")
Back to Journals » Nature and Science of Sleep » Volume 7
Unmet needs of patients with narcolepsy: perspectives on emerging treatment options
Authors Wozniak D, Quinnell T
Received 2 February 2015
Accepted for publication 25 March 2015
Published 22 May 2015 Volume 2015:7 Pages 51—61
DOI https://doi.org/10.2147/NSS.S56077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Steven A Shea
Dariusz R Wozniak, Timothy G Quinnell
Respiratory Support and Sleep Centre, Papworth Hospital, Cambridge, UK
Abstract: The treatment options currently available for narcolepsy are often unsatisfactory due to suboptimal efficacy, troublesome side effects, development of drug tolerance, and inconvenience. Our understanding of the neurobiology of narcolepsy has greatly improved over the last decade. This knowledge has not yet translated into additional therapeutic options for patients, but progress is being made. Some compounds, such as histaminergic H3 receptor antagonists, may prove useful in symptom control of narcolepsy. The prospect of finding a cure still seems distant, but hypocretin replacement therapy offers some promise. In this narrative review, we describe these developments and others which may yield more effective narcolepsy treatments in the future.
Keywords: cataplexy, hypocretin, H3 antagonist, GABA-B agonists, immunotherapy
Introduction
Narcolepsy is a chronic neurological disorder characterized by a pentad of excessive daytime sleepiness (EDS), cataplexy, sleep paralysis, hypnagogic hallucinations, and disturbed nocturnal sleep. EDS is always present and usually appears first. Cataplexy occurs in approximately 70% of patients with narcolepsy, while the other symptoms feature less frequently and in various combinations.1 A substantial number of patients suffer from associated sleep disorders including rapid eye movement (REM) sleep behavior disorder, periodic limb movements, vivid dreams, and nightmares.2
The third edition of the International Classification of Sleep Disorders divides narcolepsy into type 1, previously known as narcolepsy with cataplexy, and type 2, previously described as narcolepsy without cataplexy.3 In the majority of subjects, type 1 narcolepsy is caused by autoimmune-mediated loss of hypocretin-secreting neurons in genetically predisposed individuals. The pathophysiology of type 2 narcolepsy is less well understood.4 The prevalence of narcolepsy in the United States and Europe ranges from 20 to 67 per 100,000, although as many as 80% of people may still go undiagnosed.5–7
Narcolepsy is a debilitating condition which can affect all aspects of life. Psychosocial functioning and quality of life are reduced.8,9 Unemployment rates are higher and income levels among those who work are lower compared with non-narcoleptic controls.10 Narcolepsy is associated with increased health costs, with higher rates of health-related contact and medication use.11 Negative impact of the disease on academic performance, relationships, and recreational and sexual life is well documented, and depression is common.12,13 Given the cardinal features, it is not surprising that the risk of accidents at home, at work, or while driving is increased for those suffering from narcolepsy.14
When considering unmet needs of patients with narcolepsy, the importance of establishing an early diagnosis cannot be overemphasized. Hearing the diagnosis is likely to be a key, if ambivalent, moment in a patient’s life. On one hand, it implies a lifelong, incurable condition which can substantially limit functional status and undermine future prospects. On the other hand, symptom validation and the prospect of treatment can provide considerable relief after protracted, unexplained debility. The diagnostic process is now facilitated by clearly defined diagnostic criteria and modern diagnostic tools.3 Nonetheless, a substantial number of patients still experience a delay of between 10 and 15 years for narcolepsy to be confirmed, while others remain undiagnosed.7 Lack of disease awareness and misdiagnosis by health care professionals, and poor patient and public awareness, are probably the key factors responsible for this.7
Nearly all patients diagnosed with narcolepsy require lifelong treatment. Behavioral methods, such as scheduled daytime naps, are helpful but rarely suffice as monotherapy. Over 90% of patients require regular pharmacotherapy to combat daily, debilitating symptoms.15
In this review, we briefly outline the currently available pharmacological treatments and their limitations. Our main focus, however, is on emerging treatment options and novel therapeutic concepts which are in various stages of development. We summarize current knowledge in this area.
Pharmacotherapy for narcolepsy
The current pharmacotherapeutic approach to narcolepsy is based on symptom control. It includes newer drugs supported by evidence from randomized clinical trials as well as compounds which have not been assessed in robust studies but are known for their efficacy (Table 1).
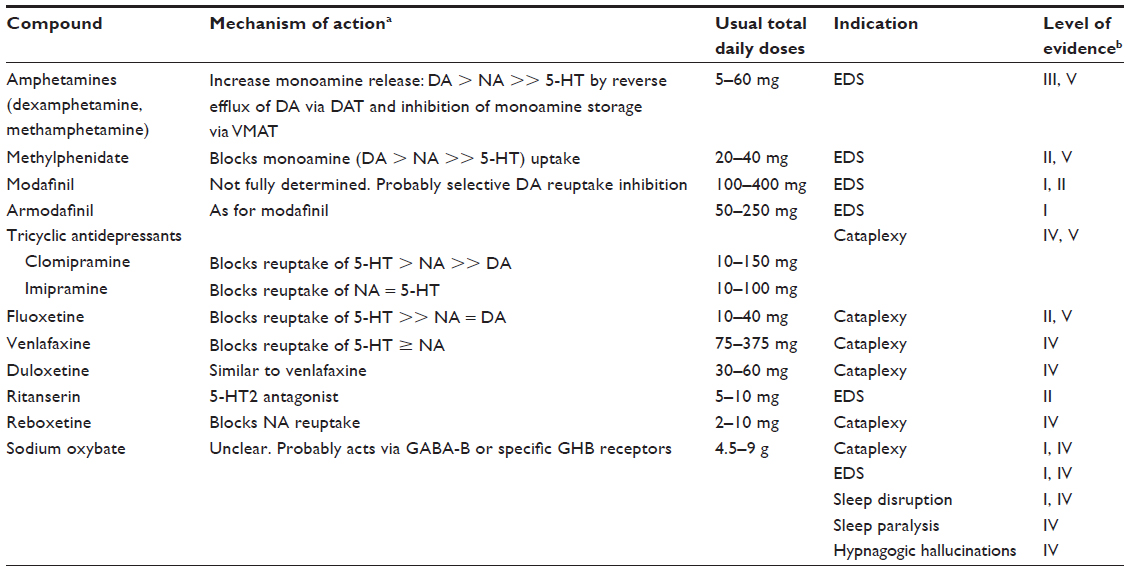 | Table 1 Selected compounds used in narcolepsy |
Amphetamine was first introduced as a treatment for narcolepsy in 1935.17 Its derivatives (d-amphetamine, methamphetamine) and amphetamine-like compounds (methylphenidate) subsequently became the mainstay of EDS management and are still widely used. They are generally well tolerated, but minor sympathomimetic side effects are common.15 Cardiovascular side effects may prevent their use in some patients, particularly the elderly and others with relevant comorbidities. Long-term use has been linked to adverse psychological events.18 Abuse of amphetamine derivatives in well-defined narcolepsy subjects is rare, but tolerance can develop in up to a third of patients.19
Newer stimulants, such as modafinil or its r-enantiomer, armodafinil, are generally less potent.20–22 However, favorable safety profiles and higher-level evidence of effectiveness mean that they are now first-line treatment for the EDS of narcolepsy.1,16,20 Pemoline and mazindol are other mild sympathomimetic stimulants, but their use is restricted in most countries due to safety concerns or inadequate evidence.22
Cataplexy is not always severe enough to require specific treatment, or it sometimes improves sufficiently when adequate control of EDS is achieved with amphetamine-like medications.23,24 When necessary, it has traditionally been treated with antidepressants. Tricyclic antidepressants, such as imipramine or clomipramine, have been used as anticataplectic agents since the 1960s, but they are not always easy to tolerate.15 Anticholinergic and antihistaminergic side effects, weight gain, sexual dysfunction, and tremor often hamper treatment. Newer antidepressants, including selective serotonin reuptake blockers, serotonin/norepinephrine reuptake inhibitors, and norepinephrine reuptake inhibitors, have better side effect profiles, and are usually chosen over tricyclics.15 Efficacy is variable across the groups, but those drugs with the strongest norepinephrine reuptake inhibition, such as venlafaxine or duloxetine, are probably most useful.20,25
