")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Unintended Pregnancy and Associated Factors Among HIV Positive Women in Ilu Aba Bora zone, South Western Ethiopia: A Facility-Based Cross-Sectional Study
Authors Teklu T , Belina S , Chemir F , Tessema M , Yismaw W
Received 23 October 2020
Accepted for publication 14 January 2021
Published 16 February 2021 Volume 2021:13 Pages 197—203
DOI https://doi.org/10.2147/HIV.S288373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Tigist Teklu,1 Sena Belina,2 Fantaye Chemir,2 Martha Tessema,2 Worke Yismaw1
1Nursing Department, Mettu University, Mettu, Oromia, Ethiopia; 2Institute of Health, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Tigist Teklu
Department of Nursing, Mettu University Public Health and Medical Science Faculty, Mettu, Oromia, Ethiopia
Tel +25910091307
Email [email protected]
Background: Unintended pregnancy reflects the existence of unprotected sex. Understanding factors associated with unintended pregnancy among HIV-positive women is very important to design strategies for the prevention of further transmission and infection with the virus. However, there is scarce information in this regard. Given the degree of HIV prevalence among women and the current antiretroviral therapy scale up in Ethiopia, it is important to understand factors associated with un-intended pregnancy in order to prevent mother to child HIV transmission (MTCT).
Methods: An institution-based cross-sectional study design was employed. The sample size was 353; all HIV/AIDS sero-positive reproductive age group (15– 49) women having any pregnancy history after their diagnosis and having started HAART were included and simple random sampling was used to select study participants. Data collection period was from March 9 to April 13, 2019.
Results: The prevalence of unintended pregnancy among the participants was 40.9%. In the multivariate logistic regression, unemployment (AOR, 3.36; 95% CI: 1.55– 7.26), not being knowledgeable on MTCT and prevention of MTCT (PMTCT) (AOR, 3.18; 95% CI: 1.92– 5.24), and having had no discussion on reproductive health issues (AOR, 1.83; 95% CI: 1.09– 3.07) are factors significantly associated with unintended pregnancy occurrence among HIV-positive women on antiretroviral therapy.
Conclusion and Recommendation: The prevalence of unintended pregnancy among the women in the study is high. To avoid unintended pregnancies, HIV-infected women need access to effective family planning services and risk reduction discussions during routine care visits.
Keywords: unintended pregnancy, women on ART, Ilu Aba Bora zone, Southwest Ethiopia
Introduction
Unintended pregnancy is a pregnancy that is reported to have been either unwanted (i.e., it occurred when no children or no more children were desired) or mistimed (i.e., it occurred earlier than desired).1 HIV preserves both biological as well as behavioral effects on fertility issues among people living with the virus. HIV-positive pregnancies are associated with a high maternal mortality rate that is ten-fold higher than that of HIV-negative women and there were an estimated 56,100 HIV-related maternal deaths, accounting for approximately 20% of maternal deaths globally.2,3 Sub-Saharan Africa records the highest incidence of HIV as well as unplanned pregnancies. Approximately 20–40% of the total number of pregnancies which occur in sub-Saharan Africa are estimated to be unplanned and 20–35% of women are also estimated to have an unmet need for contraception.3,4
Unintended pregnancy can cause serious health, social, and economic consequences for women, families, and communities. It is linked with late entry into prenatal care as well as low birth weight babies and poor maternal nutrition.5 In addition to a higher risk of morbidity and mortality, unplanned pregnancies have been associated with other adverse economic, physical and social effects.6,7 To effectively plan family planning interventions related to HIV care and prevention of mother to child HIV transmission (PMTCT), there is a need for information on the prevalence of unintended pregnancy and its associated factors among HIV-infected women. So, the aim of this study was to assess the magnitude and associated factors of unintended pregnancy among HIV-positive women on HAART in order to give an input in the process of preventing new HIV infection and making conception safer. Pregnancies that are mistimed or unwanted can lead to adverse outcomes for both the mother and her newborn. Identifying the risk factors associated with unintended pregnancy can help with developing effective policy changes and interventions to minimize the odds of experiencing an unintended pregnancy and its associated consequences.
