")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Undiagnosed Hypertension and Associated Factors Among Adults in Hawela Tula Sub-City, Hawassa, Southern Ethiopia: A Community-Based Cross-Sectional Study
Authors Wachamo D , Geleta D , Woldesemayat EM
Received 14 August 2020
Accepted for publication 15 September 2020
Published 15 October 2020 Volume 2020:13 Pages 2169—2177
DOI https://doi.org/10.2147/RMHP.S276955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Demelash Wachamo,1 Dereje Geleta,2 Endrias Markos Woldesemayat2
1Hawassa College of Health Sciences, Department of Public Health, Hawassa, Ethiopia; 2Hawassa University, College of Medicine and Health Sciences, School of Public Health, Hawassa, Ethiopia
Correspondence: Endrias Markos Woldesemayat
Hawassa University, School of Public Health, Hawassa, Ethiopia
Email [email protected]
Background: Hypertension (HTN) is a major public health problem and often it is unnoticed. Undiagnosed HTN may lead to a high burden of cardiovascular diseases and complications such as stroke and heart attack. In this study, we aimed to assess the prevalence and associated factors of undiagnosed HTN.
Methods: From February to June 2019, a community-based cross-sectional study was conducted on 383 randomly selected adults in Hawela Tulla Sub-city, Hawassa, southern Ethiopia. Data were collected by pretested questionnaires, and physical measurements of weight, height and blood pressure were collected through standardized procedures adapted from WHO STEPS survey tools. Data entry and analysis were carried out using SPSS version 23 statistical software. Descriptive analysis and logistic regression models were used to describe the results. Logistic regression analysis results were declared statistically significant if the P-value was below 0.05 and the 95% CI did not cross the null value.
Results: The prevalence of undiagnosed HTN among the respondents was 12.3%. Only 152 (39.7%) of the study population knew the symptoms of HTN. Males (adjusted odds ratio [AOR] =2.5, 95% CI: 1.2, 5.2; P=0.016), people with a family history of HTN (AOR=2.7, 95% CI: 1.0, 7.0; P= 0.044), people who chewed khat (AOR=4.6, 95% CI: 2.0, 10.2; P< 0.001), overweight or obese individuals (AOR=3.5, 95% CI: 1.7, 7.3; P=0.001) and people with diabetes mellitus (AOR=3.2, 95% CI: 1.1, 9.3; P=0.036) had a higher risk of undiagnosed HTN than their counterparts.
Conclusion: Identification of people with the risk factors of undiagnosed HTN and delivering health education to reduce the risky behaviors could reduce the burden and consequences of HTN. Integrating interventions at the community level may be important.
Keywords: undiagnosed HTN, health-seeking behavior, Hawassa city, Ethiopia
Background
Globally, hypertension (HTN) has caused morbidity in about one billion people1 and killed 10 million people.2 In 2018, the prevalence of HTN among adults was 32.0% in urban areas and 24.0% in rural areas.3 In the early stages, symptoms of HTN are often not detectable and thus many people with the disease are left undiagnosed.4,5 Undiagnosed HTN increases the risk of complications such as renal failure, myocardial infarction, heart failure, stroke and premature death.6
About 75% of people with HTN live in low- and middle-income countries. People in such settings often have low awareness related to HTN, its treatment and control measures.7 This may lead to low healthcare-seeking behavior, which in turn results in a high prevalence of undiagnosed HTN in these populations. The prevalence of undiagnosed HTN was found to be 30% in the sub-Saharan Africa (SSA). Of those with HTN, 73% were unaware of their HTN; only 18% received treatment and 7% had a controlled blood pressure measurement.8
About 70% of people with HTN in Indonesia had undiagnosed HTN.9 A similar report in Vietnam found a prevalence of 17.4%.10 The prevalence of undiagnosed HTN was 22.0% in the USA,11 31.7% in Sri Lanka,12 10.1% in a rural population in India13 and 26% in western India.14 Another study, from northern India, reported a prevalence of 40.1%.15 In Byblos, Lebanon, 42.7% of study participants had undiagnosed or uncontrolled HTN.16 The prevalence of undiagnosed HTN in a rural community in Sudan was 38.2% (36.7% among males and 39.3% among females).17 In Dabat, northern Ethiopia, only 16.4% of patients with HTN were on antihypertensive treatment, while 83.4% had not been diagnosed and/or treated for HTN.18 The prevalence of undiagnosed HTN was 13.3% in Gulele Sub-city, Addis Ababa, Ethiopia.19 Over 80% of patients with HTN had no awareness of their status.20 In Gondar, northern Ethiopia, among people with HTN, 37.0% did not know that they had HTN.21
Harmful alcohol consumption, obesity and high salt intake were the risk factors significantly associated with undiagnosed HTN in northern India.15 In the same study, age (45–69-year age group), male gender, socioeconomic status and marital status were other risk factors which predicted having undiagnosed HTN.15 High age and illiteracy predicted undiagnosed HTN in a rural community in Sudan.17 In Nigeria, undiagnosed HTN was significantly higher among older, married and obese traders.22 Age, occupation and marital status were significantly associated with undiagnosed HTN in Gulele Sub-city, Addis Ababa, Ethiopia.19
The prevalence of HTN was higher among khat chewers in the past year than among non-chewers in Nekemte town in western Ethiopia.23 Chronic khat chewing was associated with increased systolic and diastolic blood pressure in Gurage Zone, southern Ethiopia.24 However, no reports have investigated the association between khat chewing and undiagnosed HTN. Moreover, the report from Ethiopia NCD STEPS in 2016 indicated that 76.6% of the total population had never had their blood pressure measured. There was a high prevalence of undiagnosed HTN among adolescents.13,23 To the best of our knowledge, there have been no report in the area in southern Ethiopia. Thus, in this study, we aimed to measure the prevalence and associated factors of undiagnosed HTN among adults in Hawela Tulla Sub-city of Hawassa city administration in southern Ethiopia.