The introduction of sodium oxybate (a salt of gamma hydroxybutyrate [GHB]) has probably been the most significant advance in the treatment of narcolepsy in recent years. For the first time, monotherapy has become possible in some patients. Sodium oxybate is approved in the United States for the treatment of EDS and cataplexy, and in the European Union and Canada for the treatment of cataplexy. It can also restore sleep continuity and has positive effects on sleep paralysis and hypnagogic hallucinations.16 Sodium oxybate is well tolerated by most patients, but side effects include nausea, dizziness, nocturnal confusion, sleepwalking, and enuresis.15,20 Its administration comes with certain challenges. A short half-life means that twice-nightly dosing is required. Dose titration at treatment initiation is not always straightforward and requires close monitoring. Overdose of GHB can lead to fatal respiratory depression.26 Patients may need to alter their lifestyle. They should avoid alcohol and sedating medications, and the profound sedation of oxybate means that patients sometimes have to change living arrangements if they live alone or are sole carers.1
A recent survey was conducted in the Unites States with the aim of sharing patients’ perspectives on the treatment of narcolepsy with the US Food and Drug Administration (FDA). It included over 1,000 people with narcolepsy.27 It is unclear how many patients met the currently recognized diagnostic criteria, but 95% of responders reported having been prescribed at least one of the FDA-approved medications. Nonetheless, 74% complained of daily narcolepsy symptoms. Eighty-four percent described impaired work or school performance and judged their condition as moderate or severe. These results are consistent with an earlier European survey, which was conducted on 67 subjects with well-defined narcolepsy. Despite standard treatment, 84% felt the negative impact of symptoms on a daily basis, including 70% reporting EDS every day, and 31% suffering daily cataplexy.28
The pharmacological management of narcolepsy is particularly challenging in pregnancy and breastfeeding. Although there is no evidence that currently available drugs are teratogenic in humans when used in therapeutic doses, animal studies raised concern about potential embroyotoxicity.29 Consequently, most clinicians would recommend withdrawal of pharmacotherapy during conception, pregnancy, and breastfeeding.29 However, this may not be possible when the pregnancy is unplanned or narcolepsy symptoms are severe enough to pose risk of injury to the mother or fetus.1 Some women are unable to manage daily activities or childcare without treatment. For ethical reasons it is unlikely that clinical trials on currently available compounds will include pregnant women. However, prospective registries of pregnancy outcomes in patients who decide to continue the treatment are needed to support advice on the best management of narcolepsy in pregnancy. Future, more physiological treatments, such as hypocretin replacement, may well be more acceptable for pregnant women.
These data highlight the unmet needs of patients suffering from narcolepsy and demonstrate the importance of ongoing efforts to develop effective new treatments.
Emerging treatment options
Therapies aimed at restoring hypocretin system signaling
The discovery that hypocretin deficiency is responsible for narcolepsy raised hopes that restoration of hypocretin signaling could lead to causative therapy. Several concepts have been proposed, including substitution of the natural neuropeptide or its analogs, engineering hypocretin receptor agonists, hypocretin cell transplantation, and gene therapy. Despite over 10 years of exploring these promising hypocretin-based approaches, no clinically effective treatments have yet been produced. Nevertheless, progress has been made. Our knowledge of the hypocretin system has grown and potential solutions to overcome some barriers to replacement therapy have been found.
Hypocretin neurons are located in the lateral hypothalamus and project throughout the brain and spinal cord, with particularly dense innervation of specific nuclei involved in sleep–wake regulation, including the locus coeruleus, dorsal raphe, tuberomammillary, laterodorsal tegmental, and pedunculopontine tegmental nuclei.30 Application of hypocretin directly to these structures or to the intracerebroventricular space increases wakefulness and suppresses cataplectic behavioral arrests in mice.31–34 The active neuropeptides are hypocretin-1 and hypocretin-2, which are cleaved from inactive prepro-hypocretin. They are fairly large molecules, consisting of 33 and 28 amino acids, respectively.35 Hypocretins act via two G protein-coupled ligand receptors, hypocretin R1 (hcrtR1) and hypocretin R2 (hcrtR2). Expression of both receptors, particularly hcrtR2, is preserved in sporadic human narcolepsy, so hypocretin-based therapies are a realistic aim.36 Unfortunately, one of the main obstacles to substituting these neuropeptides is their poor central nervous system (CNS) penetration when administered peripherally. The central route of administration is not practical in humans. Early experiments in canine models showed that intravenous hypocretin penetrated the blood–brain barrier poorly, and only when given at very high concentration. The functional effects of intravenous hypocretin were unconvincing and results overall were not promising enough to justify clinical studies.37,38 Far more appealing and convenient is noninvasive intranasal delivery. Macromolecules are transported via olfactory and trigeminal nerves, bypassing the blood–brain barrier and reaching the brain within minutes. Systemic absorption and potential associated side effects are reduced. Another advantage is that the neuropeptides do not necessarily require modification and so retain their original properties.39 Intranasal drug delivery can be optimized further by adding a vasoconstrictor to the formulation, which minimizes systemic absorption, increasing the amount of drug available to the CNS. One study combined 1% phenylephrine with an intranasal hypocretin preparation, reducing systemic absorption by 65%. Olfactory epithelial deposition was increased threefold and CNS hypocretin concentration was significantly higher.40
Intranasal administration of hypocretin-1 improved cognitive performance in sleep-deprived rhesus monkeys, and was more effective than intravenous doses ten times larger. Furthermore, these behavioral effects were associated with changes in metabolic activity in the specific brain regions that were engaged in the cognitive tasks and affected by sleep restriction.41
Intranasal hypocretin was first used in humans with narcolepsy in 2008. Baier at al found that it restored olfactory dysfunction, but effects on other narcolepsy symptoms were not assessed.42 This was followed by a double-blind, randomized, placebo-controlled crossover trial in which eight patients with narcolepsy were given recombinant human hypocretin-1 intranasally before nocturnal sleep.43 Hypocretin-1 was reported to reduce and stabilize REM sleep. Nocturnal wakefulness was not altered, but this could have been a consequence of nonphysiological timing of hypocretin administration.44 Weinhold et al recently repeated their trial, but this time administered hypocretin to 14 narcoleptic patients in the morning.45 Participants subsequently underwent Modified Maintenance of Wakefulness Tests (MMWTs), attention testing, and nocturnal polysomnography. Intranasal hypocretin-1 induced fewer false reactions in divided attention tests. In MMWTs, there were fewer wake–REM sleep transitions and REM sleep duration was reduced, but the difference in REM sleep latency did not reach statistical significance. On the subsequent night, duration of stage 2 non-REM (NREM) (N2) sleep increased but no other changes in sleep architecture, REM latency, total sleep time, or sleep efficiency were observed. Subjective ratings of sleepiness were not altered by hypocretin.
