")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Updated Review on the Diagnosis and Primary Management of Psychogenic Nonepileptic Seizure Disorders
Authors Lanzillotti AI, Sarudiansky M, Lombardi NR, Korman GP , D´Alessio L
Received 27 February 2021
Accepted for publication 1 May 2021
Published 4 June 2021 Volume 2021:17 Pages 1825—1838
DOI https://doi.org/10.2147/NDT.S286710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Alejandra Inés Lanzillotti,1 Mercedes Sarudiansky,1 Nicolás Robertino Lombardi,2 Guido Pablo Korman,1 Luciana D´Alessio2,3
1Buenos Aires University, Psychology School, Psychology School Research Institute National Council for Scientific and Technical Research (CONICET), Buenos Aires, Argentina; 2Buenos Aires University, Ramos Mejía Hospital, Epilepsy Center, Buenos Aires, Argentina; 3Buenos Aires University, Medicine School, Cell Biology and Neuroscience Institute (IBCN)- National Council for Scientific and Technical Research (CONICET), Buenos Aires, Argentina
Correspondence: Luciana D´Alessio
Buenos Aires University, Ramos Mejía Hospital, Epilepsy Center, Buenos Aires, Argentina
Tel + 54-11-59509500
Email [email protected]
Abstract: Psychogenic nonepileptic seizures (PNES) are paroxystic and episodic events associated with motor, sensory, mental or autonomic manifestations, which resemble epileptic seizures (ES), but are not caused by epileptogenic activity. PNES affect between 20% and 30% of patients attending at epilepsy centers and constitute a serious mental health problem. PNES are often underdiagnosed, undertreated and mistaken with epilepsy. PNES are diagnosed after medical causes (epilepsy, syncope, stroke, etc.) have been ruled out, and psychological mechanisms are involved in their genesis and perpetuation. For psychiatry, there is not a single definition for PNES; the DSM-IV and ICD-10/11 describe the conversion and dissociative disorders, and the DSM-5 describes the functional neurological disorders. However, patients with PNES also have a high frequency of other comorbidities like depression, particularly trauma and post-traumatic stress disorder. It has been postulated that PNES are essentially dissociations that operate as a defensive psychological mechanism that use the mind as a defense to deal with traumas. With the advent of VEEG in the 90s, the recognition of PNES has significantly increased, and several psychological treatments have been developed. In this manuscript, we carried out a state-of-the-art review, with the aim to provide a critical approach to the extensive literature about PNES, focusing on diagnostic aspects, the primary management, and the available treatments that have been shown to be effective for the improvement of PNES.
Keywords: psychogenic nonepileptic seizures, conversion disorder, dissociative disorder, diagnosis, treatment
Introduction
Psychogenic nonepileptic seizures (PNES) are sudden and involuntary episodic events (paroxystic), associated with motor, sensory, mental or autonomic manifestations. During PNES, normal functioning of central nervous system is altered, and self-control is reduced.1,2 PNES frequently resemble epileptic seizures (ES) but the symptoms are not caused by epileptogenic activity. PNES are diagnosed when medical causes (ie, epilepsy, syncope, stroke), have been ruled out and psychological mechanisms are involved in their genesis and perpetuation. PNES are often underdiagnosed, undertreated and mistaken with epilepsy.2–4
The term PNES was coined by contemporary neurologists after the implementation of the video-electroencephalogram (VEEG) in epilepsy centers. In 1964, Liske and Forster created the term pseudo-seizures to refer to the paroxysmal events similar to epileptic seizures but without the electroencephalographic changes of epilepsy.5,6 Several other names have received the PNES over time: “psychogenic seizures,” “nonepileptic seizures,” “pseudo-seizures,” “psychogenic pseudo-seizures”, “psychogenic nonepileptic attacks”, however currently, the most widespread term in the scientific literature is “psychogenic nonepileptic seizures”.7–9 Recently, some researchers have proposed to mention this condition as “dissociative seizures” or “functional seizures”.10–12 In this regard, is important to achieve to an international consensus on the terminology used. It has been found that the methods of communicating the PNES diagnosis to patients, produce different effects on their understanding, acceptance and/or rejection.13–15 Therefore, a consensus on the terminology could favor the improvement of the relationships between the health professional and the patients, the inter-professional communications, and enhance the therapeutic relationship in the execution of treatments.14–16
Different theories according to psychopathological models have been developed to explain the etiology and phenomenology of PNES.1–3,17 In addition, with the advent of VEEG in the 90s, the recognition of these entities has significantly increased and several mental health interventions and psychological treatments have been developed in the last years.18–25 In this article, we present an updated review of the main diagnostic aspects, primary management and available treatments of patients with PNES. We have made special emphasis on mental health approaches and psychological treatments, which have been shown to be effective for the improvement of PNES. The aim of this manuscript is to review the main data of PNES in order to recognize PNES and to implement the correct psychotherapeutic treatment early.
Methods
We carried out a state-of-the-art review, narrative type. This type of review aims to provide a critical approach to the extensive literature about PNES, emphasizing on those articles produced in the last decades. The search strategy was made through different scientific databases (PubMed, Medline, PsycInfo), using the following descriptors: “PNES”, “psychogenic nonepileptic seizures”, OR “pseudoseizures”, and “prevalence”, “semiology”, “differential diagnosis”, “diagnosis”, “psychiatric comorbidities”, “psychotherapy”, “treatment”, and “psychological treatment”. The most recent and important articles were selected, through pair debriefing, in order to include the most updated information about each topic. This work will provide useful information to contribute to an adequate approach to the diagnosis and treatment of patients with PNES.
