")
Back to Journals » Open Access Journal of Contraception » Volume 13
Unmet Need for Family Planning Service and Associated Factors Among Homeless Women of Reproductive Age Group in Jimma Zone Administrative Towns, Ethiopia
Authors Terefe G , Abebe F , Teka B
Received 2 March 2022
Accepted for publication 31 May 2022
Published 8 June 2022 Volume 2022:13 Pages 83—93
DOI https://doi.org/10.2147/OAJC.S363258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Gemechu Terefe,1 Fikadu Abebe,1 Bekelu Teka2
1Department of Midwifery, Jimma University, Jimma Town, Oromia, Ethiopia; 2Department of Population and Family Health, Jimma University, Jimma Town, Oromia, Ethiopia
Correspondence: Gemechu Terefe, Email [email protected]
Background: The majority of homeless women (75%) do not wish to have or delay a pregnancy during this difficult time, yet many do not use contraception in developing countries. In Ethiopia, there is limited evidence of unmet need for family planning in settings where homelessness is on the increase. This study aims to assess the unmet need for family planning services among homeless women and identify associated factors in Jimma Town, southwestern, Ethiopia.
Methods: A community-based cross-sectional study was conducted on May 3rd and 4th, 2021. The complete enumeration was done to include 206 homeless women. Epidata version 3.1 data entry and exported to SPSS version 20 were used for analysis. Bivariate and multivariable logistic regressions were used to identify factors associated with the unmet need for family planning. Associated factors were determined by a 95% confidence interval of AOR and P-value < 0.05 in the multivariable model.
Results: The unmet need for family planning among homeless women was 47.3% [95% CI (38.2, 49.7)]. Being with a disability; [(AOR: 4.10, 95% CI (1.73– 9.56), visited by a health care provider in the last 12 months; [(AOR: 0.25, CI (0.09– 0.65)], and a number of living children; [(AOR: 0.42, CI (0.18– 96)] were significantly associated with an unmet need for family planning.
Conclusion: The unmet need for family planning methods among homeless women was high compared to the national standard of unmet need for family planning, being with a physical disability, visited by a health care provider in the last twelve months, and having a number of living children contributed to the unmet need for family planning. Therefore, health care professionals should focus on providing health education on family planning among these women at the grass-root level to reduce the unmet need for family planning among these women.
Keywords: unmet need, contraceptive use, reproductive-age women, homeless, Jimma, Ethiopia
Introduction
The unmet need for family planning is for those women who are fecund, sexually active, or not using any method of contraception to report what they want to limit.1 This unmet need for family planning was identified between reproductive intentions and birth control methods.2,3 Homeless reproductive age group women have an unmet need for family planning for birth spacing, ie they are at risk of not using contraception and do not want to get pregnant within the next two years. Whereas there is an unmet need for birth limiting if women are at risk of becoming pregnant, do not use contraception, and want no more children, pregnant with an unwanted pregnancy.1,4
Reproductive age group women who use family planning services face significant health and social challenges in their communities around the world. In 2019, approximately 842 million women in the reproductive age group who required family planning services used a modern contraceptive method, out of a total of 1.11 billion women in the reproductive age group, while 270 million women still had an unmet need for family planning methods.5 This unmet need for family planning services is worse in the developing world, where over 232 million women cannot access a modern contraceptive method when needed.6 According to the report of the Ethiopia demographic health survey of 2016, the total unmet need for modern contraceptive methods was 36% in Ethiopia.4
In the homeless reproductive age group, women are ever prone to significant health risks and complications during pregnancy than women who live in stable households. As a result, they are more susceptible to pregnancy-related complications, such as antepartum hemorrhage, postpartum hemorrhage, preeclampsia, eclampsia, intrauterine fetal death, and death, among others.7,8 These reproductive age groups of women are particularly vulnerable to risky sex and rape due to their living conditions. Also, they face a higher number of reproductive health-related problems, traumas, unplanned pregnancies, miscarriages, and abortions than their other peers. Over 50% of homeless women had a history of unwanted pregnancy.9,10 Besides, homeless women are more likely to become pregnant and far more likely to experience multiple pregnancies than other women.7,11,12
A study conducted in Los Angeles among homeless women showed that 73% of these women had an unintended pregnancy. Moreover, the non-use of contraceptives method was high among such women.13 According to a study conducted in Ethiopia, half of the homeless women had a history of unwanted pregnancies and experience numerous challenges in obtaining maternal health care services.14
To the best of my knowledge, there has never been a study on the unmet need for family planning services among homeless women in Ethiopia, so this study was aimed to assess the unmet need for family planning services and associated factors among homeless reproductive age group women in Jimma zone administrative towns, Ethiopia.
