")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Use of traditional medicines and traditional practitioners by children in Indonesia: findings from a national population survey in 2014–2015
Received 29 January 2019
Accepted for publication 11 March 2019
Published 26 April 2019 Volume 2019:12 Pages 291—298
DOI https://doi.org/10.2147/JMDH.S203343
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supa Pengpid,1,2 Karl Peltzer2
1ASEAN Institute for Health Development, Mahidol University, Nakhonpathom, Thailand; 2Research and Innovation Office, North West University, Potchefstroom, South Africa
Background: Little data are available about traditional and complementary medicine use in children in the general population in Southeast Asia, including Indonesia. The aim of this investigation was to assess the prevalence of the use of traditional medicines and traditional practitioners in children in a national population-based survey in Indonesia.
Methods: The cross-sectional sample included 15,739 children (0–14 years) (median age 7.0 years, inter quartile range =7.0) that took part in the Indonesia Family Life Survey in 2014–2015.
Results: The prevalence of use of traditional medicines as a treatment in the past four weeks was 6.2%, vitamins or supplements 19.9%, and over-the-counter modern medicine 61.1%. The prevalence of traditional practitioner use in the past 4 weeks was 3.4%, and the prevalence of the use of traditional medicines and/or traditional practitioner in the past 4 weeks was 8.8%. The purpose of consulting the traditional practitioner was mainly massage (86.8%) and treatment for illness (14.8%). In the adjusted logistic regression analysis, having a birth certificate (as a proxy for better economic status) and poor self-rated health were associated with traditional medicine use. Younger age and poor self-rated health were associated with traditional practitioners use.
Conclusion: A high prevalence of traditional medicine use in children in Indonesia was found, and several social factors and poor health status of its use were identified.
Keywords: traditional medicines, traditional practitioner, utilization, children, Indonesia
Introduction
A significant number of people in “Association of Southeast Asian (ASEAN) member states” utilizes traditional health care.1–4 Among adults in Indonesia, “24.4% had used a traditional practitioner and/or traditional medicine in the past four weeks, and 32.9% had used complementary medicine in the past four weeks”.5 There is lack of information on traditional health care among children in the general population,6 including in Indonesia.
One of the most common types of treatment provided by traditional health practitioners in Indonesia was found to be massage for babies (71.4%).7 In a small study of 91 children (6–18 years old) who were admitted to hospital in Indonesia, 39.6% had used Indonesian herbal medicine prior to admission.8 Several investigations have been carried out on the use of traditional medicine for specific acute and chronic conditions, such as fever, diarrhea, and cancer in Indonesia and Malaysia.9–12 Suparmi et al,13,14 have pointed out some of the risks associated with the use of jamu, Indonesian herbal medicines, for the general public, including children, in Indonesia.
The general population prevalence of the past 7 days use of “herbal medicinal products” among children and adolescents (0–17 years) in Germany was 5.8%.6 In the USA less than 0.5% of the children (0–12 years) had used herbal remedies in the past 7 days,15 in Italy 2.4% in the past 3 years (0–13 years).16 The prevalence of past month use of traditional and complementary medicine among children and adolescents (0–18 years) in Taiwan was 4.7%.17 In a study in Germany, herbal medicines were mainly used for treating coughs and colds of children and adolescents.6
Some studies found associations between specific sociodemographic characteristics and traditional and/or complementary medicine use among children and adolescents. For example, younger age,6 female gender,17 and higher socioeconomic status.8,16,17 While in a study in Ethiopia, lower education of the parents was associated with traditional medicine use for children.18 Having a poor health status was also associated with increased use of herbal medicine in Germany.6 The aim of this investigation was to assess the prevalence of the use of traditional medicines and traditional practitioners in children in a national population-based survey in Indonesia.