Methods
Study Setting and Study Population
A community-based cross-sectional study was carried out between February 01 and May 01, 2019 in Hawela Tulla Sub-city of the Hawassa city administration in Sidama Region, southern Ethiopia. Tula is the capital town of Hawela Tulla Sub-city, which is located at a distance of 284 km to the south of Addis Ababa. Based on the report from the sub-city administration office, the total population was about 135,793 in 2018. Of this total, 69,255 (51%) were above 18 years of age. Hawela Tula Sub-city is known for its high level of cultivation of the khat plant and the khat market in Sidama Region. The source population considered in this study was adults living in the sub-city. The study population was randomly selected adults from the sampled households. People above the age of 18 years were included in the study. Medically confirmed cases of HTN, pregnant women and adults who did not agree to be interviewed because of any serious illnesses were excluded from the study.
Sample Size and Sampling Technique
Though we calculated a sample size of 390, the number of people involved in this study was 383. This sample size was calculated using a single-population proportion formula, considering the following assumptions. The prevalence of undiagnosed HTN (P=13.25%) was taken from a previous similar study conducted in Gulele Sub-city, Addis Ababa, Ethiopia.19 A value of precision of 1.96, a design effect of 2 and 10% for a possible non-response rate were also considered.
A multistage sampling technique was employed to recruit the study participants. In the first stage, using a simple random sampling technique, we selected five kebeles (lowest level of administration in Ethiopia) out of the 12 kebeles found in the sub-city. In the second stage, households were selected from the kebeles by employing a systematic random sampling technique. For each kebele, we took the list of households from the family folder located at the health posts (the institutions providing community health services in Ethiopia). Then, we randomly selected one adult aged above 18 years from each household.
Study Variables
The dependent variable considered in this study was undiagnosed HTN. Independent variables measured in the study were socio-demographic characteristics such as sex, age, occupation; personal and family history of morbidities; and knowledge and practice of the study participants towards HTN. We also collected data on tobacco smoking, alcohol consumption and performing of physical activity. Undiagnosed HTN refers to a person having a systolic blood pressure (SBP) of at least 140 mmHg and/or diastolic pressure (DBP) of at least 90 mmHg, which was not diagnosed before we conducted the survey.25 Khat chewing was defined as regular chewing of khat (a psychoactive substance) for at least 1 year before we conducted the survey. Khat has a physiological effect which may make a person who uses it not notice the early symptoms of HTN. Current alcohol drinking was defined as drinking of any amount and type of alcohol within 1 year prior to the survey. Current smoker referred to an adult who had smoked cigarettes within 1 year before the survey.25 Body mass index (BMI) was calculated as the weight of an individual in kilograms per height in meters squared. Obesity or overweight was considered when the BMI was above 25 kg/m2. Sedentary lifestyle referred to a type of lifestyle involving little or no physical activity, such as reading, watching television or using a mobile phone for a long time during the day. A family history of HTN was considered if a person’s first-degree relative (a parent, a grandparent or a sibling) had been diagnosed with HTN and/or were receiving drug therapy for HTN.
Data Collection Tools and Procedures
Five nurses with diploma-level training were recruited as enumerators. A Public Health Officer with Bachelor degree training supervised the data collection. Both the enumerators and the supervisor were selected from the health centers found in Hawassa town administration. DW delivered training for the enumerators and the supervisor on issues related to the study.
The survey instrument was adapted from the documents Ethiopian NCD STEPS25 and a modified WHO STEP-wise approach surveillance instrument version 3.26 The instrument consists of four main sections: socio-demographic characteristics, history of morbidity, knowledge or perception towards HTN and behavioral characteristics such as tobacco smoking, alcohol consumption and physical inactivity. It was prepared in English, then translated into Sidaamu Afoo language and then retranslated back to English to check the consistency in meaning.
Using a pretested questionnaire, a face-to-face interview was conducted. After completing the interview, the weight, height and blood pressure of the study participant were measured. We used calibrated instruments and standardized techniques to take the measurements. Weight was measured using an electronic scale. The instrument was checked and adjusted to zero for each measurement. Height was measured in the standing position. Blood pressure was measured three times in a sitting position using a standard mercury sphygmomanometer. The study participant rested for 3–5 minutes between the consecutive measurements. The measurement was taken after confirming that the study participant had not smoked or drunk any caffeinated beverage within 30 minutes before measuring the blood pressure. The average of the three blood pressure measurements was calculated to determine the blood pressure of the participant.
Data Quality Control Measurements
Both the data collectors and the supervisor were trained. The study material and the procedures were pretested before conducting the main study. After data collection, study materials were checked for completeness and incomplete questionnaires were corrected. Data were cleaned.
Data Analysis
Data entry and analysis were performed using SPSS version 23 statistical software. Descriptive statistics were computed to present frequency distributions. Bivariable logistic regression analysis was carried out to identify candidate variables for multivariable logistic regression analysis. All factors with a P-value of ≤0.2 in the bivariate logistic regression analysis were included in the multivariable model. The variables included in the multivariate analysis were gender, age, educational status, occupation, family history of HTN, khat chewing, alcohol drinking, BMI and diabetes mellitus. A multivariable logistic regression model was used to identify the independent predictors of undiagnosed HTN. Odds ratios (ORs) with a 95% confidence intervals (CI) were calculated. The result declared statistically significant if the P-value was below 0.05 and the 95% CI did not cross the null value. The Hosmer–Lemeshow goodness-of-fit statistic was used to assess whether the necessary assumptions for the application of multiple logistic regression were fulfilled.