Methods
Study Setting and Period
A community-based cross-sectional study was conducted among women of the reproductive age group on May 3rd and 4th, 2021 in Jimma zone administrative towns on May 3rd and 4th, 2021. Jimma town is one of the zones of Oromia regional state located in the southwest of Ethiopia, which is located 356 Kilometers away from Addis Ababa, the capital city of Ethiopia. In the Jimma zone, there are two administrative towns named “Jimma” and “Agaro’. All homeless women in the reproductive age groups (15–49 years of age) in Jimma zone administrative towns were the source of population and all homeless reproductive age group women in Jimma zone administrative towns who fulfilled the selection criteria and were willing to participate in were the study population.
The sample size was determined using a single population proportion formula with the assumption prevalence of unmet need (p=0.41, from the previous study), 95% CI (Ζ1−α/2)=1.96), 5% degree of marginal error (d), finite population correction formula (because the total number of homeless women in the town were less than 10,000 that the sample size become 154). After the sample size was calculated, a complete enumeration of homeless reproductive age women by census sampling was done, and a total of 225 homeless were found in Jimma zone administrative towns. Among these 6 reproductive women had communication problems and 15 reproductive women were not available during the interview. After the exclusion of all these homeless women, 206 reproductive age group women were finally included in the study.
Data Collection Measurement and Procedure
A semi-structured interview administered questionnaire, which was adapted and developed from relevant literature,15–17 was used to collect data. The questionnaire was primarily developed in the English language and then translated to local languages Afan Oromo and Amharic versions for consistency. It comprises four parts: background of respondents, reproductive characteristics, knowledge-related factors, and the unmet need and current use of contraceptives. Data was collected by fifteen diploma nurses and was supervised by four BSc nurses by accessing the homeless women by using field guider. Therefore, data were collected after the census of homeless women is demarcated sites in all kebeles of the two administrative towns. The demarcated sites in each kebele include main roadsides, isolated slum areas (bridge sides), around taxi/bus stations, traffic lights sides, road junctions, churches and/or mosques, and streets where homeless women usually live or sleep. To assure the quality of the data, the principal investigator gave training to the data collectors and supervisors for one day. The supervisors and investigators checked the filled questionnaires daily. Also, data collectors asked the study participants if they were interviewed on a similar matter to reduce redundancy. The questionnaire was pretested on 5% of homeless women in Bedele town and some modifications were made based on the finding of the pretest result such as any ambiguity, incompleteness, or other problems being addressed immediately.
Study Variables
Dependent Variable
Unmet need for family planning methods.
Independent Variables
Socio-demographic, reproductive, and service provision-related variables.
Operational Definitions
Unmet need for family planning Refers to the number or percent of women who are fecund and sexually active but are not using any method of contraception, and report not wanting any more children or wanting to delay the next child.18
The unmet need for limiting is the number or percentage of women who desire no additional children and who do not currently use a contraceptive method.
Unmet need for spacing: is the number or percentage of women who desire to postpone their next birth by a specified length of time (for example, for at least two years from the date of a survey) and who do not currently use a contraceptive method.
Homeless: For this study, women who lived on the street sides, in shelters, and religious areas use as a usual living place at least for a week, were homeless.
Homeless women who live on the street: The respondents who use their nighttime sleep there under the compound of different institutions, verandas, near the bus station, on-street are categorized as on street.
Homeless women who live off the street: According to this study, nighttime sleep in a shelter was considered an off-street.
Knowledge of contraceptives: Knowledge about family planning was measured by using three knowledge questions to construct a composite score. The first three questions have multiple responses and add each response from no answer to answering all options. The rest of the questions are based on Yes and No by giving 1 to Yes and 0 to No. Based on the summation score, ≥60% from knowledge measuring questions were considered as having good knowledge, whereas those who scored less than 60% were considered as having poor knowledge.
Data Management and Analysis Procedure
Following the data collection, data were rechecked for completeness and were entered into Epidata 3.1 version prepared templates and then exported to SPSS statistical software version 21. Descriptive analysis was used to summarize the characteristics of study participants. Bivariate logistic regression analysis was done to select candidate variables for multivariate logistic regression analysis. Variables with a p-value less than 0.25 in the bivariate analysis were considered as candidates to be entered into the final model. Hosmer and Lemeshow’s test was used to determine the model fitness, and independent variables were checked for multicollinearity with no variable dropped from the analysis. Finally, the association was declared with a p-value less than 0.05 with an adjusted odds ratio (AOR) at a 95% confidence interval.
Results
Descriptions of the Study Participants
A total of 206 participants were included in the study, having a 91.5% response rate.
The study participants were between 16 and 49 years of age with a mean age of 27 and a standard deviation of 6.2 years of age. By the age group, 57 (27.7%) of the study participants were between the ages of 25–29 years old. The respondents were predominantly Orthodox by followers of their religion that is 100 (48.5%) and Oromo by ethnic group, ie 107 (51.9%). One hundred and thirty-eight (67.0%) study participants did not join formal education, while 75 (36.4%) of study participants were unmarried. Regarding the income of the respondents, 149 (72.3%) had less than 500 ETB average monthly income. Nearly one-third (27.7%) of the respondents were using their nighttime sleeping in shelters made under the compound of different institutions’ (Table 1).