Although showing some promise, more work is needed to establish whether intranasal hypocretin represents a truly effective treatment option. The studies to date have examined only single-dose effects and provided little data on clinically meaningful outcomes. Long-term effects, optimal dosage, timing of administration, and pharmacokinetics remain unknown. The role of hypocretin replacement on cataplexy has yet to be explored.
An alternative way to restore hypocretin signaling, potentially free of the neuropeptide delivery problems, is to use a non-peptide hcrtR agonist. In the past few years there has been considerable research focused on hcrtR antagonism. This work resulted in FDA approval of the first orally active hcrtR antagonist, suvorexant, for the treatment of insomnia in August 2014.46,47 However, engineering an hcrtR agonist is proving more challenging and, to our knowledge, no successful compounds have yet been developed. Hopefully, biotechnological advances will enable some progress in this area.48
Another proposed treatment strategy is hypocretin cell transplantation, to replace the lost neurons. This was attempted in a single study using a rat model of narcolepsy.49 The authors found some evidence of improvement in somnolence in transplanted animals, but graft cell survival was poor. In humans, an additional challenge would be sourcing the hypocretin cells, which are acquired from postnatal tissue in animal studies. A possible solution could be to use hypocretin neuroblasts derived from stem cells but exploratory work is yet to be undertaken.
In a more advanced stage of development is viral vector-delivered gene therapy. This can establish long-term CNS protein expression after a single administration. Gene therapies evolved particularly as a novel treatment for neurodegenerative disorders such as Parkinson’s disease. Viral mediated delivery of enzymes (aromatic l-amino acid decarboxylase and glutamic acid decarboxylase) or neurotrophic factors (neurturin, glial-derived neurotrophic factor) was initially developed in animal models but then progressed to Phase I and Phase II clinical trials with some promising clinical outcomes.50 This technology was adopted in narcolepsy. One group investigated hypocretin gene transfer in a series of mouse experiments using different viral vectors and targeting specific brain areas. In the first study, a replication-defective herpes simplex virus-1 was used to transfer the prepro-hypocretin gene into the lateral hypothalamus of hypocretin knockout mice.51 Hypocretin was expressed in numerous neurons and detected in the cerebrospinal fluid. Both cataplexy and narcoleptic sleep–wake behavior were improved during the 4-day lifespan of the vector. This was followed by an experiment in which a different vector, recombinant adeno-associated virus (rAAV) was used.52 This vector has the advantage of facilitating long-term gene expression and has been successfully used in humans without concerning adverse events. Hypocretin gene transfer into neurons of the zona incerta and lateral hypothalamus blocked cataplexy, but the same intervention into the striatum and directly into melanin-concentrating hormone neurons was ineffective, indicating site specificity. In the third study, neurons of the dorsolateral pons involved in muscle tone regulation were targeted. Again, rAAV-hypocretin gene transfer significantly reduced cataplexy.53
These studies have identified potential target brain regions where surrogate neurons can be used to facilitate expression and function of hypocretin. Hopefully, as with Parkinson’s disease, this novel therapy will be evaluated in humans.
H3 antagonists
The human histaminergic system plays a vital role in maintenance of wakefulness and sleep–wake regulation. It consists of approximately 64,000 neurons located exclusively in and around the tuberomammillary nucleus.54 From there, histaminergic neurons send input either directly or indirectly to various brain regions involved in sleep–wake regulation. They are active specifically during wakefulness in a manner dependent on circadian rhythm and behavioral state.55 Importantly, hypocretin neurons densely innervate the tuberomammillary nucleus and directly stimulate histaminergic neurons. A low concentration of histamine was found in the cerebrospinal fluid of narcoleptic patients, in keeping with its reduced secretion.56 However, in contrast to the hypocretin system, histaminergic neurons are well preserved in narcolepsy and are capable of promoting wakefulness via hypocretin-independent pathways.57 This rationale prompted the development of drugs which increase histamine release in the CNS.
Histamine acts in the CNS via its aminergic G protein-coupled receptors: H1, H2, H3, and H4. All four are believed to play specific roles in the brain, but the functions of H1 and H3 are better understood.54 The wake-promoting effect is directly mediated via H1, whereas H3 functions as a constitutively active auto- and heteroreceptor. As an autoreceptor, H3 inhibits cell firing, as well as synthesis and release of histamine. As a presynaptic heteroreceptor, H3 inhibits the release of other neurotransmitters involved in sleep–wake regulation, including acetylcholine, dopamine, serotonin, and noradrenaline.55 Since its discovery over 30 years ago, H3 has been a target for the development of both agonists and antagonists, able to facilitate sleep and wakefulness, respectively.58 Several H3 antagonists developed by independent pharmaceutical companies have been repeatedly shown in animal models to improve a heterogeneous collection of somnolence and vigilance deficiency states.57
So far only one compound, pitolisant, has progressed to Phase III clinical trials. In two small, proof-of-concept studies, pitolisant reduced subjective EDS in narcolepsy.59,60 A subsequent multicenter, double-blind, parallel-groups study compared the safety and efficacy of pitolisant to modafinil and placebo in narcolepsy.61 Ninety-five patients were randomly allocated to one of the three study arms. Both drugs were uptitrated to maximum recommended doses (400 mg modafinil and 40 mg pitolisant) and continued for 8 weeks. Pitolisant was superior to placebo in reducing both subjective and objective EDS. Mean Epworth Sleepiness Scale (ESS) score decreased by 5.8 points with pitolisant and by 3.4 points with placebo (difference −3.0, 95% confidence interval: −5.6 to −0.4; P=0.024). Maintenance of Wakefulness Test (MWT) and the No-Go domain of the Sustained Attention to Response Task (SART) were also significantly improved with pitolisant. There were no significant differences in EDS reductions between pitolisant and modafinil. Pitolisant was well tolerated and only minor side effects were reported.
These results are encouraging, but we need to learn more about pitolisant before its role in clinical practice is established. The impact of pitolisant on cataplexy in humans is largely unknown and was not fully assessed in this trial. Longer-term effects, particularly in terms of potential for tolerance, have not been reported. A novel treatment is most needed in patients who are unable to tolerate currently used stimulants or with refractory sleepiness. It remains to be determined whether pitolisant is at all useful in these groups. Other H3 antagonists are still being evaluated in clinical trial (NCT00424931).
GABA-B agonists
Sodium oxybate is one of the most effective single agents for simultaneously treating all symptoms of narcolepsy.16,20 However, as already discussed, it is far from being the ideal solution. It is, therefore, important to find a compound with similar therapeutic efficacy that is more practical and safer to use.