Results
Socio-Demographic Characteristics
We interviewed a total of 383 participants, which yielded a response rate of 98.2%. Nearly half, 187 (48.8%), of the studied people were male and 191 (49.9%) were in the age category of 30–49 years with a mean (standard deviation) of 33.5 (10.3) years. The majority, 320 (83.6%), of the studied people were married and 258 (67.4%) were rural dwellers. Regarding educational status, 58 participants (15.1%) had no formal schooling. Concerning occupation, 137 (35.8%) were farmers. For more than half, 201 (52.5%), of the respondents, their households earned over 1,920 ETB (65.37 USD) per month (Table 1).
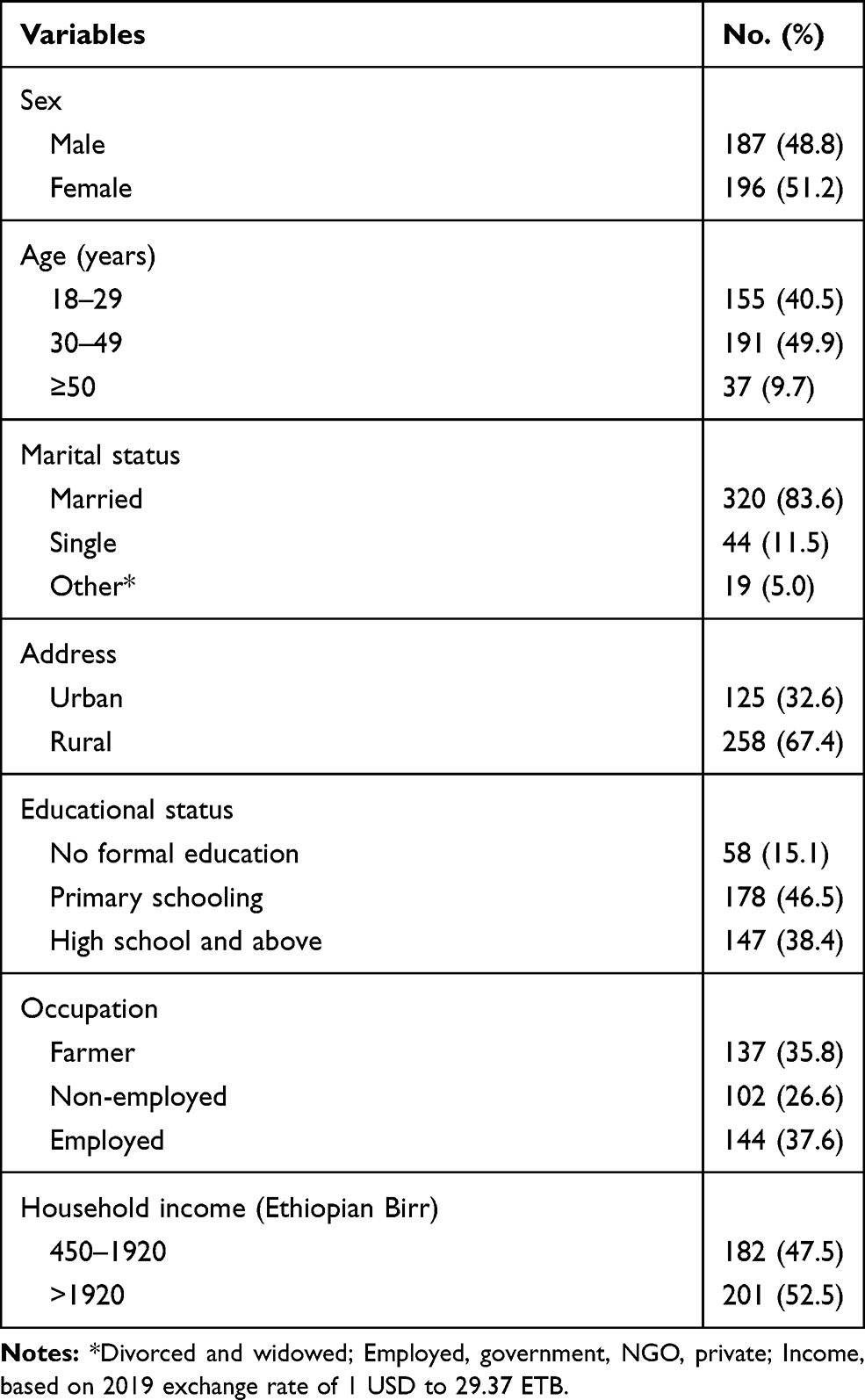 |
Table 1 Socio-Demographic Characteristics of the Study Participants |
Behavioral Characteristics and History of Morbidities
Only 14 (3.7%) of the study participants were current cigarette smokers, while 48 (12.5%) were khat chewers. Regarding alcohol consumption, 63 participants (16.4%) had drunk alcohol in the previous year. A sedentary lifestyle was seen in 148 (38.6%) of the studied people (Table 2). The BMI for 84 (21.9%) of the study participants was 25 kg/m2 or more. Undiagnosed HTN was observed in 47 (12.3%) of the study participants. Table 2 shows the behavioral characteristics, personal and family history of morbidities of the study participants.