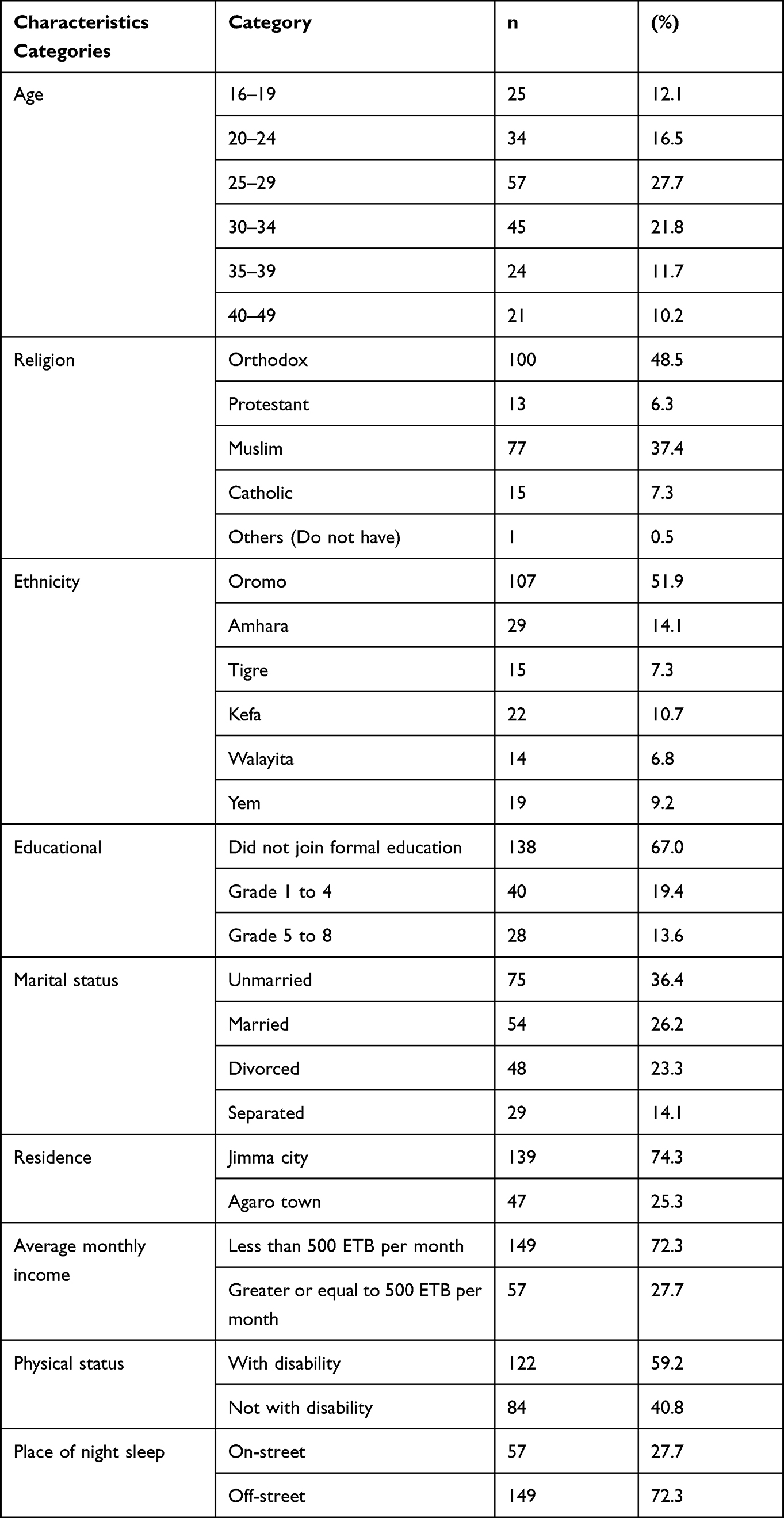 |
Table 1 Sociodemographic Characteristics of Homeless Women of Jimma Zone Administrative Towns, Ethiopia, 2021 |
Reproductive Health Characteristics
Seventy-seven (37.4%) of homeless women had a history of sexual assault, which was a non-consensual sexual act against their will in their life, while 97 (47.1%) of the respondents had first sexual intercourse before the age of eighteen years old. Three-fourth (75.2%) of homeless women had a history of pregnancy, from this about 103 (50%) had less than four number of pregnancies. More than half of the study participants had a history of pregnancy after they became homeless. The main reason for becoming pregnant was not using the contraceptive methods (50.5%) as they mentioned. Fifty-eight (37.4%) of respondents have a history of abortion during their homeless life (Table 2). The main reason for homeless women desiring more children is because they have few children as mentioned by 39.5% (Figure 1).
