")
Back to Journals » International Medical Case Reports Journal » Volume 7
Unusual presentation of spinal lipomatosis
Authors Stephenson W, Kauflin M
Received 13 September 2013
Accepted for publication 10 June 2014
Published 23 September 2014 Volume 2014:7 Pages 139—141
DOI https://doi.org/10.2147/IMCRJ.S54456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
William Stephenson,1 Matthew J Kauflin2,3
1Primary Care, Huntington Veteran's Affairs Medical Center, Huntington, WV, USA; 2Department of Pharmacy, Grandview Medical Center, Dayton, Ohio, OH, USA; 3Ohio Northern University, Ada, Ohio, OH, USA
Abstract: Spinal epidural lipomatosis (SEL) is a rare condition characterized by overgrowth of normal adipose tissue in the extradural space within the spinal canal that can lead to significant spinal cord compression. It is most commonly reported in patients receiving chronic glucocorticoid therapy. Other causes can include obesity and hypercortisolism. Occasionally, idiopathic SEL will occur in patients with no known risk factors, but cases are more generally reported in obesity and males. We present the case of a 35 year-old non-obese woman found to have rapidly progressive SEL that was not associated with any of the common causes of the disorder.
Keywords: lipomatosis, laminectomy, hypercortisolism
Introduction
Spinal epidural lipomatosis (SEL) leads to accumulation of adipose tissue within the spinal canal. The excessive fat depositions associated with SEL may cause direct mechanical compression of the spinal cord or nerve roots involving the lumbar and thoracic spine.1,2 It is most frequently seen in patients exposed to chronic glucocorticoid therapy and typically presents as back pain, radiculopathy, claudication, and paraparesis.3 Diagnosis of SEL remains challenging and typically involves computed tomography or magnetic resonance imaging (MRI) to rule out other conditions such as spinal tumors, spinal abscess, hematoma, disc prolapse, and demyelinating diseases. MRI is the most sensitive and specific test for assessing adipose tissue and it may also suggest the histological nature of the compressive lesion.4–6 The treatment approach depends on the severity of the symptoms and the related neurological impairment. Conservative management is indicated for mild symptoms, and consists of weight reduction, tapering of exogenous steroids, and physical therapy. In patients with debilitating symptoms, decompression is achieved through laminectomy and debulking of the hypertrophied epidural fat.4,7 We present the case of a 35 year-old woman who, after hospital admission, developed progressive neurological impairment related to idiopathic SEL.
Report of case
A 35 year-old African American woman with a past medical history of type 1 diabetes mellitus and end stage renal disease presented to our emergency room via ambulance after being found unresponsive by her boyfriend at home. The patient had recent complaints of lower extremity weakness and denied use of glucocorticosteroids in the past. Her admission weight was 61 kg, and her height was 152 cm (body mass index [BMI]: 26.4 kg/m2). Unfortunately, serum cortisol levels were not measured during this admission. The patient was initially admitted to our medical intensive care unit with a diagnosis of bacteremia and was found to have a methicillin-sensitive Staphylococcus aureus tricuspid valve endocarditis. After initial stabilization, and treatment of her infection, the patient complained of the inability to stand or ambulate, especially on her right side. MRI without contrast of the thoracic spine showed extensive epidural fat, consistent with lipomatosis, extending from T1 through T9 (Figure 1). MRI with contrast of the thoracic spine confirmed this and failed to show any evidence of epidural abscess. MRI of the cervical and lumbar spine was unremarkable. At this point, a posterior decompression laminectomy was performed from T3 through T7. During surgery, a very large compressive epidural lipomatosis was visualized. The most significant spinal cord compression was seen at levels T4 through T6. Pathology of the specimen failed to show malignancy and was reported as adipose tissue. Following surgery the patient was eventually transferred to a rehabilitation hospital, where she continued to improve her functional status. The patient continued to improve and was ambulating at follow-up 11 months later.
