")
Back to Journals » Infection and Drug Resistance » Volume 7
Update on management options in the treatment of nosocomial and ventilator assisted pneumonia: review of actual guidelines and economic aspects of therapy
Received 27 August 2013
Accepted for publication 4 October 2013
Published 18 December 2013 Volume 2014:7 Pages 1—7
DOI https://doi.org/10.2147/IDR.S25985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Michael Wilke,1 Rolf Grube1
1Dr. Wilke GmbH, Munich, Germany
Objective: Nosocomial or more exactly, hospital-acquired (HAP) and ventilator-associated pneumonia (VAP) are frequent conditions when treating intensive care unit (ICU) patients that are only exceeded by central line-associated bloodstream infections. In Germany, approximately 18,900 patients per year suffer from a VAP and another 4,200 from HAP. We therefore reviewed the current guidelines about HAP and VAP, from different sources, regarding the strategies to address individual patient risks and medication strategies for initial intravenous antibiotic treatment (IIAT).
Material and methods: We conducted an analysis of the recent guidelines for the treatment of HAP. The current guidelines of the American Thoracic Society, the treatment recommendations of the Paul-Ehrlich-Gesellschaft (PEG), the guidelines from the British Society for Antimicrobial Chemotherapy, the VAP guideline of the Canadian Critical Care trials group, as well as the new German S3-guideline for HAP were examined.
Results: All guidelines are based on grading systems that assess the evidence underlying the recommendations. However, each guideline uses different grading systems. One common aspect of these guidelines is the risk assessment of the patients for decision making regarding IIAT. Most guidelines have different recommendations depending on the risk of the presence of multidrug resistant (MDR) bacteria. In guidelines using risk assessment, for low-risk patients (early onset, no MDR risk) aminopenicillins with beta-lactamase inhibitors (BLI), second or third generation cephalosporins, quinolones, or ertapenem are recommended. For patients with higher risk, imipenem, meropenem, fourth generation cephalosporins, ceftazidime or piperacillin/tazobactam are recommended. The PEG recommendations include a combination therapy in cases of very high risk (late onset, MDR risk, ICU, and organ failure) of either piperacillin/tazobactam, dori-, imi- or meropenem or cefepime or ceftazidime with ciprofloxacin, levofloxacin, fosfomycin or an aminoglycoside. For the treatment of HAP caused by methicillin-resistant Staphylococcus aureus (MRSA), either linezolid or vancomycin is recommended. With regard to the ZEPHyR-trial, linezolid has shown higher cure rates but, no difference in overall survival. Economic analyses show the relevance of guideline-adherent IIAT (GA-IIAT). Besides significantly better clinical outcomes, patients with GA-IIAT cause significantly lower costs (€28,033 versus (vs) €36,139) (P=0.006) and have a shorter length of stay in hospital (23.9 vs 28.3 days) (P=0.022).
Conclusion: We conclude that most current treatment guidelines take into account the individual patient risk and that the correct choice of IIAT affects clinical as well as economical outcomes.
Keywords: nosocomial pneumonia, ventilator, assoc. pneumonia, antibiotics, guidelines, review
Introduction
When treating intensive care unit (ICU) patients, nosocomial infection or more exactly, hospital acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP) are frequent conditions only exceeded by central line−associated bloodstream infections.1 The epidemiologic data about HAP and VAP are associated with a relatively high level of uncertainty because of varying definitions and methodologies.
In Germany, according to data from the hospital infection surveillance system, [Krankenhaus-Infektions-Surveillance-System (KISS)], approximately 18,900 patients in an ICU per year suffer from a VAP, and another 4,200 suffer from HAP without being mechanically ventilated.2,3 In contrast, based on a query from the Federal Statistical Office, in 2011, HAP was coded in 103,040 cases in Germany (Statistisches Bundesamt, email communication, April, 2013).