GHB is an endogenous fatty acid and, at physiological concentration, functions as a neurotransmitter via its own receptor (GHBr). At pharmacological doses, GHB binds to γ-aminobutyric acid type b (GABA-B) receptor (GABAbR).23 The mechanism of action of GHB is still debated, but compelling evidence suggests that it is, at least partially, mediated by the GABAbR.20 In animal models, deactivation of GABAbR prevents all behavioral and sleep-related effects of exogenous GHB.62,63
Baclofen is another GABAbR agonist which is widely used in clinical practice, particularly in the treatment of spasticity. It is well tolerated with a good safety profile, although causes drowsiness at higher doses. Similar to GHB, baclofen increases slow-wave sleep and total sleep time, the mechanisms by which GHB was thought to improve nocturnal sleep and consequently reduce EDS and cataplexy. Disappointingly, unlike for GHB, baclofen trials showed no improvement in cataplexy or daytime sleepiness of human narcolepsy.64 This suggests that other, GABAbR-independent, mechanisms play a role. The differential effects of GHB and baclofen on sleep were also demonstrated in mice by Vienne et al.63 They found functional differences in one of the two GABAbR isoforms. It has been hypothesized that, whilst GABAbR is crucial in mediating the actions of both agonists, differences in receptor affinity, compound half-life, dose, and route of administration may be responsible for the varying effects.20
The hope of finding a GABAbR agonist useful in narcolepsy was recently restored by Black et al.65 Their well-designed study compared GHB and the r-enantiomer of baclofen, r-baclofen, in two different mouse models of narcolepsy, using a chronic dosing paradigm. R-baclofen suppressed cataplexy to a greater extent than GHB. It was also more effective in consolidating sleep and wakefulness, and increased time spent in NREM sleep and NREM delta power. R-baclofen has a threefold higher affinity for GABAbR than the racemate.65 Nonetheless, if interspecies differences once again prove important, r-baclofen may turn out to be no more useful in human narcolepsy then its racemic version. We obviously need to learn more about the role of GABAbR in narcolepsy. Several preparations of r-baclofen (arbaclofen [STX 209]) have already been studied in various conditions, including autism spectrum disorders, multiple sclerosis, and gastroesophageal reflux.66 Given the pharmacological knowledge already generated in these human studies and provided that the findings of Black et al65 are corroborated, the role of r-baclofen in human narcolepsy may be worth exploring.
Thyrotropin-releasing hormone analogs
Thyrotropin-releasing hormone (TRH) is a tripeptide traditionally known for its central regulatory role in the hypothalamic–pituitary–thyroid axis.67 Through this axis, TRH plays a major role in energy homeostasis, thermoregulation, and autonomic function.68 Independently of its endocrine role, TRH acts as a neuromodulator in the brain and exerts multiple effects. It increases locomotor activity, depolarizes spinal motor neurons, modulates pain perception, reverses phenobarbital induced sedation, decreases seizure threshold, and regulates mood.69–73 More recently, a role in pathological aging and neurodegenerative processes has been postulated.74 Owing to these properties, TRH has attracted interest as a potential treatment in various conditions, including depression, epilepsy, spinal cord injury, spinocerebellar degeneration, cancer-related fatigue, and Alzheimer’s disease.72,75–79 It is also a potent CNS stimulant and participates in regulation of sleep and wakefulness.73,80 For these reasons, TRH may be a useful treatment in narcolepsy.
The pharmacokinetic profile of TRH is characterized by a short half-life of up to 5 minutes, low intestinal absorption, and poor CNS permeability.81,82 The hormone is, therefore, not suitable for chronic clinical application. To overcome this, modifications of the C or N terminals have produced several TRH analogs of varying potencies, which have been studied in different neurological conditions.83 The potential role of TRH analogs has been explored in canine models of narcolepsy.84,85 In the first experiment,84 acute administration of biologically stable TRH analogs resulted in suppression of both slow-wave and REM sleep as well as significant reduction in cataplexy. In the second study,85 chronic administration of an oral TRH compound (CG-3703) was evaluated. Given over 2 weeks, this reduced cataplexy and EDS. It was reasonably well tolerated and, importantly, there were no behavioral or physiological changes to suggest endocrine side effects. However, drug tolerance was observed during the second week of administration, and, to the best of our knowledge, these early studies were not followed by further experiments or trials in human narcolepsy. Another potential barrier to the development of TRH analogs is their pleiotropic effects, which can undermine drug tolerance.
These analogs are probably species-specific and display varying affinities to TRH receptor subtypes. Two subtypes (TRH-R1 and TRH-R2) have been identified in several species. They exhibit an overall identity of around 50%.83 Both receptors have distinct patterns of distribution across the CNS, which led to the hypothesis that TRH-R2 is responsible for CNS effects of TRH, whereas TRH-R1 mediates thyroid-stimulating hormone release.86 Centrally acting TRH analogs, free of hormonal side effects, would be of particular interest in narcolepsy. However, the hypothesis of TRH-R2’s central role was later challenged.87 Furthermore, only a single receptor subtype has been identified in humans, which shows closer similarity to TRH-R2 than TRH-R1.88 Of many TRH analogs developed in animal models, taltirelin is one that shows improved CNS and lower hormonal activity and is also effective in humans. It is the only TRH analog which has been approved for the treatment of spinal muscular atrophy.88 Drug tolerance may also be less of a problem with taltirelin.89
The exact mechanism of TRH action in regulation of sleep and wakefulness is not well understood, but recent research sheds some light on the possible downstream pathways.
The dorsomedial hypothalamus is a center critical for the expression of circadian rhythms. Around 35% of its neurons projecting to the lateral hypothalamus contain TRH. In two studies, TRH was found to directly excite hypocretin neurons, and a close apposition between TRH-immunoreactive nerve terminals and hypocretin A-immunoreactive cell bodies was confirmed.90,91 Clearly, if TRH effects on sleep and wakefulness are mediated solely by hypocretin neurons, its analogs would be of little use in narcolepsy. However, other possible mechanisms by which TRH controls arousal is through the activation of histaminergic neurons and inhibition of melanin-concentrating hormone cells.92,93
Immunotherapy
Autoimmunity is thought to underlie the selective destruction of hypocretin neurons. Narcolepsy is tightly associated with HLA-DQB1*06:02 haplotype and polymorphisms in the T-cell receptor alpha locus.94 A protective HLA variant has been found in a genome-wide association study.95 Furthermore, circulating autoantibodies against Tribbles homolog 2 (TRIB2) have been detected in some narcoleptic patients in three independent studies.96–98 TRIB2 is a protein produced in hypocretin neurons. Anti-TRIB2 titers were particularly high in the first 2 years after narcolepsy onset. However, it is not clear whether they are pathogenic, incidental, or produced in response to hypocretin neuron damage.99
As with many other autoimmune conditions, environmental factors such as bacterial or viral infections probably induce an autoimmune response in genetically predisposed individuals. This concept is supported by a surge of narcolepsy cases following pandemic H1N1 infection and vaccination with Pandemrix.100–102 Molecular mimicry is the most plausible explanation for this.103
Trials have examined immunotherapy as a potential disease-modifying treatment. Corticosteroids, plasmapheresis, and intravenous immunoglobulins have been assessed in small studies, producing mixed results. Some patients did not respond at all while others improved, but complete and sustained symptom resolution was not achieved.104–107 Relapses required repeated treatment and side effects led to treatment discontinuation.108–110 The uncontrolled nature of these studies, small patient numbers, and varying treatment regimens prevent firm conclusions being drawn on the effectiveness of immunotherapy. However, one observation is valid: the successful interventions were typically administered early in the disease course. It is thought likely that narcolepsy with cataplexy only manifests when a patient has lost nearly all hypocretin cells. If so, then application of immunotherapy close to disease onset is probably conditional to its success.111
Monoclonal antibodies specifically targeting T or B lymphocytes have not been assessed in narcolepsy. There is one case report of a patient with narcolepsy who was subsequently diagnosed with a low-grade T-cell lymphoma and treated with alemtuzumab, a humanized monoclonal antibody that binds to CD52. During treatment, complete remission of cataplexy was observed and sustained until his death 1.5 years later.112
These compounds are potent immunosuppressants and their repeated administration risks potentially serious side effects. Before they are considered for trials in narcolepsy, we need to better understand which of the cellular and humoral immune processes are involved, so that the right biologics are chosen.
