")
Back to Journals » Clinical Ophthalmology » Volume 8
Unusually delayed presentation of persistent Descemet’s membrane tear and detachment after cataract surgery
Authors Morkin M, Hussain R, Young R, Ravin T, Dubovy S, Alfonso E
Received 4 April 2014
Accepted for publication 15 May 2014
Published 28 August 2014 Volume 2014:8 Pages 1629—1632
DOI https://doi.org/10.2147/OPTH.S65520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Melina I Morkin,1,2 Rehan M Hussain,2 Ryan C Young,2 Tracy Ravin,2 Sander R Dubovy,2 Eduardo C Alfonso2
1Department of Ophthalmology, Shiley Eye Center, University of California – San Diego, San Diego, CA, 2Department of Ophthalmology, Bascom Palmer Eye Institute, Miller School of Medicine, University of Miami, Miami, FL, USA
Abstract: A 51-year-old male who had undergone phacoemulsification in his left eye 11 months prior presented with complaint of sudden onset of blurred vision in the same eye. Review of his clinical course, slit-lamp exam, pachymetry, and specular endothelial microscopy led to the diagnosis of acute hydrops caused by Descemet’s membrane dehiscence at the site of the incision. He was initially managed with medical treatment and observation. In the subsequent months of follow-up, the corneal edema and the patient’s visual acuity did not improve. Intracameral gas injection was performed 7 months after presentation, but because of persistent corneal edema and nonattached Descemet’s membrane, penetrating keratoplasty was performed. Histopathologic examination confirmed the diagnosis. The patient has had a clear corneal graft since then. Although Descemet’s membrane detachment is a rather common complication after intraocular surgery, its unusually delayed presentation can also occur, and should not be confused with pseudophakic bullous keratopathy. Many mechanisms have been studied for the development of early tears and detachments after cataract surgery, but little is known about late presentations. The authors explore possible causes, and highlight the importance of instructing patients to avoid eye rubbing and any other type of trauma to the cornea after intraocular surgery.
Keywords: Descemet’s membrane tear, detachment, cataract surgery, phacoemulsification
Introduction
Descemet’s membrane tearing is often attributable to surgical procedures, and is usually confined to the incision site. Early in the postoperative period, patients can be asymptomatic, and clinical signs might be difficult to detect. When apparent, Descemet’s membrane tears and detachments may cause decreased vision and corneal edema in the first days or weeks after surgery.
Few cases of Descemet’s detachments occurring late in the postoperative period have been reported, and very rarely months after surgery. Wong et al reported a case of a patient who developed a Descemet’s detachment 8 months after THC:YAG (thulium, holmium, chromium-doped yttrium aluminum garnet crystal) laser sclerostomy.1 Stewart et al reported a case of a Descemet’s detachment that occurred 5 months after uncomplicated cataract surgery.2 To our knowledge, this is the first report of delayed Descemet’s tear and detachment occurring 11 months after cataract surgery.
Case report
A 51-year-old Hispanic male was referred to the Bascom Palmer Eye Institute cornea service with a complaint of sudden onset of blurred vision in the left eye 3 weeks prior. He had undergone uncomplicated phacoemulsification (Alcon) with posterior chamber intraocular lens insertion 11 months prior in the left eye and 5 years prior in the right eye. He had been using topical prednisolone acetate 1% and sodium chloride 5% for 3 weeks with no improvement in his symptoms.
The exam revealed best-corrected visual acuity of 20/20 in the right eye and 20/40 in the left eye, with a -2.50 sphere at 61°. Intraocular pressures were 10 mmHg in both eyes by Tono-Pen. Slit-lamp exam (Zeiss) of the left eye revealed a healed temporal corneal incision wound and abnormal Descemet’s membrane wrinkling with irregular edges. Stromal edema was noted just nasally to this site, which extended centrally through the visual axis (Figure 1). The cornea of the right eye was clear. The anterior chambers were deep and quiet. The posterior chamber intraocular lenses were well positioned. Mild-to-moderate posterior capsular opacification was present bilaterally. The vitreous was clear bilaterally. The view of the fundus was hazy in the left eye, but both retinas appeared flat and without lesions, and the optic nerves were unremarkable (Topcon indirect ophthalmoscope; Alcon MA60 posterior chamber lens).
