")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Urgent Need of Integrated Health and Social Care to Alleviate High Psychological Distress in People with Disabilities: A Cross-Sectional National Representative Survey in Australia
Received 7 November 2020
Accepted for publication 27 January 2021
Published 15 April 2021 Volume 2021:14 Pages 1541—1550
DOI https://doi.org/10.2147/RMHP.S291004
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Wei Du,1,2 Jiali Wang,3,4 Qingsheng Zhou5
1School of Public Health, Southeast University, Nanjing, People’s Republic of China; 2Research School of Population Health, Australian National University, Canberra, Australia; 3Research School of Finance, Actuarial Studies & Statistics, Australian National University, Canberra, Australia; 4Massachusetts Eye and Ear Institute, Harvard University, Cambridge, USA; 5Faculty of Health Science, University of Sydney, Sydney, Australia
Correspondence: Wei Du Tel +86 25 8327 2303
Email [email protected]
Objective: To investigate factors in association with high psychological distress in people with disabilities.
Methods: We used the 2015 national survey on disability in Australia to derive the representative study population of 7936 people with disabilities aged 18+ years. The Kessler Psychological Distress Scale (K10) was used to define high psychological distress (scores ≥ 22). The explanatory variables included socioeconomic status, physical health, social relationships and environment factors. Adjusted Odds Ratios (ORs) and 95% Confidence Intervals (CIs) were evaluated using weighted Logistic regression models with lasso techniques.
Results: Approximately 21 in 100 study participants experienced high psychological distress. The risk of high psychological distress decreased with age and high educational attainment. Having non-English speaking background (2.31; 1.87– 2.85) and need for assistance in cognitive or emotional tasks (3.25; 2.65– 3.98) were independently significantly associated with high psychological distress in people with disabilities. Delay seeing a GP was associated with a 2-fold risk increase.
Conclusion: Integrated healthcare and social support are warranted with appropriate targeting to improve mental health outcomes in people with disabilities.
Keywords: people with disability, high psychological distress, integrated healthcare, social support
Introduction
Disability is a global public health challenge with estimated 650 million people worldwide living with some form of restriction or impairment to their daily activities.1 Unmet needs and adverse outcomes are common in people with disabilities (PWDs),2 calling for global actions to improve services and outcomes in PWDs.3
PWDs experience elevated risks of anxiety and depression,4 and such a high psychological distress (HPD) also demonstrated an impact on health-related lifestyles in PWDs,5 and reduce their quality of life,6 requiring multi-sectoral efforts to enhance their mental health and wellbeing. While clinically significant manifestations of HPD would possibly lead to comorbid psychosocial impairment in PWDs,4 the psychosocial resources of them may vary in relation to different types of impairment. However, the available healthcare services for PWDs are invariably of poor quality,1–3 which further complicates the provision of psychosocial support they need. Identification of factors in relation to distress, encompassing its social elements,7 is crucial to provide PWDs with appropriate psychosocial support.8,9 These factors can have a different impact on health and social needs in PWDs,10 and therefore person-centred strategies may be tailored to fit for purpose, for example, identifying a PWD subgroup with specific psychosocial needs, then providing alternative options to this targeted subgroup. A service utilisation model comprising physical health, as well as social and environment enabling factors, may inform targeted strategies to improve mental health and wellbeing among PWDs.11 Population-level research using this theoretic framework with a comprehensive assessment of a range of health and social need factors in relation to distress in PWDs is much needed.2
Using the most recent nationally representative survey in Australia, we aimed to quantify the prevalence rate of HPD and investigate its factors among adults with disabilities, which is fundamental to develop targeted person-centred strategies in this vulnerable group. Findings may inform an integrated health and social care strategy to address unmet mental health needs in similar settings.
Methods
Data Source
Data were sourced from Australian Bureau of Statistics (ABS) Confidentialised Unit Record Files (CURF) – the 2015 Survey of Disability, Ageing and Carers (SDAC) in Australia. The 2015 SDAC was designed to derive a nationally representative sample selected at random using multistage sampling schemes with strict quality control measures to ensure survey coverage, reliability and confidentially.12 It comprises holistic information to measure the disability prevalence rates in Australia, and rich sociodemographic, healthcare need, and received support information for people with disabilities. The 2015 SDAC population comprised 63,515 household respondents with a response rate of ~80% in private dwellings. Sample weights were calculated allowing for the complex survey design. Ethics approval for the ABS to conduct the household interview was granted under the Census and Statistics Act 1905. Additional approval for the current study was granted by the Australian National University Human Research Ethics Committee (reference: 2017/175).
Study Outcome
In the 2015 SDAC, psychological distress was measured by the Kessler Psychological Distress Scale (K10).13 We categorised high psychological distress with clinical significance (K10 scores ≥22) as binary, ie, yes, or no.