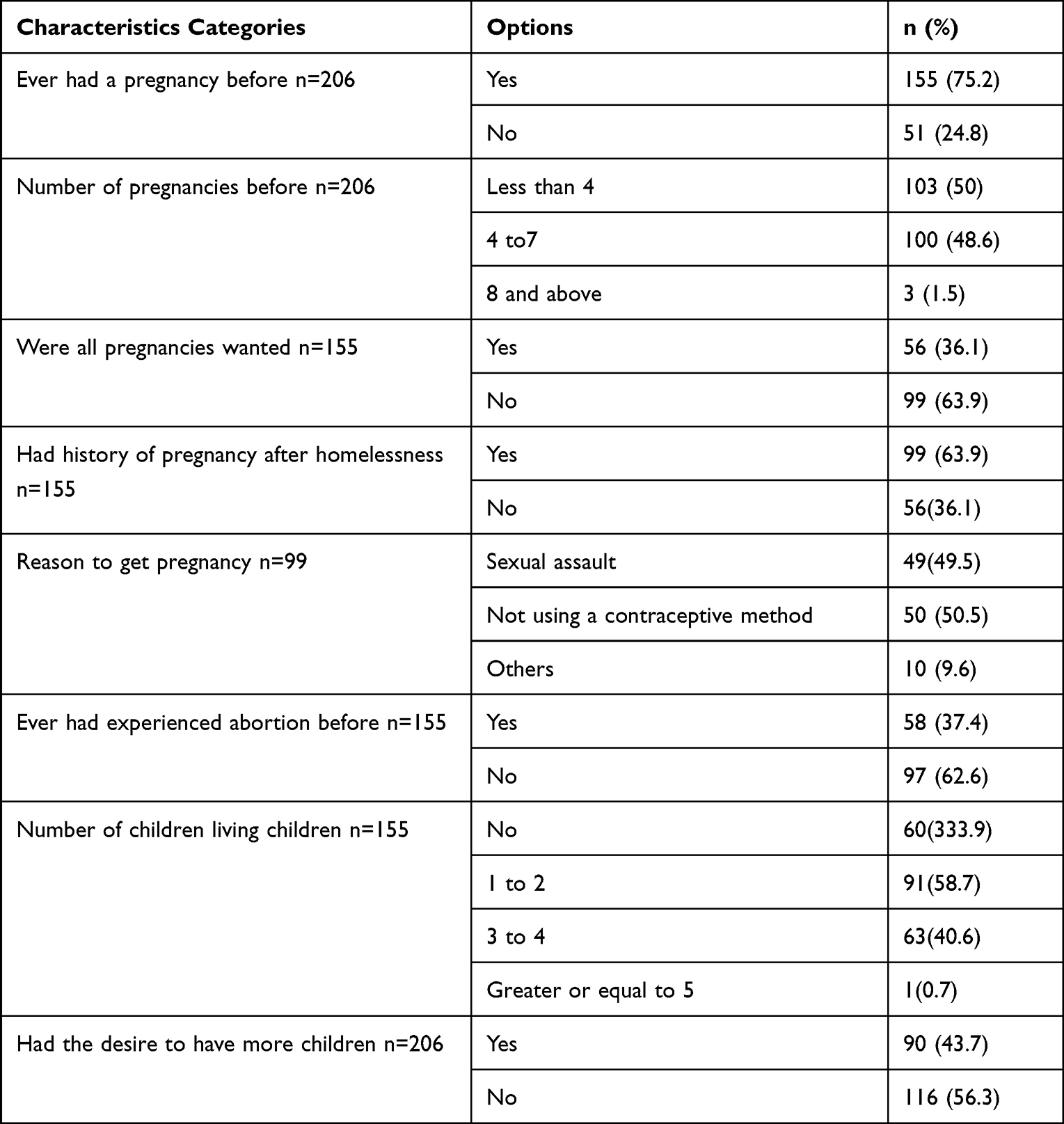 |
Table 2 Reproductive Health-Related Characteristics of Homeless Women of Jimma Zone Administrative Towns, Ethiopia, 2021 |
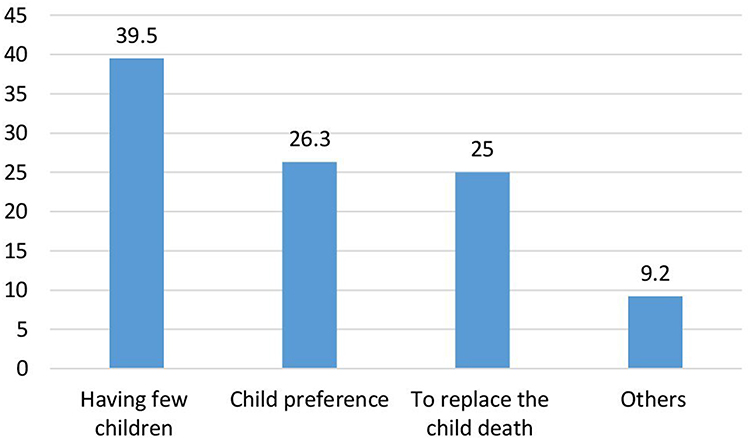 |
Figure 1 A reason to desire additional children among homeless women in Jimma zone adminstrative Towns, Ethiopia 2021. |
Knowledge of Family Planning-Related Factors
Regarding the knowledge of homeless women about family planning services, 13% of the study, participants had good knowledge, while (87%) had poor knowledge of contraceptive methods.