In the United States, approximately five to ten HAP episodes per 1,000 hospital admissions occur4 or about 200 to 400 thousand HAP episodes per year, according to admission statistics from the US.5
The objective of this review paper was to give an overview of the current therapy guidelines for the treatment of HAP/VAP and to summarize the most common recommendations, to provide useful and practical information for clinical decision making. Moreover, the economic consequences of guideline-adherent initial intravenous antibiotic therapy (GA-IIAT) versus (vs) non-GA-IIAT was also examined.
Materials and methods
The current guidelines of the American Thoracic Society (ATS)4 and the British Society for Antimicrobial Chemotherapy (BSAC),6 the VAP guideline of the Canadian Critical Care trials group (CCCTG),7 as well as the new S3-guideline for HAP in Germany were included in this review.8 In addition, the treatment recommendations published by the Paul-Ehrlich-Gesellschaft (PEG) were reviewed as well.9,10
All guidelines were examined under the following criteria:
- Which system was used to grade the underlying evidence?
- Does the guideline contain risk assessment addressing the presence of complicated pathogens?
- Which treatment recommendations are given for initial intravenous antibiotic therapy (IIAT)?
We retrieved the original texts of all the guidelines as well as the level of evidence for each recommendation. Next we examined the guidelines as described above. We then summarized the results in tables, attempting to summarize the most common recommendations as well as their level of evidence. Finally we conducted a search for papers that examine the economic consequences of treatment in HAP, and these were reviewed.
Results
