")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Urinary orosomucoid: a new marker of cardiovascular risk in psoriatic patients?
Authors Németh B , Péter I, Boncz I, Jagicza A, Kiss I , Csergő Á, Kőszegi T , Kustán P, Horváth IG , Ajtay Z
Received 10 December 2018
Accepted for publication 25 April 2019
Published 5 July 2019 Volume 2019:15 Pages 831—837
DOI https://doi.org/10.2147/TCRM.S197633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Balázs Németh,1,2 Iván Péter,1 Imre Boncz,1 Anna Jagicza,1 István Kiss,2 Ágnes Csergő,2 Tamás Kőszegi,3,4 Péter Kustán,3,4 Iván G Horváth,5 Zénó Ajtay1,5
1Dermatology Unit, Zsigmondy Vilmos SPA Hospital, Harkány, Hungary; 2Department of Public Health Medicine, Medical School, University of Pécs, Pécs, Hungary; 3Department of Laboratory Medicine, Medical School, University of Pécs, Pécs, Hungary; 4János Szentágothai Research Centre, University of Pécs, Pécs, Hungary; 5Heart Institute, Medical School, University of Pécs, Pécs, Hungary
Purpose: Psoriasis is one of the most common lifelong lasting dermatologic diseases. According to the latest studies, psoriatic patients have a higher risk of developing cardiovascular diseases. Psoriasis is considered as a systemic inflammatory disease. Several oxidative stress markers have been shown to be elevated in psoriasis. However, a panel of biomarkers has not been used yet. This study was aimed at exploring the connection between a panel of biomarkers (C-reactive protein, asymmetric dimethylarginine, uric acid, total antioxidant capacity, malondialdehyde, and orosomucoid [ORM]) and cardiovascular risk in psoriatic patients.
Patients and methods: The inclusion criterion was the onset of psoriasis with skin lesions. Exclusion criteria were impaired renal function (eGFR<60 mL/min/1.73 m2,), acute inflammations (urinary, respiratory, skin inflammation, etc), autoimmune disorders (rheumatoid arthritis, systemic lupus erythematosus, or inflammatory bowel disease), and any kind of biological antipsoriatic treatment. Patients with a medical history of myocardial infarction, coronary heart disease, stroke, transient ischemic attack, and carotid artery stenosis were also excluded. Biomarkers were measured by routine procedures, ELISA and HPLC. QRISK®2-2017 was used to assess 10-year risk of cardiovascular disease development. Psoriasis severity was measured by the Psoriasis Area and Severity Index.
Results: One hundred and fourteen psoriatic patients were enrolled. Only urinary orosomucoid and urinary orosomucoid/urinary creatinine (u-ORM/u-CREAT) ratio showed significant correlation with QRISK score (u-ORM, r=0.245; u-ORM/u-CREAT, r=0.309). When comparing mild psoriatic patients to moderate psoriatic patients, significant differences could only be found in u-ORM and u-ORM/u-CREAT ratio.
Conclusion: There seems to be a connection between urinary ORM and cardiovascular risk. U-ORM and u-ORM/u-CREAT ratio could be used as an indicator of low-grade inflammation in mild and moderate psoriasis. However, it is the 10-year follow-up of cardiovascular events that will determine the usefulness of this biomarker panel.