Methods
Study design and participants
Cross-sectional data were analyzed from the child module of the “Indonesia Family Life Survey (IFLS-5)”, which was conducted in 2014–2015. The IFLS-5 is a household survey representative of 83% of the population in Indonesia, with a survey response rate above 90%; more details on the complex sampling method.19–21 “Two randomly selected children of the head and spouse age 0–14 years” were included per household.19 Questionnaires were administered to the child’s mother, guardian, or caretaker or older sibling if the child was less than 11 years old. “Children between the ages of 11 and 14 were allowed to respond for themselves if they felt comfortable doing so.”19 The IFLS-5 had been approved by the ethics review boards of RAND (“Research ANd Development”) and the University of Gadjah Mada.19–21 Prior to the interview, informed consent was obtained from all the respondents.19–21
Measures
Traditional medicines use
“Now, we’d like to know whether [CHILD’S NAME] has taken medicine on his/her own during the past 4 weeks, namely since […] date, 4 weeks ago?” Response options were “Consumed over-the-counter modern medicines (like bodrexin, inzana, paramex); Consumed traditional herbs or traditional medicines as treatment; Used topical medicines (like eyedrops, cream, medical plaster, ointment and the like); Vitamins/Supplements; Massage, coining, etc.”19
Traditional practitioner use
“In the last 4 weeks, did [CHILD’S NAME] visit a hospital, health center, clinic, doctor’s practice, or a health worker?” Response options were “Public hospital (General or Specialty); Public Health Centre/Auxiliary Centre; Private Hospital; Polyclinic, Private Clinic, Medical Centre; Private Physician (General Practitioner, Specialist, Dentist); Nurse, Paramedic, Midwife practitioner; Traditional practitioner (shaman, wise man, kyai, Chinese herbalist, masseur, acupuncturist, etc.); Other.”19
Last health care provider visit
“Now, I’d like to ask you some questions about [CHILD’S NAME] LAST VISIT to health care providers. What is the type of medical facility or type of provider?”19 Response options as above.
“What was the purpose of [CHILD’S NAME] visit to that facility?”19 Response options “Immunization; Consultation; Medical check-up; Medications; Injection; Treatment for Injury; Treatment for Illness; Massage; Other.”19 (Multiple responses were possible)
“How much did you pay out of pocket for [CHILD’S NAME]’s outpatient care at […] during the past 4 weeks?”19
“Did you use insurance to pay for all or some of this visit?”(Yes, No)19
“What do you think about the services that were provided by this facility?” Response options were “1= Satisfactory, 2= Somewhat satisfactory, 3= Not satisfactory and 4= Far from satisfactory.”19
Socio-demographic factor questions included age, gender, mother’s and father’s education, and having a birth certificate as an indicator of socioeconomic status.19
Self-reported health status was measured with the question, “In general, how is your health?” Response options ranged from 1= Very healthy to 4= Unhealthy.19–21
Data analysis
Descriptive statistics were used to describe the sample and the prevalence of health care utilization. Logistic regression analysis was conducted to calculate the crude and adjusted odds ratios with 95% confidence intervals to assess the associations between the independent variables and traditional medicines use and traditional health practitioner use, separately. Age and all other variables that were found statistically significant in univariate analyses were included in the multivariable models. Potential multicollinearity was not detected. P<0.05 was considered significant. “Cross-section analysis weights were applied to match the 2014 Indonesian population”.5,19 All statistical analyses were conducted considering the complex design of the study using STATA software version 13.0 (Stata Corporation, College Station, TX, USA).
Results
Sample characteristics
The sample included 15,739 children (0–14 years) (median age 7.0 years, Inter Quartile Range =7.0); 51.5% were male and 48.5% were female, and 17.5% did not have a birth certificate.
Health care utilization
Among seven different health care providers, traditional health practitioners had the fourth highest past 4-weeks prevalence (3.4%), after “nurse, paramedic or midwife practitioners” (6.5%), public health centers (5.7%) and private physician (3.9%). The past 4-weeks prevalence of traditional medicine use as self-treatment was 6.2%, vitamins or supplements 19.9%, and over-the-counter modern medicine 61.1%. The past 4-weeks prevalence of the use of traditional medicines and/or traditional practitioner was 8.8%.
The average expenditure for the past 4-weeks health care provider utilization was lowest for public health centers (10,385 rupiah) and third lowest for traditional practitioners (91,330 rupiah). The average expenditure for the past 4-weeks self-treatment utilization was highest for vitamins or supplements (24,206 rupiah), followed by traditional medicines (10,706 rupiah) and the lowest costs were for massage or coining (6,548 rupiah) (see Table 1).