Prevalence of PNES
The prevalence of PNES is approximately 1.5% per 100,000 inhabitants per year.26,27 However, the frequency tends to rise, and it is present among 20–30% of the patients admitted at specialized epilepsy centers. Patients with PNES are referred to epilepsy centers with suspected epilepsy with poor response to treatment and are frequently misdiagnosed as having drug resistant epilepsy (DRE).26,27 In addition, between 5% and 40% of patients with PNES have comorbid epilepsy, generating a complex situation during therapeutic management.27–29 In turn, a delay to reach PNES diagnosis is about seven to nine years on average, according different studies.29,30 In our experience, a delay of seven to eleven years has been found among patients with PNES, and most of the patients were previously suspected to have drug resistant epilepsy.22 The trouble to identify subpopulation of patients with PNES may be due to various factors: The difficulty in accessing to VEEG due to the high costs and low availability in primary health centers; the difficult of patients with PNES to connect with mental health services after having received the diagnosis; and the difficult in recognizing epileptic seizures versus PNES.24,26,27
Regarding sex, women presented PNES with a higher prevalence compared to men in all studies.21,22,24,31–33 In addition, multicenter studies showed approximately a 70% of women among patients with PNES.34–36 Several authors linked the gender differences with a history of physical and sexual trauma, suffered more frequently by women in different cultures.32,37,38,39 In this regard, it has been postulated that PNES are essentially dissociations, that operate as a defensive psychological mechanism that use the mind as a defense to deal with traumas. In our casuistic, the trauma history was present among 48% of patients with PNES, and 22% of the patients met full-criteria for post-traumatic stress disorder.22 In this regard, a higher prevalence of trauma and sexual trauma was found among adults comparing to pediatric populations of PNES, suggesting more severe presentations associated with trauma in adult-onset PNES compared with younger ages.41
Clinical Semiology of the PNES; Differential Diagnosis with Epileptic Seizures and the Role of VEEG
The clinical confirmation of PNES is through the complementary method of VEEG, based on the exclusion of epilepsy and other medical diseases. VEEG consists of the continuous monitoring of the patient’s behavior during the paroxysmal episodes, while the electrical activity of the brain is simultaneously recorded through the surface electrodes of the electroencephalogram (EEG).19,42 In medical practice, VEEG is indicated to study the clinical and topographic aspects of the epileptic discharges in patients with epilepsy, and also to study the possibility of epilepsy surgery. However, VEEG is also indicated to carry out the differential diagnosis between ES (epileptic seizures) and PNES when there are diagnostic doubts.19,29,42–44 The aim of VEEG is to corroborate the existence of an electro-clinical correlation during the paroxystic events. PNES is confirmed when the typical episodes described by the patients or relatives, are present during VEEG, without associating any ictal epileptiform activity, and psychological aspects are involved.19,43,44
As well VEEG is the gold standard to define the differential diagnosis, some semiological differences are described between PNES and epileptic seizures. The longer time duration of episodes is a common finding among patients with PNES. However, there are no pathognomonic signs that allow us to totally rule out epileptic seizures.21,44–46 Furthermore, studies have shown that certain signs that were considered typical of PNES (ie, non-synchronic hypermotor symptoms), were not actually specific since they could also be seen in epileptic seizures originated in the frontal lobe.47,48 On the other hand, between 8% and 31% of patients with PNES have suffered injuries during seizures such as tongue biting, bumps and falls. This situation had traditionally been linked to epilepsy.34,35,46 Loss of sphincter control and the appearance of seizures during sleep, have been also described in some patients with PNES, although they are more frequent in epilepsy.46–48 Thus, many times in clinical practice, the diagnosis of PNES cannot be reached only by the clinical manifestations, being the VEEG the method of choice to confirm the differential diagnosis.44,45
Table 1 resumes the main semiological characteristics observed among patients with PNES, according to the studies based on VEEG analysis.34,35,44,49–56 If PNES compromise motor functions (ie, hypermotor), they may resemble epileptic generalized tonic-clonic seizures or frontal lobe epilepsy. Those PNES that compromise the state of consciousness (lack of responsiveness, psychic symptoms, aura), or some localized sensory-motor function (focal motor, akinetic), may resemble partial epileptic seizures with automatisms and/or generalized absence seizures.21,44 Some types of PNES (ie, psychogenic atonic seizures, dialeptic or pseudosyncope), may present behavioral arrest, immobility, psychic auras, depersonalization, derealization, unusual somatic sensations and auditory, visual and olfactory hallucinations resembling complex partial epileptic seizures of temporal lobe origin.21,44,49–56
 |
Table 1 Clinical Manifestations of PNES Based on VEEG Analysis |
Psychiatric Diagnosis of Patients with PNES
There is not a single definition of what neurologists called PNES. Different diagnostic categories defined by the contemporary psychiatric nosographies represent the so-called PNES. For the fourth revised version of the Diagnostic and Statistical Manual of Mental Disorders (DSM IV-TR), PNES with motor symptoms are mainly represented in the category of conversion disorders (somatoform disorders).57 The DSM-IV subdivides conversion disorders into four categories: conversion with sensory symptoms or deficit, with motor symptoms, with seizures, and mixed presentation with more than one type of conversion symptom.57 However, when symptoms affect consciousness, PNES would be better represented within dissociative disorders. In relation to these differences between conversion and dissociation, some controversies have arisen. While conversion is regarding at a purely descriptive level, the role of dissociation implies a psychological mechanism that affects the processing and integration of objective and subjective data of the experience. In this sense, all conversion disorders also imply dissociation of motor experiences.58,23 In addition, it has been postulated that dissociation is the central mechanism that explains the disturbances of consciousness and cognitive control.60 Therefore, contemporary authors have been proposed the dissociation term to unify and refer to the PNES.10,11,59 Recently, the diagnostic category of functional neurological disorders (FND) have been replaced the conversion and dissociative categories in the Diagnostic and Statistical Manual of Mental Disorders 5 version, DSM-5 and encompassed all PNES types.60 In this definition, the term “functional”, describes a group of disorders in which there is a functional rather than a structural disturbance of the nervous system.60