Keywords: psoriasis, orosomucoid, oxidative stress, C-reactive protein, biomarker, cardiovascular risk
Introduction
Psoriasis is one of the most common lifelong lasting dermatologic diseases.1 Psoriasis has a considerable negative effect on the quality of life, due to physical and psychical symptoms.2 Furthermore, psoriasis is often associated with a higher risk of developing insulin resistance, obesity, diabetes, depression, inflammatory bowel disease, and some malignities.3,4 Moreover, psoriasis is associated with higher cardiovascular risk and adverse outcomes. According to the meta-analysis published by Miller et al, psoriasis was associated with cardiovascular risk factors and ischemic heart disease.5,6 The exact pathomechanism of psoriasis is currently not known; however, several factors have been identified to play a role in the development of psoriasis. Genetical background and the onset of general risk factors (stress, obesity, smoking, and alcohol consumption) can lead to an excessive activation of the immune system, which has been identified as a key factor in the development of psoriasis.7 The diagnosis of psoriasis is made based on its skin symptoms; nevertheless as a result of the latest studies, psoriasis is nowadays considered as a systemic disease. Several studies were performed to investigate the usefulness of biomarkers of oxidative stress in psoriatic patients.8,9
C-reactive protein (CRP) is a widely used marker of inflammation. Previous studies have found increased CRP levels in patients suffering from psoriasis; some of these studies suggested that CRP could be a marker of psoriasis severity.10–13 Increased CRP levels in psoriatic patients were confirmed by a meta-analysis published by Dowlatshahi et al. Nevertheless, the meta-regression did not show significant association between CRP levels and psoriasis severity.14
Asymmetric dimethylarginine (ADMA) is another well-recognized marker of inflammation and oxidative stress.15,16 The major biological function of ADMA is the inhibition of nitric oxide synthase (NOS), which is responsible for generating nitric oxide (NO) from L-Arginine (L-Arg)17. L-Arg/ADMA ratio is an indirect indicator of NO bioavailability. Bilgiç et al showed elevated ADMA concentrations and reduced L-Arg/ADMA ratio in psoriatic patients compared to controls.18
Malondialdehyde (MDA) as a product of lipid peroxidation is another widely used marker of oxidative stress. Relhan et al found elevated MDA levels in psoriatic patients compared to healthy controls.19 This was later confirmed by a larger study published by Kadam et al.20
As a naturally occurring scavenger of free radicals, uric acid seems to play an important role in the antioxidant mechanisms of the body.21,22 However, according to a meta-analysis Western European psoriatic patients have significantly higher uric acid levels compared to controls.23
A non-enzymatic scavenger system is a part of the defense system responsible for attenuating oxidative stress. The “activity” of this system is measured by the total antioxidant capacity (TAC). Several studies described that TAC is reduced in psoriatic patients compared to controls.24–26
Orosomucoid (ORM) or α-1-acid glycoprotein is another major acute phase protein mainly produced by the liver, accounting for approximately 0.5–1.2 g/L of serum proteins.27 Serum ORM (se-ORM) levels may increase in several acute and chronic disorders in response to systemic inflammation. Elevated se-ORM has been found in patients suffering from infections, malignancies, and autoimmune diseases such as rheumatoid arthritis, inflammatory bowel disease, psoriasis, and after cardiac surgery too.28–30 It appears that se-ORM is a non-specific and non-sensitive marker of inflammation. Recent studies have demonstrated that urinary orosomucoid (u-ORM) could be a more sensitive, non-invasive biomarker of inflammatory activation than se-ORM. The clinical utility of u-ORM is yet to be explored.29 In healthy individuals, urinary excretion of ORM is low; u-ORM concentrations are 0.1–3.0 mg/L (0.01–0.3 mg/mmol if referred to urinary creatinine).31 Nevertheless, increased u-ORM levels have been described in certain acute and chronic diseases.29,32 The elevation of u-ORM seems to be associated with systemic inflammation and endothelial dysfunction, which are also considerable factors in the pathomechanism of psoriasis.1–5 The current study was aimed at exploring the connection between the oxidative stress markers mentioned earlierand cardiovascular risk in psoriatic patients. QRISK®2-2017 (University of Nottingham and EMIS) was used to assess 10-year risk of cardiovascular disease development.33
Materials and methods
The present study was performed at our ISO 9001 accredited Dermatology Rehabilitation Unit between November 2016 and August 2017. Inclusion criterion was the onset of psoriasis with skin lesions. Exclusion criteria were impaired renal function (eGFR<60 mL/min/1.73 m2), acute inflammations (urinary, respiratory, skin inflammation, etc.), autoimmune disorders (rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease), and any kind of biological antipsoriatic treatment and withdrawal of consent. Patients with a medical history of myocardial infarction, coronary heart disease, stroke, transient ischemic attack and carotid artery stenosis were also excluded. Venous blood and midstream first morning urine samples were simultaneously obtained from every patient.
The study protocol was approved by the Regional Ethics Committee of The University of Pécs, Pécs, Hungary (Permission No.: 5919/2.), in accordance with the 2008 Helsinki declaration.
Written informed consent was obtained from every patient.
Psoriasis severity was measured by the Psoriasis Area and Severity Index (PASI). Patients were categorized based on PASI as mild (PASI<7) moderate (PASI 7-12) and severe (PASI>12) groups.34 To rule out interobserver errors, PASI was assessed by the same dermatologist in all cases.