Current Contraceptive Use Pattern of the Study
Eighty-five (41.2%) of respondents have been using family planning methods. Of those users, 54 (26.2%) respondents have used birth spacing, and 31 (15.0%) used birth limiting. Their main reason for not using contraceptives was difficulty getting family planning services (Figure 2).
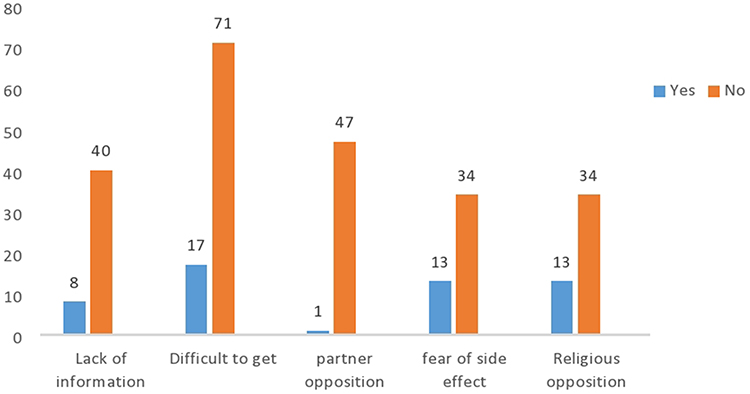 |
Figure 2 Reasons for not using family planning methods among homeless women in Jimma zone administrative towns, Ethiopia, 2021. |
Unmet Need for Family Planning Methods Among Homeless Women Contraceptive Methods
The unmet need for family planning methods was found to be 97 (47.1%) [95% CI (38.2, 49.7)], with 80 (38.8%) and 17 (8.3%) for spacing and limiting, respectively. If all homeless women in this study area who have an unmet need for family planning for spacing and limiting the use of family planning methods, the prevalence of family planning would rise from 41.5% to 46.7%. (Figure 3).
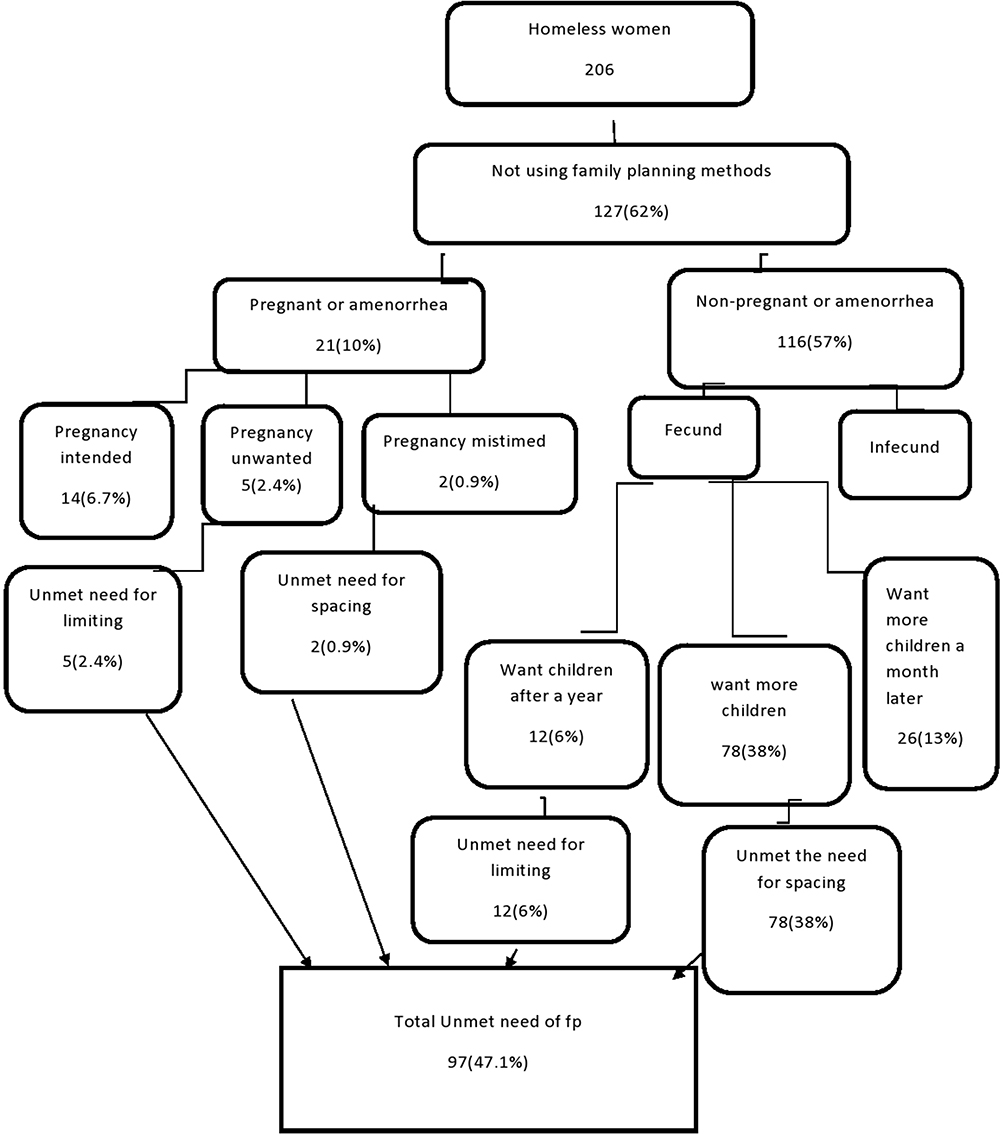 |
Figure 3 Unmet need for family planning among homeless women in Jimma zone administrative towns, Ethiopia, 2021. |
Factors Associated with Unmet Need for Family Planning Methods Among Homeless Women
A multivariable logistic regression analysis Physical status, visited by health care providers in the last twelve months, and the number of living children was predictors of unmet need for family planning among homeless women.