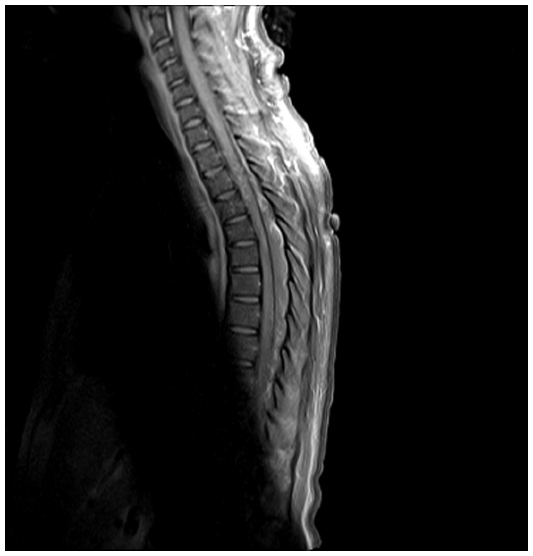 | Figure 1 Patient’s MRI showing lipomatosis extending from T1 through T9. |
Comment
SEL is a rare condition first diagnosed in 1975. Currently, the underlying pathogenesis of SEL is unknown. One proposed mechanism implies that elevated levels of cortisol lead to hypertrophy of adipose tissue that is already present in the extradural space of the thoracic and lumbosacral spine.2,8 Despite this, approximately 17% of cases are idiopathic.9 Typically, males are more commonly affected than females. The clinical manifestations of this disease depend greatly on the level of canal compromise. It has been reported that SEL of the thoracic levels causes myelopathy while SEL at the lumbar levels results in radiculopathy. The manifestations of this disorder can also mimic other conditions such as: spinal tumors, spinal abscess, hematoma, and demyelinating conditions. Treatment of this disorder usually begins with conservative measures such as weight loss along with steroid tapering and analgesics. However, in patients who present with signs or symptoms of spinal compression, the recommended first line treatment is surgical decompression. This procedure has been shown to be effective in a large percentage of case reports for symptomatic relief.3 Our case is unusual in that it arose in a non-obese female patient, with no known glucocorticoid exposure and rapid symptom progression. This led to a decompressive laminectomy prior to trial of conservative treatments secondary to the presence of spinal cord compression. This spinal cord compression was established by MRI and later confirmed via operative visualization. A second surgical option available instead of laminectomy would be the re-insertion of the lamina with titanium miniplates. This procedure has shown decreased postoperative deformities. However, the rate of postoperative deformity is low; especially when more than 50% of facet joints are left intact.10
Conclusion
SEL is a rare condition that can lead to severe physical and functional limitation. This condition is usually associated with a male predisposition and steroid use or hypercortisolism. Conservative initial therapy consists of physical rehabilitation along with weight loss. However, if conservative measures fail, surgical decompression is indicated. SEL should be considered in the evaluation of patients with low back pain, persistent radicular pain and progressive myelopathy, particularly in obese patients or those with chronic steroid exposure.
Disclosure
The authors report no conflicts of interest for this manuscript.
References
López-González A, Resurrección Giner M. Idiopathic spinal epidural lipomatosis: urgent decompression in an atypical case. Eur Spine J. 2008;17(Suppl 2):S225–S227. | |
Alvarez A, Induru R, Lagman R. Considering symptomatic spinal epidural lipomatosis in the differential diagnosis. Am J Hosp Palliat Care. 2013;30(6):617–619. | |
Chen CC, Lee WY, Cho DY. Spinal epidural lipomatosis. Zhonghua Yi Xue Za Zhi (Taipei). 2002;65(2):86–89. | |
Fogel GR, Cunningham PY 3rd, Esses SI. Spinal epidural lipomatosis: case reports, literature review and meta-analysis. Spine J. 2005;5(2):202–211. | |
Pinkhardt EH, Sperfeld AD, Bretschneider V, Unrath A, Ludolph AC, Kassubek J. Is spinal epidural lipomatosis an MRI-based diagnosis with clinical implications? A retrospective analysis. Acta Neurol Scand. 2008;117(6):409–414. | |
Ishikawa Y, Shimada Y, Miyakoshi N, et al. Decompression of idiopathic lumbar epidural lipomatosis: diagnostic magnetic resonance imaging evaluation and review of the literature. J Neurosurg Spine. 2006;4(1):24–30. | |
Wälchli B, Benini A. Spinal epidural lipomatosis. Swiss Med Wkly. 2001;131(23–24):359. | |
Choi KC, Kang BU, Lee CD, Lee SH. Rapid progression of spinal epidural lipomatosis. Eur Spine J. 2012;21 Suppl 4:S408–S412. | |
Al-Khawaja D, Seex K, Eslick GD. Spinal epidural lipomatosis – a brief review. J Clin Neurosci. 2008;15(12):1323–1326. | |
Medscape [homepage on the Internet]. Schatio B, Pluta RM, Schaller K. Laminoplasty; [updated June 21, 2012]. Available from: http://emedicine.medscape.com/article/1890493-overview. Accessed December 8, 2013. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.