Laboratory tests were performed at the university’s clinical laboratory (accreditation no.: NAH-1-1553/2016). Conventional inflammatory parameters (high sensitivity C-reactive protein (hsCRP), white blood cell count (WBC), uric acid), and serum orosomucoid (se-ORM) were measured by routine procedures. MDA levels were measured by using enzyme-linked immunosorbent assay (product no.: MAK085-1KT, Sigma Aldrich, Saint Louis, MO, USA). L-arginine, ADMA and SDMA levels were determined by liquid chromatography-tandem mass spectrometry method described by Martens-Lobenhoffer et al.35 Minor modifications were implemented to transfer the method to our Dionex Ultimate 3000 HPLC/Thermo Q Exactive setup (Thermo Fisher Scientific, Waltham, MA, USA). Target substances were separated using a Kinetex HILIC column (product no.: 00D-4461-AN; Phenomenex, Torrance, CA, USA). Data obtained in MS2 mode were extracted by pseudo-MRM method using the “Xcalibur 2.2 Qual Browser” evaluation software (Thermo Fisher Scientific). L-arginine monohydrochloride (product no.: A5131; Sigma Aldrich, Saint Louis, MO, USA), and NG,NG Dimethylarginine dihydrochloride (product no.: D4268; Sigma Aldrich) standards were used for calibration. The quantitation range was 0.0203–4.94 μM for ADMA and 0.063–250 μM for L-arginine. The regression coefficient was R2>0.995 and the precision was lower than 10% relative standard deviation (RSD) for all compounds in case of the calibrations. The accuracy was ±15% for the quality control (QC) samples (spiked plasma). U-ORM was determined by an automated turbidimetric assay using ORM immunparticles (Dako A/S, Glostrup, Denmark).36 To avoid the influence of the variations of urinary solute concentrations, u-ORM levels were divided by u-creatinine (u-ORM/u-CREAT, mg/mmol). TAC was determined by using a chemiluminescence-based method.37
QRISK®2-2017 was calculated using a commercially available calculator (https://qrisk.org/).33 The score was calculated from the following parameters: age, sex, ethnicity, smoking status, diabetes status, angina, or heart attack in a 1st degree relative under 60, chronic kidney disease, atrial fibrillation, on blood pressure treatment, rheumatoid arthritis, cholesterol/HDL ratio, systolic blood pressure (mmHg), and body mass index.
Statistical analysis was performed with IBM SPSS Statistics for Windows Version 22 (IBM Corp., New York, NY, USA). Values were compared by Mann-Whitney U test. To reveal correlations, the Spearman’s test was used. Data are presented as median and interquartile (IQR). All p-values less than 0.05 were considered statistically significant.
Results
One hundred and fourteen psoriatic patients were enrolled in the present study (age 63±9.98). The clinical characteristics of the involved patients and controls are presented in Table 1. The mean PASI of the patients was 6.52±7.11. Based on PASI, 78 of the patients had mild psoriasis, 20 had moderate, and 16 had severe psoriasis (34). As high as 33% of the patients had positive family history of psoriasis. The mean onset of psoriasis was 25.5±16.7 years. Significantly higher hsCRP and s-ORM levels were found when comparing the hsCRP and the s-ORM levels of the mild psoriatic patients to the hsCRP and s-ORM levels of the severe psoriatic patients (hsCRP, p=0.003; s-ORM, p=0.005). Significantly higher u-ORM levels and u-ORM/u-CREAT ratio were found in patients suffering from moderate psoriasis when comparing the u-ORM levels and u-ORM/u-CREAT ratio of the mild psoriatic patients to the u-ORM levels and u-ORM/u-CREAT ratio of the moderate psoriatic patients (u-ORM, p=0.003; u-ORM/u-CREAT, p=0.005). Furthermore, u-ORM levels and u-ORM/u-CREAT ratio were found to be significantly higher in patients suffering from type I diabetes compared to patients not suffering from type I diabetes (u-ORM (p=0.041); u-ORM/u-CREAT (p=0.036)).