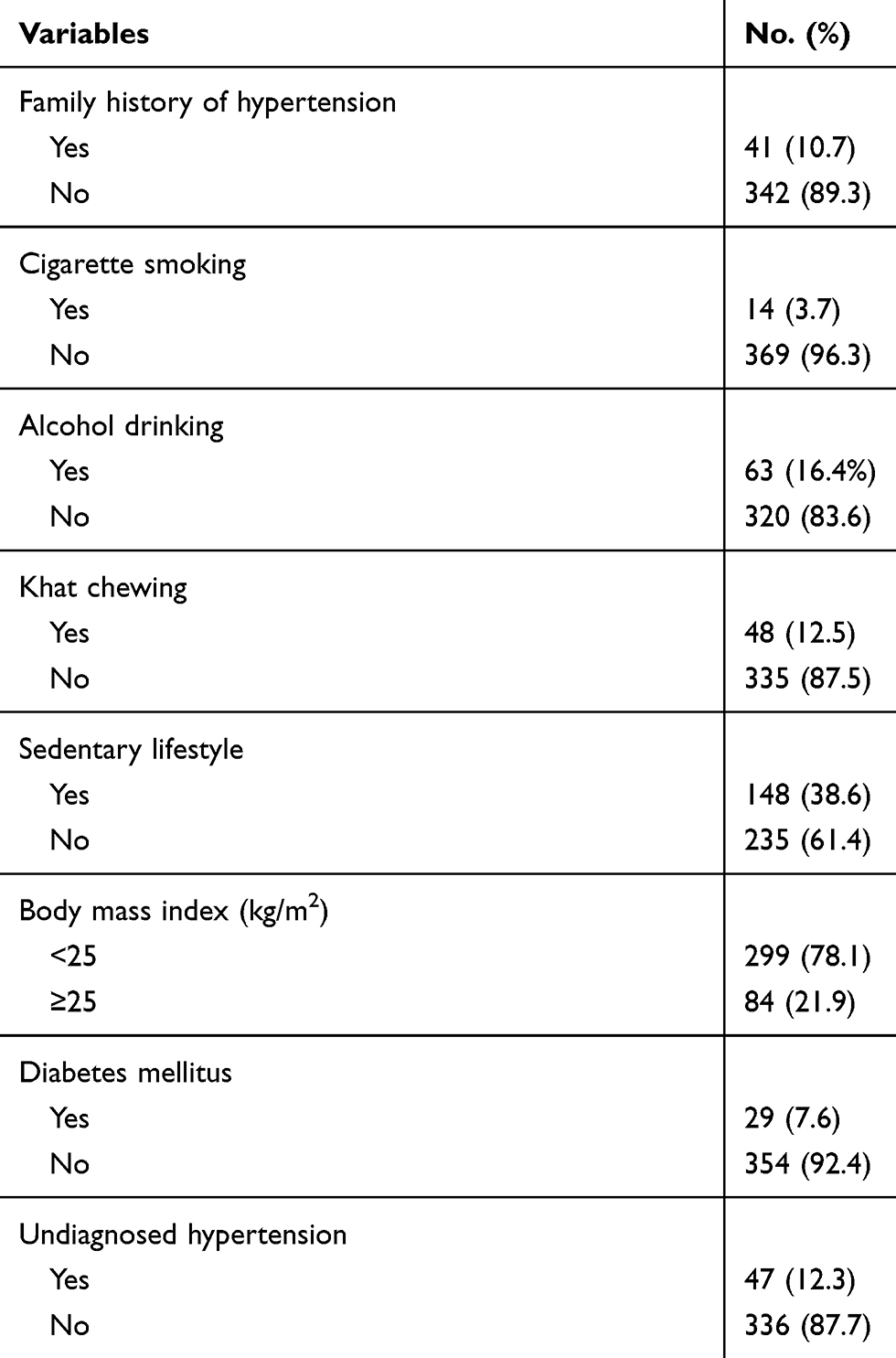 |
Table 2 Behavioral Characteristics, Personal and Family History of Morbidities of the Study Participants |
Knowledge, Perception and Practice of the Study Participants
Among the interviewed people, only 152 (39.7%) knew about HTN symptoms. About one-third of the study participants, 123 (32.1%), responded that HTN can be prevented, while 160 (41.8%) knew that HTN could cause complications. Moreover, 138 study participants (36.0%) perceived their susceptibility to HTN. The number of people who sought healthcare for HTN symptoms was 92 (24.0%), whereas 26 participants (6.8%) reported that their BP had never been measured at any time before the survey (Table 3).
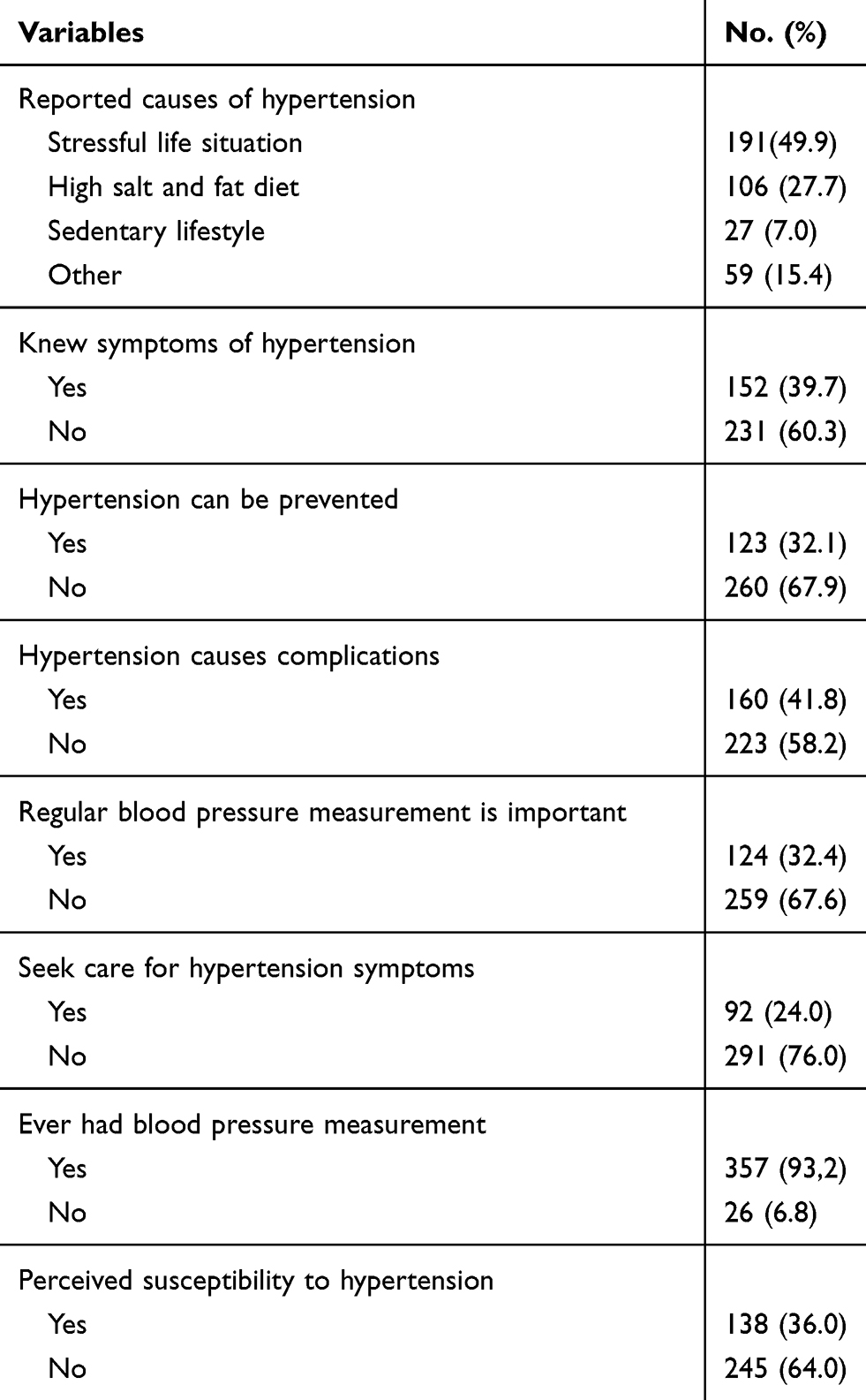 |
Table 3 Knowledge, Perception and Practice of the Study Participants Towards Hypertension |
Risk Factors of Undiagnosed HTN
In a bivariate analysis, gender, age, educational status, occupation, family history of HTN, khat chewing, alcohol drinking, BMI and diabetes mellitus showed significant statistical association with undiagnosed HTN. In a multivariate analysis, however, only gender of the respondent, family history of HTN, khat chewing, BMI and having diabetes mellitus