This is one of the studies exploring occurrence of unintended pregnancy under ART treatment units. Thus, it gives insight on preventing unintended pregnancy among HIV-positive women. Hence, it should fill a gap in wide-ranging HIV prevention and care programs; it can help HIV-positive individuals, policymakers and healthcare providers to develop their programs for safer, supportive pregnancy and family planning for HIV-positive individuals in their communities and it will be a resource for further studies to be used by researchers. So, the aim of this study to assess the prevalence and factors affecting unintended pregnancy among HIV-positive women in Ilu Ababora zone, south-western Ethiopia.
Methods
Study Design and Setting
A facility based cross-sectional study design was employed. Ilu Ababora is one of the zones of the Oromia regional state. Based on the 2012 Census conducted by the CSA, this zone has a total population of 1, 271,609, of whom 636,986 are men and 634,623 women. Mettu is the capital city of the zone and is 600 km away from Addis Ababa. The study was conducted from March 9 to April 13,2019.
Study Participants
All sampled HIV sero-positive reproductive age group (15–49) women having any pregnancy history after their diagnosis and attending ART follow up clinics at public health facilities of Ilu Aba Bora zone and visiting selected health facilities for ART service during the data collection period.
Sample Size Determination and Sampling Technique
The sample size was determined by the single population proportion formula by considering 46% to be the proportion of unintended pregnancy among HIV-infected women after their diagnosis in Addis Ababa8 with a marginal error of 5% between the sample and the population at 95% confidence level, which was 353. Purposive random sampling was used for the qualitative study sample while saturation of information was the criteria for saturation of information; those who participated in the quantitative study were not included in the qualitative study.
Eligibility Criteria
All HIV/AIDS sero-positive reproductive age group (15–49) women having any pregnancy history after their diagnosis and having started HAART.
Data Collection Procedure and Tool
A structured questionnaire for this study was adapted based on instruments that were used in other related and published studies in Ethiopia.8,9 The tool has five parts: part I – Socio-demographic and economic data; part II – information on family planning use; part III – HIV diagnosis, ART treatment condition and knowledge of MTCT and PMTCT; part IV – reproductive characteristics; and part V – sexuality and reproductive health information. Before going to data collection, a pre-test was conducted in Bedele hospital on 5% of the final sample (18 women fulfilling the inclusion criteria) to ensure the validity of the survey tool. The questionnaire was filled by ten diploma female nurses working out of ART clinics. One day of training was given for data collectors and supervisors while the overall data collection process was followed and controlled by the principal investigator. The questionnaire was translated to Afan-Oromo and Amharic by language experts and then translated back to English to check for consistency by an independent language expert.
Measurements
Unintended pregnancy: a pregnancy reported by a woman as mistimed or unwanted.8
MTCT knowledge: If the client gets a score at the mean or above then they will be categorized as knowledgeable, and as not knowledgeable if they get a score below the mean.10
PMTCT knowledge: If the client gets a score below the mean then they will be categorized as not knowledgeable, and as knowledgeable if they score at the mean and above.10
Data Analysis
The data were entered using EPI data version3.4.3statistical software and analyzed using SPSS version 21 statistical package. Descriptive statistics such as percentage, mean, cross tabulation, tables, and graphs were used to describe the data. Variables with P-value of less than 0.25 in binary logistic regression analysis were entered into the multivariate logistic regression analysis.
Results
Socio-Demographic Characteristics
Altogether 347 women participated in the study giving a response rate of 98.2%. The majority of the respondents, 30% were in the age group of 25–29 and the mean age was 30.6 ± 5.8 years (Table 1).
