")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Unmet Need for Social and Emotional Support and Lack of Recalled Screening Is Associated with Depression in the Long-Term Course After Stroke
Authors Padberg I , Hotter B, Liebenau A , Knispel P , Lehnerer S , Heel S , Wellwood I , Meisel A
Received 3 September 2019
Accepted for publication 22 December 2019
Published 1 April 2020 Volume 2020:13 Pages 285—293
DOI https://doi.org/10.2147/RMHP.S228265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Inken Padberg,1 Benjamin Hotter,1,2 Andrea Liebenau,1 Petra Knispel,1,3 Sophie Lehnerer,1,2 Sabine Heel,4 Ian Wellwood,5 Andreas Meisel1–3
1Center for Stroke Research Berlin (CSB), Charité Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Berlin, Germany; 2Neurocure Clinical Research Center, Department of Neurology, Charité Universitätsmedizin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Berlin, Germany; 3Berliner Schlaganfall-Allianz e.V., Berlin, Germany; 4Zentrum für Ambulante Neuropsychologie und Verhaltenstherapie (ZANV), Berlin, Germany; 5Department of Public-Health and Primary Care, University of Cambridge, Cambridge, UK
Correspondence: Inken Padberg Tel +49 30 450 560142
Fax +49 30 450 560952
Email [email protected]
Purpose: Details on adequate care and prevalence of depression in long-term stroke aftercare are limited. We aimed to determine long-term depression rates after stroke and to test for an association between depression and inadequate screening, socio-economic complications and lack of sub-optimal care.
Patients and Methods: In this cross-sectional study, 57 patients were re-invited into the clinic 2– 3 years after stroke. Patients were interviewed about recalled screening concerning depression and unmet needs. Depression, the patient’s social situation, and confounders were assessed by standardized scores.
Results: In our study, 20% (n = 11) of patients were classified as depressed by the HDRS-17 score result. However, only 36% of all patients recalled to have been previously screened for depression and only 43% of those patients also recalled out-patient screening. Patients classified as depressed reported significantly lower recalled screening rates (9% vs 43%; p = 0.036) and higher rates of self-reported unmet need with emotional problems (72% vs 18%; p < 0.001). Depression in our study was further associated with a worse socio-economic situation, fewer social contacts, unmet needs with regard to emotional problems and higher rates of recommendations to apply for additional social support.
Conclusion: Our data suggest that systematic out-patient screening for depression is lacking in stroke aftercare. Furthermore, the high rate of unmet emotional needs, the poor socio-economic situation and the higher rates of recommendations for social counselling and application for benefits suggest an undersupply of care in the out-patient setting that is more prominent in patients with depression and warrants further studies to investigate the underlying causes.
Keywords: health-care quality, social-care, risk management, stroke, depression
Plain Language Summary
The study was done to better understand how frequently depression occurs 2–3 years post-stroke, whether it is continuously screened for and whether patients with post-stroke depression had more social problems than patients without depression.
We tested for depression by using a commonly used questionnaire asking for major symptoms of the disease. We also assessed the socio-economic situation, the social contacts and the housing situation of the patients and asked the patients whether a health-care professional had previously asked them for symptoms of depression after stroke.
We found that very few patients were tested for symptoms of depression after stroke during out-patient care. Compared to patients without depression, patients with a score result indicating depression less frequently reported to have previously been asked for symptoms of depression after stroke. Furthermore, patients with depression also had more social problems than patients without depression. Finally, we found that all patients classified as depressed by a questionnaire comprised of 17-items (HDRS-17) would also have been detected by using a reduced version of the questionnaire consisting of only two questions.
Introduction
Depression after stroke remains a major clinical challenge with a recent systematic review estimating a proportional frequency for post-stroke depression of approximately 30%.1 It is associated with disability, poor quality of life, increased mortality, social isolation and slow recovery2 as well as with non-adherence to medication in different medical conditions.3,4 Despite this, depression often remains undertreated.5,6 Depressive symptoms after stroke can occur directly after the event but also can arise in the course of long-term disease development and management.1 Similar to other chronical diseases, the transfer from the hospital setting (acute or rehabilitation) to out-patient aftercare presents a challenge for continuous care in stroke patients. Here, deficits may limit the potential rehabilitation success as continuous care and training of function has been reported to result in improvements up to several years after stroke-event if provided with sufficient intensity.7 Hereby, general health, opportunity and motivation for training are important factors influencing success. A recent review focused on depression as a general risk factor for organic disease and concluded, that by inducing unfavorable pathophysiological and behavioral processes, social and emotional loneliness contributes to the link between depression and physical illness.8 Vice versa it is well known that depression also is a common complication caused by stroke.1 Underdiagnosed or inadequately treated depression therefore may represent a risk factor for post-stroke complications. Current guidelines state there is a need for more research to determine if screening for depression – in conjunction with collaborative care – helps to reduce its prevalence.9 In particular, there is a lack of evidence with regard to long-term care extending up to 2–3 years after stroke. Explicit recommendations on timing of screening for depression and its relation to long-term prevalence, as well as the development of potential complications do not exist. Current clinical guidelines highlight the need for time-efficient screening tools suitable to identify patients with post-stroke depression in the aftercare setting. Short dichotomous screening tools, such as the PHQ-9 score have been shown to be effective in the general population, however, have not yet been tested in stroke patients.9,10
Here, we aimed to investigate whether prevalent depression was associated with a self-reported lack of recalled screening for depression and care in the long-term course after stroke. Further, we sought to test the hypothesis that depression is associated with loss of social support, a worse housing and financial situation, insufficient care and lower quality of life 2–3 years after stroke. Moreover, we conducted exploratory tests of sensitivity and specificity of a potential simple screening tool for identifying patients with post-stroke depression.