maintained the significance in predicting undiagnosed HTN. Men had about 2.5 times higher risk of undiagnosed HTN (AOR=2.5, 95% CI 1.2, 5.2; P=0.016] than women. People with a family history of HTN had an increased risk of undiagnosed HTN compared to sthose without (AOR=2.7, 95% CI 1.0, 7.0; P=0.044]. People who chewed khat had over four times higher risk of developing undiagnosed HTN (AOR=4.6, 95% C: 2.0, 10.2; P<0.001). People with higher BMI had an increased risk of having undiagnosed HTN (AOR=3.5, 95% CI 1.7, 7.3; P=0.001). The risk of undiagnosed HTN was higher among people with diabetes mellitus than among people without diabetes mellitus (AOR=3.2, 95% CI 1.1, 9.3; P=0.036) (Table 4).
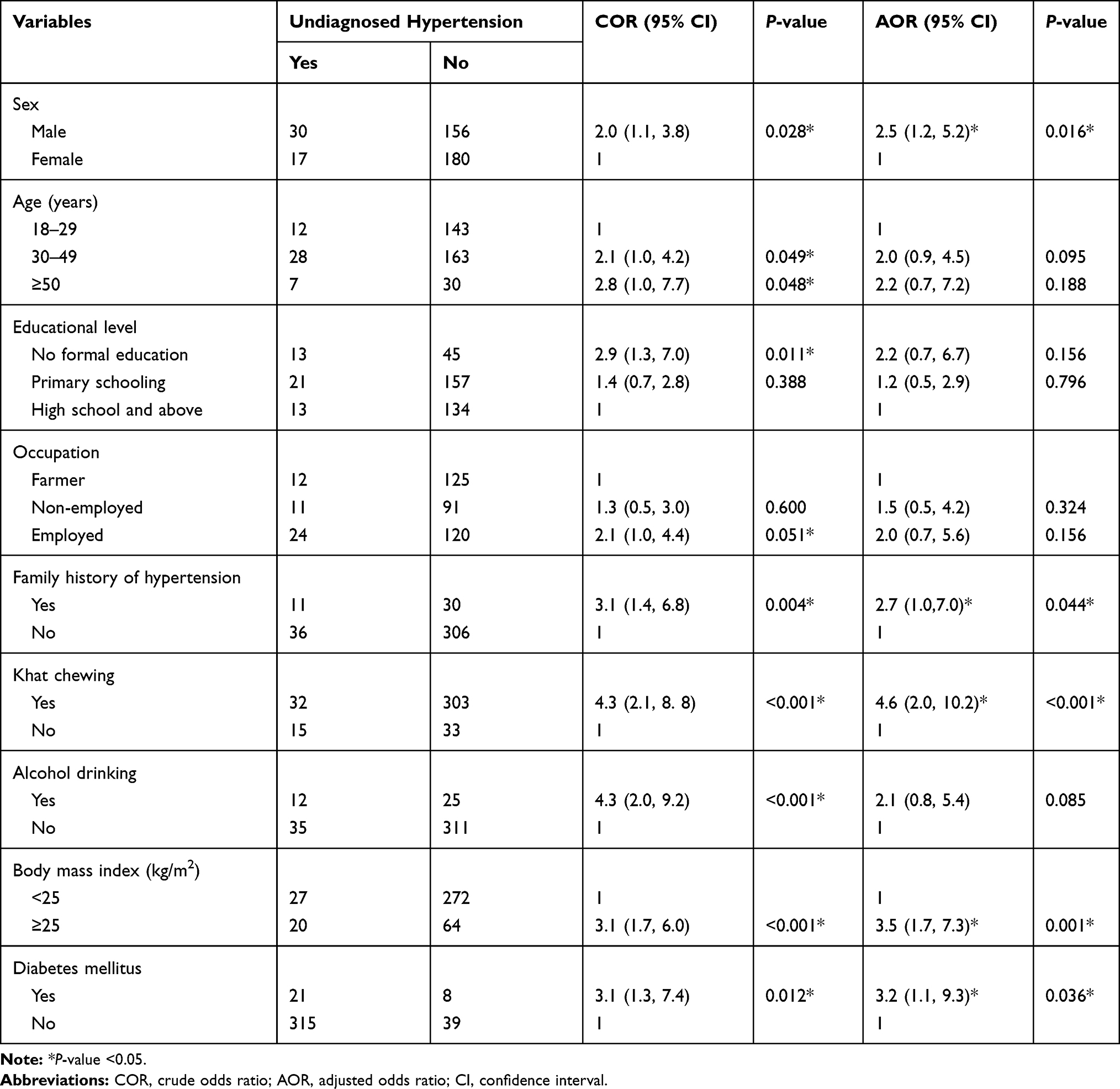 |
Table 4 Factors Associated with Undiagnosed Hypertension Among the Study Participants |
Discussion
In this community-based cross-sectional study among adult people, mainly consisting of rural dwellers, the prevalence of undiagnosed HTN was 12.3%. Our analysis showed that a high proportion of the study participants had no knowledge of the symptoms of HTN. Characteristics such as gender, family history of HTN, khat chewing, high BMI and having diabetes mellitus predicted undiagnosed HTN.