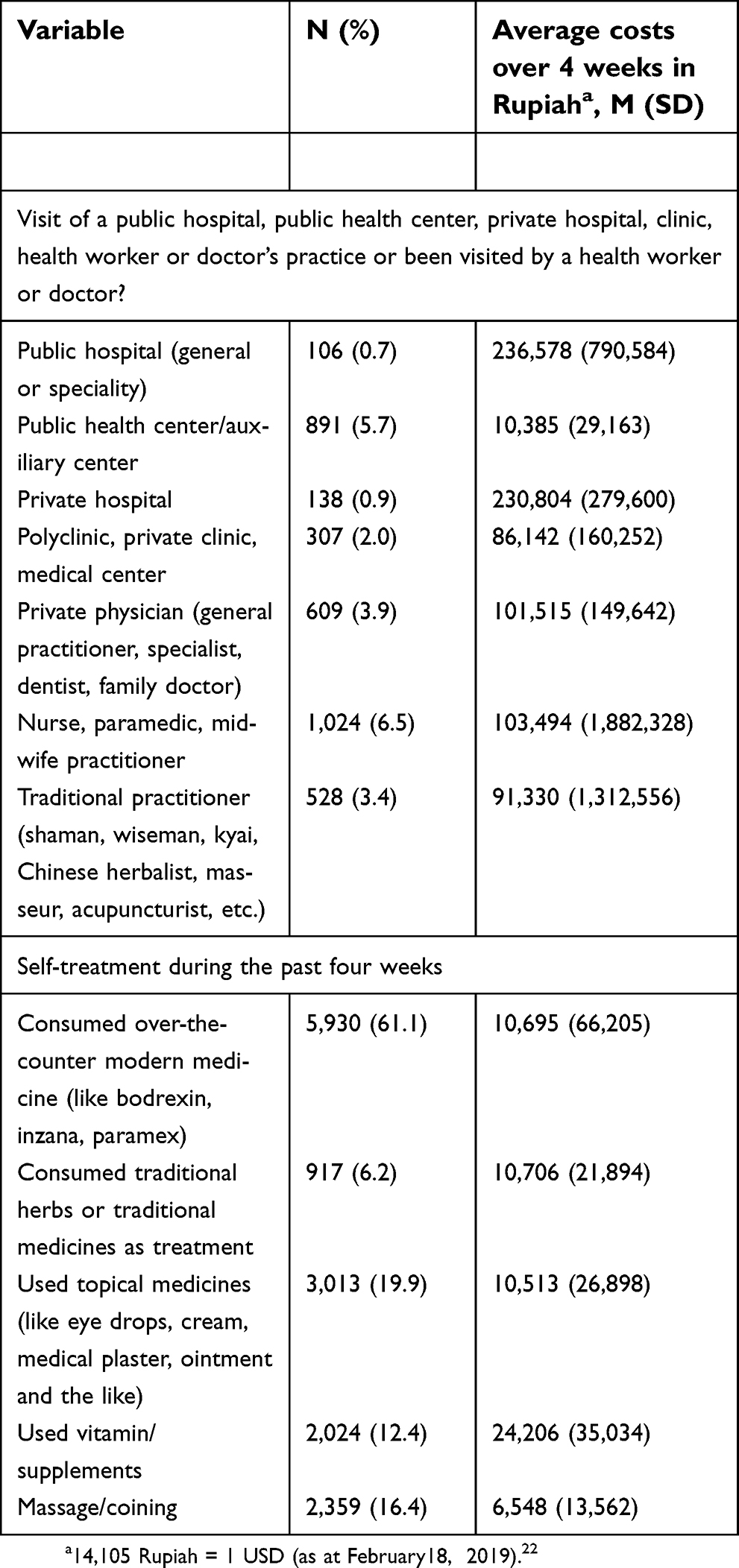 | Table 1 Health care utilization in the past four weeks in 15,739 children (0–14 years) |
The prevalence of the use of the different self-treatment modalities, including traditional medicines, did not differ much across age groups (see Figure 1).