Materials and Methods
Study-Design
The present analysis is part of the observational, cross-sectional MAS-I study (clinical trial registration number NCT02320994), which has been described previously.11 Briefly, MAS-I aimed to assess the needs and disease burden of community-dwelling stroke patients and their carers and to compare their treatment to evidence-based guidelines by a stroke neurologist. We recruited participants employing purposive sampling of previous participants of two independent and completed hospital-based acute stroke studies (a randomised-controlled trial STRAWINSKI NCT0126454934 and an observational study PREDICT NCT0107972835). Inclusion criteria used in PREDICT were acute ischemic stroke of any severity (NIHSS ≥ 1 at study inclusion, TIA excluded) and any localization, symptom onset ≤36 h and age ≥18 years. Inclusion criteria used in STRAWINSKI were age ≥18 years and severe ischemic stroke in the middle cerebral artery (score of >9 on the National Institute of Health Stroke Scale). In MAS-1, all previous participants of STRAWINSKI and PREDICT living in the Berlin metropolitan area 2–3 years after the event were invited to take part and visit our out-patient clinic for a follow-up assessment. No financial incentive was provided.11 The assessment included a comprehensive interview and an examination using the Post-Stroke-Checklist (PSC) as well as validated standard measures of (among other domains) depression, quality of life, secondary prevention and social needs. Current use of medication was assessed with a focus on secondary prevention. Recalled screening for depression and history of intake of anti-depressant medication was assessed based on self-reported information and review of discharge letters.
To counter selection bias, we offered to pay travel costs to and from our center.
Scores and Outcome Measures
In our primary research question, we attempted to understand which factors might contribute to the development of prevalent depression in the long-term aftercare after stroke. The main parameter of interest was self-reported recalled screening and its association with depression which was diagnosed using the HDRS-17 score. Further, scores used included the Stroke Survivor Need Scale, the Nikolaus Score and the EQ-5D-5L, the modified Rankin Scale, the MoCA and the Post-Stroke Checklist (PSC). Details on the above-described scores can be found in the Supplementary methods section.
Statistical Analysis
Statistical analyses were performed using SPSS software version 22.
Except for age where the assumption of normal distribution was not rejected by the Kolmogorov Smirnov test, all other group comparisons were subjected to non-parametric testing by Mann–Whitney-U, Fishers exact or chi-square test. Differences between frequency outcomes were calculated by Fisher´s exact test where the expected frequency count was <5 and by chi-square where this was not the case. Correlations were calculated by Spearman´s Rho. Missing data were subjected to listwise deletion. P-values related to primary and secondary research questions were controlled for multiple testing using the Benjamini-Hochberg procedure. Due to the small number of participants for most part of the analysis, we used simple parametric and non-parametric statistical testing. However, to clarify whether the association between recalled screening and depression may have been confounded by age, cognition, years of education, modified-Rankin scale and sex an explorative logistic regression model correcting for the factors was additionally carried out using Stata version 14.2.
Results
Prevalence, Recalled Screening and Care and Consequences of Depression
Overall 516 subjects were invited out of which 57 patients (11%) responded and were included in MAS-1.11 For 56 of these patients depression was assessed using the HDRS-17 depression scale. Eleven (20%) of the assessed patients would be diagnosed as depressed according to the score result.
Data about recalled screening for depression after stroke were available from 55 of those 56 patients. According to the patient's self-report only a minority (n=20; 36%) recalled to have been screened for depression after stroke. To better understand whether the prevalence of depression might be associated with recalled screening we compared rates of self-reported prior screening and prevalent depression according to HDRS-17 score result. Recalled screening rates were 9% (n=1) in patients who were diagnosed as depressed and 43% (n=19) in non-depressed patients, resulting in a significant difference (p=0.036) (Table 1). Furthermore, even in the group of patients who indicated to have been previously screened for depression less than 43% indicated screening had been done during the out-patient phase of disease management. In order to exclude potential modifiers or confounders causing the observed association between recalled screening and prevalent depression, we additionally calculated a logistic regression model and corrected for current age, sex, years of education, cognition and modified Rankin scale (collected 3 months after stroke). Also after correction, the association remained significant. Also, in a direct comparison none of these factors differed significantly between patients with and without prevalent depression according to HDRS-17 score result (Table 2).