The prevalence of undiagnosed HTN was nearly consistent with the findings from Addis Ababa (13.3%) and Gondar City (10.47%) in Ethiopia19,21 and other settings.13,15,27 However, it was lower compared to the study reports from Bedele town (16.9%)28 and Aksum town (16.5%).29 The result in the current study was higher compared to the report from Gilgel Gibe (7.5%)30 and Durame town, in Ethiopia (8.96%).31 These differences could be related to socioeconomic factors, differences in access to health facilities and differences in the type of study population used in the studies. The area of Gilgel Gibe is one of the national field research sites, which has been used by Jimma University for many years. This may have improved people’s awareness, which in turn could lower the prevalence of undiagnosed HTN. The study in Durame was carried out in a town population.31 However, only one-fourth of participants in the current study consisted of urban dwellers. Compared to rural dwellers, people in towns have better awareness; this may lower the prevalence of undiagnosed HTN. Other possible reasons for the observed differences may include socio-demographic differences. In the current study, adults of at least 18 years of age were considered, whereas one of the previous studies included adults aged over 30 years.31 Incorporating and implementing periodical measuring of blood pressure for people with high risk of HTN as one of the components in the health extensions package may help in reducing the burden.
Among adults in Bangladesh, 15% had no knowledge of symptoms of HTN.32 In contrast to this, a high proportion (39.7%) of the study participants in the current study did not know the symptoms of HTN. This could be related to the low socioeconomic status of the study participants in Hawela Tulla Sub-city. Lack of knowledge on the symptoms of HTN may lead to incorrect practices, such as not going to health facilities for investigation and treatment. This may lead patients to face complications of HTN, such as stroke and heart attack, owing to the delayed diagnosis of HTN. To prevent such adverse outcomes, it is important to improve awareness about the symptoms of HTN by providing health education.
Unlike study reports from northern India,15 Sudan,17 Nigeria22 and Addis Ababa, Ethiopia,19 in the current study, the age of the study participants did not show an association with undiagnosed HTN. However, we found an increased risk of undiagnosed HTN among male participants compared to females. This finding is in agreement with reports from Durame town, in southern Ethiopia,31 and northern India.15 The higher risk of undiagnosed HTN among men may be related to an increased prevalence of the risk factors for HTN in men. These risk factors include regular consumption of meals with high calorie content, having a high BMI and smoking cigarettes. Interventions to minimize the risk factors of HTN and improving the health-seeking behavior of men in the study area are suggested to lower the risk of having undiagnosed HTN.
The risk of undiagnosed HTN was higher among adults with a family history of HTN. This result is in line with reports from other settings.17,33 The increased risk of undiagnosed HTN among people with a family history of HTN could be related to genetic factors which cause an increased risk of blood pressure, as seen in other reports.21,34 Identifying people with a family history of HTN and teaching them to undergo timely check-ups and to take physical activity may reduce the burden of undiagnosed HTN and its consequences.
Our data showed that people who chewed khat were more likely to have undiagnosed HTN. This result is in agreement with the study report from Mizan-Aman town, in south-west Ethiopia, in which khat chewing was reported as one of the risk factors of HTN.35 Khat may make people less likely to notice the early symptoms of HTN. If symptoms go unnoticed, people do not go to health facilities for the diagnosis of HTN. The habit of khat chewing carries a high expense for buying khat and this may result in poor healthcare-seeking behavior of people owing to the economic challenges. In addition to this, chewing khat makes people sit for a long time to enjoy its effects, which may promote a sedentary lifestyle, and its effect may inhibit identification of the early symptoms of HTN. Based on the results of our study, we advise that adults should avoid chewing khat to minimize the risk of undiagnosed HTN and its adverse outcomes.
In the current study, being overweight or obese increased the risk of undiagnosed HTN. This was in agreement with the study findings from Gondar city in north-west Ethiopia,36 Durame town in southern Ethiopia,31 India15 and Nigeria.22 High BMI is a well-known risk factor of HTN.37 It is important to teach people with high BMI to use interventions which could reduce their BMI and to check their BP regularly to reduce the risk of undiagnosed HTN and its consequences.