On the other hand, the International Classification of Diseases 10 version (ICD-10) includes the category dissociative (conversion) disorders, which comprises the diagnoses of hysteria, conversion hysteria, hysterical psychosis, conversion reaction, and dissociative seizures from other nomenclatures.61 Regarding the ICD-10, PNES are classified within mental and behavioral disorders as somatoform disorders and dissociative (conversion) disorders, a category of neurotic disorders and stress-related disorders. Dissociative (conversion) disorders are characterized by the partial or complete loss of normal integration between certain memories of the past, awareness of one’s own identity and sensations of loss of control of body movements.61 However, some differences in the diagnostic categories were proposed by the International Classification of Diseases 11 version (ICD-11).62 In the chapter about mental, behavioral or neurodevelopmental disorders, dissociative disorders were included to separate somatic symptoms from those related to the perception or awareness, of the individual identity and the environment. The ICD 11 also added the dissociative identity disorder and the partial dissociative disorder, as separated diagnoses. The ICD 11 deleted any reference to multiple personality disorder and the conversion classification, including the neurotic, the somatoform and the stress-related disorder.62
Psychiatric Comorbidities in Patients with PNES
Patients with PNES comprise a heterogeneous group from a psychiatric point of view3,17,21,22 and may be considered as a clinical syndrome that is frequently associated with psychiatric comorbidities. These comorbidities constitute the underlying cause of PNES in many cases, such as PTSD (post-traumatic stress disorder), however in other patients a psychiatric comorbidity may be a trigger for PNES or a consequence of chronic PNES.4,8,17,22
Among psychiatric comorbidities, depression is the most frequent psychiatric disorder which can occur in approximately 60% of PNES or more.17,22,63–65 Secondly, traumatic experiences and the post-traumatic stress disorder (PTSD) have been found in approximately 50% of patients with PNES, followed by anxiety disorders in 45%, according to different studies.22,63–66 In addition, the clinical presentation of patients with PNES is even more complex when personality disorders are presented as a psychiatric comorbidity since they can contribute to the poor psychosocial functioning.22,64 Within the personality disorders, cluster B disorders (borderline personality disorder), are the most frequently reported. Cluster C personality disorders have been also reported among patients with PNES.22,64
Although the causes of PNES are multifactorial and they result from the combination of biological, psychological, environmental and social factors, patients with PNES report high rates of general trauma. Traumatic experiences constitute the most important factor involved in the etiology of the PNES. The history of traumatic events were found between 44% and 100% and the prevalence of sexual abuse has been reported ranging between 23% and 77% of patients with PNES.17,34,37,65 Trauma was associated with the activation of dissociation mechanisms and with a high prevalence of comorbid depression and personality disorders.1,21,22,65,66
Therapeutic Approaches of Patients with PNES
The first therapeutic strategy after confirming the diagnosis of PNES consists of informing to the patient and his family of the nonepileptic origin of the seizures, through a psychoeducation intervention.67 This type of initial intervention seeks to raise awareness of the diagnosis and the psychogenic origin of the problem. In a pioneering study in 1998, the use of the health system before and after carrying out the VEEG, was compared in patients with PNES.68 In this report, a clear explanation on PNES diagnosis, combined with immediate psychological treatment, markedly reduced the use of medical services. In addition, a brief and clear communication of the diagnosis can remit the symptoms in a certain proportion of patients.69 It is important that the communication of the diagnosis refers to an adequate, clear and understandable explanation for the patient and relatives, and ideally, both neurologist and mental health professionals should participate.4,8,28 In sum, how the diagnosis is communicated is very important. Communication with the new diagnosis has been reported to have consequences on the evolution of seizures.70,71 In our experience, patients who did not accept the newly diagnosis have shown a worse outcome.19
Since PNES are frequently mistakenly considered as epileptic seizures, most patients with PNES have received antiepileptic medication (AE) for long periods.22 The International League Against Epilepsy (ILAE) defines drug-resistant epilepsy (DRE) when seizure control fails with at least two AE schemes (either in monotherapy or in combination).72 Patients with PNES are usually diagnosed as DRE, and they also tend to suffer the imposition of stigma and restrictions on the lifestyle of patients with DRE.3,21,22 On the other hand, AE can generate adverse effects, toxicity and unnecessary high costs for the patient and/or the health system. Once the diagnosis of PNES is made, and as long as there are no comorbid epileptic seizures, the treating neurologist will gradually discontinue the AE medication while the patient simultaneously starts the treatment of choice (mental health treatment, psychotherapy and/or psychotropic medication, interdisciplinary approach).8
After the diagnosis has been explained to the patient and the family, patients with PNES should be addressed by the mental health team.74 The core symptoms of PNES (types of conversion and dissociation symptoms), the presence of comorbid psychiatric disorders potentially treatable with specific medication (ie, depressive disorders, anxiety disorders and post-traumatic stress disorders), and the presence of comorbidity with personality disorders, should be evaluated in each case in particular.8,17,67,73 Antidepressants are frequently indicated when depression comorbidity is present, and also to treat post-traumatic stress disorder. Sertraline showed reduction of PNES after patients received sertraline in combination with cognitive behavioral therapy.75 At the moment, there are no specific drugs with efficacy to treat conversion and/or dissociative symptoms (the core symptoms of PNES), and the treatment of choice is psychotherapy.76–89
Psychotherapeutic Interventions for Patients with PNES
Psychotherapy is a priority for treating PNES. The therapeutic approaches for patients with PNES are varied and depends on the diagnoses and comorbidities presented by these patients. Psychotherapeutic interventions and coping strategies specially oriented to PNES have been developed with the aim to improve the quality of life of the patients. The main studies reported in the literature about psychotherapeutic interventions for patients with PNES are summarized in Table 2.
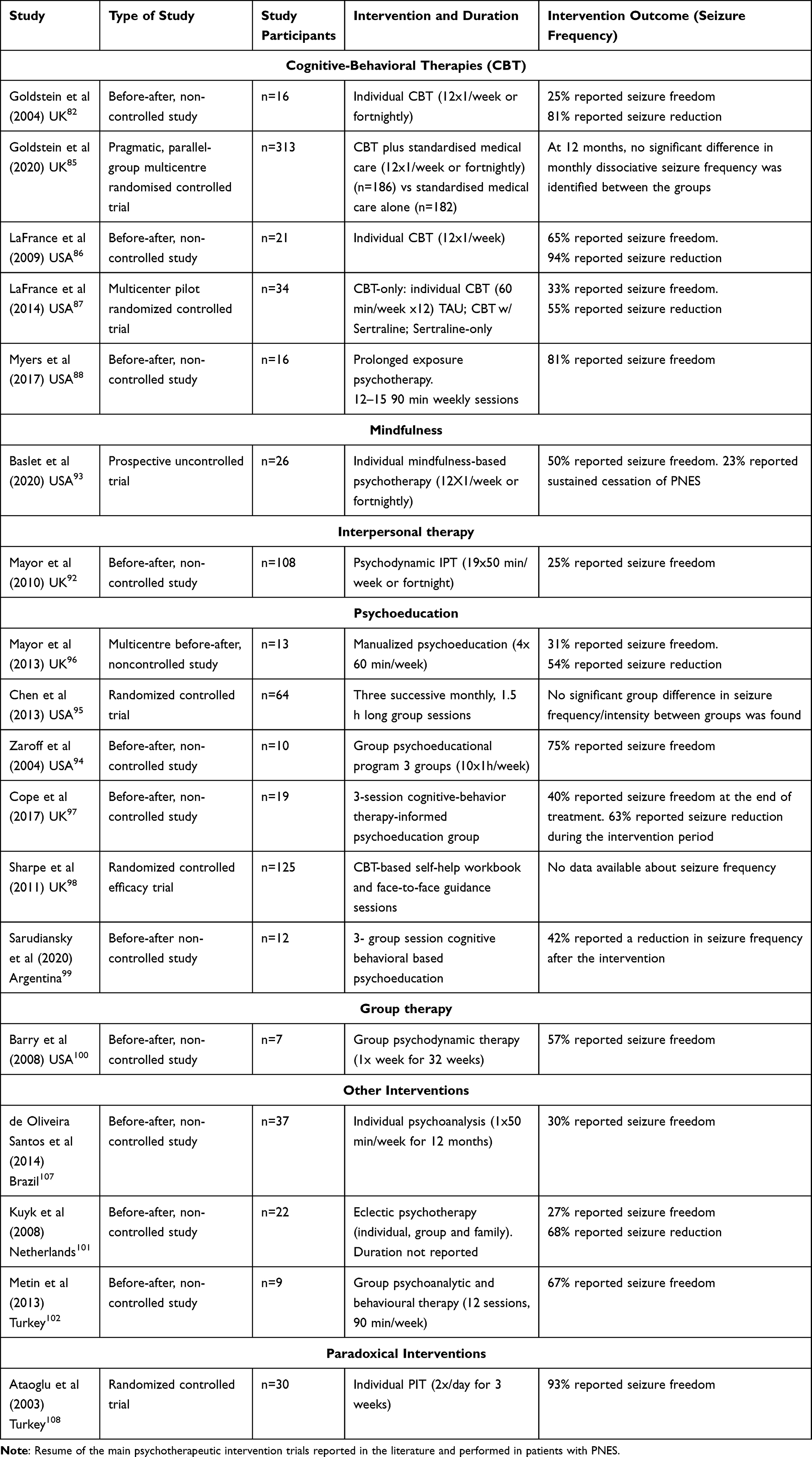 |
Table 2 Psychotherapeutic Interventions in Patients with PNES |
Cognitive-Behavioral Therapies
Cognitive-Behavioral Therapy (CBT) has been effective in the treatment of somatoform disorders of DSM-IV according randomized and controlled studies.80 Also, CBT has a proven effectiveness for depression and anxiety disorders,81 frequently associated with the development and maintenance of PNES. Thus, different manualized cognitive-behavioral treatments have been developed for patients with PNES.