Another interesting technique is antigen-specific immunotherapy which involves vaccination with a selected autoantigen. It has been attempted in several autoimmune conditions including systemic sclerosis and type 1 diabetes mellitus. So far, outcomes have been disappointing, but research continues.113 This approach could be also be tried in narcolepsy provided a target antigen is found.
JZP-110
Finally, JZP-110 ((R)-2-amino-3-phenylpropylcarbamate hydrochloride) is a new compound previously known as ADX-N05, R228060, and YKP-10A. It is a hydrochloric acid salt of an optically pure phenylalanine derivative, which was originally developed as an antidepressant in animal models.114 Its antidepressant properties have not been confirmed in humans but a common side effect in Phase II trial was insomnia.115 A subsequent murine study showed the compound to have wake-promoting activity.114 Its mechanism of action is thought to involve simultaneous antagonism of dopamine and norepinephrine transporters.
According to the manufacturer, JZP-110 has significantly reduced subjective sleepiness (ESS) and increased objective alertness (MWT) in two Phase II placebo-controlled trials. These results have been presented at a conference but no data have yet been published.116 A Phase III long-term safety and maintenance of efficacy study is due to start shortly (NCT02348632). Formal publication of trial data is needed for us to understand whether JZP-110 has a potential role to play in the future treatment of narcolepsy.
Summary
Narcolepsy is a disease of complex pathophysiology, understanding of which has greatly increased over the last two decades. Treatment is also complex and remains challenging. While symptomatic improvement is usually possible, patients’ expectations are not always met. We have described some of the most promising areas of development for future therapeutics. Several potential solutions are still in the early stages of research. Substantial obstacles have to be overcome before it can be established which, if any, of these are likely to translate into readily available treatments. The complexity of sleep–wake regulation adds to the challenge. However, the hope for the future is that our therapeutic armamentarium for easing the burden of narcolepsy will be larger and more effective, and instead of discussing symptomatic treatment we will be comparing disease-modifying therapies.
The prospects for improving the treatment of narcolepsy look good, but to help achieve this, one more need must be met. The gap between symptom onset and diagnosis must be narrowed, as this is a major barrier to the timely provision of effective treatment. Narcolepsy is not a progressive disease, but if not diagnosed early, its impact on peoples’ lives can be difficult to reverse.
Disclosure
TGQ has received educational support in terms of conference attendance from UCB Pharma, the European supplier of sodium oxybate (European sleep conferences: 2012 and 2014). The authors report no other conflicts of interest in this work.
References
Thorpy MJ, Dauvilliers Y. Clinical and practical considerations in the pharmacologic management of narcolepsy. Sleep Med. 2015;16(1):9–18. | |
Frauscher B, Ehrmann L, Mitterling T, et al. Delayed diagnosis, range of severity, and multiple sleep comorbidities: a clinical and polysomnographic analysis of 100 patients of the innsbruck narcolepsy cohort. J Clin Sleep Med. 2013;9(8):805–812. | |
International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014. | |
Overeem S, Mignot E, van Dijk JG, Lammers GJ. Narcolepsy: clinical features, new pathophysiologic insights, and future perspectives. J Clin Neurophysiol. 2001;18(2):78–105. | |
Dauvilliers Y, Arnulf I, Mignot E. Narcolepsy with cataplexy. Lancet. 2007;369(9560):499–511. | |
Ohayon MM, Priest RG, Zulley J, Smirne S, Paiva T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population. Neurology. 2002;58(12):1826–1833. | |
Thorpy MJ, Krieger AC. Delayed diagnosis of narcolepsy: characterization and impact. Sleep Med. 2014;15(5):502–507. | |
Dodel R, Peter H, Spottke A, et al. Health-related quality of life in patients with narcolepsy. Sleep Med. 2007;8:733–741. | |
Ingravallo F, Gnucci V, Pizza F, et al. The burden of narcolepsy with cataplexy: how disease history and clinical features influence socio-economic outcomes. Sleep Med. 2012;13:1293–1300. | |
Jennum P, Ibsen R, Petersen ER, Knudsen S, Kjellberg J. Health, social, and economic consequences of narcolepsy: a controlled national study evaluating the societal effect on patients and their partners. Sleep Med. 2012;13(8):1086–1093. | |
Jennum P, Knudsen S, Kjellberg J. The economic consequences of narcolepsy. J Clin Sleep Med. 2009;5(3):240–245. | |
Broughton WA, Broughton RJ. Psychosocial impact of narcolepsy. Sleep. 1994;17(8 Suppl):S45–S49. | |
Daniels E, King MA, Smith IE, Shneerson JM. Health-related quality of life in narcolepsy. J Sleep Res. 2001;10(1):75–81. | |
Philip P, Sagaspe P, Lagarde E, et al. Sleep disorders and accidental risk in a large group of regular registered highway drivers. Sleep Med. 2010;11:973–979. | |
Nishino S, Kotorii N. Overview of management of narcolepsy. In: Goswami M, Pandi-Perumal SR, Thorphy MJ, editors. Narcolepsy: A Clinical Guide. New York: Springer; 2010:251–265. | |
Morgenthaler TI, Kapur VK, Brown T, et al; Standards of Practice Committee of the American Academy of Sleep Medicine. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep. 2007;30(12):1705–1711. | |
Prinzmetal M, Bloomberg W. The use of Benzedrine for the treatment of narcolepsy. JAMA. 1935;105(25):2051–2054. | |
Berman SM, Kuczenski R, McCracken JT, London ED. Potential adverse effects of amphetamine treatment on brain and behavior: a review. Mol Psychiatry. 2009;14(2):123–142. | |
Guilleminault C. Amphetamines and narcolepsy: use of the Stanford database. Sleep. 1993;16(3):199–201. | |