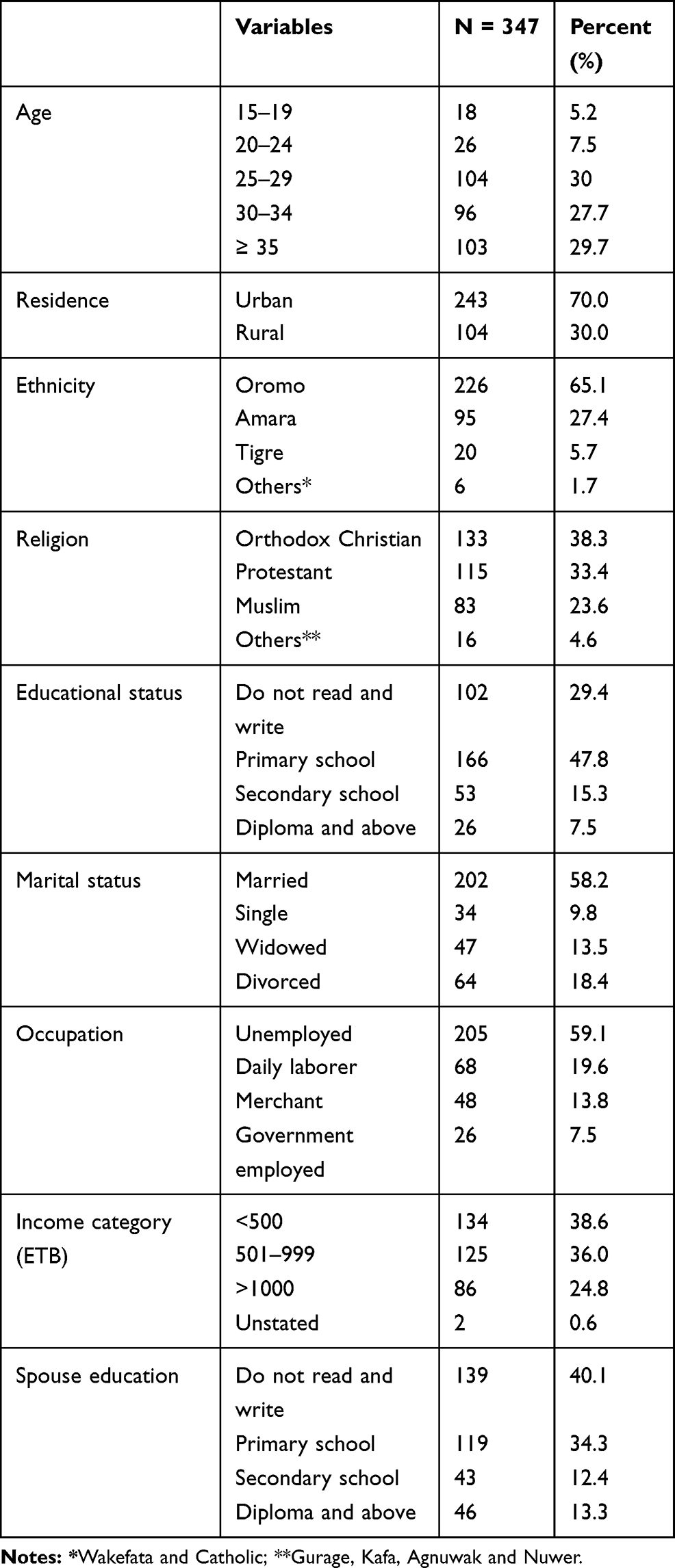 |
Table 1 Distribution of Study Participants by Their Socio-Demographic and Economic Characteristics at Ilu Aba Bora Zone ART Centers, Ethiopia, 2019 (n = 347) |
Information on Contraception and Unintended Pregnancy
Among study participants, 207 (59.7%) had been informed on family planning by their ART providers and 196 (56.5%) were informed at the time of screening for ART eligibility. However, only 132 (38.0%) of the participants were informed on unintended pregnancy by their ART provider (Figure 1).