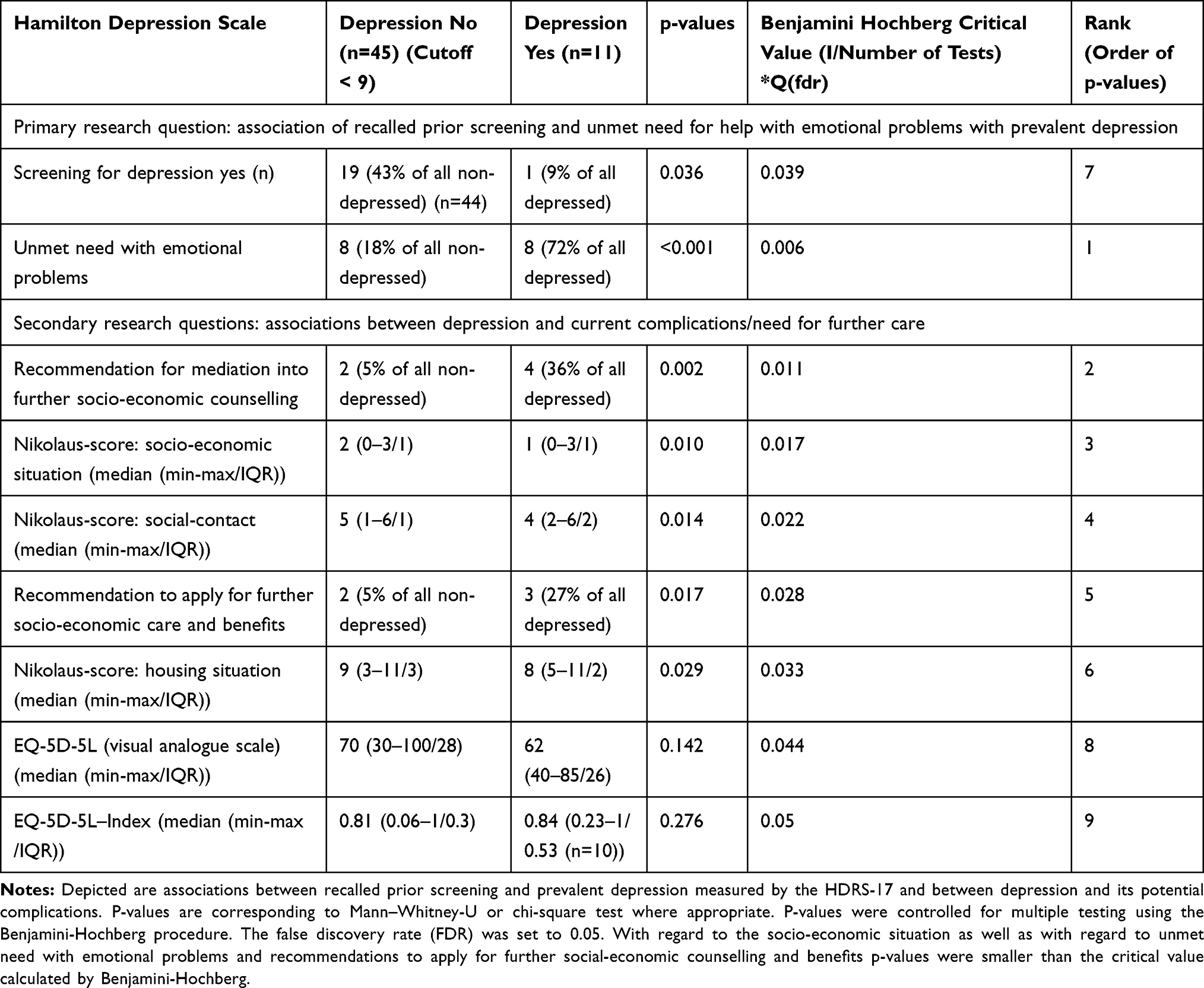 |
Table 1 Overview of Recalled Screening, Quality of Life, Social Care and Unmet Emotional Long-Term Needs After Stroke are Depicted in Patients with and Without Prevalent Depression |
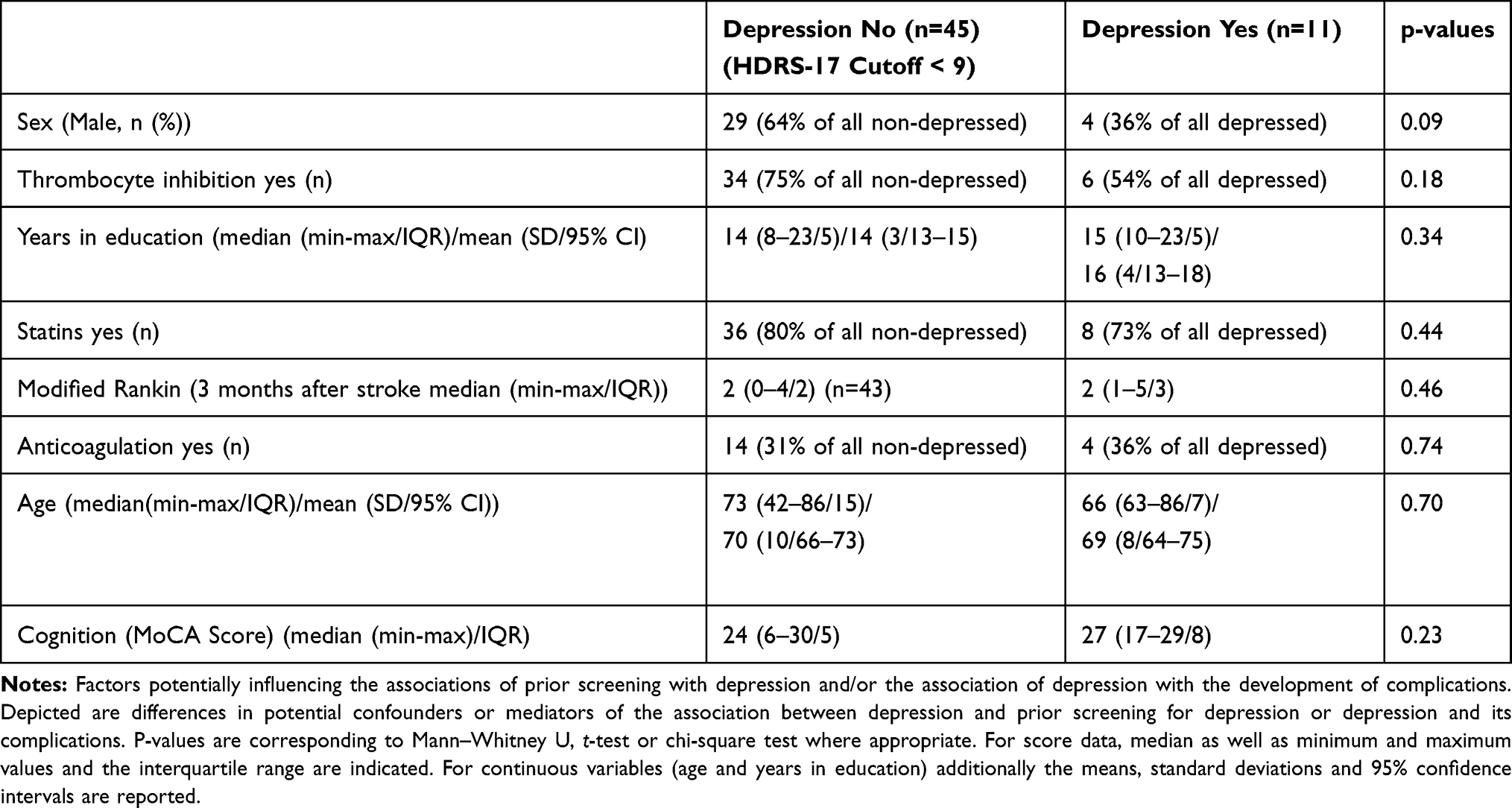 |
Table 2 Patient Characteristics That are Potentially Associated with Depression |
We furthermore found that eight of eleven (72%) patients with and eight of 45 (18%) patients without a score-based diagnosis of depression also expressed an unmet need with regard to help with emotional problems (defined as confusion/depression/crying) after the stroke (p-value <0.001) (Table 1).
For 34 of our 56 patients, information on whether prior anti-depressant medication had been prescribed was available. Altogether eleven of these 34 patients