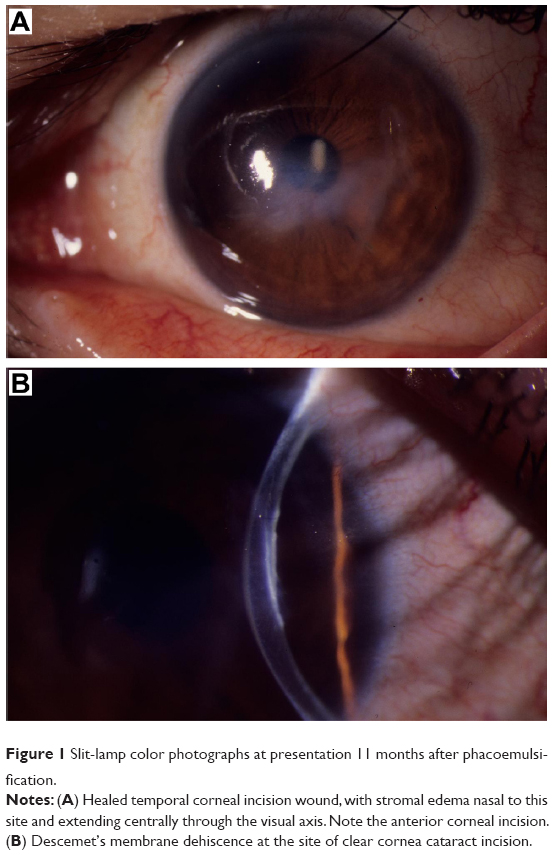 | Figure 1 Slit-lamp color photographs at presentation 11 months after phacoemulsification. |
Orbscan pachymetry revealed central corneal thickness of 614 μm in the right eye and 878 μm in the left eye (1,093 μm temporally, 702 μm nasally). Topcon keratometry readings of the left eye revealed 2.5 D of astigmatism at 61°. Specular endothelial microscopy and cell count showed no significant difference between the two eyes (2,427 cells/mm2 oculus dexter, 2,320 cells/mm2 oculus sinister; Topcon).
The patient was diagnosed with a spontaneous Descemet’s dehiscence at the site of the clear cornea cataract incision. As the corneal edema was mild, medical treatment was continued with hyperosmotic saline ointment at bedtime, hyperosmotic drops in the morning, timolol 0.5% daily, and tapering off the prednisolone. He was also instructed to use a hair dryer to the eye in the morning, avoid eye rubbing, and use a protective shield at bedtime. In the subsequent months of follow-up, the corneal edema and visual acuity remained the same.
At 7 months after our initial evaluation, the patient reported decreased vision in the left eye associated with pain. He was not using any medication. The exam revealed a best-corrected visual acuity of 20/200 in the left eye, intraocular pressure of 18 mmHg, and microcystic corneal edema extending from the site of the Descemet’s tear (Figure 2). A low-lying Descemet’s detachment could not be ruled out, so surgical intervention with 0.25 mL of 100% sulfur hexafluoride gas injection was elected.