One common aspect of the guidelines we reviewed is the risk assessment of patients designed to guide decision making regarding the IIAT. All the guidelines use a system of risk assessment to determine the presence of bacteria that require special coverage when determining IIAT.
The reviewed guidelines differ in several aspects. The CCCTG guideline focuses on VAP, while the German guideline as well as the BSAC guideline and the PEG recommendation cover both HAP and VAP. The ATS guideline additionally discusses the newly introduced concept of health-care associated pneumonia (HCAP), as a third class of nosocomial pneumonias.
All guidelines use different approaches and terminology to measure evidence. The different systems are shown in Table 1. The effects of these differences are demonstrated by the recommendations about the duration of antibiotic therapy. The PEG recommends duration of 3−5 days after good clinical improvement, but not more than 10−14 days (grade C, BSAC, see Table 1). The ATS guideline recommends shortening the duration from 14−21 to 7 days in the absence of Pseudomonas aeruginosa and when the patient has had a good clinical response (level 1). The BSAC and the Canadian guideline recommend a maximum of 8 days in responding patients (BSAC: grade C; CCCTG: recommend). The German guideline gives a strong recommendation (grade A) for the duration of 8 days in regular cases (Table 1).
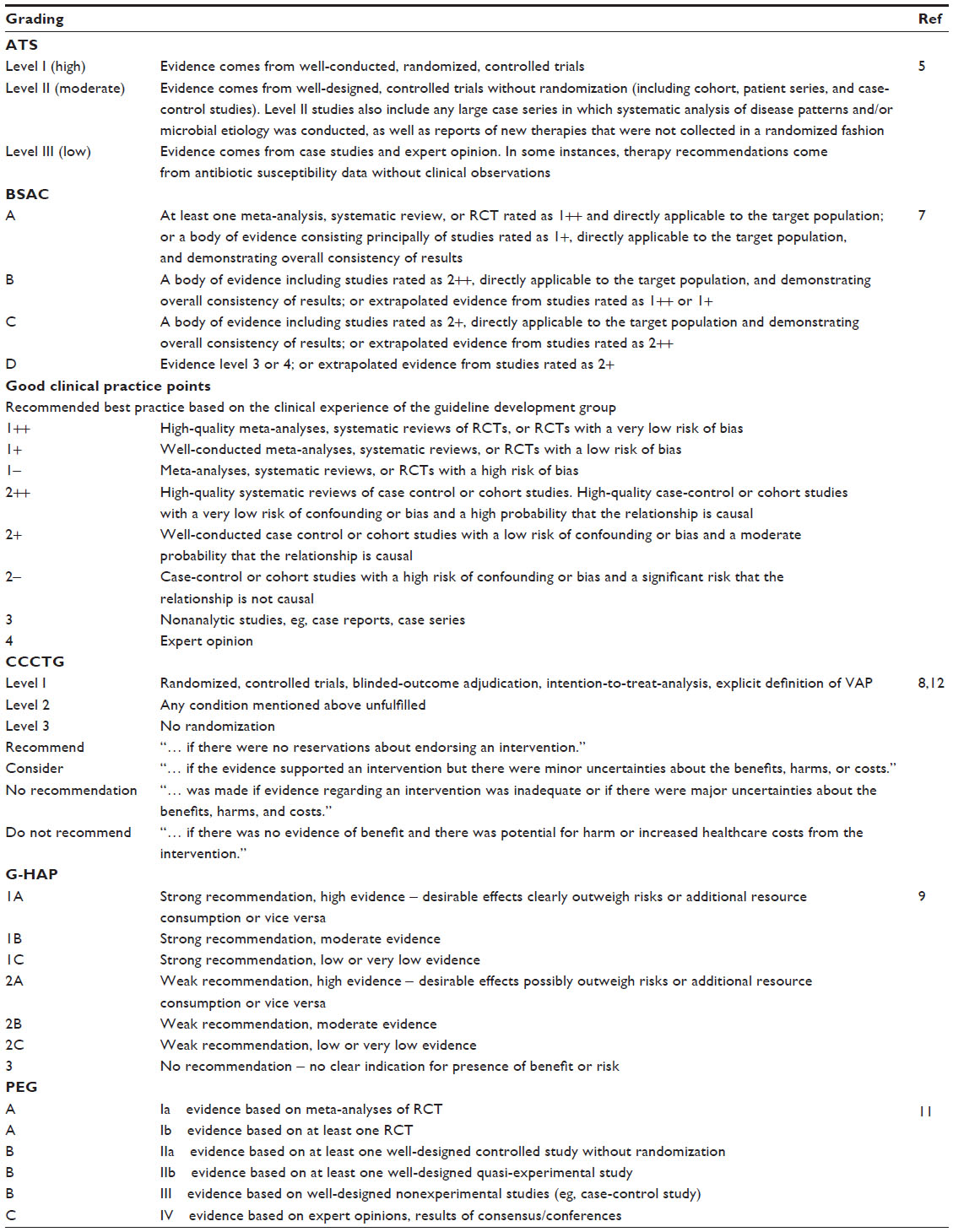 | Table 1 Synopsis of grading systems used in the respective guidelines |
Except for the CCCTG guideline, all the guidelines make use of risk stratification to a greater or lesser extent. The PEG recommendation uses a scoring system to allocate patients to groups based upon the Complicated Pathogen Risk assessment Score (CPRS).9 Based on the CPRS, groups of antibiotics are recommended to be used until the pathogens are identified by microbiological methods (Table 2). The pharmacological strategies for the IIAT are summarized in Table 3.
