imai K, Okada K, Orihashi K, Sueda T. Novel Doppler technique to assess systemic vascular resistance: the snuffbox technique. Circ J. 2005;69(6):688–694. doi:10.1253/circj.69.688
31. Lee E-P, Hsia S-H, Huang -C-C, et al. Strong correlation between doppler snuffbox resistive index and systemic vascular resistance in septic patients. J Crit Care. 2019;49:45–49. doi:10.1016/j.jcrc.2018.10.010
32. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
33. Liu VX, Fielding-Singh V, Greene JD, et al. The Timing of Early Antibiotics and Hospital Mortality in Sepsis. Am J Respir Crit Care Med. 2017;196(7):856–863. doi:10.1164/rccm.201609-1848OC
34. Yerke J, Strnad K, Bauer SR. Corticosteroids for Septic Shock: another Chapter in the Saga. Hospital Pharm. 2020;55(2):135–142. doi:10.1177/0018578719829416
35. Douglas IS, Alapat PM, Corl KA, et al. Fluid Response Evaluation in Sepsis Hypotension and Shock: a Randomized Clinical Trial. Chest. 2020;158(4):1431–1445. doi:10.1016/j.chest.2020.04.025
36. Das SK, Choupoo NS, Pradhan D, Saikia P, Monnet X. Diagnostic accuracy of inferior vena caval respiratory variation in detecting fluid unresponsiveness: a systematic review and meta-analysis. Eur J Anaesthesiol. 2018;35(11):831–839. doi:10.1097/EJA.0000000000000841
37. Shi R, Monnet X, Teboul J-L. Parameters of fluid responsiveness. Curr Opin Crit Care. 2020;26(3):319–326. doi:10.1097/MCC.0000000000000723
38. Girotto V, Teboul J-L, Beurton A, et al. Carotid and femoral Doppler do not allow the assessment of passive leg raising effects. Ann Intensive Care. 2018;8(1):67. doi:10.1186/s13613-018-0413-7
39. Ospina-Tascon GA, Hernandez G, Alvarez I, et al. Effects of very early start of norepinephrine in patients with septic shock: a propensity score-based analysis. Crit Care. 2020;24(1):52. doi:10.1186/s13054-020-2756-3
40. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi:10.1097/CCM.0b013e31827e83af
41. Devia Jaramillo G, Castro Canoa J, Valverde Galvan E. Approach of minimal invasive monitoring and initial treatment of the septic patient in emergency medicine. Open Access Em Med. 2018;10:183–191. doi:10.2147/OAEM.S177349
42. Varpula M, Tallgren M, Saukkonen K, Voipio-Pulkki L-M, Pettila V. Hemodynamic variables related to outcome in septic shock. Intensive Care Med. 2005;31(8):1066–1071. doi:10.1007/s00134-005-2688-z
43. Maheshwari K, Nathanson BH, Munson SH, et al. The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Intensive Care Med. 2018;44(6):857–867. doi:10.1007/s00134-018-5218-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.