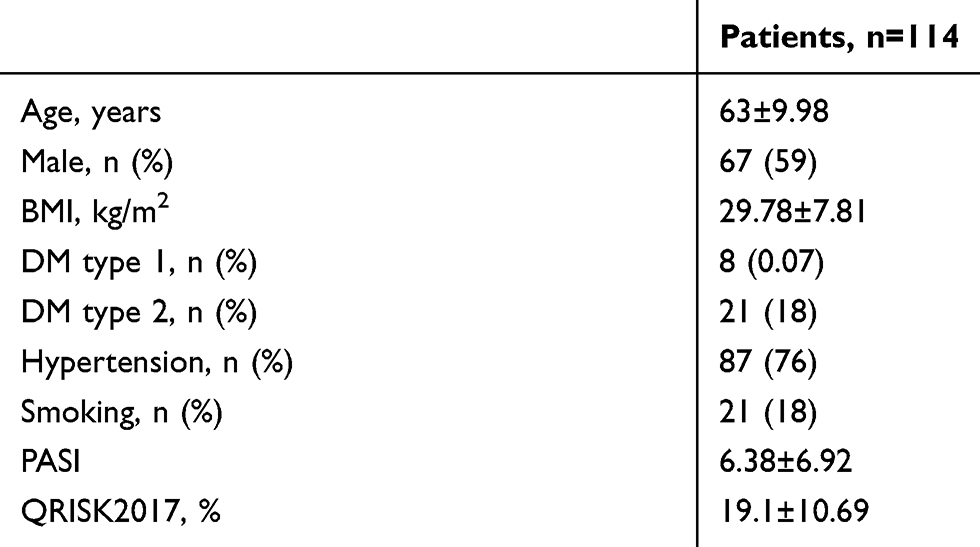 |
Table 1 Clinical characteristics of the involved individuals |
Regarding complications, significantly higher ADMA and MDA levels were found in patients suffering from psoriatic arthritis when comparing the ADMA and the MDA levels of the patients suffering from arthritis to the patients not suffering from arthritis (ADMA (p=0.021); MDA (p=0.021)). Detailed results of the biomarker measurements are shown in Table 2.
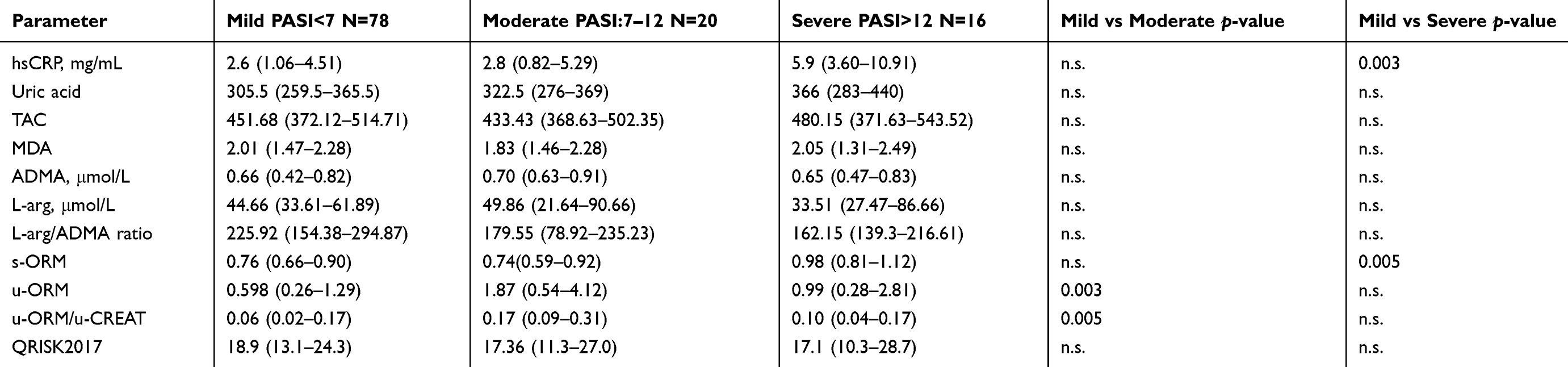 |
Table 2 Parameters of psoriatic patients based on the Psoriasis Area and Severity Index |
U-ORM and u-ORM/u-CREAT showed significant correlation with 10-year risk of cardiovascular disease development (u-ORM, r=0.245; u-ORM/u-CREAT, r=0.309). The detailed list of correlations is shown in Table 3.