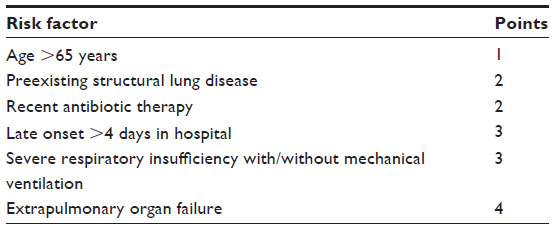 | Table 2 Score for risk factors influencing antibiotic strategy according to the PEG recommendation |
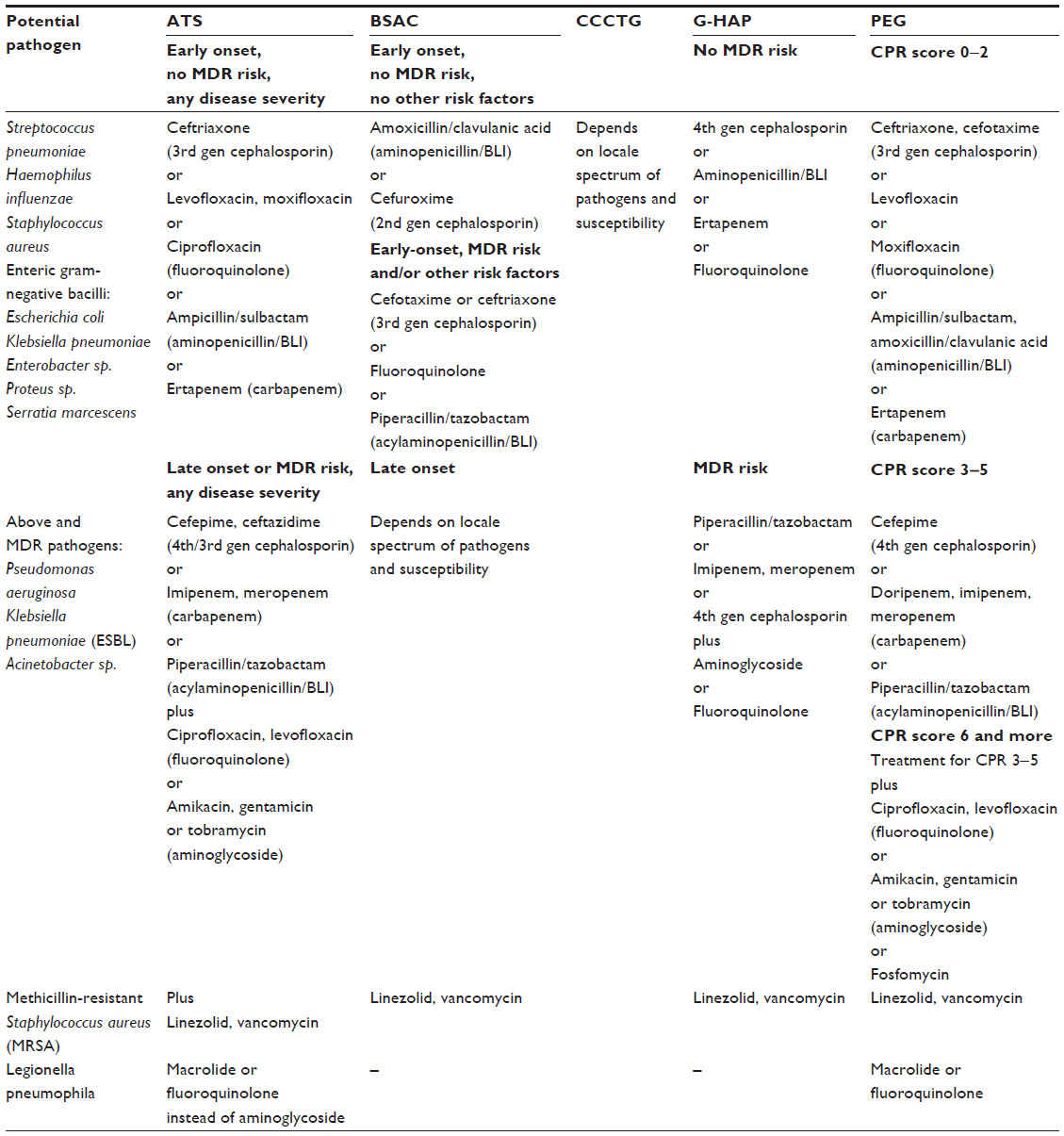 | Table 3 Overview of recommendations from all examined guidelines |
The topic of prevention is discussed in the ATS guideline, the PEG recommendation, as well as in the BSAC guideline but not in the German or the CCCTG guideline. The CCCTG published a separate guideline about VAP prevention.11
Table 3 provides an overview of the therapy recommendations for IIAT (where included in the guideline). The table shows that the guidelines examined have substantial differences in risk assessment. The PEG recommendations provide – using the CPRS – the most straightforward decision making process, which is easy to use in clinical practice.