The results of our study showed that the risk of undiagnosed HTN was higher among adults with diabetes mellitus. This finding is in agreement with reports from north-west Ethiopia38 and Sudan.17 The higher risk of having undiagnosed HTN among diabetic cases may be related to the sharing of common risk factors between the two diseases, such as lack of physical activity and having a high BMI.39 Thus, performing the recommended level of physical activity and controlling BMI among diabetic cases may lower the risk of undiagnosed HTN among people in the study area. Furthermore, screening of patients with diabetes mellitus may help to reduce the risk of complications related to undiagnosed HTN.
We conducted a community-based study which consisted of mainly rural dwellers (over three-fourths of the study participants were rural dwellers). This may be considered as the strength of our study. On the other hand, the chicken-and-egg dilemma may be considered as the main limitation. The study could not establish a causal relationship of independent and dependent variables, as we implemented a cross-sectional study design.
Conclusions
In this study, we found a prevalence of undiagnosed HTN comparable with the findings in other settings in Ethiopia and elsewhere. A high proportion of the study participants was unaware of the symptoms of HTN. Being male, having a family history of HTN, khat chewing, being overweight or obese and having diabetes mellitus were found to be determinant factors of undiagnosed HTN among the study population. The study findings suggested the necessity of establishing strategies which may help in the timely detection of HTN. Identification of people with risk factors, delivering health education to reduce risky behaviors and carrying out timely check-ups may reduce the burden of undiagnosed HTN and its consequences. More attention should be given to adults with the identified risk factors. Incorporating periodical measuring of blood pressure for high-risk people as one of the components in the health extensions package may be used as a strategy to reduce the burden.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; DBP, diastolic blood pressure; ETB, Ethiopian Birr; mmHg, millimeters of mercury; NCD, non-communicable disease; SBP, systolic blood pressure; WHO, World Health Organization.
Data Sharing Statement
The datasets used in this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Board (IRB) of Hawassa University College of Medicine and Health Sciences and the study was conducted in accordance with the Declaration of Helsinki. A letter of support was obtained from Hawassa City Administration and Hawela Tulla Sub-city Health Offices. All participants were informed about the purpose, risks, benefit and confidentiality issues related to the study. Participation was on a voluntary basis and written informed consent was obtained from each participant, while verbal informed consent was obtained for participants who could not read and write.
Acknowledgments
The authors would like to thank Hawassa University for providing funding for the study. The authors are grateful to all data collectors and study participants for their valuable contributions
Author Contributions
DW wrote the research proposal, study design, execution, acquisition of data, analysis and interpretation. EMW and DG reviewed and approved the proposal and participated in data analysis. EMW reviewed the manuscript. All authors made a significant contribution to the work reported, data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Hawassa University provided funding for the study. The funder had no role in designing the study and conducting the analysis.
Disclosure
The authors declare that they have no conflict of interests for this work.
References
1. Forouzanfar MH, Liu P, Roth GA, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm hg, 1990–2015. JAMA. 2017;317(2):165–182. doi:10.1001/jama.2016.19043
2. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Kardiologia Polska (Polish Heart J). 2019;77(2):71–159. doi:10.5603/KP.2019.0018
3. Ezejimofor M, Uthman O, Chen Y-F, et al. Magnitude and pattern of hypertension in the Niger Delta: a systematic review and meta-analysis of community-based studies. J Glob Health. 2018;8(1):010420. doi:10.7189/jogh.08.010420
4. Global Burden of Disease Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788.
5. World Health Organization. A global brief on hypertension, monitoring the impact of action to tackle hypertension. Switzerland: WHO Press; 2013.
6. Misganaw A, Melaku YA, Tessema GA, et al. National disability-adjusted life years (DALYs) for 257 diseases and injuries in Ethiopia, 1990–2015: findings from the global burden of disease study 2015. Popul Health Metr. 2017;15(1):28. doi:10.1186/s12963-017-0146-0
7. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–450.
8. Ataklte F, Erqou S, Kaptoge S, et al. Burden of undiagnosed hypertension in Sub-Saharan Africa: a systematic review and meta-analysis. Hypertension. 2015;65:291–298.
9. Hussain MA, Mamun AA, Reid C, Huxley RR. Prevalence, awareness, treatment and control of hypertension in indonesian adults aged ≥40 years: findings from the Indonesia Family Life Survey (IFLS). PLoS One. 2016;11(8):e0160922. doi:10.1371/journal.pone.0160922
10. Van Minh H, Byass P, Chuc NTet al Gender differences in prevalence and socioeconomic determinants of hypertension: findings from the WHO STEPs survey in a rural community of Vietnam. J Hum Hypertension. 2008;20(2):109–115.
11. Crews DC, Plantinga LC, Miller ER, et al. Prevalence of chronic kidney disease in persons with undiagnosed or pre-hypertension in the U.S. Hypertension. 2011;55(5):1102–1109. doi:10.1161/HYPERTENSIONAHA.110.150722
12. Jayawardana NWIA, Jayalath WATA, Madhujith WMT, et al. Aging and obesity are associated with undiagnosed hypertension in a cohort of males in the Central Province of Sri Lanka: a cross-sectional descriptive study. BMC Cardiovasc Disord. 2017;17(1):165. doi:10.1186/s12872-017-0600-8
13. Undavalli VK, Mp H. Prevalence of undiagnosed hypertension: a public health challenge. Int J Community Med Public Health. 2018;5(4):1366–1370. doi:10.18203/2394-6040.ijcmph20180974
14. Shukla AN, Madan T, Thakkar BM, et al. Prevalence and predictors of undiagnosed hypertension in an apparently healthy Western Indian population. Adv Epidemiol. 2015;2015:1–5. doi:10.1155/2015/649184
15. Tripathy JP, Thakur JS, Jeet G, Chawla S, Jain S. Alarmingly high prevalence of hypertension and pre-hypertension in North India-results from a large cross-sectional STEPS survey. PLoS One. 2017;12(12):e0188619. doi:10.1371/journal.pone.0188619
16. Kanj H, Khalil A, Kossaify M, et al. Predictors of undiagnosed and uncontrolled hypertension in the local community of Byblos, Lebanon. Health Services Insights. 2018;11:1–7.