Goldstein et al developed a treatment based on the fear, escape or avoidance model, which considers PNES as dissociative responses to different signals (cognitive, emotional, physiological or environmental).82,83 Such responses would be associated with extremely stressful or dangerous experiences, for example, abuse or trauma, which have produced unbearable feelings of fear and discomfort in early life.82,8382,83 With this theoretical foundation, based on the research of Chalder,8584 Goldstein presented a 12-session model focused on the cognitive, emotional, physiological and behavioral aspects of PNES.8483 This treatment proposes home works and psychoeducational bibliography about PNES and has five clearly differentiated stages: 1) Commitment to treatment and rational explanation; 2) Techniques for controlling pseudo-seizures; 3) Exposure techniques to reduce avoidance; 4) Management of cognitions and emotions related to seizures; and 5) Relapse prevention. This model has a randomized and controlled study in which cognitive-behavioral therapy is compared with Standard Medical Care (SMC). SMC included supervised withdrawal of antiepileptic drugs, and supportive sessions in which explanations about the psychological bases of seizures were provided. Results indicated that CBT in addition to SMC, significantly reduced seizure frequency in patients with PNES, in comparison to SMC alone.
Recently, the CODES group – Cognitive and Behavioral Approach for the treatment of Dissociative [non-epileptic] Seizures – published the results of a multicenter randomized controlled trial, which compared the effectiveness of a 12-session CBT protocol plus standardized medical care with SMC alone, for the reduction of dissociative seizure frequency. The authors concluded that although CBT did not show benefit to seizure frequency after 12 months, improvements in other outcome measures, such as psychosocial functioning were reported.8685
The model developed by LaFrance was based on the assumption that patients with PNES have had traumatic experiences that lead them to develop maladaptive core beliefs, cognitive distortions and somatic symptoms. The 12-session treatment aimed to promote behavioral changes generate greater self-control and self-efficacy. It has been specially designed for patients with PNES for the treatment of seizures and their comorbidities. The results showed that, of 21 participants, 16 had managed to reduce seizures by 50% and 11 of the 17, were seizure-free at the end of treatment.86 In a subsequent study, a randomized controlled trial was conducted with 35 patients with a diagnosis of PNES confirmed by VEEG. These patients were assigned to four treatments: Antidepressant Medication (Sertraline), CBT, CBT and Medication, and Standard medical treatment. The CBT intervention showed a significant reduction in seizures, and an improvement in general functioning and symptoms. The combination of CBT and Medication showed improvements, but less than the application of antidepressant alone. Medication showed signs of improvement, while standard medical treatment did not show any decrease of PNES.87
Also, based on trauma as a key aspect for PNES occurrence, Myers et al88 applied a modified protocol of Prolonged Exposure (PE) psychotherapy to 16 adult patients with VEEG-confirmed PNES and PTSD. PE consisted of 12–15 90-minute sessions, which included psychoeducation about trauma an PTSD, different techniques such as breathing retraining, sensory grounding, deep breathing, and exposure to real life situations, places, and activities associated to the traumatic event. Authors affirm that PE was effective in reducing seizure frequency, and also improving symptoms related to PTSD and mood disorders.88
Interpersonal Therapy
A brief psychodynamic interpersonal therapy was developed for patients with PNES.89 The authors adapted the brief psychodynamic interpersonal therapy model and combined it with an adapted model for functional somatic disorders.90,91 They proposed an empathetic approach, aimed at improving coping styles and promoting patient collaboration. This model assumes that the patient’s problems originate or are exacerbated by disturbances in their significant personal relationships, with dysfunctional interpersonal patterns, which are related to the patient’s symptoms. This approach uses different types of hypotheses: “comprehensive hypotheses”, to promote awareness of feelings; “Linking hypothesis”, to establish connections between current feelings and other feelings; and “explanatory hypotheses”, aimed at looking for possible underlying reasons for the patient’s behaviors. These hypotheses seek to facilitate the identification and change of dysfunctional patterns in interpersonal relationships, and a more effective processing of current and past painful emotions. Treatment consists of an initial 2-hour semi-structured interview, followed by up to nineteen therapy sessions of approximately 50 minutes, weekly or at two-week intervals. In the first session, it is expected to a) Create an initial commitment; b) Develop a case formulation. To do this, an individualized PPPT (predisposing, precipitating and perpetuating factors and seizure triggers) model is used, based on the history of symptoms, life chronology, interpersonal relationships, current life stressors, coping resources; c) Change the illness perception; d) Control of symptoms, through breathing and relaxation techniques. The objectives of the subsequent sessions are increase independence, introducing strategies that promote autonomy and self-care; to include caregivers and other health professionals; to improve the emotional process encouraging patients to communicate their feelings; trauma processing. When evaluating the efficacy of this model on 108 patients, the authors found that between 12 and 60 months after the end of therapy, 25% of the patients were seizure-free and 40% presented a 50% reduction; furthermore, the use of health services had decreased significantly.93
Mindfulness
Mindfulness-based therapies (MBT) are those psychotherapeutic approaches that promote self-regulation of attention, and the adoption of an attitude of curiosity, openness, and acceptance towards one’s own experience at each moment. Baslet et al developed a manualized 12-session MBT program for PNES. The program is organized in 5 modules and includes psychoeducation, stress management strategies, mindfulness for everyday life, emotion management, and relapse prevention. The results indicated improvements, with a lower seizure frequency and intensity, and a better quality of life.93
Psychoeducation
Psychoeducation is one of the central aspects of treatment for patients with PNES. Given the difficulties that many patients have in understanding this condition, explanatory and educational modules about PNES have been included in most of the interventions. Interventions aimed solely to promoting understanding of PNES, have also been proposed. Also, most psychoeducational approaches are designed in a group format, which in turn, support a better efficiency of mental health resources.
One of the first psychoeducational interventions has been proposed by Zaroff et al in USA.94 It consisted of 10 weekly sessions, aimed to explaining the psychogenic origin of seizures and the associated aspects such as anxiety and depression. In addition, the role of trauma was also introduced and explained. This intervention was conducted with 7 patients with PNES, but the authors did not report a significant decrease in seizure frequency. However, they reported improvements in PTSD symptoms and dissociation, as well as in patients’ perceived quality of life.
Also, in USA, Chen et al developed an intervention that consisted of 3 monthly meetings. They offered information regarding the relationship between physical symptoms and emotions, and strategies oriented to promote frustration tolerance and relaxation, among others.95 The authors compared the effects of the intervention, with a control group. Similar to Zaroff et al, the authors did not report a significant reduction in the frequency or in the intensity of the PNES. However, they did find that patients who participated in the psychoeducational intervention showed improvements in psychosocial aspects, and reduced the use of health services.