According to the finding, homeless women who were with physical disabilities were four times more likely to have an unmet need for family planning methods as compared with their counterparts [(AOR: 4.10, 95% CI (1.73–9.59)].
Homeless women who were visited by health care providers in the last twelve months were 75% less likely to have an unmet need for family planning methods than those who were visited [(AOR: 0.25, CI (0.09–0.65)].
Lastly, the number of living children was reversely associated with the unmet need for family planning among homeless women. Homeless women who had one or two living children were 68% less likely to have an unmet need for family planning methods compared to those who had three or more [(AOR=0.42, 95% CI: 0.18–0.96)] (Table 3).
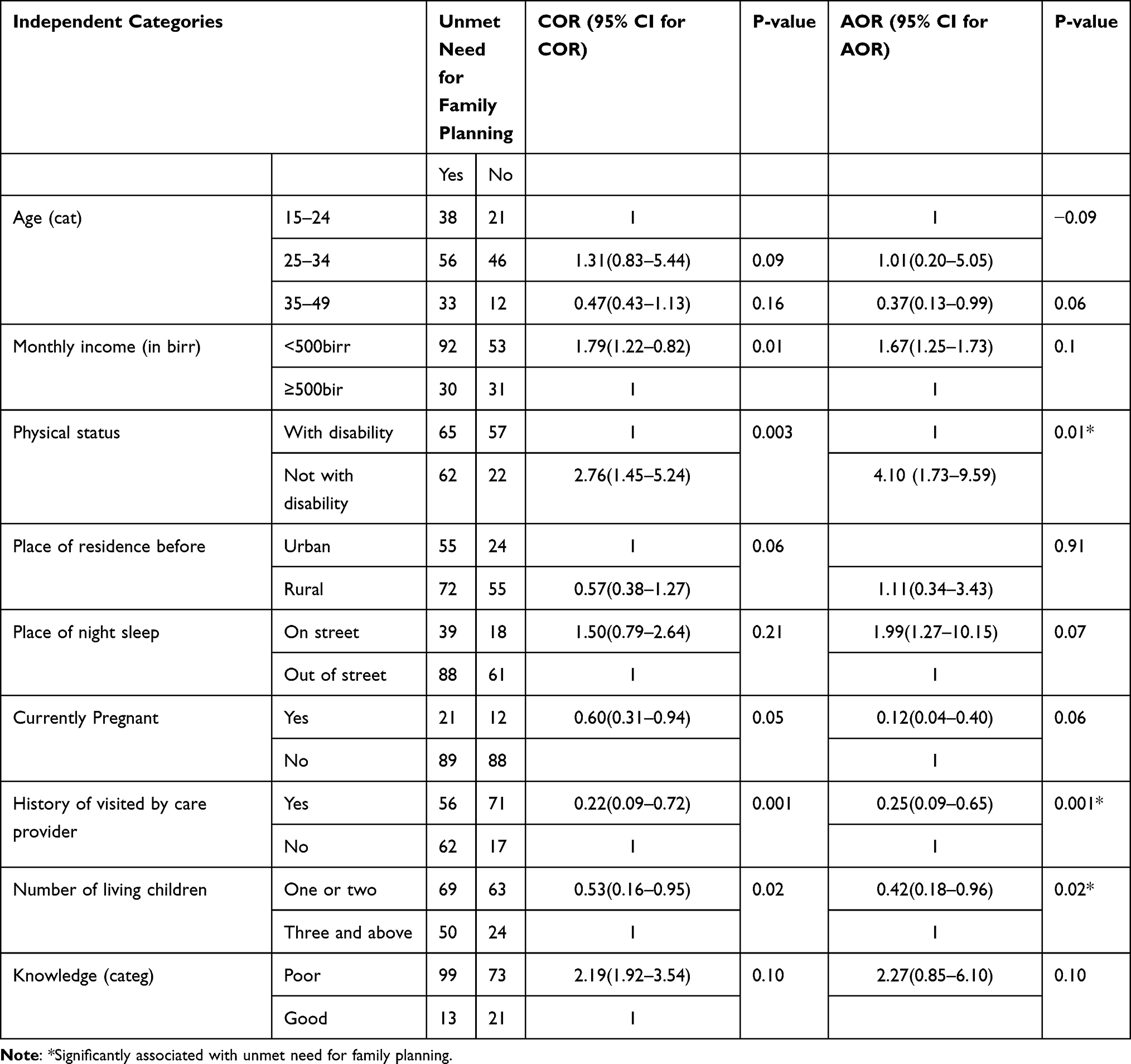 |
Table 3 A Multiple Logistic Regression on Associated Factors of Unmet Need of Family Planning of Jimma Zone Administrative Towns, Ethiopia, 2021 |
Discussion
According to this study, the prevalence of unmet need for family planning among homeless women was found to be (47.1%) [95% CI (38.2, 49.7)]. The unmet need among homeless women is higher than the national unmet need (22%) of EDHS 2016.10 The discrepancy might be due to homeless women facing several life challenges regarding service provision, nighttime residence, socio-economic status, and educational status. This shows that these women need special attention for family planning services to prevent further perpetuating health risks.