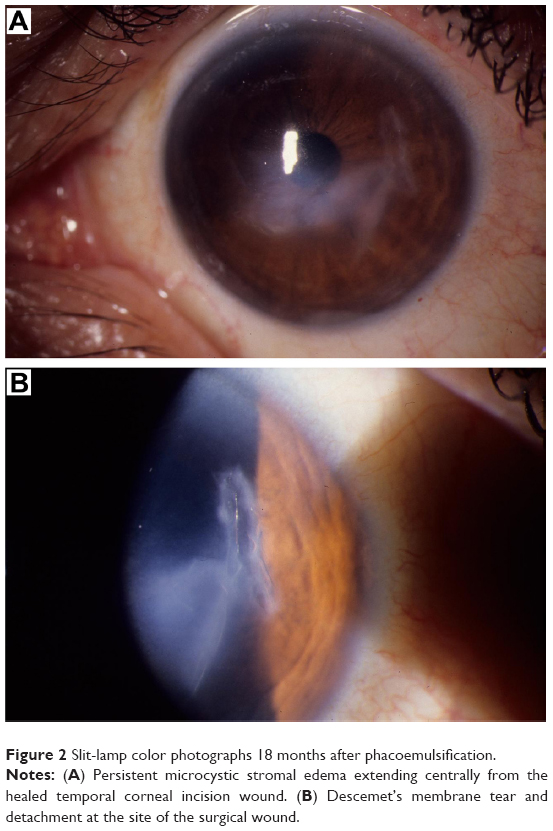 | Figure 2 Slit-lamp color photographs 18 months after phacoemulsification. |
One month after the intracameral gas injection, the vision remained at 20/200 and there was no improvement in the corneal edema. Penetrating keratoplasty – the best surgical option at that time since Descemet’s stripping endothelial keratoplasty was not available – was discussed with the patient, but he decided to continue medical therapy and observation. Four months later, he presented with vision of 20/400 in the left eye, persistent corneal edema, and Descemet’s disruption. The patient finally decided to undergo penetrating keratoplasty.
The histopathologic examination of the corneal button revealed an edematous corneal stroma. Descemet’s membrane was intact over half of the button and became discontinuous centrally. The remainder of Descemet’s membrane was partially detached from the corneal stroma (Figure 3).
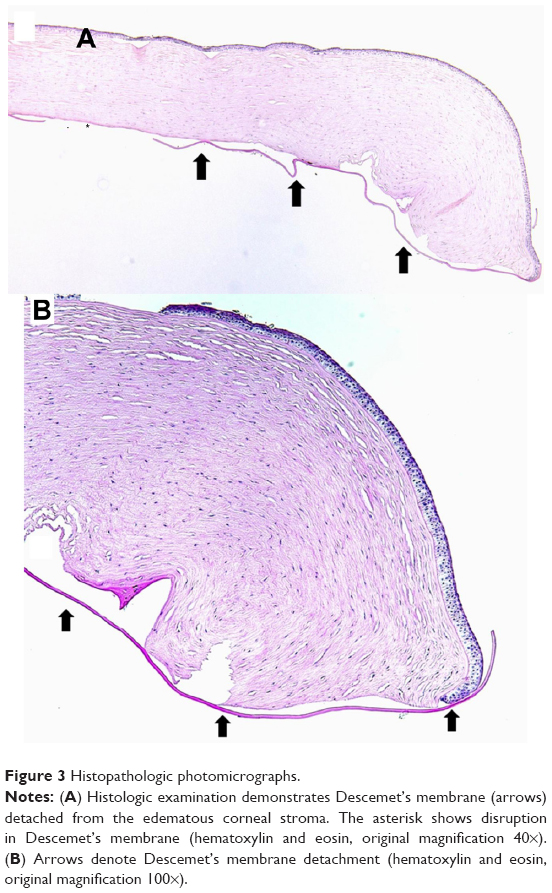 | Figure 3 Histopathologic photomicrographs. |
The postoperative course was uncomplicated. Ten years after surgery, the best-corrected visual acuity in the left eye was 20/25, and the graft remained clear.
Discussion
We report a case of delayed Descemet’s membrane detachment and tear leading to hydrops 11 months after uncomplicated phacoemulsification using a temporal clear cornea approach. The proximity of the edema to the corneal wound suggests this as the source, despite the fact that the wound had been made 11 months prior, appeared well healed, and had been asymptomatic until 3 weeks prior.
Known risk factors that may increase the likelihood of traumatic entry into the anterior chamber include oblique angle of entry, anterior and shelved incisions, use of a blunt knife, injection of viscoelastic or antibiotics anteriorly to Descemet’s membrane, a shallow anterior chamber, soft eye, previous surgery, and recent episode of corneal edema.3–5 The location of the incision may have contributed to the development of the Descemet’s membrane tear in this patient. We noted an anterior temporal corneal entry incision wound to the anterior chamber, leading to a Descemet’s membrane prone to detachment and tear after phacoemulsification.