In the UK, Mayor et al reported the results of a before-and-after study of a four-session psychoeducational treatment.96 This study included explanations regarding the mind–body relationship, relaxation, distraction exercise, execution of avoided activities, among other interventions. In this study, almost half of the patients reported a significant decrease in the frequency of PNES.
Another psychoeducational intervention has been proposed by Sharpe et al, who used a CBT intervention that included both face-to-face sessions and bibliotherapy. When comparing this intervention with the usual treatment, the authors reported improvements of the symptoms. Nevertheless, no reports regarding seizure frequency were exposed.97
Also based on CBT, Cope et al have proposed a three-session group psychoeducational intervention for patients with functional neurological disorders, with and without epilepsy. The authors reported that almost 40% of the patients finished the treatment without PNES, and that approximately 75% reported a significant decrease in seizure frequency.98 They also reported improvements in illness perception, especially regarding concerns about duration, and a better understanding of the condition.
Psychoeducational interventions have also been applied in other cultures. For example, in our casuistic in Argentina, Sarudiansky et al investigated the effects before and after of a psychoeducational intervention for low-income patients with PNES.99 The results reported in 12 patients indicate that there was a significant reduction in seizure frequency in 40% of participants. Furthermore, in line with Cope et al, the patients also reported a reduction in the negative illness perception.98 Nevertheless, more studies in other non-Western (non-Caucasian) populations are needed, in order to provide cross-cultural evidence about the efficacy of psychoeducational interventions in patients with PNES.
Group Therapy and Family Interventions
Group therapies have shown variable results regarding the reduction of seizures, but have demonstrated improvements in psychological well-being in patients with PNES.100–102
Other studies evaluated the efficacy of family therapy in patients with PNES. It has been found that the families of patients with PNES would be more conflictive than those of patients with epilepsy.103104,105 McMaster’s family therapy model has been applied to patients with PNES,106 yielding positive results.106
Psychodynamic Therapies for Patients with PNES
The treatments for patients with PNES based on the psychoanalytic concept of trauma, using principles of Anna Freud’s ego psychology and object relations theory, have been also reported. De Oliveira Santos et al applied individual psychoanalysis, and reported a 30% of seizure-freedom in patients with PNES.107
Eye Movement Desensitization and Reprocessing, and Paradoxical Interventions for Patients with PNES
EMDR has been proposed for the treatment of PNES given its use as a therapeutic strategy in patients with post-traumatic stress disorder (PTSD). However, it has not shown sufficient positive results in the treatment of PNES, either as a first-line treatment or as part of a battery of interventions.89 Paradoxical interventions showed a reduction in conversion seizures and in the anxiety levels.108 Nevertheless, the research carried out on this type of interventions is still scarce.
Discussion
In this manuscript, we carried out a state-of-the-art review, with the aim to provide a critical approach to the extensive literature about PNES, focusing on diagnostic aspects, the primary management, and the available treatments that have been shown to be effective for the improvement of PNES.
As well the recognition of PNES increased significantly in the last years following the setting-up of VEEG, PNES still constitute a serious mental health unresolved problem. PNES are prevalent among patients admitted for intractable seizures or referred to epilepsy centers. However, the interdisciplinary approach, involving the neurologist, the psychiatrist and the psychologist, is essential for the correct diagnosis and treatment of patients with PNES.26–29 Furthermore, there is a delay of several years to reach PNES diagnosis in different countries, which is still too long and too late to implement the correct treatment.22,29,30 The difficulties accessing to VEEG which is privative of specialized centers of epilepsy make this access even more difficult.22,29,30 The PNES syndrome constitute a mental health problem to be treated by psychiatrists and psychologists, nevertheless a misdiagnosis between PNES and epilepsy is very frequent.29,30,34–36 According to the semiology, PNES may have some clinical differences comparing epileptic seizures nevertheless, differential diagnosis based only on clinical semiology is sometimes very difficult and the VEEG is the complementary method of choice, to confirm the differential diagnosis.44,45
Most patients with PNES present at least one current and recognizable psychiatric disorder and many studies showed high rates of somatization, conversive and dissociative disorders, in combination with other comorbid disorders such as depression. The history of sexual abuse, trauma and posttraumatic stress disorder (PTSD) have been considered etiopathogenic factors.3,17,21,22,63–65 Indeed, a mental health approach for patients with PNES is mandatory. In addition, for treating PNES, psychotherapy is the first-line treatment.67,69
In the last decades psychotherapeutic interventions have been proposed from different theoretical models (cognitive behavioral therapy, psychoanalysis, interpersonal therapy, etc.). However, more controlled studies are needed to increase empirical support for these treatments. Likewise, increasing cross-cultural researches are desirable to enhance representation of other countries and cultures.25,99 Despite this, patient improvements continue to be partial and different lines of research should be continued in the future. For sum, the individualization of the treatment for each patient, is highly recommended.
Disclosure
The authors reported no conflicts of interest for this work.
References.
1. BasletGP. Psychogenic non-epileptic seizures: amodel of their pathogenic mechanism. Seizure. 2011;20(1):1–13. doi:10.1016/j.seizure.2010.10.032
2. Brown RJ, Reuber M. Towards an integrative theory of psychogenic non-epileptic seizures (PNES). Clin Psychol Rev. 2016;47:55–70. doi:10.1016/j.cpr.2016.06.003
3. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry. 1996;153(1):57–63. doi:10.1176/ajp.153.1.57
4. Reuber M. Psychogenic non-epileptic seizures: answers and questions. Epilepsy Behav. 2008;12(4):622–635. doi:10.1016/j.yebeh.2007.11.006
5. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology. 1964;14(1):41–49. doi:10.1212/WNL.14.1.41
6. Goodwin J, Gross M. Pseudoseizures and incest. Am J Psych. 1979;136(9):1231. doi:10.1176/ajp.136.9.1231
7. Brigo F, Igwe SC, Ausserer H, et al. Terminology of psychogenic nonepileptic seizures. Epilepsia. 2015;56(3):e21–e25. doi:10.1111/epi.12911
8. Scévola L, Korman GP, Oddo S, Kochen S, D`alessio L. Crisis no epilépticas de origen psicógeno: diagnóstico diferencial con la epilepsia, presentación clínica y abordaje terapéutico. Polemos Vertex. 2014;25:266–274.