Mignot EJ. A practical guide to the therapy of narcolepsy and hypersomnia syndromes. Neurotherapeutics. 2012;9(4):739–752. | |
Mitler MM, Hajdukovic R. Relative efficacy of drugs for the treatment of sleepiness in narcolepsy. Sleep. 1991;14(3):218–220. | |
Billiard M, Dauvilliers Y, Dolenc-GroŠelj L, Lammers GJ, Mayer G, Sonka K. Management of narcolepsy in adults. In: Gilhus NE, Barnes M, Brainin M, editors. European Handbook of Neurological Management. Vol 1. 2nd ed. Oxford: Blackwell Publishing; 2011:513–538. | |
Dauvilliers Y, Siegel JM, Lopez R, Torontali ZA, Peever JH. Cataplexy – clinical aspects, pathophysiology and management strategy. Nat Rev Neurol. 2014;10(7):386–395. | |
Guilleminault C, Aftab FA, Karadeniz D, Philip P, Leger D. Problems associated with switch to modafinil – a novel alerting agent in narcolepsy. Eur J Neurol. 2000;7(4):381–384. | |
Izzi F, Placidi F, Marciani MG, et al. Effective treatment of narcolepsy-cataplexy with duloxetine: a report of three cases. Sleep Med. 2009;10(1):153–154. | |
Zvosec DL, Smith SW, Porrata T, Strobl AQ, Dyer JE. Case series of 226 γ-hydroxybutyrate-associated deaths: lethal toxicity and trauma. Am J Emerg Med. 2011;29(3):319–332. | |
McDonnell K. Narcolepsy patient community prepares to share life impacts, treatment perspectives with FDA regulators [press release]. Worcester, MA: Wake Up Narcolepsy, Inc.; 2013 [September 19]. Available from: http://www.wakeupnarcolepsy.org/press-releasenarcolepsy-patient-community-prepares-share-life-impacts-treatment-perspectives-fda-regulators. Accessed March 20, 2015. | |
Shneerson JM, Dauvilliers YA, Plazzi G, Myers AJ, Garcia-Borreguero D. The impact of narcolepsy and its treatment – a European study. Eur Neurol Rev. 2008;3(2):105–108. | |
Thorpy M, Zhao CG, Dauvilliers Y. Management of narcolepsy during pregnancy. Sleep Med. 2013;14(4):367–376. | |
Hasegawa E, Yanagisawa M, Sakurai T, Mieda M. Orexin neurons suppress narcolepsy via 2 distinct efferent pathways. J Clin Invest. 2014;124(2):604–616. | |
Bourgin P, Huitrón-Résendiz S, Spier AD, et al. Hypocretin-1 modulates rapid eye movement sleep through activation of locus coeruleus neurons. J Neurosci. 2000;20(20):7760–7765. | |
Huang ZL, Qu WM, Li WD, et al. Arousal effect of orexin A depends on activation of the histaminergic system. Proc Natl Acad Sci U S A. 2001;98(17):9965–9970. | |
Xi MC, Morales FR, Chase MH. Effects on sleep and wakefulness of the injection of hypocretin-1 (orexin-A) into the laterodorsal tegmental nucleus of the cat. Brain Res. 2001;901(1–2):259–264. | |
Mieda M, Willie JT, Hara J, Sinton CM, Sakurai T, Yanagisawa M. Orexin peptides prevent cataplexy and improve wakefulness in an orexin neuron-ablated model of narcolepsy in mice. Proc Natl Acad Sci U S A. 2004;101(13):4649–4654. | |
Thompson MD, Xhaard H, Sakurai T, Rainero I, Kukkonen JP. OX1 and OX2 orexin/hypocretin receptor pharmacogenetics. Front Neurosci. 2014;8:57. | |
Mishima K, Fujiki N, Yoshida Y, et al. Hypocretin receptor expression in canine and murine narcolepsy models and in hypocretin-ligand deficient human narcolepsy. Sleep. 2008;31(8):1119–1126. | |
Fujiki N, Yoshida Y, Ripley B, Mignot E, Nishino S. Effects of IV and ICV hypocretin-1 (orexin A) in hypocretin receptor-2 gene mutated narcoleptic dogs and IV hypocretin-1 replacement therapy in a hypocretin-ligand-deficient narcoleptic dog. Sleep. 2003;26(8):953–959. | |
John J, Wu MF, Siegel JM. Systemic administration of hypocretin-1 reduces cataplexy and normalizes sleep and waking durations in narcoleptic dogs. Sleep Res Online. 2000;3(1):23–28. | |
Hanson LR, Frey WH 2nd. Intranasal delivery bypasses the blood-brain barrier to target therapeutic agents to the central nervous system and treat neurodegenerative disease. BMC Neurosci. 2008; 9 Suppl 3:S5. | |
Dhuria SV, Hanson LR, Frey WH 2nd. Novel vasoconstrictor formulation to enhance intranasal targeting of neuropeptide therapeutics to the central nervous system. J Pharmacol Exp Ther. 2009;328(1):312–320. | |
Deadwyler SA, Porrino L, Siegel JM, Hampson RE. Systemic and nasal delivery of orexin-A (hypocretin-1) reduces the effects of sleep deprivation on cognitive performance in nonhuman primates. J Neurosci. 2007;27(52):14239–14247. | |
Baier PC, Weinhold SL, Huth V, Gottwald B, Ferstl R, Hinze-Selch D. Olfactory dysfunction in patients with narcolepsy with cataplexy is restored by intranasal orexin a (hypocretin-1). Brain 2008;131(Pt 10):2734–2741. | |
Baier PC, Hallschmid M, Seeck-Hirschner M, et al. Effects of intranasal hypocretin-1 (orexin A) on sleep in narcolepsy with cataplexy. Sleep Med. 2011;12(10):941–946. | |
Lammers GJ. Intranasal hypocretin-1: making sense of scents? Sleep Med. 2011;12(10):939–940. | |
Weinhold SL, Seeck-Hirschner M, Nowak A, Hallschmid M, Göder R, Baier PC. The effect of intranasal orexin-A (hypocretin-1) on sleep, wakefulness and attention in narcolepsy with cataplexy. Behav Brain Res. 2014;262:8–13. | |
Sun H, Kennedy WP, Wilbraham D. Effects of suvorexant, an orexin receptor antagonist, on sleep parameters as measured by polysomnography in healthy men. Sleep. 2013;36(2):259–267. | |
Boss C. Orexin receptor antagonists – a patent review (2010 to August 2014). Expert Opin Ther Pat. 2014;24(12):1367–1381. | |
Heifetz A, Barker O, Morris GB, Law RJ, Slack M, Biggin PC. Toward an understanding of agonist binding to human orexin-1 and orexin-2 receptors with G-protein-coupled receptor modeling and site-directed mutagenesis. Biochemistry. 2013;52(46):8246–8260. | |
Arias-Carrión O, Murillo-Rodríguez E. Effects of hypocretin/orexin cell transplantation on narcoleptic-like sleep behavior in rats. PLoS One. 2014;9(4):e95342. | |
Stayte S, Vissel B. Advances in non-dopaminergic treatments for Parkinson’s disease. Front Neurosci. 2014;8:113. | |
Liu M, Thankachan S, Kaur S, et al. Orexin (hypocretin) gene transfer diminishes narcoleptic sleep behavior in mice. Eur J Neurosci. 2008;28:1382–1393. | |