Our study population comprised 7936 PWDs aged 18+ years living in households. Considering most people with psychiatric disabilities would experience comorbid mental disorders and HPD,14,15 psychosocial and medical interventions are deemed necessary strategies. Therefore, we excluded people with psychiatric disabilities to derive the final study population.
For the sensitivity analysis, we estimated the prevalence of HPD including people with psychiatric disabilities. Taking into account that the PWD group is heterogeneous, we also repeated our analysis stratified by different impairment types in PWDs with or without psychiatric disabilities.
Explanatory Variables
We used the Andersen–Newman model to classify self-reported characteristics into 3 broad groups,11 and further used the lasso (least absolute shrinkage and selection operator) method to exploit the redundancy of variable input and select the candidate variables for association analysis.16 The lasso technique is advantageous in efficient variable selection for a parsimonious model, to further narrow down the number of variables with statistically significant association with HPD in the current setting. Those variables not being selected by the lasso model were excluded for further confirmatory regression modelling. Specifically, these modelled factors were listed as follows:
- predisposing factors, including 1.1) age groups categorised as ≤44, 45–64, 65–84, or ≥85 years; 1.2) sex as male or female; 1.3) country of birth as Australia, other English speaking countries, or non-English speaking countries; 1.4) marital status as married, separated, divorced, widowed, or never married; 1.5) highest educational attainment as bachelor’s degree or higher, diploma or certificate, high school, or not finish high school; 1.6) remoteness of residence using ARIA+,17 as major cities, inner regional, or outer regional areas; 1.7) housing tenure as owner without a mortgage, owner with a mortgage, or renter; 1.8) government concession card holders as yes or no;
- enabling factors, set as binary, ie, yes or no, including 2.1) communication limitation because of disability; 2.2) avoiding situations due to disability; 2.3) feeling of safety home alone during the day/after dark; 2.4) leaving home as often as would like; 2.5) having available support in a time of crisis; and 2.6) attending cultural venues and events; and
- health-need factors, including in the last 12 months ever use of 3.1) general practitioner (GP), 3.2) Dentist, or 3.3) inpatient care, categorised as no need, delayed due to cost, delayed due to other reasons, or yes when needed, respectively; 3.4) whether or not seeing 3 or more health professionals for the same condition in the last 12 months; 3.5) whether or not having difficulty with self-care; 3.6) cognitive or emotional tasks; and 3.7) household chores, respectively. We set a number of impairment types (3.8) as a continuous variable. We further considered whether or not having a comorbid condition (3.9–3.17), including nervous or emotional condition, shortness of breath or difficulty breathing, cancer, endocrine, psychology, sight, cardiovascular disease, musculoskeletal disorder, symptoms and signs, respectively, and categorised these comorbid conditions as binary, ie yes or no.
A separate category was created for unclassifiable values.
Statistical Analysis
We carried out all analyses using “glmnet” package to facilitate the lasso technique for best-model selection and “survey” package to facilitate analysis of complex survey data in R software (version 3.3.1).18,19 Considering the complex SDAC sampling design, we incorporated to sample and replicate weights provided by ABS to our analysis. We calculated the descriptive statistics including weighted numbers, proportion, and prevalence rates of high psychological distress in the study population. We initially used the “glmnet” package to fit the logistic lasso regression, and by adjusting for the tunning parameter λ to control the strength of the penalty for the number of parameters in a complex model, we excluded non-significant variables with coefficients shrunk to 0 for model dimensional reduction. The tunning parameter λ was chosen by 10-fold cross-validation. Factors with at least one categorical level of being significant were considered for further modelling. Secondly, we used the “survey” package to fit the logistic regressions among the study population. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated for HPD in relation to each of the explanatory variables described above. We considered p-values less than 0.05 as statistically significant.
Because psychosocial impairments do not necessarily comprise the diagnosis of high psychological distress,20 we conducted additional sensitivity analysis without excluding people having psychosocial impairments. Taking into account the heterogeneity among PWDs, we performed stratified subgroup analysis by major disability types, ie, sensory/speech impairment; intellectual impairment; physical restriction; psychosocial impairment; and traumatic head injuries, stroke or acquired brain injury, where appropriate, and found no material changes in results.
Results
Population Characteristics
The study population comprised 7936 PWDs, equivalent to a weighted total of 2.6 million PWDs aged 18+ years living in households in Australia. In the study population, 49% were seniors aged 65 years or older, 53% were females, 54% were married, and 26% attained a tertiary degree. Approximate half of the study population were house outright owners (50%), and two thirds were concession card holders (64%) (Table 1). Approximate 94% of PWDs reported having support available in a time of crisis from someone not living in the same household and 66% PWDs attended selected cultural venues and events in the last 12 months (Table 2). Although the majority (96%) needed to see a GP in the last 12 months, one thirds (28%) delayed seeing a GP due to financial or other reasons. Similarly, delayed visiting a dental professional was common (23%), but less than 2% delayed their hospital inpatient care. The leading comorbid condition was musculoskeletal problems, accounting for more than half of PWDs (64%), followed by cardiovascular conditions (44%) (Table 3).