9. Asadi-Pooya AA, Sperling MR. Epidemiology of psychogenic non-epileptic seizures. Epilepsy Behav. 2015;46:60–65. doi:10.1016/j.yebeh.2015.03.015
10. Goldstein LH, Mellers JD, Landau S, et al. Cognitive behavioural therapy vs standardised medical care for adults with Dissociative non-Epileptic Seizures (CODES): a multicentre randomised controlled trial protocol. BMC Neurol. 2015;15(1):98. doi:10.1136/jnnp-2015-311750.24
11. Kerr WT, Stern JM. We need a functioning name for PNES: consider dissociative seizures. Epilepsy Behav. 2020;105:107002. doi:10.1016/j.yebeh.2020.107002
12. Asadi-Pooya AA, Brigo F, Mildon B, Nicholson TR. Terminology for psychogenic nonepileptic seizures: making the case for “functional seizures”. Epilepsy Behav. 2020;104:106895. doi:10.1016/j.yebeh.2019.106895
13. Stone J, Campbell K, Sharma N, Carson A, Warlow CP, Sharpe M. What should we call pseudoseizures? The patient’s perspective. Seizure. 2003;12(8):568–572. doi:10.1016/s1059-1311(03)00055-4
14. Hall Patch L, Brown R, House A, et al. Acceptability and effectiveness of a strategy for communication of the diagnosis of psychogenic nonepileptic seizures. Epilepsia. 2010;51(1):70–78. doi:10.1111/j.1528-1167.2009.02099.x
15. LaFrance WC
16. Sarudiansky M, Lanzillotti AI, Areco Pico MM, et al. What patients think about psychogenic nonepileptic seizures in Buenos Aires, Argentina: a qualitative approach. Seizure. 2017;51:14–21. doi:10.1016/j.seizure.2017.07.004
17. Popkirov S, Asadi‐Pooya AA, Duncan R, et al. The aetiology of psychogenic non‐epileptic seizures: risk factors and comorbidities. Epileptic Disord. 2019;21(6):529–547. doi:10.1684/epd.2019.1107
18. Lesser RP. Psychogenic seizures. Neurology. 1996;46(6):1499–1507. doi:10.1212/wnl.46.6.1499
19. Silva W, Giagante B, Saizar R, et al. Clinical features and prognosis of nonepileptic seizures in a developing country. Epilepsia. 2001;42(3):398–401. doi:10.1046/j.1528-1157.2001.45299.x
20. Abubakr A, Kablinger A, Caldito G. Psychogenic seizures: clinical features and psychological analysis. Epilepsy Behav. 2003;4(3):241–245. doi:10.1016/s1525-5050(03)00082-9
21. D’Alessio L, Giagante B, Oddo S, et al. Psychiatric disorders in patients with psychogenic non-epileptic seizures, with and without comorbid epilepsy. Seizure. 2006;15(5):333–339. doi:10.1016/j.seizure.2006.04.003
22. Scévola L, Teitelbaum J, Oddo S, et al. Psychiatric disorders in patients with psychogenic non-epileptic seizures and drug-resistant epilepsy: a study of an Argentine population. Epilepsy Behav. 2013;29(1):155–160. doi:10.1016/j.yebeh.2013.07.012
23. Brown RJ, Reuber M. Psychological and psychiatric aspects of psychogenic non epileptic seizures (PNES): a systematic review. Clin Psychol Rev. 2016;45:157–182. doi:10.1016/j.cpr.2016.01.003
24. Kanemoto K, LaFrance WC
25. Korman GP, Sarudiansky M, Lanzillotti AI, et al. Long-term outcome in a sample of underprivileged patients with psychogenic nonepileptic seizures (PNES) living in Argentina. Epilepsy Behav. 2019;94:183–188. doi:10.1016/j.yebeh.2019.03.005
26. Duncan R, Razvi S, Mulhern S. Newly presenting psychogenic nonepileptic seizures: incidence, population characteristics, and early outcome from a prospective audit of a first seizure clinic. Epilepsy Behav. 2011;20(2):308–311. doi:10.1016/j.yebeh.2010.10.022
27. Benbadis SR, Allen Hauser W. An estimate of the prevalence of psychogenic non-epileptic seizures. Seizure. 2000;9(4):280–281. doi:10.1053/seiz.2000.0409
28. Reuber M, Elger CE. Psychogenic non-epileptic seizures: review and update. Epilepsy Behav. 2003;4(3):205–216. doi:10.1016/S1525-5050(03)00104-5
29. LaFrance WC
30. Reuber M, Fernandez G, Bauer J, Helmstaedter C, Elger CE. Diagnostic delay in psychogenic nonepileptic seizures. Neurology. 2002;58(3):493–495. doi:10.1212/wnl.58.3.493
31. Van Merode T, De Krom M, Andre Knottnerus J. Gender-related differences in non-epileptic attacks: a study of patients’ cases in the literature. Seizure. 1997;6(4):311–316. doi:10.1016/s1059-1311(97)80079-9
32. Rosenbaum M. Psychogenic Seizures: why Women? Psychosomatics. 2000;41(2):147–149. doi:10.1176/appi.psy.41.2.147
33. Oto M, Conway P, McGonigal A, Russell A, Duncan R. Gender differences in psychogenic non-epileptic seizures. Seizure. 2005;14(1):33–39. doi:10.1016/j.seizure.2004.02.008
34. Asadi-Pooya AA, Valente K, Alessi R, et al. Semiology of psychogenic nonepileptic seizures: an international cross-cultural study. Epilepsy Behav. 2017;75:210–212. doi:10.1016/j.yebeh.2017.08.016
35. Asadi-Pooya AA, Valente K, Restrepo AD, et al. Adult-onset psychogenic nonepileptic seizures: a multicenter international study. Epilepsy Behav. 2019;98:36–39. doi:10.1016/j.yebeh.2019.06.013
36. Asadi-Pooya AA, Myers L, Valente K, et al. Sex differences in demographic and clinical characteristics of psychogenic nonepileptic seizures: a retrospective multicenter international study. Epilepsy Behav. 2019;97:154–157. doi:10.1016/j.yebeh.2019.05.045
37. Asadi-Pooya AA, Bahrami Z. Sexual abuse and psychogenic nonepileptic seizures. Neurol Sci. 2019;40(8):1607–1610. doi:10.1007/s10072-019-03887-3
38. Myers L, Trobliger R, Bortnik K, Lancman M. Are there gender differences in those diagnosed with psychogenic nonepileptic seizures? Epilepsy Behav. 2018;78:161–165. doi:10.1016/j.yebeh.2017.10.019
39. Myers L, Perrine K, Lancman M, Fleming M, Lancman M. Psychological trauma in patients with psychogenic nonepileptic seizures: Trauma characteristics and those who develop PTSD. Epilepsy Behav. 2013;28:121–126. doi:10.1016/j.yebeh.2013.03.033
40. Sawchuk T, Asadi-Pooya AA, Myers L, et al. Clinical characteristics of psychogenic nonepileptic seizures across the lifespan: an international retrospective study. Epilepsy Behav. 2020;102:106705. doi:10.1016/j.yebeh.2019.106705