Kansal and Sugar explored the possibility of an underlying anatomic predisposition for the development of Descemet’s membrane detachment after phacoemulsification, possibly explained by an abnormality in the fibrillary stromal adhesion to Descemet’s membrane.6 Some patients may have an abnormal attachment between the stroma and Descemet’s membrane caused by dysfunction of the anchoring protein βig-h3.7,8 The predisposition is more evident in cases of bilateral Descemet’s membrane detachment after cataract surgery9 and among siblings.10
Many mechanisms have been easily attributable to the occurrence of early detachments after cataract surgery. However, the scarce literature on the very few late presentations does not methodically discuss mechanisms responsible for delayed cases, especially when they present with tears. Why had this patient developed Descemet’s membrane tear several months after cataract surgery? A logical explanation for this unusually late presentation is that he might have traumatized his cornea, eg, by eye rubbing or unnoticed trauma, to a point that he caused further disruption of an already-susceptible Descemet’s membrane and acute onset of edema in this area. In patients with keratoconus, corneal hydrops can be triggered by eye rubbing. We ruled out any evidence of keratoconus or corneal ectasia. The central corneal thickness in the right eye appeared relatively high at the time of presentation. However, based on previous readings from the patient, we considered the pachymetry results to be symmetrically conserved, except for the area of edema in the left eye, which was thicker. Interestingly, preexistent endothelial dysfunction has been reported as the only significant preoperative risk factor by Ti et al.11 The endothelium in both eyes appeared to be normal by specular microscopy, excluding endothelial dysfunction and pseudophakic bullous keratopathy as the cause of hydrops. The uneventful 10 year follow-up has supported the original evaluation.
It is important to be aware of the potential causes of corneal edema months after cataract surgery, in order that they may be diagnosed and treated appropriately. Instructing patients to avoid eye rubbing or any other type of trauma to the cornea should always be emphasized after intraocular surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
Wong VK, Koenig SB, Fogel ES, Freedman MI. Late detachment of Descemet’s membrane after subconjunctival THC:YAG (holmium) laser sclerostomy ab externo. Am J Ophthalmol. 1993;116(4):514–515. | ||
Stewart CM, Li F, McAlister JC. Late-onset persistent Descemet’s membrane detachment following uncomplicated clear corneal incision cataract surgery. Clin Experiment Ophthalmol. 2011;39(2):171–174. | ||
Chow VW, Agarwal T, Vajpayee RB, Jhanji V. Update on diagnosis and management of Descemet’s membrane detachment. Curr Opin Ophthalmol. 2013;24(4):356–361. | ||
Bhattacharjee H, Bhattacharjee K, Medhi J, Altaf A. Descemet’s membrane detachment caused by inadvertent vancomycin injection. Indian J Ophthalmol. 2008;56(3):241–243. | ||
Al-Mezaine HS. Descemet’s membrane detachment after cataract extraction surgery. Int Ophthalmol. 2010;30(4):391–396. | ||
Kansal S, Sugar J. Consecutive Descemet membrane detachment after successive phacoemulsification. Cornea. 2001;20(6):670–671. | ||
Hirano K, Kojima T, Nakamura M, Hotta Y. Triple anterior chamber after full-thickness lamellar keratoplasty for lattice corneal dystrophy. Cornea. 2001;20(5):530–533. | ||
Streeten BW, Qi Y, Klintworth GK, Eagle RC Jr, Strauss JA, Bennett K. Immunolocalization of βig-h3 protein in 5q31-linked corneal dystrophies and normal corneas. Arch Ophthalmol. 1999;117(1):67–75. | ||
Shalchi Z, O’Brart DP, Ilari L. Bilateral Descemet membrane detachment following cataract surgery. JAMA Ophthalmol. 2013;131(4): 533–535. | ||
Felipe AF, Rapuano CJ, Nottage JM, Abazari A. Descemet membrane detachment among siblings: role of anatomic and familial predisposition. Cornea. 2012;31(7):836–840. | ||
Ti SE, Chee SP, Tan DT, Yang YN, Shuang SL. Descemet membrane detachment after phacoemulsification surgery: risk factors and success of air bubble tamponade. Cornea. 2013;32(4):454–459. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.