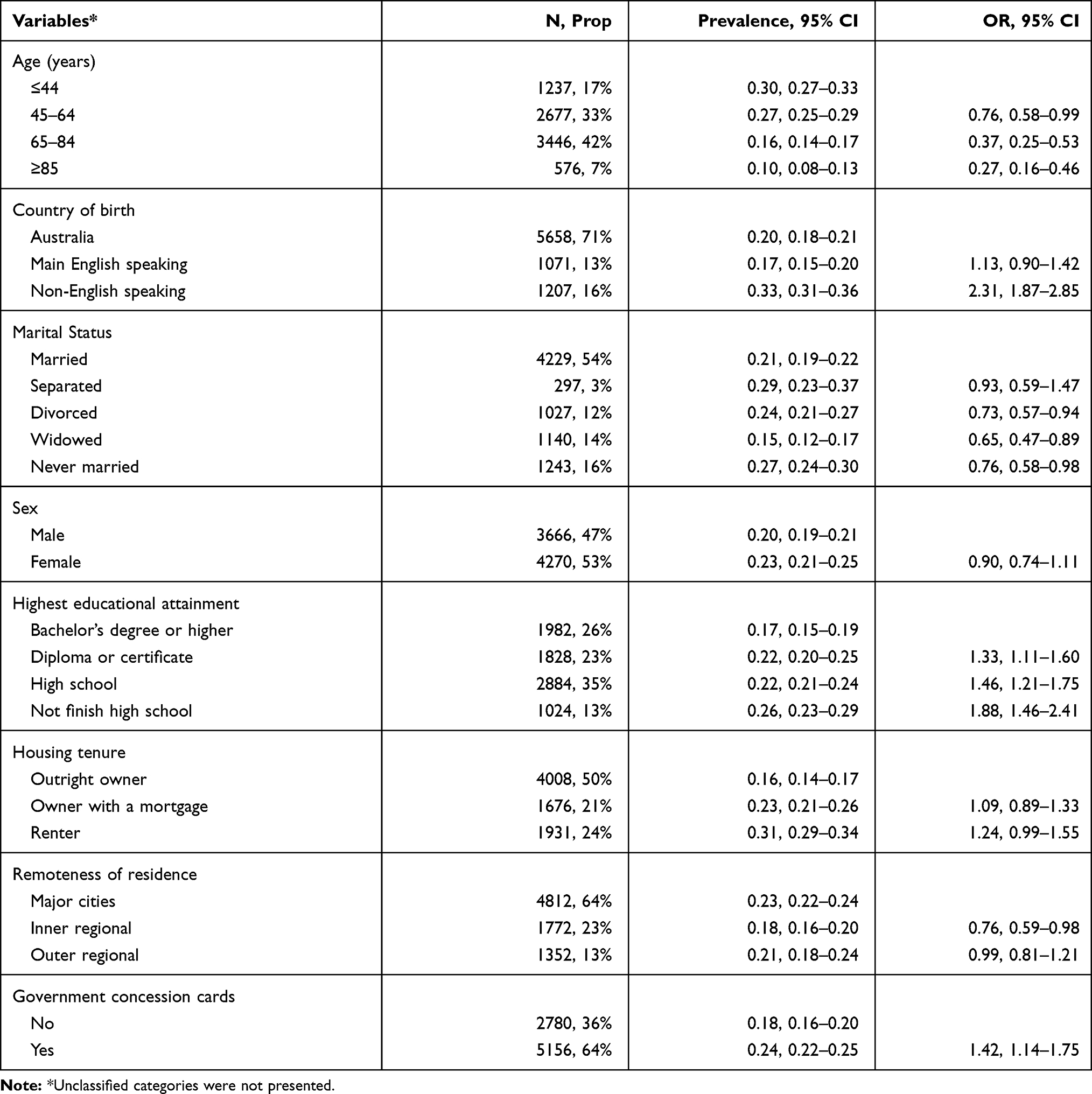 |
Table 1 Predisposing Factors in Relation to High Psychological Distress (Sample Number and Proportion; Weighted Prevalence Rates and 95% Confidence Intervals; and Odds Ratios) |
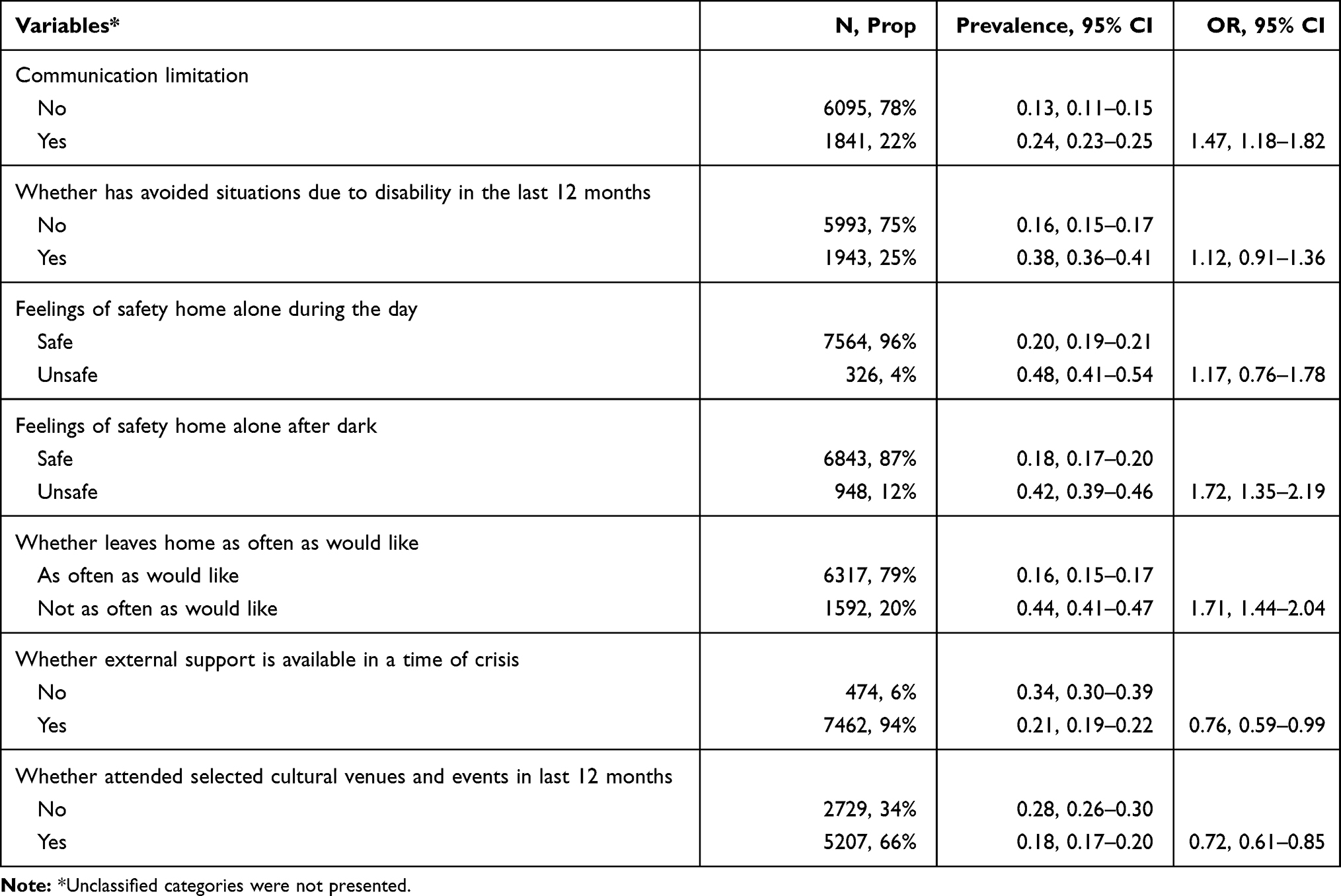 |
Table 2 Enabling Factors in Relation to High Psychological Distress (Sample Number and Proportion; Weighted Prevalence Rates and 95% Confidence Intervals; and Odds Ratios) |
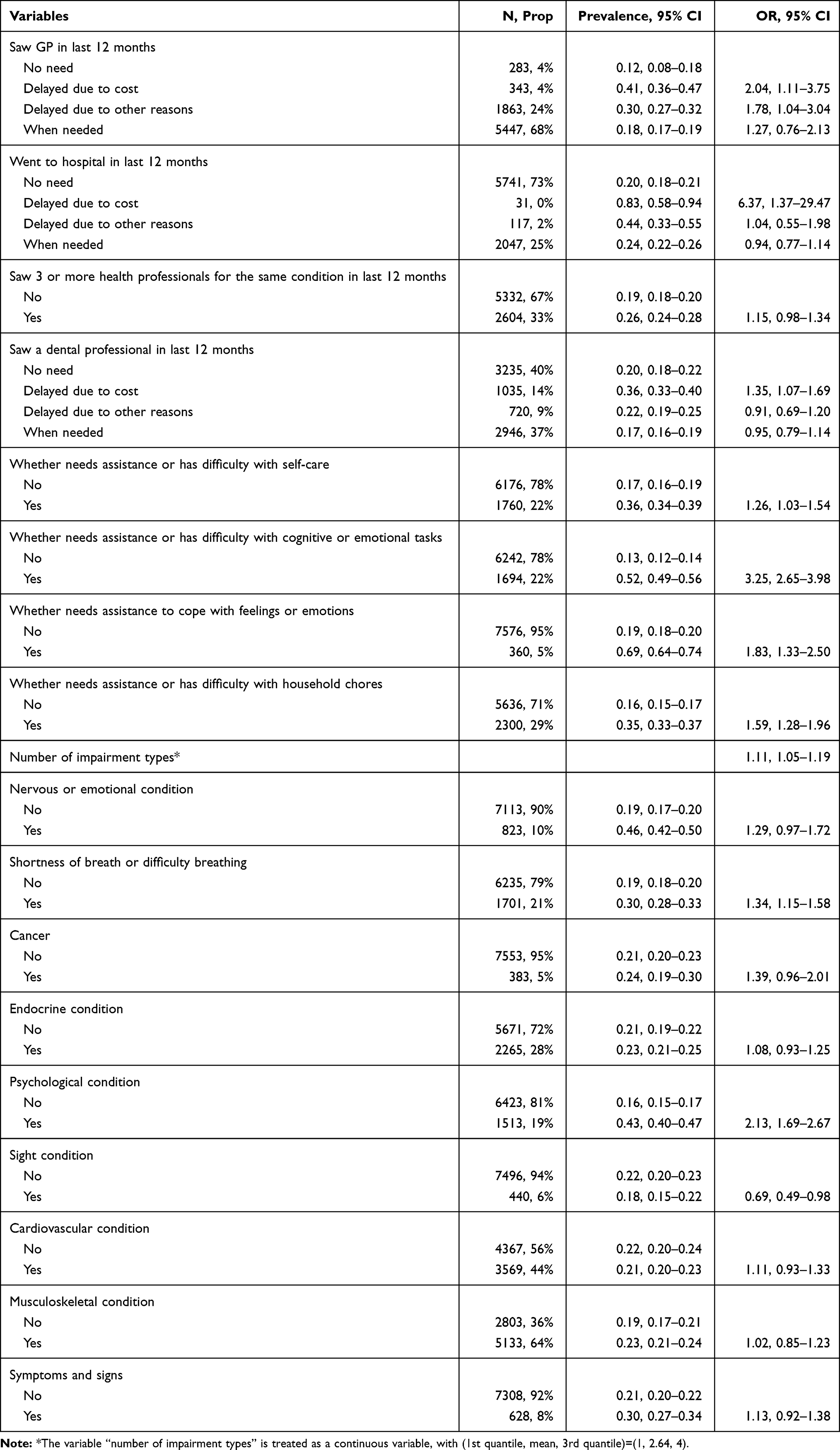 |
Table 3 Health-Need Factors in Relation to High Psychological Distress (Sample Number and Proportion; Weighted Prevalence Rates and 95% Confidence Intervals; and Odds Ratios) |
Prevalence of High Psychological Distress
Approximately 21 in 100 PWDs experienced high psychological distress (weighted prevalence: 21%; 95% CI: 20–23%). The weighted prevalence of HPD decreased with age, and increased with decreasing educational attainment. Renters experienced more HPD than outright owners (31% versus 16%). About a quarter PWDs seeing 3 or more health professionals for the same condition