For better comparability, we have defined the following classes for assessing the risk of complicated pathogens:
- No multidrug resistance (MDR) risk (early onset of pneumonia, no prior antibiotic therapy, no VAP, no comorbidities, and no other organ failure)
- Medium MDR risk (prior antibiotic therapy, late onset, and comorbidities)
- High MDR risk (late onset, VAP, prior antibiotic therapy, comorbidities, and organ failures)
Table 4 shows the most commonly given recommendations for treatment and the frequency with which the therapy is recommended in a guideline.
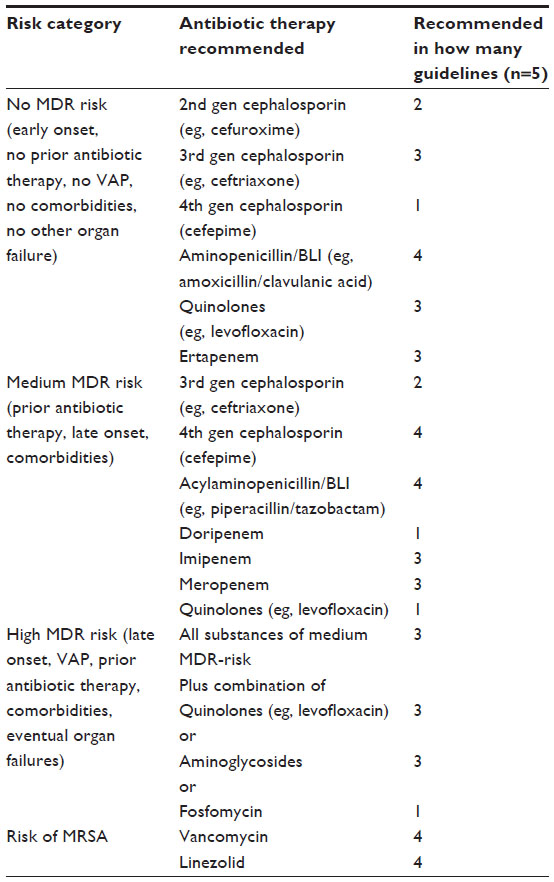 | Table 4 Most common recommendations risk-adjusted |
Discussion
Together, HAP and VAP are the second most reason of nosocomial infection and a substantial risk for hospitalized patients. Barbier et al showed, not only a rate up to 16 episodes per 1,000 ventilator days but also, attributable mortality of 3%−17%.12 In a retrospective matched cohort study comparing patients with VAP with patients without VAP, Kollef et al reported prolonged ventilation episodes (21.8 vs 10.3 days), ICU stay (20.5 vs 11.6 days), and hospital stay (32.6 vs 19.5 days), but a significantly lower mortality (22.5% vs 29.4%).13 The authors of the present article reported results of a retrospective study of HAP from five German tertiary care hospitals;14 in that study, the overall mortality of patients with HAP was 20.3%.
It can accordingly be concluded that adequate preventive, diagnostic and therapeutic measures can improve, not only economic outcome parameters but also, the clinical outcome of patients.
Comparing the details of the guidelines was difficult due to the different grading systems used. These different approaches clearly affect the quality of guidelines, as shown by Atkins et al15 as well as Aarts et al.16
The treatment of HAP is also an economic challenge for hospitals, especially in countries where payment is dependent on diagnosis-related groups (DRGs). Kollef et al reported the excess costs of VAP cases compared with ventilated patients who do not acquire VAP to be US$39,828,13 while Moller et al showed that the costs to prevent a VAP episode are only €4,451.17 Thompson et al18 found a significant difference in mortality (10.7% vs 1.2% [P<0.001]) when HAP occurred after abdominal surgery. The mean length of stay (LOS) for patients who developed HAP after intra-abdominal surgery was significantly greater compared with patients who did not develop HAP after intra-abdominal surgery (17.10 days vs 6.07 days) (P<0.001). After adjusting for patient characteristics, HAP was independently associated with a 75% mean increase in total hospital charges (US$28,160.95; 95% confidence interval: US$27,543.76–US$28,778.13).