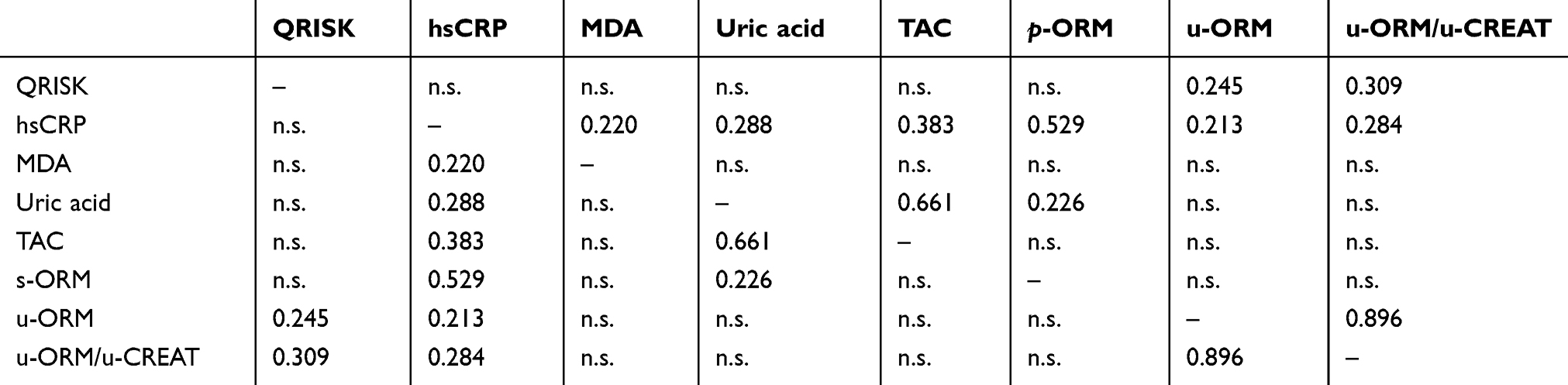 |
Table 3 List of correlations |
Discussion
Psoriasis is a lifelong autoimmune disease affecting about 2–4% of the population. It is responsible for considerable psychosocial disability and negative effects on quality of life.1–5 The increased prevalence of risk factors of cardiovascular diseases, such as metabolic syndrome, diabetes, obesity, hypercholesterolemia, hypertension, and endothelial dysfunction, among psoriatic patients was described in several studies.5,6,9,11,38,39 This was confirmed by a meta-analysis published by Miller et al.6 According to Mehta et al, severe psoriasis is responsible for an additional 6.2% absolute risk of a 10-year rate of major adverse cardiac events.40 In the current study, 43% of the patients had high 10-year cardiovascular risk (QRISK score higher than 20%).41 Psoriasis is considered as a systemic immune-mediated inflammatory disease of the skin. Oxidative stress is a considerable factor in the pathophysiology of psoriasis and cardiovascular diseases.20,42 To the best of our knowledge, this is the first study that compares the information provided by a biomarker panel containing oxidative stress markers and inflammatory markers to a cardiovascular risk score among psoriatic patients. In this paper, we report the baseline values of our biomarker panel. Seemingly, a 10-year follow-up needs to be performed to evaluate its usefulness and feasibility. The biomarker panel was compiled to represent different indicators of oxidative stress and inflammation. In other words, we aimed to view the same picture from different angles. CRP as a marker of general inflammation,14 ADMA16 and MDA9,20 as indirect indicators of oxidative stress, L-Arg/ADMA as an indicator of NO bioavailability,18 and TAC and uric acid levels as indicators of free radical scavenging capability.24–26 Furthermore, we aimed to compare the levels of s-ORM and u-ORM to these recognized markers. In line with previous findings, hsCRP and s-ORM levels were found to be significantly higher in severe psoriatic patients compared to mild psoriatic patients.10–12,43,44
When comparing mild psoriatic patients to moderate psoriatic patients, significant differences could only be found in u-ORM and u-ORM/u-CREAT ratio. On the other hand, the difference of u-ORM and u-ORM/u-CREAT ratio did not reach statistical significance when comparing mild psoriatic patients to severe psoriatic patients. This can be explained with the low number of patients of severe psoriatic patients (n=16). However, the levels of non-specific inflammatory markers (s-ORM and CRP) were significantly higher in patients suffering from severe psoriasis compared to mild psoriatic patients. This indicates that in the case of severe psoriatic patients some grade of systemic inflammation is present.9,45 In our previous study, both u-ORM and u-ORM/u-CREAT ratio were significantly higher in psoriatic patients compared to controls.45 Taking this into account, u-ORM and u-ORM/u-CREAT ratio could be used as an indicator of low-grade inflammation or oxidative stress in mild and moderate psoriasis, as other biomarkers investigated in this study were not able to indicate significant inflammation or excessive oxidative stress in the case of mild and moderate psoriatic patients. However, further research is needed to clarify the clinical usefulness of u-ORM.