had a history of prior treatment with anti-depressants mostly starting during the stay in the acute or rehabilitation hospital due to the acute presence of symptoms (such as crying/loss of interest) for depression (Table 3).
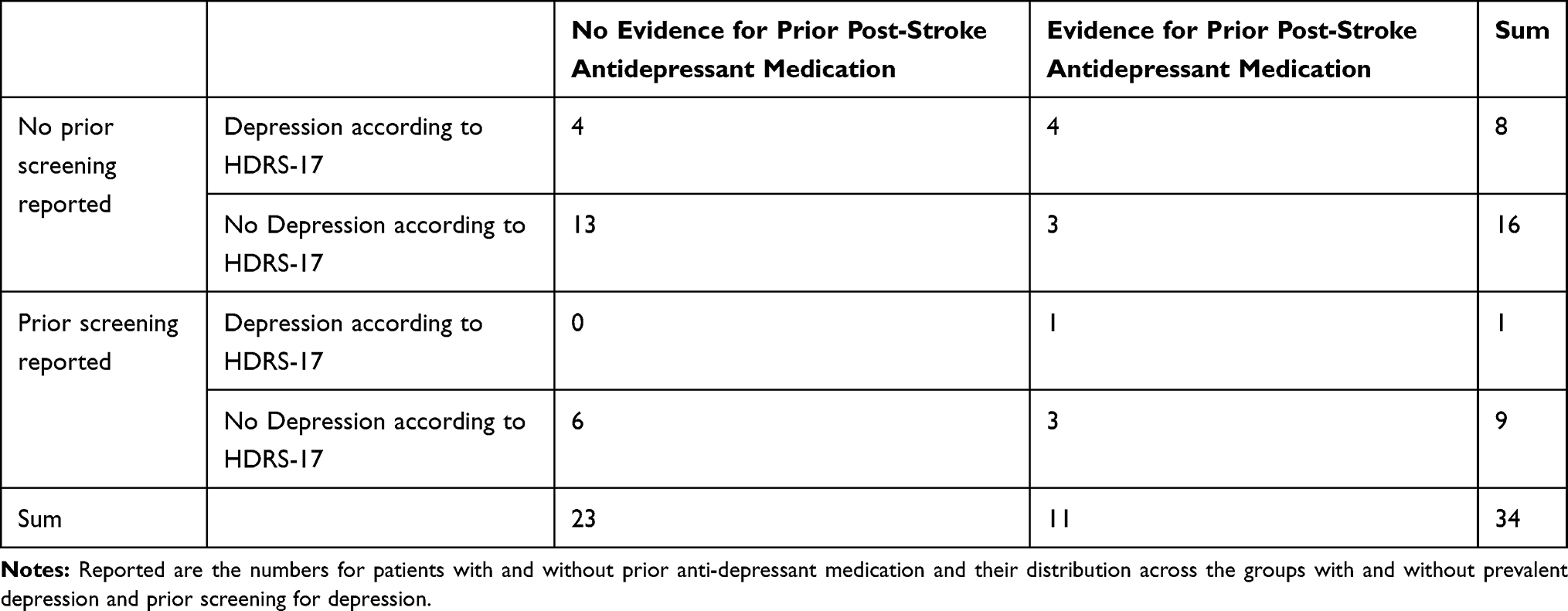 |
Table 3 Overview of Intake of Antidepressant Medication After Stroke |
Interestingly, five of eleven patients with anti-depressant medication in our study still were classified as depressed according to their current HDRS-17 result and four of these five patients did not recall to have previously been screened for depression (Table 3). Altogether the recalled screening rate reported in patients with a history of prior anti-depressant treatment did not differ from the overall recalled screening rate for depression (36%) (Table 3).