Only very few analyses have examined the impact of the correct IIAT on clinical and economic outcomes. Piskin et al reported a significantly longer hospital LOS for patients receiving inadequate antibiotic therapy compared with patients receiving adequate antibiotic therapy (for HAP, this was +4.6 days [P=0.001]; for VAP, this was +16.4 days [P=0.009]).19 Inadequate IIAT was also shown to cause – besides worse clinical outcomes – the additional costs of €8,106 (P=0.006) and a prolongation of LOS of 4.5 days (P=0.022) in a retrospective analysis undertaken by the authors of the present article.14 In contrast, Kett et al designed a prospective observational multicenter study for VAP possibly caused by MDR pathogens. Their results showed a higher mortality of patients in the guideline-compliant group (34%) compared with the noncompliant group (20%)20 even when the models were adjusted for covariates. The authors do not exclude the possibility of unobserved factors that may influence mortality. Becher et al compared the effect of use of locally adjusted guidelines for HAP with the use of the ATS guideline, in retrospective data, and found better coverage of resistance with the local guideline.21 These findings clearly show that further research on guideline outcomes is necessary.
Conclusion
Most guidelines recommend an IIAT according to the individually assessed risk. For uncomplicated cases, the combination of aminopenicillins plus a beta-lactamase inhibitor (BLI) is most frequently mentioned as a first-line therapy option, followed by third generation cephalosporins, quinolones, and ertapenem.
For more complicated cases, the use of acylaminopenicillins/BLI (eg, piperacillin/tazobactam), followed by imi- and meropenem and fourth generation cephalosporins is recommended.
In the group of most complicated cases, three guidelines recommend a combination therapy of acylaminopenicillins/BLI (eg, piperacillin/tazobactam), followed by imi- and meropenem and fourth generation cephalosporins plus quinolones, aminoglycosides, or fosfomycin.
If there is a risk of methicillin-resistant Staphylococcus aureus (MRSA), all the guidelines recommend vancomycin or linezolid. Due to recent trial results, linezolid is recognized to have better cure rates, but the 60-day mortality was similar in both groups.21
We conclude that the current treatment guidelines take into account the individual patient risk, and the correct choice of IIAT affects clinical as well as economical outcomes.
Disclosure
The authors disclose the following possible conflicts of interests: RG and MW received research grants and honoraria for lectures from Pfizer Pharma GmbH, Germany. Until 2010, MW received honoraria for lectures from Wyeth Pharma GmbH, Germany. The authors report no other conflicts of interest in this work.
References
Rosenthal VD, Maki DG, Jamulitrat S, et al; INICC Members. International Nosocomial Infection Control Consortium (INICC) report, data summary for 2003–2008, issued June 2009. Am J Infect Control. 2010;38(2):95–104. e2. | |
Kohlenberg A, Schwab F, Behnke M, Geffers C, Gastmeier P. Pneumonia associated with invasive and noninvasive ventilation: an analysis of the German nosocomial infection surveillance system database. Intensive Care Med. 2010;36(6):971–978. | |
Geffers C, Gastmeier P. Nosocomial infections and multidrug-resistant organisms in Germany: epidemiological data from KISS (the Hospital Infection Surveillance System). Dtsch Arztebl Int. 2011;108(6):87–93. | |
American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. | |
American Hospital Association. Fast Facts on US Hospitals. Chicago, IL: Health Forum LLC; 2013. Available from: http://www.aha.org/research/rc/stat-studies/fast-facts.shtml. Accessed October 5, 2013. | |
Masterton RG, Galloway A, French G, et al. Guidelines for the management of hospital-acquired pneumonia in the UK: report of the working party on hospital-acquired pneumonia of the British Society for Antimicrobial Chemotherapy. J Antimicrob Chemother. 2008;62(1):5–34. | |