in the last 12 months (26%), having communication limitations (24%), or having musculoskeletal problems experienced high psychological distress (23%) (Tables 1–3).
Contributing Factors
After being adjusted for the other factors, the odds of HPD was greater in PWDs born in non-English speaking countries than their Australian-born counterparts (OR: 2.31; 95% CI: 1.87–2.85) (Table 1). Delay seeing a GP, a dental professional, and admission to hospital due to financial reasons were associated with 2-fold, 1-fold and 6-fold risk increase of HPD, respectively (Table 3). Odds of HPD was elevated among those who needed assistance in common activities of daily living, including self-care (1.26; 1.03–1.54), cognitive or emotional tasks (3.25; 2.65–3.98) and household chores (1.59; 1.28–1.96).
Tables 1–3 described that increased odds of HPD was associated with having communication limitation (1.47; 1.18–1.82), feeling unsafe home alone after dark (1.72; 1.35–2.19), and restriction in everyday activities by shortness of breath (1.34; 1.15–1.58). Conversely, when having support available in a time of crisis or attending selected cultural venues and events in PWDs, the odds of HPD decreased by approximately 24% and 28%, respectively. Having psychological disorders elevated the odds of HPD (2.13; 1.69–2.67), whereas having comorbid sight problems reduced the odds of HPD by 40% (0.69; 0.49–0.98).
Sensitivity Analysis
Without considering psychosocial impairment, the HPD prevalence was 7% in sensory impairment and head injury groups as opposed to 39% in people with intellectual impairment and 24% in people with physical impairment (Supplementary Table 1). Without excluding psychosocial impairment, there was no material change in risk estimates (Supplementary Tables 2.1–2.3). Whilst most of the model results agreed with each other (Tables 1–3 and Supplementary Tables 3.1–3.3), there were some differences between subgroups. The odds of HPD in relation to delays in GP visits were more pronounced (increased by 2-fold) in people with physical impairment compared with the other PWD groups (Supplementary Table 3.3).