17. Bushara SO, Noor SK, Elmadhoun WM, Sulaiman AA, Ahmed MH. Undiagnosed hypertension in a rural community in Sudan and association with some features of the metabolic syndrome: how serious is the situation? Ren Fail. 2015;37(6):1022–1026. doi:10.3109/0886022X.2015.1052951
18. Abebe S, Berhane Y, Worku A, Getachew A. Prevalence and associated factors of hypertension: a crossectional community based study in Northwest Ethiopia. PLoS One. 2015;10(4):e0125210. doi:10.1371/journal.pone.0125210
19. Getachew F, Dirar A, Solomon D. Prevalence of undiagnosed hypertension and associated factors among residents in Gulele Sub-City, Addis Ababa, Ethiopia. J Community Med Health Educ. 2018;8(590):2161–0711.
20. Tesfaye T. Assessment of the prevalence of hypertension and associated factors among Ethiopian federal police officers Addis Ababa, Ethiopia: a community based cross-sectional study. EC Cardiology. 2017;2(6):278–286.
21. Awoke A, Awoke T, Alemu S, Megabiaw B. Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-sectional study. BMC Cardiovasc Disord. 2012;12(1):113. doi:10.1186/1471-2261-12-113
22. Vincent-Onabajo GO, Adaji JO, Umeonwuka CI. Prevalence of undiagnosed hypertension among traders at a regional market in Nigeria. Ann Med Health Sci Res. 2017;7:97–101.
23. Geleta T, Cheme MC, Roro EM. Physical, behavioral and sociodemographic determinants of hypertension among the adult population in Nekemte town, western Ethiopia: community based study. BMC Res Notes. 2019;12:764. doi:10.1186/s13104-019-4804-0
24. Geta TG, Woldeamanuel GG, Hailemariam BZ, Bedada DT. Association of chronic khat chewing with blood pressure and predictors of hypertension among adults in Gurage Zone, Southern Ethiopia: a comparative study. Integr Blood Press Control. 2019;12:33–42. doi:10.2147/IBPC.S234671
25. survey NCDNn, ed. Guidelines on clinical and programmatic management of major non-communicable diseases. Addis Ababa: Ethiopian Federal Democratic Republic of Ethiopia Ministry of Health AND Ethiopian Public Health Association; 2016.
26. A survey on prevalence of noncommunicable diseases (NCDs) and their risk factors among adults in Mekelle and Kilte-Awlaelo, Ethiopia. 2018.
27. Van Minh H, Byass P, Chuc NTK, Wall S. Gender differences in prevalence and socioeconomic determinants of hypertension: findings from the WHO STEPs survey in a rural community of Vietnam. J Hum Hypertens. 2006;20(2):109.
28. Gudina EK, Bonsa F, Hajito KW. Prevalence of hypertension and associated factors in Bedele Town, Southwest Ethiopia. Ethiop J Health Sci. 2014;24(1):21–26.
29. Gebrihet TA, Mesgna KH, Gebregiorgis YS, Kahsay AB, Weldehaweria NB, Weldu MG. Awareness, treatment, and control of hypertension is low among adults in Aksum town, northern Ethiopia: a sequential quantitative-qualitative study. PLoS One. 2017;12(5):e0176904. doi:10.1371/journal.pone.0176904
30. Alemseged F, Haileamlak A, Tegegn A, et al. Risk factors for chronic non-communicable diseases at Gilgel Gibe Field Research Center, southwest Ethiopia: population based study. Ethiop J Health Sci. 2012;22(4):19–28.
31. Helelo TP, Gelaw YA, Adane AA. Prevalence and associated factors of hypertension among adults in Durame Town, Southern Ethiopia. PLoS One. 2014;9(11):e112790.
32. Rahman N, Alam SS, Mia A, Haque M, Islam K. Knowledge, attitude and practice about hypertension among adult people of selected areas of Bangladesh. MedCrave. 2018;7(4):211–214.
33. Joshi SR, Saboo B, Vadivale M, et al. Prevalence of diagnosed and undiagnosed diabetes and hypertension in India – results from the Screening India’s Twin Epidemic (SITE) study. Diabetes Technol Ther. 2012;14(1):8–15. doi:10.1089/dia.2011.0243
34. Asresahegn H, Tadesse F, Beyene E. Prevalence and associated factors of hypertension among adults in Ethiopia: a community based cross-sectional study. BMC Res Notes. 2017;10(1):629.
35. Yarinbab TE, Alemseged F. Prevalence and determinants of modifiable risk factors for chronic non-communicable diseases among adults in Mizan-Aman Town, Ethiopia: a community based cross sectional study. Int Acad J Health Med Nurs. 2017;1:54–65.
36. Demisse AG, Greffie ES, Abebe SM, et al. High burden of hypertension across the age groups among residents of Gondar city in Ethiopia: a population based cross sectional study. BMC Public Health. 2017;17:647. doi:10.1186/s12889-017-4646-4
37. Oyekale AS. Effect of obesity and other risk factors on hypertension among women of reproductive age in Ghana: an instrumental variable probit model. Int J Environ Res Public Health. 2019;16:4699.
38. Worede A, Alemu S, Gelaw YA, Abebe M. The prevalence of impaired fasting glucose and undiagnosed diabetes mellitus and associated risk factors among adults living in a rural Koladiba town, northwest Ethiopia. BMC Res Notes. 2017;10(1):251.
39. Li C, Cheung BM. Diabetes and hypertension: is there a common metabolic pathway? Curr Atheroscler Rep. 2012;14(2):160–166.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.