41. Krumholz A. Non-epileptic seizures: diagnosis and management. Neurology. 1999;53(5Suppl2):S76–S83.
42. Alsaadi TM, Thieman C, Shatzel A, Farias S. Video-EEG telemetry can be a crucial tool for neurologists experienced in epilepsy when diagnosing seizure disorders. Seizure. 2004;13(1):32–34. doi:10.1016/S1059-1311(03)00072-4
43. Lombardi N, Scévola L, Sarudiansky M, et al. Differential semiology based on video electroencephalography monitoring between psychogenic nonepileptic seizures and temporal lobe epileptic seizures. Psychosomatics. 2020. doi:10.1016/j.psym.2020.07.003
44. Lobello K, Morgenlander J, Radtke R, Buschnell C. Video/EEG monitoring in the evaluation of paroxysmal behavioral events: duration, effectiveness, and limitations. Epilepsy Behav. 2006;8(1):261–266. doi:10.1016/j.yebeh.2005.10.010
45. Peguero E, Abou-Khalil B, Fakhoury T, Mathews G. Self-Injury and Incontinence in psychogenic seizures. Epilepsia. 1995;36(6):586–591. doi:10.1111/j.1528-1157.1995.tb02572.x
46. Saygi S, Katz A, Marks DA, Spencer SS. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology. 1992;42(7):1274–1277. doi:10.1212/WNL.42.7.1274
47. Walczak T, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia. 1996;37(2):208–210. doi:10.1111/j.1528-1157.1996.tb00013.x
48. Gröppel G, Kapitany T, Baumgartner C. Cluster analysis of clinical seizure semiology of psychogenic nonepileptic seizures. Epilepsia. 2000;41(5):610–614. doi:10.1111/j.1528-1157.2000.tb00216.x
49. Selwa LM, Geyer J, Nikakhtar N, Brown MB, Schuh LA. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia. 2000;41(10):1330–1334. doi:10.1111/j.1528-1157.2000.tb04613.x
50. Seneviratne U, Reutens D, Souza WD. Stereotypy of psychogenic nonepileptic seizures: insights from video-EEG monitoring. Epilepsia. 2010;51(7):1159–1168. doi:10.1111/j.1528-1167.2010.02560.x
51. Hubsch C, Baumann C, Gospodaru N, Vignal J, Hervé V, Maillard L. Clinical classification of psychogenic non-epileptic seizures based on video-EEG analysis and automatic clustering. J Neurol Neurosurg Psychiatry. 2011;82(9):955–960. doi:10.1136/jnnp.2010.235424
52. Yalinay DP, Unlusoy Acar Z, Gurses C. Clinical events in sychogenic non-epileptic seizures based on semiological seizure classification. Neurol Res. 2013;35(10):1070–1075. doi:10.1179/1743132813Y.0000000249
53. Wadwekar V, Pankajakshan P, Murgai A. Semiologic classification of psychogenic non epileptic seizures (PNES) based on video EEG analysis: do we need new classification systems? Seizure. 2014;23(3):222–226. doi:10.1016/j.seizure.2013.12.005
54. Magaudda A, Laganà A, Calamuneri A, et al. Validation of a novel classification model of psychogenic nonepileptic seizures by video-EEG analysis and a machine learning approach. Epilepsy Behav. 2016;60:197–201. doi:10.1016/j.yebeh.2016.03.031
55. Madaan P, Gulati S, Chakrabarty B, et al. Clinical spectrum of psychogenic non epileptic seizures in children; an observational study. Seizure. 2018;59:60–66. doi:10.1016/j.seizure.2018.04.024
56. Devinsky O, Putman FW, Grafman J. Dissociation states and epilepsy. Neurology. 1989;39(6):835–840. doi:10.1212/WNL.39.6.835
57. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR. Barcelona: Masson; 2002.
58. Pick S, Mellers JDC, Goldstein LH. Dissociation in patients with dissociative seizures: relationship with trauma and seizure symptoms. Psychol Med. 2017;47(7):1215–1229. doi:10.1017/S0033291716003093
59. Reuber M, House AO, Pukrop R, Bauer J, Elger CE. Somatization, dissociation and general psychopathology in patients with psychogenic non-epileptic seizures. Epilepsy Res. 2003;57(2–3):159–167. doi:10.1016/j.eplepsyres.2003.11.004
60. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. VA: American Psychiatric Publishing; 2013.
61. WorldHealth Organization. International Classification of Diseases and Related Health Problems, 10th Revision. Ginebra: WHO; 1992.
62. WorldHealth Organization. International Classification of Diseases and Related Health Problems, 11th Revision. Ginebra: WHO; 2019.
63. Galimberti CA, Ratti MT, Murelli R, et al. Patients with psychogenic non-epileptic seizures, alone or epilepsy-associated, share a psychological profile distinct from that of epilepsy patients. J Neurol. 2003;250(3):338–346. doi:10.1007/s00415-003-1009-0
64. Bailles E, Pintor L, Fernandez-Egea E, Torres X, Matrai S, Arroyo S. Psychiatric disorders, trauma, and MMPI profile in Spanish sample of non epileptic seizure patients. Gen Hosp Psychiatry. 2004;26(4):310–315. doi:10.1016/j.genhosppsych.2004.04.003
65. Fiszman A, Alves-Leon SV, Nunes RG, D’Andrea I, Figueira I. Traumatic events and posttraumatic stress disorder in patients with psychogenic non-epileptic seizures: a critical review. Epilepsy Behav. 2004;5(6):818–825. doi:10.1016/j.yebeh.2004.09.002
66. Arnold LM, Privitera MD. Psychopathology and trauma in epileptic and psychogenic seizure patients. Psychosomatics. 1996;37(5):438–443. doi:10.1016/S0033-3182(96)71531-1
67. LaFrance WC
68. Martin RC, Gilliam FG, Kilgore M, Faught E, Kuzniecky R. Improved health care resource utilization following video-EEG-confirmed diagnosis of nonepileptic psychogenic seizures. Seizure. 1998;7(5):385–390. doi:10.1016/S1059-1311(05)80007-X
69. Duncan R, Horwood J, Razvi S, Mulhern S. Psychogenic nonepileptic seizures that remit when the diagnosis is given: just good luck? Epilepsy Behav. 2020;102:106667. doi:10.1016/j.yebeh.2019.106667
70. Carton S, Thompson PJ, Duncan JS. Non-epileptic seizures: patients’ understanding and reaction to the diagnosis and impact on outcome. Seizure. 2003;12(5):287–294. doi:10.1016/S1059-1311(02)00290-X
71. Thompson R, Isaac CL, Rowse G, Tooth CL, Reuber M. What is it like to receive a diagnosis of nonepileptic seizures? Epilepsy Behav. 2009;14(3):508–515. doi:10.1016/j.yebeh.2008.12.014
72. Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, French J. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE commission on therapeutic strategies. Epilepsia. 2010;51(6):1069–1077. doi:10.1111/j.1528-1167.2009.02397.x
73. Wiseman H, Reuber M. New insights into psychogenic nonepileptic seizures 2011–2014. Seizure. 2015;29:69–80. doi:10.1016/j.seizure.2015.03.008
74. LaFrance WC
75. Baird GL, Harlow LL, Machan JT, LaFrance WC