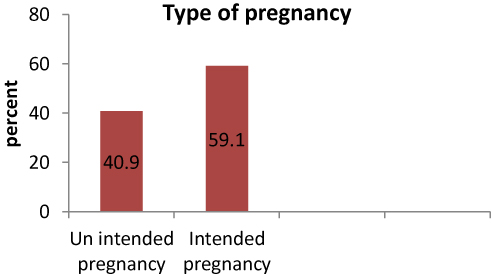 |
Figure 1 Type of pregnancy occurred after diagnosis among HIV-positive women attending ART clinics at public health facilities of Ilu Aba Bora zone, Ethiopia, 2018/19. |
Sexuality and Reproductive Health Information of the Respondents at ART Treatment Units
More than half, 188 (54.2%) of the study participants first had sexual intercourse at the age of 15–19. The majority of the study participants, 329 (94.8%) had sexual intercourse in the last 12 months of which 271 (78.1%) had only one sexual partner and 200 (57.6%) of them usually used a condom. Regarding the provision of a family planning service in ART clinics, 154 (44.4%) of them strongly support the idea (Table 2). The majority (294; 84.7%) of the study participants need to discuss any RH topics with their ART providers. However, only 158 (45.5%) had ever discussed RH issues with their ART providers and condom use (92.6%) was the most commonly discussed topic while a safe abortion service (20; 12.7%) was the least discussed of the RH topics.
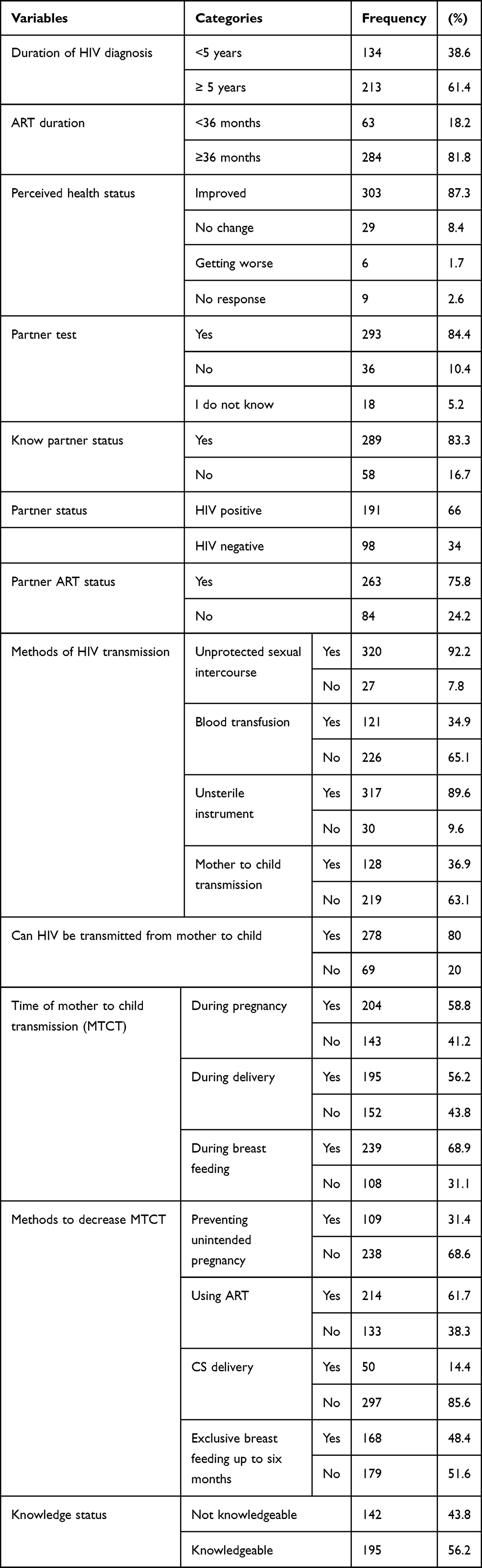 |
Table 2 HIV Status and Knowledge of Transmission Methods Among HIV-Positive Women Attending 13 ART Centers at Public Health Facilities of Ilu Aba Bora Zone, Ethiopia, 2019 (n = 347) |
Factors Associated with Unintended Pregnancy
In the multivariate logistic regression, unemployment (AOR, 3.36; 95% CI: 1.55–7.26), not being knowledgeable on MTCT and PMTCT (AOR, 3.18; 95% CI: [1.92–5.24), having no discussion on reproductive health issues (AOR, 1.83; 95% CI: 1.09–3.07) are factors significantly associated with unintended pregnancy occurrence among HIV-positive women on antiretroviral therapy (Table 3).