Association Between Depression, Current Social Situation, Medication Adherence and Quality of Life
With regard to their current situation, patients with depression reported significantly lower social contacts and a worse socio-economic and housing situation than patients without depression (Table 1). The socio-economic situation in our study was evaluated by an experienced social worker who recommended further mediation, counselling or application for benefits if necessary. To better understand whether differences in the socio-economic situation also reflected differences in the need for further intervention, in a next step we compared the rate of recommendations for counselling and applications for benefits in depressed and non-depressed patients. We found significantly higher recommendation rates for further intervention in patients with depression (Table 1).
These results remained significant even after correction for multiple testing (Table 1). However, we observed no association between depression and overall level of quality of life in this group comparison. Despite of this post-hoc analyses for correlation between HDRS-17 values with the visual analogue scale of the EQ-5D-5L showed a significant association (r2=−0.382, p =0.004).
Furthermore, also correlations between the assessments used to determine the social situation and the HDRS-17 results were significant (Supplementary Table 1).
Performance of Single Items of the HDRS-17 for Diagnosis of Depression After Stroke
Lower rates of recalled out-patient screening in patients with prevalent depression might be attributed to regular screening using the standard tools is too time-consuming for general practitioners. Therefore, we aspired to exploratively test how a reduced version of the Hamilton depression scale using only two items in a dichotomous manner would perform compared to the full 17-item version of the Hamilton scale. When comparing single items of the HDRS-17 (dichotomized in healthy or pathological irrespective of the strength of the items) differences between depressed and non-depressed stroke patients (Figure 1) were highest for loss of interest in work and other activities (Item 7), feelings of guilt (Item 2) and depressive mood (Item 1) (Figure 1).
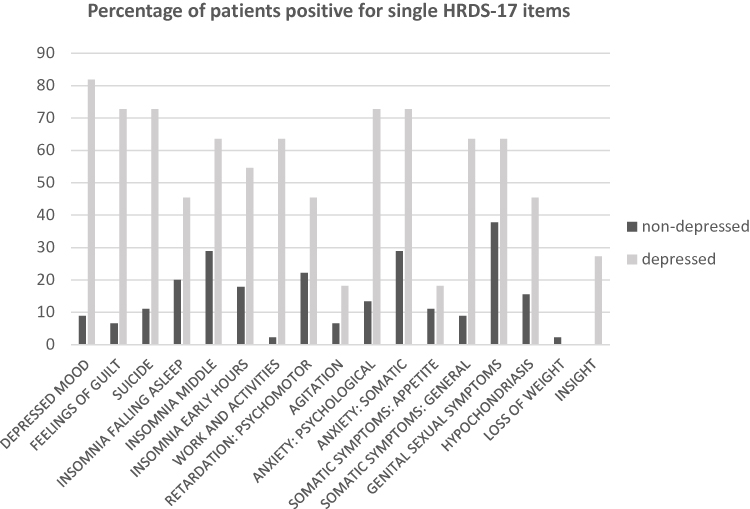 |
Figure 1 HDRS 17-items. Notes: Impairments in patients with and without post-stroke depression. Shown are the percentages of depressed vs non-depressed patients who are positive for the single items. |
Items 1 and 7 of the HDRS-17 also represent the two criteria that are necessary for a diagnosis of depression according to the DSM-5 (depressive mood/loss of interest or pleasure in work and other activities), so in a next step, we strove to see how these items would compare to the overall score with regard to sensitivity and specificity of detecting depression. For a combination of item 1 and item 7, the sensitivity for detecting depressed patients was at 100%. In other words, all patients who were diagnosed as depressed according to the 17-item version of the HDRS-17, could also be detected by a two-item screening. The specificity for using only two questions was 0.91 when compared with the overall HDRS-17 (Table 4).