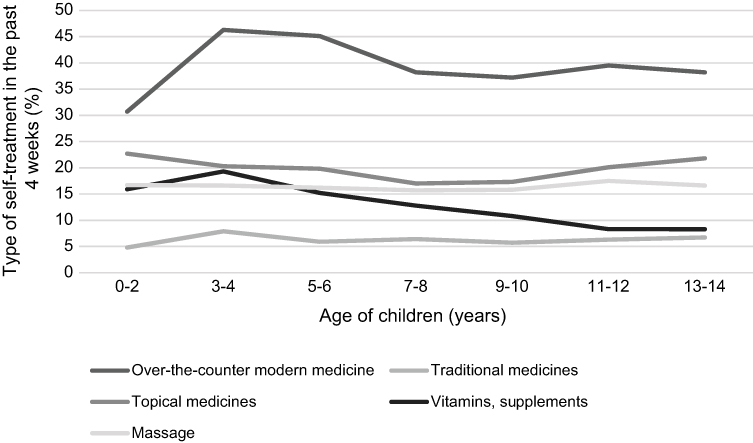 | Figure 1 Prevalence of self-treatment. |
Characteristics of the last health care visit
The purposes of the child’s last health care visit included eight categories, such as immunization and treatment for illness (multiple responses were possible). The purpose of consulting the traditional practitioner was mainly massage (86.8%) and treatment for illness (14.8%). Immunizations were mainly provided by the private hospital (8.2%) and the nurse, paramedic or midwife practitioner (6.3%). Consultations were the highest for the private hospital (16.4%), and medications were the highest for nurse, paramedic or midwife practitioner (64.7%). Medical check-up was the highest in the public hospital (42.0%) ad polyclinic, private clinic or medical center (38.6%). Children were mostly provided an injection by the private physician (18.0%) ad public hospital (12.5%). Treatment for an injury was mainly provided by public and private hospitals (3.4% and 2.5%, respectively). Except for traditional practitioners, all other health care agencies provided above 60% treatment for illness.
Health insurance did not pay for visits to traditional practitioners (0.0%) and only a few for “nurse, paramedic or midwife practitioners” (1.8%) and for almost in half the cases (46.6%) for public hospital visits. Among the last health care service attendees, the highest satisfaction rates were reported for private hospitals (21.3%), followed by traditional health practitioners (19.8%) and private physician (18.3%). Lower health care satisfaction rates were found for public health centers (12.5%) and public hospitals (9.1%) (see Table 2).