Liu M, Blanco-Centurion C, Konadhode R, et al. Orexin gene transfer into zona incerta neurons suppresses muscle paralysis in narcoleptic mice. J Neurosci. 2011;31:6028–6040. | |
Blanco-Centurion C, Liu M, Konadhode R, Pelluru D, Shiromani PJ. Effects of orexin gene transfer in the dorsolateral pons in orexin knockout mice. Sleep. 2013;36(1):31–40. | |
Haas HL, Sergeeva OA, Selbach O. Histamine in the nervous system. Physiol Rev. 2008;88(3):1183–1241. | |
Lin JS, Sergeeva OA, Haas HL. Histamine H3 receptors and sleep-wake regulation. J Pharmacol Exp Ther. 2011;336(1):17–23. | |
Nishino S, Sakurai E, Nevsimalova S, et al. Decreased CSF histamine in narcolepsy with and without low CSF hypocretin-1 in comparison to healthy controls. Sleep. 2009;32(2):175–180. | |
De la Herrán-Arita AK, García-García F. Current and emerging options for the drug treatment of narcolepsy. Drugs. 2013;73(16):1771–1781. | |
Schwartz JC. The histamine H3 receptor: from discovery to clinical trials with pitolisant. Br J Pharmacol. 2011;163(4):713–721. | |
Lin JS, Dauvilliers Y, Arnulf I, et al. An inverse agonist of the histamine H(3) receptor improves wakefulness in narcolepsy: studies in orexin-/- mice and patients. Neurobiol Dis. 2008;30(1):74–83. | |
Inocente C, Arnulf I, Bastuji H, et al. Pitolisant, an inverse agonist of the histamine H3 receptor: an alternative stimulant for narcolepsy-cataplexy in teenagers with refractory sleepiness. Clin Neuropharmacol. 2012;35(2):55–60. | |
Dauvilliers Y, Bassetti C, Lammers GJ, et al; HARMONY I study group. Pitolisant versus placebo or modafinil in patients with narcolepsy: a double-blind, randomised trial. Lancet Neurol. 2013;12(11):1068–1075. | |
Kaupmann K, Cryan JF, Wellendorph P, et al. Specific gamma-hydroxybutyrate-binding sites but loss of pharmacological effects of gamma-hydroxybutyrate in GABA(B)(1)-deficient mice. Eur J Neurosci. 2003;18(10):2722–2730. | |
Vienne J, Bettler B, Franken P, Tafti M. Differential effects of GABAB receptor subtypes, {gamma}-hydroxybutyric acid, and baclofen on EEG activity and sleep regulation. J Neurosci. 2010;30(42):14194–14204. | |
Huang YS, Guilleminault C. Narcolepsy: action of two gamma-aminobutyric acid type B agonists, baclofen and sodium oxybate. Pediatr Neurol. 2009;41(1):9–16. | |
Black SW, Morairty SR, Chen TM, et al. GABAB agonism promotes sleep and reduces cataplexy in murine narcolepsy. J Neurosci. 2014; 34(19):6485–6494. | |
Frye RE. Clinical potential, safety, and tolerability of arbaclofen in the treatment of autism spectrum disorder. Drug Healthc Patient Saf. 2014;6:69–76. | |
Kolesnick RN, Gershengorn MC. Thyrotropin-releasing hormone and the pituitary. New insights into the mechanisms of stimulated secretion and clinical usage. Am J Med. 1985;79(6):729–739. | |
Nillni EA. Regulation of the hypothalamic thyrotropin releasing hormone (TRH) neuron by neuronal and peripheral inputs. Front Neuroendocrinol. 2010;31(2):134–156. | |
Sun Y, Zupan B, Raaka BM, Toth M, Gershengorn MC. TRH-receptor-type-2-deficient mice are euthyroid and exhibit increased depression and reduced anxiety phenotypes. Neuropsychopharmacology. 2009;34(6):1601–1608. | |
Van den Bergh P, Octave JN, Lechan RM. Muscle denervation increases thyrotropin-releasing hormone (TRH) biosynthesis in the rat medullary raphe. Brain Res. 1991;566(1–2):219–224. | |
Eto K, Kim SK, Nabekura J, Ishibashi H. Taltirelin, a thyrotropin-releasing hormone analog, alleviates mechanical allodynia through activation of descending monoaminergic neurons in persistent inflammatory pain. Brain Res. 2011;1414:50–57. | |
Horita A. An update on the CNS actions of TRH and its analogs. Life Sci. 1998;62:1443–1448. | |
Lechan RM, Fekete C. The TRH neuron: a hypothalamic integrator of energy metabolism. Prog Brain Res. 2006;153:209–235. | |
Daimon CM, Chirdon P, Maudsley S, Martin B. The role of thyrotropin releasing hormone in aging and neurodegenerative diseases. Am J Alzheimers Dis (Columbia). 2013;1(1). | |
Pitts LH, Ross A, Chase GA, Faden AI. Treatment with thyrotropin-releasing hormone (TRH) in patients with traumatic spinal cord injuries. J Neurotrauma. 1995;12(3):235–243. | |
Kelly JA, Boyle NT, Cole N, et al. First-in-class thyrotropin-releasing hormone (TRH)-based compound binds to a pharmacologically distinct TRH receptor subtype in human brain and is effective in neurodegenerative models. Neuropharmacology. 2015;89:193–203. | |
Kamath J, Feinn R, Winokur A. Thyrotropin-releasing hormone as a treatment for cancer-related fatigue: a randomized controlled study. Support Care Cancer. 2012;20(8):1745–1753. | |
Sah N, Rajput SK, Singh JN, et al. L-pGlu-(2-propyl)-L-His-L-ProNH2 attenuates 4-aminopyridine-induced epileptiform activity and sodium current: a possible action of new thyrotropin-releasing hormone analog for its anticonvulsant potential. Neuroscience. 2011;199:74–85. | |
Kato Z, Okuda M, Okumura Y, et al. Oral administration of the thyrotropin-releasing hormone (TRH) analogue, taltireline hydrate, in spinal muscular atrophy. J Child Neurol. 2009;24(8):1010–1012. | |
Broberger C, McCormick DA. Excitatory effects of thyrotropin-releasing hormone in the thalamus. J Neurosci. 2005;25(7):1664–1673. | |
Khomane KS, Meena CL, Jain R, Bansal AK. Novel thyrotropin-releasing hormone analogs: a patent review. Expert Opin Ther Pat. 2011;21(11):1673–1691. | |
Redding TW, Schally AV. On the half life of thyrotropin-releasing hormone in rats. Neuroendocrinology. 1972;9(4):250–256. | |
Monga V, Meena C, Rajput S, et al. Synthesis, receptor binding, and CNS pharmacological studies of new thyrotropin-releasing hormone (TRH) analogues. ChemMedChem. 2011;6(3):531–543. | |
Nishino S, Arrigoni J, Shelton J, Kanbayashi T, Dement WC, Mignot E. Effects of thyrotropin-releasing hormone and its analogs on daytime sleepiness and cataplexy in canine narcolepsy. J Neurosci. 1997; 17(16):6401–6408. | |