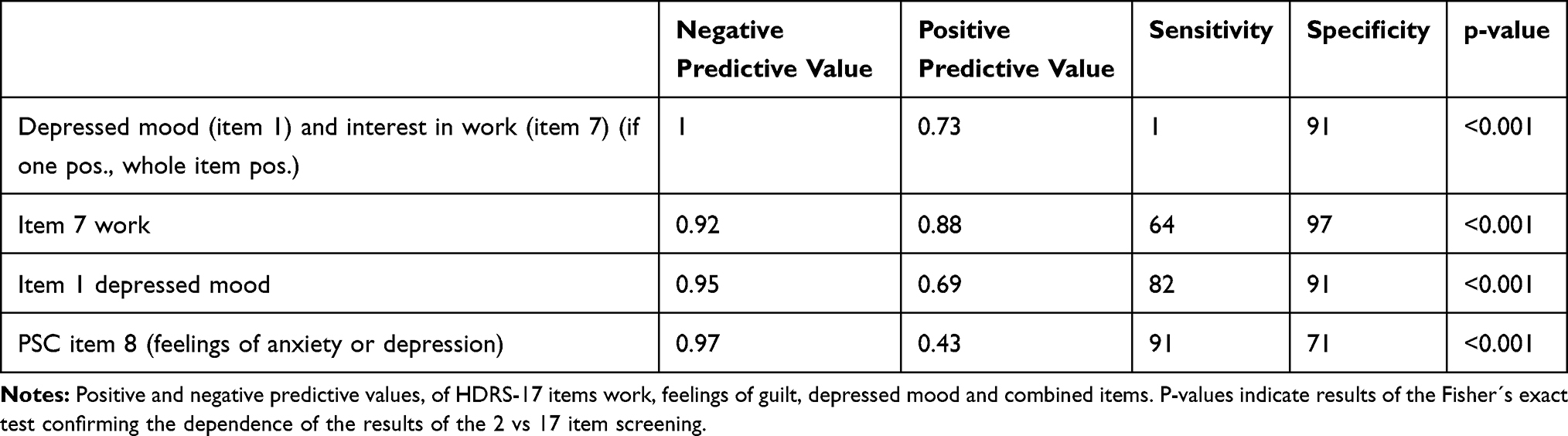 |
Table 4 Negative and Positive Predictive Value, Sensitivity and Specificity for a Combination of Two and Single Items in Detecting Depression |
For item 8 (asking about “feelings of anxiety and depression”) of the PSC, the sensitivity and specificity for detecting depression in comparison to the HDRS-17 was lower than for the two-item screenings (0.91 and 0.71, respectively). However, when comparing the single items, the sensitivity for detecting depression was highest for item 8 of the PSC (91%), compared to 82% and 64% of the single items 1 and 7 of the HDRS-17.
Among the single items of the HDRS-17 for which the strength of the rating also was highly correlated (Table 5) with overall score results, again were “interest in work and other activities” (Item 7 of the HDRS-17), depressive mood (Item 1) and their combination.
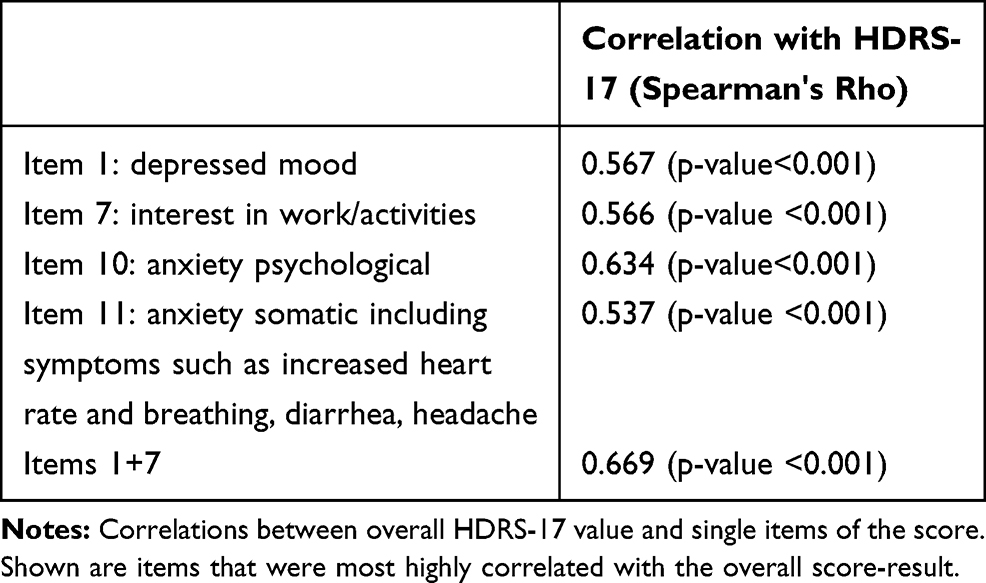 |
Table 5 Correlations Between Overall HDRS-17 Value and Ratings for Single Items of the Score |
Discussion
With low-recalled screening rates we observed a high rate of manifest depression 2 to 3 years after stroke onset. Patients with depression further reported experiencing a poor social situation and less emotional support, which might increase the risk for developing additional medical complications such as cardiovascular disease, metabolic syndrome or chronic pain.8 Furthermore, social counselling and application for benefits were recommended more frequently in patients with depression. The lower rate of recalled screening, the higher rates of expressed unmet need with regard to emotional problems and the undersupply of social care may indicate that in patients with depression social problems and emotional needs currently were not adequately addressed during aftercare for stroke. Since some of the patients who did not recall screening already had received prior anti-depressant medication mostly initiated during the hospital stay, a lack of adequate care in the out-patient setting could indicate that further treatment recommendations for patients with depression were not adequately followed up after the transfer to the out-patient setting. However, this remains speculative, since we had only limited information on the anti-depressant medication used and no information on the circumstances of prescription or whether and which recommendations for out-patient treatment were given specifically. Future studies should investigate this issue in more detail considering that anti-depressant drugs might also be prescribed prophylactically or for the treatment of post–stroke pain.12 Furthermore, response rates to anti-depressant treatment can change over time. Therefore, continuous screening for disease symptoms may be essential to improve out-patient treatment and adequately address emotional needs. Simplified screening methods for out-patient depression after stroke might support general practitioners to monitor the disease in a time-effective fashion. Our data suggest that loss of interest in work and other activities (Item 7 of the HDRS-17) in combination with depressed mood (Item 1) in our study displayed the same sensitivity as the 17-item HDRS-17 for detecting depression in our sample.