Another finding of our study is that there was significant correlation with u-ORM and QRISK score. The evidence on the connection between u-ORM and CV diseases is limited. Hou et al found increased u-ORM levels in patients suffering from heart failure compared to healthy controls.32 Other studies found that u-ORM could be a marker of endothelial dysfunction and atherosclerosis.46,47 Furthermore, the urinary excretion of ORM seems to be strongly associated with diabetes mellitus, which is a known risk factor of CV diseases. This was confirmed by our study; u-ORM levels and u-ORM/u-CREAT ratio were found to be significantly higher in patients suffering from diabetes mellitus46,47 Taking all this together, we suggest that u-ORM can be an indicator of cardiovascular risk among psoriatic patients.
Among the limitations of the study, the low number of severe and moderate psoriatic cases can be mentioned. The lack of a control group can be seen as a limitation as well. Moreover, due to the relatively low number of patients, the existence of a beta-type error cannot be ruled out. However, the main goal of the study will have been fulfilled by the end of the 10-year follow-up period.
Conclusion
U-ORM and u-ORM/u-CREAT ratio could be used as an indicator of low-grade inflammation in mild and moderate psoriasis. U-ORM seems to be in connection with cardiovascular risk in psoriatic patients. However, the 10-year follow-up of cardiovascular events will determine the feasibility of this biomarker panel.
Acknowledgments
The authors would like to thank all the nurses of the Dermatology Ward of Zsigmondy Vilmos SPA Hospital for their invaluable help.
The present scientific contribution is dedicated to the 650th anniversary of the foundation of the University of Pécs, Hungary. Balázs Németh was supported by the ÚNKP-18-3-III New National Excellence Program of the Ministry of Human Capacities, Hungary. The funding sponsors had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parisi R, Symmons DP, Griffiths CE, et al. Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133:377–385. doi:10.1038/jid.2012.339
2. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370:263–271. doi:10.1016/S0140-6736(07)61128-3
3. Rapp SR, Feldman SR, Exum ML, et al. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41:401–407. doi:10.1016/S0190-9622(99)70112-X
4. Smith CH, Barker JN. Psoriasis and its management. Bmj. 2006;333:380–384. doi:10.1136/bmj.333.7564.380
5. Shahwan KT, Kimball AB. Psoriasis and cardiovascular disease. Med Clin North Am. 2015;99:1227–1242. doi:10.1016/j.mcna.2015.08.001
6. Miller IM, Ellervik C, Yazdanyar S, et al. Meta-analysis of psoriasis, cardiovascular disease, and associated risk factors. J Am Acad Dermatol. 2013;69:1014–1024. doi:10.1016/j.jaad.2013.06.053
7. Huerta C, Rivero E, Garcia Rodriguez LA. Incidence and risk factors for psoriasis in the general population. Arch Dermatol. 2007;143:1559–1565. doi:10.1001/archderm.143.12.1559
8. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361:496–509. doi:10.1056/NEJMra0804595
9. Péter I, Jagicza A, Ajtay Z, et al. Psoriasis and oxidative stress. Orv Hetil. 2016;157:1781–1785. doi:10.1556/650.2016.30589
10. Coimbra S, Oliveira H, Reis F, et al. C-reactive protein and leucocyte activation in psoriasis vulgaris according to severity and therapy. J Eur Acad Dermatol Venereol. 2010;24:789–796. doi:10.1111/j.1468-3083.2009.03527.x
11. Vadakayil AR, Dandekeri S, Kambil SM, et al. Role of C-reactive protein as a marker of disease severity and cardiovascular risk in patients with psoriasis. Indian Dermatol Online J. 2015;6:322–325. doi:10.4103/2229-5178.164483
12. Isha Jain VK, Lal H. C-reactive protein and uric acid levels in patients with psoriasis. Indian J Clin Biochem. 2011;26:309–311. doi:10.1007/s12291-011-0132-4
13. Vanizor Kural B, Orem A, Cimşit G, et al. Evaluation of the atherogenic tendency of lipids and lipoprotein content and their relationships with oxidant-antioxidant system in patients with psoriasis. Clin Chim Acta. 2003;328:71–82.