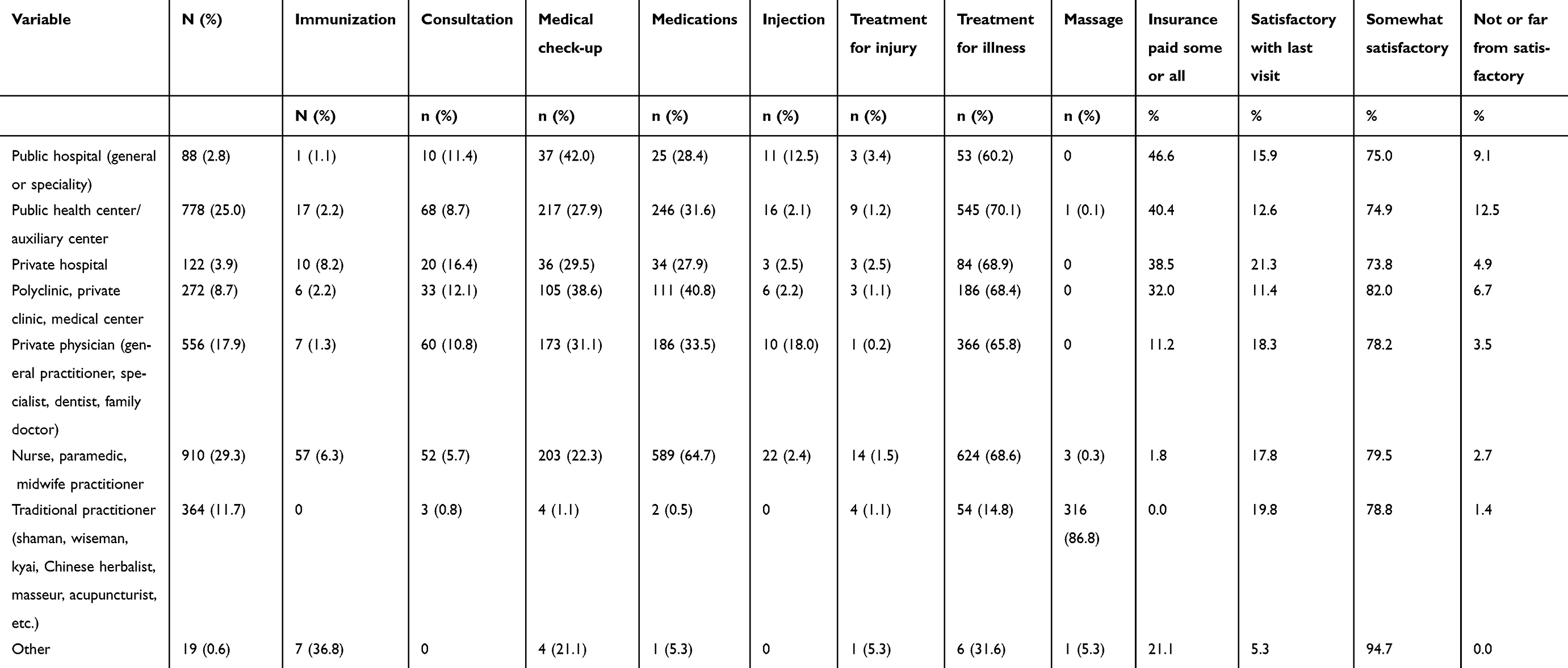 | Table 2 Characteristics of the last health care provider visit (N=3,109) |
Associations with traditional medicine and traditional practitioner use
In the adjusted logistic regression analysis, having a birth certificate (as a proxy for economic status) and poor self-rated health status were associated with traditional medicine use. Younger age and poor self-rated health status were associated with traditional practitioners use (see Table 3).
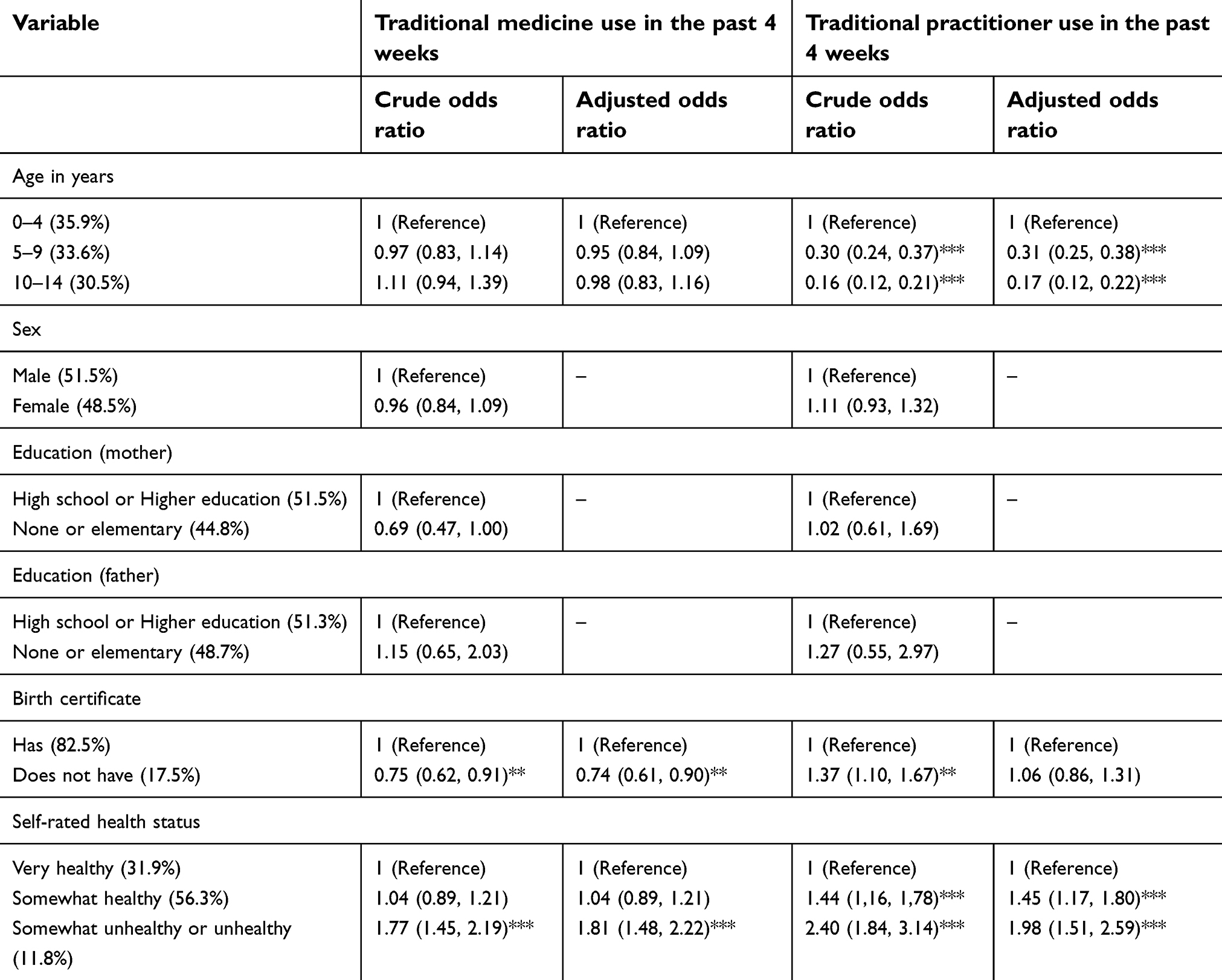 | Table 3 Associations with current traditional and complementary medicine use |
Discussion
The study found that in a nationally representative child sample in Indonesia in 2014–15 that the past month prevalence of traditional or herbal medicines use was 6.2%, the past month use of traditional health practitioners was 3.4%, and the past 4-weeks prevalence of the use of traditional medicines and/or traditional practitioners was 8.8%. These general child population prevalences of traditional or herbal and/or complementary medicine use seem higher than found in Italy (2.4% in the past 3 years)16 and USA (0.5% in the past 7 days),13 but similar to Germany (5.8% in the past 7 days),6 and Taiwan (4.7% in the past month).17 The purpose of consulting the traditional practitioner was mainly massage (86.8%) and treatment for illness (14.8%) in this study. This is in agreement with a previous study among adults in Indonesia that indicated that massage for babies (71.4%) was one of the most common traditional treatment types,9 while in a study in Germany, herbal medicines were mainly used for treating coughs and colds of children and adolescents.6 Herbal medicines are available in drug stores without prescription and professional monitoring in Indonesia.8 Parents or guardians should be given health education about herbal medicines and they should also inform health practitioners about the use of herbal medicines of their children in order to prevent negative drug interactions.8 In addition, the producers of herbal medicinal preparations should follow government regulations in producing safe herbal medicines.13,14
The past 4-weeks prevalence of over-the-counter modern medicine use was in this study 61.1% in the past 4 weeks. This result is much higher than in a national survey in children (0–17 years) in Germany, with 25.2% having used self-medication, including 17.0% over-the-counter drugs, in the previous week.23 The very common use of over-the-counter drugs among the child population can be potentially harmful.23 Further research should be conducted on the type of self-medication and indication to assess possible inappropriate drug use.