Previous work found two-question-screenings for depression to be similarly accurate as more extensive instruments13 and mail-delivered short versions to be similar to long versions of self-assessment tools (Beck depression inventory) after stroke.14 The Beck depression inventory (self-assessment) and the HDRS-17 (interviewer-based face to face assessment) moreover have been evaluated to be similarly useful in the detection of depression.15 Interviewer-based ratings and diagnoses, however, compares favorably to real-life situations when patients visit their general practitioner in out-patient aftercare. For this type of interview, studies confirming the efficiency of using reduced score versions of face-to-face assessments such as the HDRS-17 during the post-stroke aftercare have been lacking so far. Previous studies using a 9 item version of the Hamilton depression inventory indicate that these versions also displayed high internal consistency and test –retest reliability.16 However, they were never established in clinical routine. Other two-item versions of screening tools for depression such as the PHQ-2 have been tested successfully for depression but were not validated in stroke patients.9 Our small study was not powered for a detailed analysis of the precision of a two-item score. However, an exploratory comparison of the full versus the two-item version, data collected in our study indicated that using verbal screening including two items in a dichotomous manner in our study would have left no patient with depression undetected.
Limitations of our study include first of all the small size of our exploratory study. Due to this, we can only draw limited conclusions. Larger long-term studies following the intake and effects of antidepressant medication are needed to confirm our findings. However, the patients were well characterized with the exception that information on prior anti-depressant medication intake was only available for 34 of 57 and for nine of eleven patients that were classified as depressed according to the HDRS-17. Data collected in smaller studies can be prone to different forms of bias and data on screening in our study were self-reported and collected retrospectively. Therefore, we cannot exclude a recall bias with regard to the screening for depression. Such a bias may distort our results as patients with depression tend to have cognitive impairments as well.17 However, in our study, we did not see differences in people with and without depression with regard to cognitive impairment and results remained significant also after adjusting for confounding factors including cognition. Furthermore, although we offered transportation we cannot exclude a selection bias concerning patients unable to attend our study center.
Even though we controlled for a wide panel of potential confounders we did not control for stroke lesion. However, the type of lesion induced by the stroke may explain some of the variability associated with depression, but – especially since differences with regard to cognition did not seem to be an issue – is unlikely to affect recalled screening or the quality of medical support with regard to emotional problems. Therefore, the type of lesion should not confound our results with regard to the association between recalled screening and depression.
Due to the cross-sectional design of our study, we have only limited information on the status of depression and unmet need at stroke onset. Therefore, we cannot be certain whether the outcomes such as unmet need for support with emotional problems or lower social-support represent consequences of the depression or should be considered risk factors in the development of the disease. In any case, social loneliness has previously been reported to provide a link between depression and organic disease.8 Also, the fact that further socio-economic counselling and care in our study was recommended at significantly higher rates in patients with depression underlines the need for detection of depression in long-term stroke aftercare to identify vulnerable patients that may not be able to organize optimal care for themselves.
Finally, the results from the two-item screening are not independent from the overall results of the HDRS-17. Consequently, the high sensitivity rate for detecting depression using the two-item version of the HDRS-17 needs to be interpreted with great care.
In conclusion, we found that a minority of patients recalled to have been screened for post-stroke depression. In patients with depression a lower rate of recalled screening, a worse social situation and more unmet need with emotional problems were observed. Patients with post-stroke depression further were more often recommended to apply for social support and benefits, indicating that available resources were not being used to the extend they were needed to ensure optimal stroke aftercare. Undersupply of care in patients with post-stroke depression might induce a vicious circle increasing the risk for additional medical complications leading to increased mortality and disability.2,5 Results of our exploratory analysis further question whether using only two items of the HDRS-17 scale may be sufficient for detecting patients at risk for post-stroke depression when time does not allow for more detailed assessment of all patients. This finding could be important, since previous studies have demonstrated that unassisted judgments of general practitioners for depression in their patients lack sensitivity.18 Our findings warrant larger, prospective, multicenter studies exploring in more detail the effect of a better treatment and a more efficient screening for post-stroke depression in improving medical and social outcomes in the long-term course of stroke.