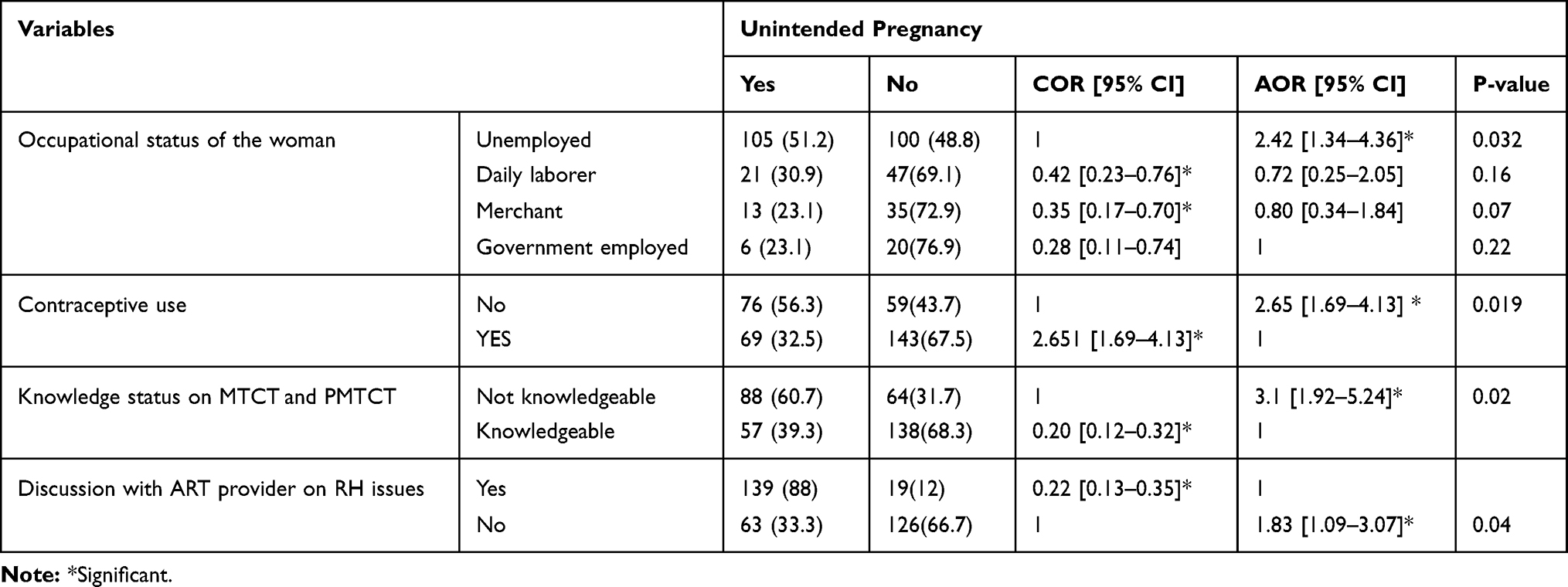 |
Table 3 Multivariate Logistic Regression Result for Factors Associated with Unintended Pregnancy Among HIV Positive Women Attending 13 ART Clinics at Ilu Aba Bora Zone ART Centers, Ethiopia, 2019 (n = 347) |
Discussion
The study revealed that 40.9% of the recent pregnancies after HIV diagnosis were unintended. The finding is in line with a study held in Addis Ababa (46%)8 and Enugu, Nigeria (37.2%).11 However, this finding is higher than the national unintended pregnancy rate of 24% but in line with a Oromia Regional State report of 39.8%.12
Occurrence of unintended pregnancy is three times more likely among unemployed (AOR 3.36; 95% CI: 1.55–7.26) compared with government-employed women. In line with this study, women with unintended pregnancies were more likely to be unemployed in a study held in Botswana.13 This could be because financial insecurity is not only a substantial barrier to obtaining the care needed to protect women’s sexual and reproductive health, but also affects women’s decision making about having children, more children or no children.14
Unintended pregnancy is twice as likely to occur among women not using contraceptives after their HIV diagnosis (AOR 1.85; 95% CI: 1.18–3.65) compared with contraceptive users. This is maybe because effective users of family planning are less likely to have an unintended pregnancy.