14. Dowlatshahi EA, van der Voort EA, Arends LR, et al. Markers of systemic inflammation in psoriasis: a systematic review and meta-analysis. Br J Dermatol. 2013;169:266–282. doi:10.1111/bjd.12355
15. Németh B, Kustán P, Németh Á, et al. Asymmetric dimethylarginine: predictor of cardiovascular diseases? Orv Hetil. 2016;157:483–487. doi:10.1556/650.2016.30396
16. Cooke JP. Asymmetrical dimethylarginine: the Uber marker? Circulation. 2004;109:1813–1818. doi:10.1161/01.CIR.0000126823.07732.D5
17. Németh B, Ajtay Z, Hejjel L, et al. The issue of plasma asymmetric dimethylarginine reference range - A systematic review and meta-analysis. PLoS One. 2017;12:e0177493. doi:10.1371/journal.pone.0177493
18. Bilgiç Ö, Altınyazar HC, Baran H, et al. Serum homocysteine, asymmetric dimethyl arginine (ADMA) and other arginine– NO pathway metabolite levels in patients with psoriasis. Arch Dermatol Res. 2015;307:439–444. doi:10.1007/s00403-015-1553-3
19. Relhan V, Gupta SK, Dayal S, et al. Blood thiols and malondialdehyde levels in psoriasis. J Dermatol. 2002;29:399–403.
20. Kadam DP, Suryakar AN, Ankush RD, et al. Role of oxidative stress in various stages of psoriasis. Indian J Clin Biochem. 2010;25:388–392. doi:10.1007/s12291-010-0043-9
21. Ames BN, Cathcart R, Schwiers E, et al. Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: a hypothesis. Proc Natl Acad Sci USA. 1981;78:6858–6862. doi:10.1073/pnas.78.11.6858
22. Fabbrini E, Serafini M, Colic Baric I, et al. Effect of plasma uric acid on antioxidant capacity, oxidative stress, and insulin sensitivity in obese subjects. Diabetes. 2014;63:976–981. doi:10.2337/db13-1396
23. Li X, Miao X, Wang H, et al. Association of serum uric acid levels in psoriasis: a systematic review and meta-analysis. Medicine. 2016;95:e3676. doi:10.1097/MD.0000000000004864
24. Gabr SA, Al-Ghadir AH. Role of cellular oxidative stress and cytochrome C in the pathogenesis of psoriasis. Arch Dermatol Res. 2012;304:451–457. doi:10.1007/s00403-011-1171-7
25. Hashemi M, Mehrabifar H, Daliri M, et al. Adenosine deaminase activity, trypsin inhibitory capacity and total antioxidant capacity in psoriasis. J Eur Acad Dermatol Venereol. 2010;24:329–334. doi:10.1111/j.1468-3083.2009.03416.x
26. Lin X, Huang T. Oxidative stress in psoriasis and potential therapeutic use of antioxidants. Free Radic Res. 2016;50:585–595. doi:10.3109/10715762.2016.1162301
27. Fournier T, Medjoubi-N N, Porquet D. Alpha-1-acid glycoprotein. Biochim Biophys Acta. 2000;1482:157–171.
28. Ceciliani F, Pocacqua V. The acute phase protein alpha1-acid glycoprotein: a model for altered glycosylation during diseases. Curr Protein Pept Sci. 2007;8:91–108.
29. Kustán P, Szirmay B, Kőszegi T, et al. Monitoring urinary orosomucoid in patients undergoing cardiac surgery: a promising novel inflammatory marker. Clin Biochem. 2017;17:
30. Biljan D, Situm M, Kostović K, et al. Acute phase proteins in psoriasis. Coll Antropol. 2009;33:83–86.
31. Li F, Yu Z, Chen P, et al. The increased excretion of urinary orosomucoid 1 as a useful biomarker for bladder cancer. Am J Cancer Res. 2016;6:331–340.