Ethics and Informed Consent
All participants provided written informed consent and the study received full ethics committee and data protection approval by the institutional review board of Charité – Universitätsmedizin Berlin (reference EA1/183/14), and was registered on clinicaltrials.gov (NCT02320994).
Data Sharing Statement
Data are available based upon reasonable request from the corresponding author and the PI of the MAS study: Andreas Meisel: [email protected] and Inken Padberg: [email protected].
Acknowledgments
We thank Susanne Zöllner for help with data acquisition within the MAS-1 study and Dike Remstedt for help with data acquisition as well as for critically reviewing the English language and the wording of the manuscript.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Fund of Charité – Universitätsmedizin Berlin. These sponsors had no involvement in any of the stages from study design to submission of the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hackett ML, Pickles K. Part I: frequency of depression after stroke: an updated systematic review and meta-analysis of observational studies. Int J Stroke. 2014;9(8):1017–1025. doi:10.1111/ijs.12357
2. Ayerbe L, Ayis S, Wolfe CDA, Rudd AG. Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis. Br J Psychiatry. 2013;202(1):14–21. doi:10.1192/bjp.bp.111.107664
3. Grenard JL, Munjas BA, Adams JL, et al. Depression and medication adherence in the treatment of chronic diseases in the united states: a meta-analysis. J Gen Intern Med. 2011;26(10):1175–1182. doi:10.1007/s11606-011-1704-y
4. Kronish IM, Edmondson D, Goldfinger JZ, Fei K, Horowitz CR. Post-traumatic stress disorder and adherence to medications in survivors of strokes and transient ischemic attacks. Stroke. 2012;43(8):2192–2197. doi:10.1161/STROKEAHA.112.655209
5. Ayerbe L, Ayis S, Crichton S, Wolfe CDA, Rudd AG. The long-term outcomes of depression up to 10 years after stroke; the South London Stroke Register. J Neurol Neurosurg Psychiatry. 2014;85(5):514–521. doi:10.1136/jnnp-2013-306448
6. Barra M, Evensen GSH, Valeberg BT. Cues and clues predicting presence of symptoms of depression in stroke survivors. J Clin Nurs. 2017;26(3–4):546–556. doi:10.1111/jocn.13482
7. Palmer R, Enderby P, Paterson G. Using computers to enable self-management of aphasia therapy exercises for word finding: the patient and carer perspective. Int J Lang Commun Disord. 2013;48(5):508–521. doi:10.1111/jlcd.2013.48.issue-5
8. Bica T, Castelló R, Toussaint LL, Montesó-Curto P. Depression as a risk factor of organic diseases: an international integrative review. J Nurs Scholarship. 2017;49(4):389–399. doi:10.1111/jnu.2017.49.issue-4
9. Towfighi A, Ovbiagele B, El Husseini N, et al. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2017;48(2):e30–e43. doi:10.1161/STR.0000000000000113
10. Guideline S-Gnt. Unipolar Depression, long version. AWMF-Register-Nr: nvl-005; Vol 2. 2015.
11. Hotter B, Padberg I, Liebenau A, et al. Identifying unmet needs in long-term stroke care using in-depth assessment and the post-stroke checklist – The Managing Aftercare for Stroke (MAS-I) study. Eur Stroke j. 2018;3(3):237–245. doi:10.1177/2396987318771174
12. Kumar B, Kalita J, Kumar G, Misra UK. Central poststroke pain: a review of pathophysiology and treatment. Anesthesia Analgesia. 2009;108(5):1645–1657. doi:10.1213/ane.0b013e31819d644c
13. Whooley MA, Avins AL, Miranda J, Browner WS. Case-finding instruments for depression: two questions are as good as many. J Gen Intern Med. 1997;12(7):439–445. doi:10.1046/j.1525-1497.1997.00076.x
14. Nolte CH, Müller-Nordhorn J, Jungehülsing GJ, et al. Zwei einfache Fragen zur Diagnose der Post-Schlaganfall Depression. Fortschr Neurol Psychiatr. 2006;74:251–256. doi:10.1055/s-2005-919144
15. Berg A, Lönnqvist J, Palomäki H, Kaste M. Assessment of depression after stroke. Comparison Different Screening Instrum. 2009;40(2):523–529.
16. William R, Kobak K. Reliability and validity of the hamilton depression inventory: a paper-and-pencil version of the hamilton depression rating scale clinical interview. Psychol Assess. 1995;7:472–483. doi:10.1037/1040-3590.7.4.472
17. Zuckerman H, Pan Z, Park C, et al. Recognition and treatment of cognitive dysfunction in major depressive disorder. Front Psychiatry. 2018;9:655. doi:10.3389/fpsyt.2018.00655
18. Carey M, Jones K, Meadows G, et al. Accuracy of general practitioner unassisted detection of depression. Aust N Z J Psychiatry. 2014;48(6):571–578. doi:10.1177/0004867413520047
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.