Consistent with a previous study in Germany,6 this study found that the use of the traditional practitioner decreased with age. One reason for this could be the large proportion of massages administered to babies and small children by traditional practitioners in Indonesia.7,24 However, the use of traditional medicines did not change with age in this study. A previous study found a preponderance of unconventional medicine use among girls in Germany,25 while this study did not find any gender differences in the use of traditional medicines and traditional practitioners. This finding is in line with adult use of traditional and complementary medicine in Indonesia.5
Several previous studies in high-income countries8,17,25 found an association between higher socioeconomic status and traditional and/or complementary medicine use in children. This study also found that having a birth certificate (as a proxy for better economic status) was associated with increased use of traditional medicines. The educational status of the mother and/or father seem not to influence the use of traditional medicines and traditional practitioners in children in Indonesia. In agreement with a study in Germany,6 this study also found that having a poor health status was associated with increased use of traditional medicines and traditional practitioners in children in Indonesia. One reason for this could be that children with poorer health status, engage in a more frequent and greater variety of health care-seeking behavior, increasing the chances of traditional and/or complementary medicine use.26
In this study, satisfaction (or somewhat satisfied) with the last health care visit with a traditional practitioner was highest (98.6%) compared to other health care provider types. High satisfaction or self-rated improvement of conditions treated with herbal medicinal products was also found in Germany, with 89.2% reporting great or partly improvement of the condition treated.6 In a previous study among adults in Indonesia similar high levels (98.0%) of satisfaction (or somewhat satisfied) with the last health care visit with a traditional practitioner was found.5
In this study, consultation or treatment costs were third lowest for traditional practitioners, after public health centers and polyclinics. Similar results were found among adult health care utilization in Indonesia.6 In this study, the health care costs for the last health care visit were often paid by health insurance for public and private health care (eg, 40.4% for public health centers and 38.5% for private hospitals) but not for treatment by traditional practitioners. This result demonstrates that parents or caretakers are willing to pay a certain amount of money for the treatment by traditional health practitioners in Indonesia.
Study limitations
Although a large population sample was utilized in this survey, data are cross-sectional and therefore no causality can be established. The assessment by self-report may have biased responses. Future studies should assess more details regarding the type of herbal medicines and other treatments in relation to the specific illness or condition of the child.
Conclusions
The study found a high prevalence of traditional medicines and/or traditional practitioner use in Indonesia. Younger age, socioeconomic status, and poor self-rated health status were found to be associated with traditional medicines and/or traditional practitioner use. Health care providers should provide education to patients on traditional medicine use and on ways to combine the use of herbal and biomedical medicine, and producers should provide safe herbal medicines. This study provides a reference on the use of traditional medicines and traditional practitioners for parents, health care providers, and policy-makers. Further research should examine the effectiveness and safety of specific herbal medicinal remedies.
Data availability
Data from the IFLS-5 is available from RAND at
Acknowledgments
RAND is thanked for giving us access to the IFLS-5 data (
Disclosure
The authors report no conflicts of interest in this work.
References
1.
2. Chuthaputti A, Boonterm B. Traditional Medicine in ASEAN. Bangkok: Medical Publisher; 2010.
3. Peltzer K, Pengpid S. Utilization and practice of Traditional/Complementary/Alternative Medicine (T/CAM) in Southeast Asian Nations (ASEAN) member states. Stud Ethno-Med. 2015;9(2):209–218.
4.
5. Pengpid S, Peltzer K. Utilization of traditional and complementary medicine in Indonesia: results of a national survey in 2014–15. Complement Ther Clin Pract. 2018;33:156–163. doi:10.1016/j.ctcp.2018.10.006
6. Du Y, Wolf I-K, Zhuang W, Bodemann S, Knöss W, Knopf H. Use of herbal medicinal products among children and adolescents in Germany. BMC Complement Altern Med. 2014;14:218. doi:10.1186/1472-6882-14-218
7. Peltzer K, Pengpid S. Traditional health practitioners in Indonesia: their profile, practice and treatment characteristics. Complement Med Res. 2018. doi:10.1159/000494457
8. Suryawati, Suard HN. The use of herbal medicine in children. In:
9. Maulida TF, Wanda D. The utilization of traditional medicine to treat fever in children in western Javanese culture. Compr Child Adolesc Nurs. 2017;40(sup1):161–168. doi:10.1080/24694193.2017.1386985
10. Chandra KA, Wanda D. Traditional method of initial diarrhea treatment in children. Compr Child Adolesc Nurs. 2017;40(sup1):128–136. doi:10.1080/24694193.2017.1386980
11. Susilawati D, Sitaresmi M, Handayani K, et al. Healthcare providers’ and parents’ perspectives on complementary alternative medicine in children with cancer in Indonesia. Asian Pac J Cancer Prev. 2016;17(7):3235–3242.