32. Hou LN, Li F, Zeng QC, et al. Excretion of urinary orosomucoid 1 protein is elevated in patients with Chronic Heart Failure. PLoS One. 2014;9:e107550. doi:10.1371/journal.pone.0107550
33. Collins GS, Altman DG. An independent and external validation of QRISK2 cardiovascular disease risk score: a prospective open cohort study. Bmj. 2010;340:c2442. doi:10.1136/bmj.c293
34. Schmitt J, Wozel G. The psoriasis area and severity index is the adequate criterion to define severity in chronic plaque-type psoriasis. Dermatology. 2005;210:194–199. doi:10.1159/000083509
35. Martens-Lobenhoffer J, Bode-Böger SM. Quantification of L-arginine, asymmetric dimethylarginine and symmetric dimethylarginine in human plasma: a step improvement in precision by stable isotope dilution mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci. 2012;904:140–143. doi:10.1016/j.jchromb.2012.07.021
36. Kustán P, Szirmay B, Horváth-Szalai Z, et al. Urinary orosomucoid: validation of an automated immune turbidimetric test and its possible clinical use. Biochem Med. 2016;26:421–430. doi:10.11613/BM.2016.044
37. Kőszegi T, Sali N, Raknić M, et al. A novel luminol-based enhanced chemiluminescence antioxidant capacity microplate assay for use in different biological matrices. J Pharmacol Toxicol Methods. 2017;88:153–159. doi:10.1016/j.vascn.2017.09.256
38. González-Gay MA, González-Vela C, González-Juanatey C. Psoriasis: a skin disease associated with increased cardiovascular risk. Actas Dermosifiliogr. 2012;103:595–598. doi:10.1016/j.ad.2012.01.006
39. Shaharyar S, Warraich H, McEvoy JW, et al. Subclinical cardiovascular disease in plaque psoriasis: association or causal link? Atherosclerosis. 2014;232:72–78. doi:10.1016/j.atherosclerosis.2013.10.023
40. Mehta NN, Yu Y, Pinnelas R, et al. Attributable risk estimate of severe psoriasis on major cardiovascular events. Am J Med. 2011;124:
41. Garg N, Muduli SK, Kapoor A, et al. Comparison of different cardiovascular risk score calculators for cardiovascular risk prediction and guideline recommended statin uses. Indian Heart J. 2017;69:458–463. doi:10.1016/j.ihj.2017.01.015
42. Zhou Q, Mrowietz U, Rostami-Yazdi M, et al. Oxidative stress in the pathogenesis of psoriasis. Free Radic Biol Med. 2009;47:891–905. doi:10.1016/j.freeradbiomed.2009.06.033
43. Coimbra S, Oliveira H, Reis F, et al. Circulating levels of adiponectin, oxidized LDL and C-reactive protein in Portuguese patients with psoriasis vulgaris, according to body mass index, severity and duration of the disease. J Dermatol Sci. 2009;55:202–204. doi:10.1016/j.jdermsci.2009.05.008
44. Chodorowska G, Wojnowska D, Juszkiewicz-Borowiec M. C-reactive protein and alpha2-macroglobulin plasma activity in medium-severe and severe psoriasis. J Eur Acad Dermatol Venereol. 2004;18:180.
45. Kustán P, Kőszegi T, Miseta A, et al. Urinary orosomucoid a potential marker of inflammation in psoriasis. Int J Med Sci. 2018;15:1113–1117. doi:10.7150/ijms.25687
46. El-Beblawy NM, Andrawes NG, Ismail EA, et al. Serum and urinary orosomucoid in young patients with type 1 diabetes: a link between inflammation, microvascular complications, and subclinical atherosclerosis. Clin Appl Thromb Hemost. 2016;22:718–726. doi:10.1177/1076029616637185
47. Christiansen MS, Iversen K, Larsen CT, et al. Increased urinary orosomucoid excretion: a proposed marker for inflammation and endothelial dysfunction in patients with type 2 diabetes. Scand J Clin Lab Invest. 2009;69:272–281. doi:10.1080/00365510802531100
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.