Discussion
Using the latest nationally representative survey, our study demonstrated that high psychological distress was common in PWDs (21%), which was two times higher than that in the general population (11%) in Australia.21 Consistent with previous studies reporting the excess burden of HPD in PWDs,4–6,10,22–25 this study adds to the growing body of evidence in regards to the need for appropriate mental health care and rehabilitation in PWDs. This study also revealed that the odds of HPD increased with a number of concurrent impairments, a severity proxy. These findings were consistent with previous studies22–24 and clearly suggested that the alarming burden of HPD warrants clinical recognition and integration of psychosocial support into disability services.
Needing assistance or having difficulty with cognitive and emotional tasks was identified as one of the most important contributors towards the HPD risk. Daily cognitive and emotional tasks may require skills to remember and process information from various situations, then appraise and interpret this information while making social interactions. However, the experience of disabilities can have a detrimental impact on these necessary skills for social participation including daily activities,26 considering PWDs might feel loneliness or social isolation. In response to the change in their lives, PWDs would either adapt or fail to cope. We found the HPD risk was lower in PWDs with sight conditions, which was unexpected but perhaps reflected their adaption with resilience, expectation management, or excellent services and infrastructure in their society. Previous evidence demonstrated that mental health outcomes were improved in relation to socio-environmental interventions, such as social skills training and group-based community activities.27 For example, in comparison with limited impact on psychological symptoms from the low-vision rehabilitation services, improvements in a range of psychological outcomes were found in people with vision impairment undergoing specifically designed cognitive-behavioural therapies.28 Promising evidence was also reported for intervention strategies including telephone support, family psychoeducation therapy, peer support group, social prescribing, and a combination with mixed approaches.29 Considering the important role of these social activities or community recognition as drivers in preventing HPD,30 our findings further demonstrated an urgent need of developing relevant policy strategies addressing social connection for PWDs to alleviate their psychological distress.
In the current study, HPD risks were elevated in PWDs by 2-fold in relation to delays in GP visits and 6-fold to delays in hospitalisation. People with disability were nearly 4 times more likely to have difficulty accessing healthcare than those without disabilities.31 Other than many factors, such as inaccessible medical devices, poor public transportation, and competing priorities in the healthcare systems,32 we noticed that cost would mostly explain the elevated risk of HPD. Because PWDs were more likely to experience comorbid chronic medical conditions than people without disabilities and live in poverty,1–3 PWDs would face a high out-of-pocket spending on healthcare. For those with distress serious enough for urgent medical attention, they would have an increased healthcare service use as well as associated total healthcare costs.33 We found healthcare services were delayed in PWDs for financial reasons, which prompted us to speculate that HPD was perhaps left untreated in the current setting. Therefore, provision with appropriate healthcare in a timely manner should be encouraged. Additional intervention strategies may consider improving the provision of low-cost care and rehabilitation alternatives, such as community-based outreach and home-based program, which may have the potential to reduce psychological distress in this vulnerable population group.
We found the HPD risk decreasing with age, which is consistent with findings in general populations from other Australian settings,34 but contrary to the increasing trend with age based on the US National Health Interview Survey 2009–2013.35 This variation may be attributed to the difference of healthcare systems between these two places, with the Australian system incorporating funding support from both public and private sectors as opposed to the US system pushing towards self-provision for example through employment. However, we did not have information on their exact help-seeking patterns in relation to whether or not having dependents, more active symptoms, or substance issues in the analytic sample so cannot quantify the contribution these factors may have made towards the observed difference. Nevertheless, a recent review of studies using the same measurement across age groups and adjusting for aforementioned risk factors or their proxies reported a more consistent decreasing pattern with age.36 We used a similar risk adjustment approach and revealed that PWDs aged <45 years may need more financial and social support in the current setting. Future research should explore multiple intervention strategies to improve the service utilisation in this population of interest.
Although the current large-scale data provided extensive details of socioeconomic status, eg, marital status, country of birth, concession card status, home ownership, rurality of residence, and highest education attainment, which may play a major role for psychological distress in PWDs and contribute to developing strategies to improve disability services, the lack of potential causal data, such as mental health literacy among PWDs and service infrastructures in their residential communities, limited our ability to identify the pathways through which individuals’ socioeconomic status had an impact on high psychological distress in PWDs. For example, the findings of HPD in those holding concession card, having non-English speaking background, or without tertiary education, indicate a possible connection to mental health literacy based on conventional wisdom, assuming these subgroups might be disadvantaged in comprehending or coping emotional turmoil.