12. Hamidah A, Rustam ZA, Tamil AM, Zarina LA, Zulkifli ZS, Jamal R. Prevalence and parental perceptions of complementary and alternative medicine use by children with cancer in a multi-ethnic Southeast Asian population. Pediatr Blood Cancer. 2009;52(1):70–74. doi:10.1002/pbc.21798
13. Suparmi S, Widiastuti D, Wesseling S, Rietjens IMCM. Natural occurrence of genotoxic and carcinogenicalkenylbenzenes in Indonesian jamu and evaluation of consumerrisks. Food Chem Toxicol. 2018;118:53–67. doi:10.1016/j.fct.2018.04.059
14. Suparmi S, Ginting AJ, Mariyam S, Wesseling S, Rietjens IMCM. Levels of methyleugenol and eugenol in instant herbal beveragesavailable on the Indonesian market and related risk assessment. Food Chem Toxicol. 2019;125:467–478. doi:10.1016/j.fct.2019.02.001
15. Vernacchio L, Kelly JP, Kaufman DW, Mitchell AA. Medication use among children <12 years of age in the United States: results from the Slone Survey. Pediatrics. 2009;124(2):446–454. doi:10.1542/peds.2008-2869
16. Menniti-Ippolito F, Forcella E, Bologna E, Gargiulo L, Traversa G, Raschetti R. Use of unconventional medicine in children in Italy. Eur J Pediatr. 2002;161(12):690. doi:10.1007/s00431-002-1085-7
17. Shih C-C, Liao C-C, Su Y-C, Yeh TF, Lin J-G. The association between socioeconomic status and traditional Chinese medicine use among children in Taiwan. BMC Health Serv Res. 2012;12:27. doi:10.1186/1472-6963-12-27
18. Melesse TG, Ayalew Y, Getie GA, Mitiku HZ, Tsegaye G. Prevalence and factors associated with parental traditional medicine use for children in Motta Town, Amhara Regional State, Ethiopia, 2014. Altern Integr Med. 2015;4:179. doi:10.4172/2327-5162.1000179
19. Strauss J, Witoelar F, Sikoki B The fifth wave of the Indonesia Family Life Survey (IFLS5): overview and field report. March 2016. WR-1143/1-NIA/NICHD, 2016.
20. Peltzer K, Pengpid S. The prevalence of edentulism and their related factors in Indonesia, 2014/15. BMC Oral Health. 2018;118. doi10.1186/s12903-018-0582-7
21. Peltzer K, Pengpid S. High prevalence of depressive symptoms in a national sample of adults in Indonesia: childhood adversity, sociodemographic factors and health risk behaviour. Asian J Psychiatr. 2018;33:52–59. doi:10.1016/j.ajp.2018.03.017
22.
23. Du Y, Knopf H. Self-medication among children and adolescents in Germany: results of the National Health Survey for Children and Adolescents (KiGGS). Br J Clin Pharmacol. 2009;68(4):599–608. doi:10.1111/j.1365-2125.2009.03477.x
24. Handayani L, Suparto H, Suprapto A. Traditional system of medicine in Indonesia. In: Chaudhury RR, Rafei UM, editors. Traditional Medicine in Asia. New Dehli: World Health Organization; 2001:47–68.
25. Italia S, Brand H, Heinrich J, Berdel D, von Berg A, Wolfenstetter SB. Utilization of complementary and alternative medicine (CAM) among children from a German birth cohort (GINIplus): patterns, costs, and trends of use. BMC Complement Altern Med. 2015;15:49. doi:10.1186/s12906-015-0569-8
26. Seo H-J, Baek S-M, Kim SG, Kim T-H, Choi SM. Prevalence of complementary prevalence of complementary and alternative medicine use in a community-based population in South Korea: a systematic review. Complement Ther Med. 2013;21:260–271. doi:10.1016/j.ctim.2013.03.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.