In this study, physical status, history of visits by a health care provider, and the number of living children were found to be significantly associated with an unmet need for family planning among homeless women of reproductive age group. The status of being with a physical disability was four times more likely to have an unmet need for family planning than their counterparts. Even though the study included both participants with and without physical disabilities; the existing difference could be those. There is a global concern about the participation of disabled persons in national development. Poverty, discrimination, and stigma are the major socio-economic problems faced by persons with physical disabilities; this might include family planning services. The reproductive health problems faced by women with disabilities include sexual exploitation, unwanted pregnancy, and complications during childbirth unmet need compared with women with no disability. Because of the above life challenges, women with a disability may have more unmet needs than others. Reducing the unmet need would deliberately reduce unintended pregnancies, abortions, and maternal and child deaths.
In the study, homeless women who were visited by a health care provider in the last twelve months were 75% less likely to have unmet the need for family planning services as compared to women who were not visited. The possible explanation is that one of the service delivery packages in the urban health extension program of Ethiopia is home to home or outreach services. Using this modality, the health extension provides health education and behavior change communication related to family planning and other packages of services. According to the finding of this study, homeless women are still less accessible to family planning services. In this study, homeless women who had one or two living children were 0.42 times higher at having an unmet need for family planning methods than whom those had more than three or more living children. This is consistent with a study conducted in the Damot district of Ethiopia.19 The number of living children determines the odds of using contraception in this study, and similar associations were found in the DHS of other countries.19–21 Having children living between 1 and 2 had lower odds, and the odds increased in women having children three and above. This shows that as the number of children increased, the multiparous women might have had an idea about the family planning ser at all, or sex preference might be there in some women.22
Strength and Limitation of the Study
Strength
This study has focused on a marginalized group of people who are highly vulnerable to unintended pregnancy due to the lack of the contraceptive method where adequate information and studies are lacking. This might certainly serve as baseline information and fill some of the knowledge gaps for further studies.
Limitation
The study missed qualitative data and did not assess the contribution of health service-related factors. Studying it is still not free from social desirability and recall biases. One limitation of the study is to compare this study's findings with other studies.
The Implication of the Study
The outcomes of this study will help policymakers develop evidence-based public health programs to prevent unwanted and unexpected pregnancies among homeless women by increasing contraceptive use. In contrast to past studies on their counterparts, the unmet need for family planning was identified among homeless women in this study. The results of this study will be valuable in planning and delivering family planning services to homeless women.
Conclusion
Despite many efforts being made to reduce the unmet need for family planning was high compared to the national standard of unmet need for family planning. It was very far from the national target to reduce the unmet need for family planning to 10% by the end of 2020. The identified factors that were significantly associated with the unmet need for family planning among homeless women were being with a physical disability, a history of visits with a health care provider in the last twelve months, and a number of living children. Therefore, health professionals should have health information and health education for homeless women to promote the right time for using family planning.
Abbreviations
DHS, Demographic and Health Survey; EDHS, Ethiopian Demographic and Health Survey; ETB, Ethiopian Birr; FP, family planning; IUD, intrauterine devices; SNNP, Southern Nation and Nationalities Peoples; SPSS, Statistical Package of Social Science; STI, sexually transmitted disease; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon request from the corresponding author.
Ethics Approval and Consent to Participate
Ethical clearance for conduct was obtained by Jimma University Institute of Health's Institutional Review Board. At the initial stage of data collection, informed oral and written consent was taken from homeless women whose participation was voluntary, and they had the right to withdraw at any time from the study by protecting their health, confidentiality and rights. Written consent and assent from the guardian for those under eighteen were taken from the study participants after a detailed explanation of the aim of the study before data collection. There is no human rights violation, and our study complies with the Declaration of Helsinki.