This study presented reliable prevalence estimates of psychological distress using the large-scale nationally representative 2015 SDAC data with standardised quality control measures. Sensitivity analysis of including all people with disabilities showed little material change. Risk factors in relation to HPD were identified with adjustment for a complex framework of social-demographic, community activity, receipt of assistance, healthcare, and health factors. Compared with the conventional step-wise variable selection for modelling that was reported with limitations especially when the number of candidate variables is large, we used a modelling shrinkage method to obtain a parsimonious model with enhanced interpretability without sacrificing prediction accuracy at a later modelling stage.37 However, our study had some limitations. First, the cross-sectional nature of SDAC data limited our ability to establish causal pathways. Second, we restricted our analysis to non-institutionalised population, and therefore results should be interpreted with caution for those who live in cared accommodations. Moreover, high psychological distress indicates typically internalising psychological challenges, whereas externalising problem behaviours were not investigated in the SDAC. Future studies on cognitive shift and problem behaviours could indicate opportunities for improvement in behavioural support services for PWDs. Nevertheless, the contribution of healthcare underuse and deficiency in psychosocial support towards high psychological distress is clear. Intervention strategies focusing on the development of integrated health and social care for people with disabilities may provide insights to improve their mental health outcomes.
Conclusions
The findings highlight the need to provide psychosocial support in people with disabilities. The substantially elevated risk of high psychological distress in relation to deficiency in social participation as well as delayed healthcare in this vulnerable population suggested the targets for developing intervention strategies with the potential to achieve remarkable population health benefits. Collective efforts are expected from healthcare providers and social welfare agencies to reassure people with disabilities.
Data Sharing Statement
Information about data access and governance policies is available at https://www.abs.gov.au.
Ethics Approval and Consent to Participate
Data accessed comply with relevant data protection and privacy regulations. Ethics approval for the ABS to conduct the household interview was granted under the Census and Statistics Act 1905. Additional approval for the current study was granted by the Australian National University Human Research Ethics Committee (reference: 2017/175).
Consent for Publication
All authors read and approved the final manuscript.
Acknowledgments
We would like to thank the Australian Bureau of Statistics (ABS) for providing the Confidentialised Unit Record Files (CURF) product – the 2015 Survey of Disability, Ageing and Carers. WD is supported by the Department of Education (No. 1125000172) and Fundamental Research Funds for the Central Universities (No. 3225002002A1).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization, World Bank. World report on disability. Geneva: World Health Organization; 2011.
2. Krahn G, Walker D, Correa-De-Araujo R. Persons with disabilities as an unrecognized health disparity population. Am J Public Health. 2015;105(S2):S198–S206. doi:10.2105/AJPH.2014.302182
3. World Health Organization. WHO global disability action plan 2014–2021. Better health for all people with disability. Geneva: World Health Organization; 2011.
4. Turner R, Noh S. Physical disability and depression: a longitudinal analysis. J Health Soc Behav. 1988;29(1):23–37. doi:10.2307/2137178
5. Zhou Q, Glasgow N, Du W. Health-related lifestyles and obesity among adults with and without disability in Australia: implication for mental health care. Disabil Health J. 2019;12(1):106–113. doi:10.1016/j.dhjo.2018.08.007
6. Kagan M, Itzick M, Tal-Katz P. Demographic, psychosocial, and health- and disability-related factors associated with psychological distress among people with physical disabilities. Rehabil Psychol. 2018;63(3):392–399. doi:10.1037/rep0000206
7. Mirowsky J, Ross C. Measurement for a human science. J Health Soc Behav. 2002;43(2):152–170. doi:10.2307/3090194
8. World Health Organization. Media centre: disability and health. Available from: http://www.who.int/mediacentre/factsheets/fs352/en/.
9. Andrews G, Henderson S, Hall W. Prevalence, comorbidity, disability and service utilization: overview of the Australian National Mental Health Survey. Br J Psychiatry. 2001;178(2):145–153. doi:10.1192/bjp.178.2.145
10. Okoro CA, Strine TW, Balluz LS, et al. Serious psychological distress among adults with and without disabilities. Int J Public Health. 2009;54(1):52–60. doi:10.1007/s00038-009-0077-z
11. Andersen R, Newman J. Societal and individual determinants of medical care utilization in the United States. Milbank Q. 2005;83(4). doi:10.1111/j.1468-0009.2005.00428.x
12. Australian Bureau of Statistics. Quality declaration: summary. Available from: http://www.abs.gov.au/Ausstats/[email protected]/0/0CD3AF801A5AF108CA25804F000F61FB?OpenDocument.