Muscedere J, Dodek P, Keenan S, Fowler R, Cook D, Heyland D; VAP Guidelines Committee and the Canadian Critical Care Trials Group. Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia: diagnosis and treatment. J Crit Care. 2008;23(1):138–147. | |
Dalhoff K, Abele-Horn M, Andreas S, et al. [Epidemiology, diagnosis and treatment of adult patients with nosocomial pneumonia. S-3 Guideline of the German Society for Anaesthesiology and Intensive Care Medicine, the German Society for Infectious Diseases, the German Society for Hygiene and Microbiology, the German Respiratory Society and the Paul-Ehrlich-Society for Chemotherapy]. Pneumologie. 2012;66(12):707–765. German. | |
Lorenz J, Bodmann KF, Bauer TT, Ewig S, Trautmann M, Vogel F; German Society for Anesthesiology and Intensive Care (DGAI). [Nosocomial pneumonia: prevention, diagnosis, treatment]. Pneumologie. 2003;57(9):532–545. German. | |
Bodmann KF, Grabein B; Expertenkommission der Paul-Erlich-Gesellschaft für Chemotherapie eV. Empfehlungen zur kalkulierten parenteralen initialtherapie bakterieller er-krankungen bei erwachsenen: Update 2010. Chemother J [serial on the Internet]. 2010 [cited 2013 Aug 15];19(6):179–255. http://www.chemotherapie-journal.de/archiv/artikel/2010/06/186.html. Accessed October 5, 2013. | |
Muscedere J, Dodek P, Keenan S, Fowler R, Cook D, Heyland D; VAP Guidelines Committee and the Canadian Critical Care Trials Group. Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia: prevention. J Crit Care. 2008;23(1):126–137. | |
Barbier F, Andremont A, Wolff M, Bouadma L. Hospital-acquired pneumonia and ventilator-associated pneumonia: recent advances in epidemiology and management. Curr Opin Pulm Med. 2013;19(3):216–228. | |
Kollef MH, Hamilton CW, Ernst FR. Economic impact of ventilator-associated pneumonia in a large matched cohort. Infect Control Hosp Epidemiol. 2012;33(3):250–256. | |
Wilke M, Grube RF, Bodmann KF. Guideline-adherent initial intravenous antibiotic therapy for hospital-acquired/ventilator-associated pneumonia is clinically superior, saves lives and is cheaper than non guideline adherent therapy. Eur J Med Res. 2011;16(7):315–323. | |
Atkins D, Eccles M, Flottorp S, et al; GRADE Working Group. Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv Res. 2004;4(1):38. | |
Aarts MC, van der Heijden GJ, Rovers MM, Grolman W. Remarkable differences between three evidence-based guidelines on management of obstructive sleep apnea-hypopnea syndrome. Laryngoscope. 2013;123(1):283–291. | |
Møller AH, Hansen L, Jensen MS, Ehlers LH. A cost-effectiveness analysis of reducing ventilator-associated pneumonia at a Danish ICU with ventilator bundle. J Med Econ. 2012;15(2):285–292. | |
Thompson DA, Makary MA, Dorman, T et al. Clinical and Economic Outcomes of Hospital Acquired Pneumonia in Intra-Abdominal Surgery Patients. Ann Surg. 2006;243(4):547–552. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1448956/. Accessed November 2, 2013. | |
Piskin N, Aydemir H, Oztoprak N, et al. Inadequate treatment of ventilator-associated and hospital-acquired pneumonia: risk factors and impact on outcomes. BMC Infect Dis. 2012;12:268. | |
Kett DH, Cano E, Quartin AA, et al; Improving Medicine through Pathway Assessment of Critical Therapy of Hospital-Acquired Pneumonia (IMPACT-HAP) Investigators. Implementation of guidelines for management of possible multidrug-resistant pneumonia in intensive care: an observational, multicentre cohort study. Lancet Infect Dis. 2011;11(3):181–189. | |
Becher RD, Hoth JJ, Rebo JJ, Kendall JL, Miller PR. Locally derived versus guideline-based approach to treatment of hospital-acquired pneumonia in the trauma intensive care unit. Surg Infect (Larchmt). 2012;13(6):352–359. |
 © 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.