76. Barrett-Naylor R, Gresswell DM, Dawson DL. The effectiveness and acceptability of a guided self-help Acceptance and Commitment Therapy (ACT) intervention for psychogenic nonepileptic seizures. Epilepsy Behav. 2018;88:332–340. doi:10.1016/j.yebeh.2018.09.039
77. Clegg S, Sirois F, Reuber M. Self-compassion and adjustment in epilepsy and psychogenic nonepileptic seizures. Epilepsy Behav. 2019;100(PtA):106490. doi:10.1016/j.yebeh.2019.106490
78. Goldstein LH, Robinson EJ, Mellers JDC, et al. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial. Lancet Psychiatry. 2020;7(6):
79. Labuddaa K, Frauenheim M, Miller I, Schrecke M, Brandt C, Bien CG. Outcome of CBT-based multimodal psychotherapy in patients with psychogenic nonepileptic seizures: a prospective naturalistic study. Epilepsy Behav. 2020;106:107029. doi:10.1016/j.yebeh.2020.107029
80. Kroenke K. Efficacy of treatment for somatoform disorders: a review of randomized controlled Trials. Psychosom Med. 2007;69(9):881–888. doi:10.1097/psy.0b013e31815b00c4
81. Beck AT. The current state of Cognitive Therapy. Arch Gen Psychiatry. 2005;62(9):953–959. doi:10.1001/archpsyc.62.9.953
82. Goldstein LH, Deale AC, Mitchell-O’Malley S, Toone BK, Mellers J. An evaluation of cognitive behavioral therapy as a treatment for dissociative seizures: a pilot study. Cogn Behav Neurol. 2004;17(1):41–49. doi:10.1097/00146965-200403000-00005
83. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive–behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology. 2010;74(24):1986–1994. doi:10.1212/wnl.0b013e3181e39658
84. Chalder T. Non-Epileptic attacks: a cognitive behavioural approach in a single case with a four-year follow-up. Clin Psychol Psychother. 1996;3(4):291–297. doi:10.1002/(sici)1099-0879(199612)3:4<291::aid-cpp72>3.0.co;2-h
85. Goldstein LH, Robinson EJ, Mellers JD, et al. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial. Lancet Psychiatry. 2020;7(6):491–505. doi:10.1016/S2215-0366(20)30128-0
86. LaFrance WC
87. LaFrance WC
88. Myers L, Vaidya-Mathur U, Lancman M. Prolonged exposure therapy for the treatment of patients diagnosed with psychogenic non-epileptic seizures (PNES) and post-traumatic stress disorder (PTSD). Epilepsy Behav. 2017;66:86–92. doi:10.1016/j.yebeh.2016.10.019
89. Howlett S, Reuber M. An augmented model of brief psychodynamic interpersonal therapy for patients with nonepileptic seizures. Psychotherapy. 2009;46(1):125–238. doi:10.1037/a0015138
90. Creed F, Dawson D, Tomenson B. A controlled trial of psychological treatment for the irritable bowel syndrome. Gastroenterology. 1991;100(2):450–457. doi:10.1016/0016-5085(91)90215-7
91. Creed F, Fernandes L, Guthrie E, et al. The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology. 2004;124(2):303–317. doi:10.1053/gast.2003.50055
92. Mayor R, Howlett S, Grunewald R, Reuber M. Long-term outcome of brief augmented psychodynamic interpersonal therapy for psychogenic nonepileptic seizures: seizure control and health care utilization. Epilepsia. 2010;51(7):1169–1176. doi:10.1111/j.1528-1167.2010.02656.x
93. Baslet G, Ehlert A, Oser M, Dworetzky BA. Mindfulness-based therapy for psychogenic nonepileptic seizures. Epilepsy Behav. 2020;103:106534. doi:10.1016/j.yebeh.2019.106534
94. Zaroff CM, Myers L, Barr WB, Luciano D, Devinsky O. Group psychoeducation as treatment for psychological nonepileptic seizures. Epilepsy Behav. 2004;5(4):587–592. doi:10.1016/j.yebeh.2004.03.005
95. Chen DK, Maheshwari A, Franks R, Trolley GC, Robinson JS, Hrachovy RA. Brief group psychoeducation for psychogenic nonepileptic seizures: a neurologist initiated program in an epilepsy center. Epilepsia. 2013;55(1):156–166. doi:10.1111/epi.12481
96. Mayor R, Brown RJ, Cock H, et al. A feasibility study of a brief psycho-educational intervention for psychogenic nonepileptic seizures. Seizure. 2013;22(9):760–765. doi:10.1016/j.seizure.2013.06.008
97. Sharpe M, Walker J, Williams C, et al. Guided self-help for functional (psychogenic) symptoms: a randomized controlled efficacy trial. Neurology. 2011;77(6):564–572. doi:10.1212/WNL.0b013e318228c0c7
98. Cope SR, Smith JG, King T, Agrawal N. Evaluation of a pilot innovative cognitive-behavioral therapy-based psychoeducation group treatment for functional non-epileptic attacks. Epilepsy Behav. 2017;70:238–244. doi:10.1016/j.yebeh.2017.02.014
99. Sarudiansky M, Korman GP, Lanzillotti AI, et al. Report on a psychoeducational intervention for psychogenic non-epileptic seizures in Argentina. Seizure. 2020;80:270–277. doi:10.1016/j.seizure.2020.04.008
100. Barry J, Wittenberg D, Bullock K, Michaels J, Classen C, Fisher R. Group therapy for patients with psychogenic nonepileptic seizures: a pilot study. Epilepsy Behav. 2008;13(4):624–629. doi:10.1016/j.yebeh.2008.06.013
101. Kuyk J, Siffels MC, Bakvis P, Swinkels WA. Psychological treatment of patients with psychogenic non-epileptic seizures: an outcome study. Seizure. 2008;17(7):595–603. doi:10.1016/j.seizure.2008.02.006
102. Metin SZ, Ozmen M, Metin B, Talasman S, Yeni SN, Ozkara C. Treatment with group psychotherapy for chronic psychogenic nonepileptic seizures. Epilepsy Behav. 2013;28(1):91–94. doi:10.1016/j.yebeh.2013.03.023
103. Krawetz P, Fleisher W, Pillay N, Staley D, Arnett J, Maher J. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis. 2001;189(1):38–43. doi:10.1097/00005053-200101000-00007
104. Moore PM, Baker GA, McDade G, Chadwick D, Brown S. Epilepsy, pseudoseizures and perceived family characteristics: a controlled study. Epilepsy Res. 1994;18(1):75–83. doi:10.1016/0920-1211(94)90035-3
105. Ryan CE, Epstein NB, Keitner GI, Miller IW, Bishop DS. Evaluating and Treating Families: The McMaster Approach. New York: Routledge; 2005.
106. Archambault RC, Ryan CE. Family therapy for patients diagnosed with psychogenic nonepileptic seizures (Chapter 33). In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s Nonepileptic Seizures.
107. de Oliveira Santos N, Benute GR, Santiago A, Marchiori PE, Lucia MC. Psychogenic non-epileptic seizures and psychoanalytical treatment: results. Rev Assoc Med Bras. 2014;60(6):577–584. doi:10.1590/1806-9282.60.06.018
108. Ataoglu A, Ozcetin A, Icmeli C, Ozbulut O. Paradoxical therapy in conversion reaction. J Korean Med Sci. 2003;18(4):581–584. doi:10.3346/jkms.2003.18.4.581
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.