13. Andrews G, Slade T. Interpreting scores on the Kessler psychological distress scale (K10). Aust N Z J Public Health. 2001;25(6):494–497. doi:10.1111/j.1467-842X.2001.tb00310.x
14. Li N, Chen G, Du W, et al. Population-level prevalence estimate and characteristics of psychiatric disability among Chinese adults. J Psychiatr Res. 2011;45(11):1530–1534. doi:10.1016/j.jpsychires.2011.07.001
15. Rai D, Kosidou K, Lundberg M, et al. Psychological distress and risk of long-term disability: population-based longitudinal study. J Epidemiol Community Health. 2012;66:586–592. doi:10.1136/jech.2010.119644
16. Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc Series B Methodol. 1996;58(1):267–288. doi:10.1111/j.2517-6161.1996.tb02080.x
17. Australian Institute of Health and Welfare. Rural, regional and remote health: a guide to remoteness classifications. Canberra: AIHW; 2004.
18. Friedman J, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Stat Softw. 2010;33(1):1–22. doi:10.18637/jss.v033.i01
19. Lumley T. Analysis of complex survey samples: package ‘Survey’. Available from: http://cran.r-project.org/web/packages/survey/survey.pdf.
20. World Health Organization (WHO). The ICD-10 classification of mental and behavioural - disorders diagnostic criteria for research. Geneva: World Health Organization; 1993.
21. Australian Bureau of Statistics. Profiles of Health, Australia, 2011–13. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/4338.0main+features42011-13.
22. Shen S, Huang K, Kung P, Chiu L, Tsai W. Incidence, risk, and associated factors of depression in adults with physical and sensory disabilities: a nationwide population-based study. PLoS One. 2017;12(3):e0175141. doi:10.1371/journal.pone.0175141
23. Temple JB, Kelaher M. Is disability exclusion associated with psychological distress? Australian evidence from a national cross-sectional survey. BMJ Open. 2018;8(5):e020829. doi:10.1136/bmjopen-2017-020829
24. Houston A, Gomes AM, Naccarato T. Moderate to severe psychological distress, disability, and non-receipt of past year visits to a mental health professional. Disabil Health J. 2016;9(4):735–740. doi:10.1016/j.dhjo.2016.06.002
25. Joshy G, Thandrayen J, Koczwara B, et al. Disability, psychological distress and quality of life in relation to cancer diagnosis and cancer type: population-based Australian study of 22,505 cancer survivors and 244,000 people without cancer. BMC Med. 2020;18(1):372. doi:10.1186/s12916-020-01830-4
26. World Health Organization. World report on disability. Geneva: World Health Organization; 2011.
27. Webber M, Fendt-Newlin M. A review of social participation interventions for people with mental health problems. Soc Psychiatry Psychiatr Epidemiol. 2017;52(4):369–380. doi:10.1007/s00127-017-1372-2
28. Rees G, Ponczek E, Hassell J, Keeffe JE, Lamoureux EL. Psychological outcomes following interventions for people with low vision: a systematic review. Expert Rev Ophthalmol. 2010;5(3):385–403. doi:10.1586/eop.10.32
29. Ma R, Mann F, Wang J, et al. The effectiveness of interventions for reducing subjective and objective social isolation among people with mental health problems: a systematic review. Soc Psychiatry Psychiatr Epidemiol. 2020;55(7):839–876. doi:10.1007/s00127-019-01800-z
30. Benka J, Nagyova I, Rosenberger J, et al. Social support and psychological distress in rheumatoid arthritis: a 4-year prospective study. Disabil Rehabil. 2012;34(9):754–761. doi:10.3109/09638288.2011.619618
31. Australian Bureau of Statistics. General social survey: summary results, Australia; 2014. Available from: http://www.abs.gov.au/ausstats/[email protected]/mf/4159.0.
32. Peacock G, Iezzoni L, Harkin T. Health care for Americans with disabilities: 25 years after the ADA. NEJM. 2015;373(10):892–893. doi:10.1056/NEJMp1508854
33. Luppa M, Sikorski C, Motzek T, Konnopka A, König H, Riedel-Heller S. Health service utilization and costs of depressive symptoms in late life—a systematic review. Curr Pharm Des. 2012;18(36):5936–5957. doi:10.2174/138161212803523572
34. Jorm A, Windsor T, Dear K, Christensen H, Rodgers B. Age group differences in psychological distress: the role of psychosocial risk factors that vary with age. Psychol Med. 2005;35(9):1253–1263. doi:10.1017/S0033291705004976
35. Weissman J, Pratt L, Miller E, Parker J. Serious Psychological Distress Among Adults, United States, 2009–2013. National Center for Health Statistics: Washington; 2015.
36. Price K, Gill T, Winefield H, Koster C, Chittleborough C, Taylor A. Determinants of psychological distress-A literature review: the assessment of the determinants and epidemiology of psychological distress (ADEPD) study. Adelaide: Dept of Health, Population Research and Outcome Studies Unit; 2009.
37. Wang J, Du W. Factors associated with high psychological distress in primary carers of persons with disabilities. Aust J Gen Pract. 2019;48(4):234–239. doi:10.31128/AJGP-04-18-4559
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.