Unlike this study, unintended pregnancy was twice as likely to occur among women who used contraception in the past 12 months compared with non-users in a study held in Cape Town, South Africa.15 This controversial result may have been related to problems in effective and efficient use of contraception, which implies problems in family planning counseling.
Those not knowledgeable on MTCT and PMTCT are three times more likely (AOR 3.18; 95% CI: 1.92–5.24) to have an unintended pregnancy as compared with knowledgeable women. This implies that women having knowledge on MTCT and PMTCT knew the risk of HIV transmission and consequences of unintended pregnancy; they protect themselves from the risks of unintended pregnancy.
Unintended pregnancy is twice as likely to occur among women who have had no discussion on RH issues with their providers compared with those who did (AOR 1.83; 95% CI: 1.09– 3.07). Contraception counseling is one part of RH counseling that has been shown to be effective to decrease inconsistency and misuse of available contraceptive methods, and increase women’s use of modern contraception which prevents the occurrence of unintended pregnancy.16,17
Conclusions and Recommendation
The study revealed that 40.9% of the recent pregnancies after HIV diagnosis were unintended; the prevalence is high. To avoid unplanned pregnancies, HIV-infected women need access to effective family planning services and to have risk reduction discussions during routine care visits. So, the zone needs to strengthen monitoring and evaluation on active implementation of reproductive health integration with the ART service. Comprehensive and non-judgmental reproductive health counseling should be implemented for all women in the ART units regardless of their marital status, as every woman in the reproductive age group is potentially exposed to unintended pregnancy.
Limitation of the Study
The cross-sectional nature of the study makes it difficult to assess cause and effect relationships.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, anti-retroviral therapy; ARV, antiretroviral treatment; CPR, contraceptive prevalence rate; ETB, Ethiopian Birr; EC, emergency contraception; LBW, low birth weight; MOH, Ministry of Health; MTCT, mother to child HIV transmission; PMTCT, prevention of mother to child HIV transmission; RH, reproductive health.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
An ethical approval was obtained from IRB of Jimma university public health and medical science faculty department of nursing. Official letter of cooperation was written to Ilubabor zone and letter of cooperation was also written to each health facilities. And the study was conducted in accordance with the Declaration of Helsinki. Written informed consent which assured anonymity in publication of the final result was taken after explaining the purpose, importance of the study and right not to participate and with draw to the participants. Confidentiality of the information was maintained throughout by excluding names as identification in the questionnaire.
Acknowledgments
I would like to thank my almighty God and his mom St. Mary, my family (Tsige (mom),husband (Mr. Worke Yismaw), my children (Naty & Maryamawit), Ashu, Brukte, Manchu, Alemayehu (dad) and Mekdi) and Jimma and Mettu University for giving us the opportunity to do this research. I thank also data collectors and respondents.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research was funded by Jimma University.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. UNAIDS terminology guidelines (October 2011). 2011:16–23.