Riehl J, Honda K, Kwan M, Hong J, Mignot E, Nishino S. Chronic oral administration of CG-3703, a thyrotropin releasing hormone analog, increases wake and decreases cataplexy in canine narcolepsy. Neuropsychopharmacology. 2000;23(1):34–45. | |
Monga V, Meena CL, Kaur N, Jain R. Chemistry and biology of thyrotropin-releasing hormone (TRH) and its analogs. Curr Med Chem. 2008;15(26):2718–2733. | |
Thirunarayanan N, Nir EA, Raaka BM, Gershengorn MC. Thyrotropin-releasing hormone receptor type 1 (TRH-R1), not TRH-R2, primarily mediates taltirelin actions in the CNS of mice. Neuropsychopharmacology. 2013;38(6):950–956. | |
Thirunarayanan N, Raaka BM, Gershengorn MC. Taltirelin is a superagonist at the human thyrotropin-releasing hormone receptor. Front Endocrinol (Lausanne). 2012;3:120. | |
Asai H, Asahi T, Yamamura M, Yamauchi-Kohno R, Saito A. Lack of behavioral tolerance by repeated treatment with taltirelin hydrate, a thyrotropin-releasing hormone analog, in rats. Pharmacol Biochem Behav. 2005;82(4):646–651. | |
Hara J, Gerashchenko D, Wisor JP, Sakurai T, Xie X, Kilduff TS. Thyrotropin-releasing hormone increases behavioral arousal through modulation of hypocretin/orexin neurons. J Neurosci. 2009;29(12):3705–3714. | |
González JA, Horjales-Araujo E, Fugger L, Broberger C, Burdakov D. Stimulation of orexin/hypocretin neurones by thyrotropin-releasing hormone. J Physiol. 2009;587(Pt 6):1179–1186. | |
Parmentier R, Kolbaev S, Klyuch BP, et al. Excitation of histaminergic tuberomamillary neurons by thyrotropin-releasing hormone. J Neurosci. 2009;29(14):4471–4483. | |
Zhang X, van den Pol AN. Thyrotropin-releasing hormone (TRH) inhibits melanin-concentrating hormone neurons: implications for TRH-mediated anorexic and arousal actions. J Neurosci. 2012;32(9):3032–3043. | |
Hallmayer J, Faraco J, Lin L, et al. Narcolepsy is strongly associated with the T-cell receptor alpha locus. Nat Genet. 2009;41:708–711. | |
Hor H, Kutalik Z, Dauvilliers Y, et al. Genome-wide association study identifies new HLA class II haplotypes strongly protective against narcolepsy. Nat Genet. 2010;42:786–789. | |
Cvetkovic-Lopes V, Bayer L, Dorsaz S, et al. Elevated Tribbles homolog 2-specific antibody levels in narcolepsy patients. J Clin Invest. 2010;120:713–719. | |
Toyoda H, Tanaka S, Miyagawa T, Honda Y, Tokynaga K, Honda M. Anti-Tribbles homolog 2 autoantibodies in Japanese patients with narcolepsy. Sleep. 2010;33:875–878. | |
Kawashima M, Lin L, Tanaka S, et al. Anti-Tribbles homolog 2 (TRIB2) autoantibodies in narcolepsy are associated with recent onset of cataplexy. Sleep. 2010;33:869–874. | |
Lim AS, Scammell TE. The trouble with Tribbles: do antibodies against TRIB2 cause narcolepsy? Sleep. 2010;33(7):857–858. | |
Han F, Lin L, Warby SC, et al. Narcolepsy onset is seasonal and increased following the 2009 H1N1 pandemic in China. Ann Neurol. 2011;70:410–417. | |
Partinen M, Saarenpää-Heikkilä O, Ilveskoski I, et al. Increased incidence and clinical picture of childhood narcolepsy following the 2009 H1N1 pandemic vaccination campaign in Finland. PLoS One. 2012;7:e33723. | |
Heier MS, Gautvik KM, Wannag E, et al. Incidence of narcolepsy in Norwegian children and adolescents after vaccination against H1N1 influenza A. Sleep Med. 2013;14:867–871. | |
Ahmed SS, Schur PH, MacDonald NE, Steinman L. Narcolepsy, 2009 A(H1N1) pandemic influenza, and pandemic influenza vaccinations: what is known and unknown about the neurological disorder, the role for autoimmunity, and vaccine adjuvants. J Autoimmun. 2014;50:1–11. | |
Valko PO, Khatami R, Baumann CR, Bassetti CL. No persistent effect of intravenous immunoglobulins in patients with narcolepsy with cataplexy. J Neurol. 2008;255(12):1900–1903. | |
Plazzi G, Poli F, Franceschini C, et al. Intravenous high-dose immunoglobulin treatment in recent onset childhood narcolepsy with cataplexy. J Neurol. 2008;255(10):1549–1554. | |
Dauvilliers Y, Carlander B, Rivier F, Touchon J, Tafti M. Successful management of cataplexy with intravenous immunoglobulins shortly after narcolepsy onset. Ann Neurol. 2004;56:905–908. | |
Dauvilliers Y. Follow-up of four narcolepsy patients treated with intravenous immunoglobulins. Ann Neurol. 2006;60(1):153. | |
Lecendreux M, Maret S, Bassetti C, Mouren MC, Tafti M. Clinical efficacy of high-dose intravenous immunoglobulins near the onset of narcolepsy in a 10-year-old boy. J Sleep Res. 2003;12(4):347–348. | |
Zuberi SM, Mignot E, Ling L, et al. Variable response to intravenous immunoglobulin therapy in childhood narcolepsy. J Sleep Res. 2004; 13(Suppl 1):828. Abstract. | |
Chen W, Black J, Call P, Mignot E. Late-onset narcolepsy presenting as rapidly progressing muscle weakness: response to plasmapheresis. Ann Neurol. 2005;58(3):489–490. | |
Thannickal TC, Moore RY, Nienhuis R, et al. Reduced number of hypocretin neurons in human narcolepsy. Neuron. 2000;27(3):469–474. | |
Donjacour CE, Lammers GJ. A remarkable effect of alemtuzumab in a patient suffering from narcolepsy with cataplexy. J Sleep Res. 2012;21(4):479–480. | |
Sabatos-Peyton CA, Verhagen J, Wraith DC. Antigen-specific immunotherapy of autoimmune and allergic diseases. Curr Opin Immunol. 2010;22(5):609–615. | |
Hasan S, Pradervand S, Ahnaou A, Drinkenburg W, Tafti M, Franken P. How to keep the brain awake? The complex molecular pharmacogenetics of wake promotion. Neuropsychopharmacology. 2009;34(7):1625–1640. | |
Amsterdam JD, Brunswick DJ, Hundert M. A single-site, double-blind, placebo-controlled, dose-ranging study of YKP10A – a putative, new antidepressant. Prog Neuropsychopharmacol Biol Psychiatry. 2002; 26(7–8):1333–1338. | |
Black J, Swick T, Feldman N, et al. Efficacy and safety of oral ADX-N05 for the treatment of excessive daytime sleepiness in adults with narcolepsy: results of a randomized, double-blind, placebo-controlled trial [abstract]. Presented at: 28th Annual Meeting of the Associated Professional Sleep Societies (SLEEP); May 31–June 4, 2014; Minneapolis, MN. Abstract LBA4. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.