Acknowledgments
We are impressively thankful to Jimma University for the financial support provided for the work of this paper. We are also grateful to study participants and data collectors, in particular for their cooperation and the information they provide. Last but not least, appreciation goes to colleagues and friends for their encouragement and support for the work of this paper.
Author Contributions
All authors equally contributed to this work beginning from the conception, study design, execution, acquisition of data, analysis, and interpretation. Authors of this work took part in the drafting, revising, and/or critically reviewing of the article and finally agreed on the journal to which the article was submitted. All authors also reviewed and agreed on all versions of the article before submission, during revision, and agreed to be accountable for all aspects of the work.
Funding
This study was funded by Jimma University, Ethiopia, and the funder had no interference with the conduction, analysis, and publication process.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Unies N. World contraceptive use 2009 POP/DB/CP/Rev2009; 2009:1–4.
2. Bawah AA, Assuming P, Achana SF, Kanmiki EW, Awoonor-Williams JK, Phillips JF. Contraceptive use intentions and unmet need for family planning among reproductive-aged women in the Upper East Region of Ghana. Reprod Health. 2019;16:1–9. doi:10.1186/s12978-019-0693-x
3. Casterline JB, Sinding SW. implications for population policy unmet need for family countries and implications for population policy John B. Casterline. 2000;26135.
4. Ethiopian demographic health survey; 2016.
5. Dorling D. World Population Prospects; 2019.
6. Nations U, Affairs S. World Fertility and Family Planning; 2020.
7. Dahlem G. Women experiencing homelessness in Michigan. Common Problems and Strategies to Help; 2021.
8. Ensor T, Cooper S Overcoming barriers to health service access and influencing the demand side through purchasing; 2004.
9. Valenzuela-garcia H, Molina L, Lubbers MJ, Grau J. The relational vulnerability of people experiencing multiple exclusion homelessness (MEH) in Spain. Int J Environ Res Public Health. 2021;18(19):10275. doi:10.3390/ijerph181910275
10. Manuscript A. NIH public access; 2011.
11. Corey E, Frazin S, Heywood S, Haider S. Desire for and barriers to obtaining effective contraception among women experiencing homelessness. Contracept Reprod Med. 2020;5(1):1–7. doi:10.1186/s40834-020-00113-w
12. Gebreyesus H, Mamo A, Teweldemedhin M, Gidey B, Hdush Z. Experiences of homeless women on maternity health service utilization and associated challenge in Aksum town. BMC Heal Serv J. 2019;3:1.
13. Guta A, Amsalu B, Weldamanuel T, Sema A, Abera L. Utilization of modern contraceptives and associated factors among street women in Dire Dawa, Eastern Ethiopia: a mixed study. AIDS Care. 2021;1–12. doi:10.1080/09540121.2021.2014780
14. Note B. Situation and access to services of homeless children and adults in addis ababa briefing note; 2019.
15. Gebrecherkos K, Gebremariam B, Gebeyehu A, Siyum H, Kahsay G, Abay M. Unmet need for modern contraception and associated factors among reproductive age group women in Eritrean refugee camps, Tigray, north Ethiopia: a cross-sectional study 11 medical and health sciences 1117 public health and health services 11 medical and H. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-018-3956-7
16. Kalayu I. Unmet need for family planning and associated factors among married women in Asebot Town, West Hararge Zone, Oromia Regional State, Ethiopia, cross-sectional study design, 2018. Glob J Reprod Med. 2019;6(5):111–117.
17. Tessema AL, Bishaw MA, Bunare TS. Assessment of the magnitude and associated factors of unmet need for family planning among women of reproductive age group with disabilities in Bahir Dar City, Amhara Region, North West Ethiopia. Open J Epidemiol. 2015;05(01):51–58. doi:10.4236/ojepi.2015.51007
18. World health organization. Unmet need for family planning; 2015. Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3414.
19. Wolde A, Haile D, Anjulo U, Wolde J. Unmet need for modern contraceptive methods and associated factors among currently married women in Damot Woyde District, SNNPR, Ethiopia, 2019. Open Access J Contracept. 2020;11:17785. doi:10.2147/OAJC.S284129
20. Osmani KA, Reyer A, Osmani AK, Reyer JA, Osmani AR, Hamajima N. Factors influencing contraceptive use among women in Afghanistan: secondary analysis of Afghanistan. Nagoya J Med Sci. 2015;77(4):551–561.
21. Palamuleni ME. Socio-economic and demographic factors affecting contraceptive use in Malawi. African J of Repro Health. 2013;17(3):91.
22. Narzary PK, Sharma SM. daughter preference and contraceptive-use in matrilineal tribal societies in Meghalaya, India. Health Population Nutr. 2013;31(2):278–289.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.