2. Darak S, Hutter I, Kulkarni S, Kulkarni V, Janssen F. Occurrence of pregnancies among HIV infected Indian women: does knowledge about HIV status make a difference? Int J Popul Res. 2015;2015. doi:10.1155/2015/617907
3. Chopra M, Daviaud E, Pattinson R, Fonn S, Lawn JE. Health in South Africa 2 saving the lives of South Africa ’ s mothers, babies, and children: can the health system deliver? Lancet. 2009;374(9692):835–846. doi:10.1016/S0140-6736(09)61123-5
4. Mccoy SI, Buzdugan R, Ralph LJ, et al. Unmet need for family planning, contraceptive failure, and unintended pregnancy among HIV-infected and HIV-uninfected women in Zimbabwe. PLoS One. 2014;9:e105320. doi:10.1371/journal.pone.0105320:8
5. Carolina N. 2007 STD incidence rates. 2007:129–154.
6. Dibaba Y, Fantahun M, Hindin MJ. The effects of pregnancy intention on the use of antenatal care services: systematic review and meta-analysis. Reprod Health. 2013;10(1):1. doi:10.1186/1742-4755-10-50
7. Hall J, Barrett G, Mbwana N, Copas A, Malata A, Stephenson J. Understanding pregnancy planning in a low- income country setting: validation of the London measure of unplanned pregnancy in Malawi. BMC Pregnancy Childbirth. 2013;13(200):1–8. doi:10.1186/1471-2393-13-200
8. Zewdu G, Mekonen A, Betre M College of health sciences school of public health unmet reproductive health care needs and occurrence of unintended pregnancy among HIV positive women in antiretroviral treatment units in Addis Ababa, Ethiopia Addis Ababa University College of Health Sc. 2011.
9. Kebede HG, Nahusenay H, Birhane Y. Assessment of contraceptive use and associated factors among HIV positive women in Bahir-Dar Town, Northwest Ethiopia. Open Access Library. 2015;2:e1942.
10. kindu Y, Kemal AOS. Assessment of knowledge and attitude towards prevention of mother to child transmission of Human Immuno Deficiency Syndrome (HIV) among HIV positive pregnant women, Dessie referral hospital. Int J Pharma Sci Res Assess. 2016;7(12):477–484.
11. Ezugwu EC, Iyoke CA, Nkwo PO, Ezegwui HU, Akabueze JC, Agu PU. International journal of gynecology and obstetrics unintended pregnancy among HIV-positive pregnant women in Enugu, southeast Nigeria. Int J Gynecol Obstet. 2016;132(1):60–63. doi:10.1016/j.ijgo.2015.06.039
12. Habte D, Teklu S, Melese T, Magafu MGMD. Correlates of unintended pregnancy in Ethiopia: results from a national survey. PLoS One. 2013;8(12):1–8. doi:10.1371/journal.pone.0082987
13. Mayondi GK, Wirth K, Morroni C, et al. Unintended pregnancy, contraceptive use, and childbearing desires among HIV- infected and HIV-uninfected women in Botswana: across-sectional study. BMC Public Health. 2016;16(44):1–10. doi:10.1186/s12889-015-2639-8
14. Narasimhan M, Orza L, Welbourn A, Bewley S, Vazquez M. Sexual and reproductive health and human rights of women living with HIV: a global community survey. Bull World Health Organ. 2016;94:243–249. doi:10.2471/BLT.14.150912
15. Iyun V. prevalence and determinants of unplanned pregnancy in HIV infected and uninfected women seeking Ante natal care in Cape Town,South Africa. 2016.
16. Nakaie N, Tuon S, Nozaki I, Yamaguchi F, Sasaki Y, Kakimoto K. Family planning practice and predictors of risk of inconsistent condom use among HIV-positive women on anti-retroviral therapy in Cambodia. BMC Public Health. 2014;14:170. doi:10.1186/1471-2458-14-170
17. Levi AJ, Simmonds KE. The role of nursing in the management of unintended pregnancy. Nursing Clinics of North America. 2009;44(3):301–304. doi:10.1016/j.cnur.2009.06.007
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.