")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Understanding Resilience Factors Among Caregivers of People with Alzheimer’s Disease in Spain
Authors Durán-Gómez N , Guerrero-Martín J , Pérez-Civantos D , López Jurado CF, Palomo-López P , Cáceres MC
Received 30 July 2020
Accepted for publication 2 November 2020
Published 20 November 2020 Volume 2020:13 Pages 1011—1025
DOI https://doi.org/10.2147/PRBM.S274758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Noelia Durán-Gómez,1 Jorge Guerrero-Martín,1 Demetrio Pérez-Civantos,2 Casimiro Fermín López Jurado,1 Patricia Palomo-López,1 Macarena C Cáceres1
1Department of Nursing, University of Extremadura, Badajoz, Spain; 2Department of Biomedicine, University of Extremadura, Badajoz, Spain
Correspondence: Noelia Durán-Gómez
Faculty of Medicine, University of Extremadura, Avda De Elvas s/n, Badajoz 06071, Spain
Tel +34924289466
Email [email protected]
Introduction: Alzheimer’s disease (AD) caregivers resilience involves the interaction between different risk and protective factors. Context of care, objective stressors, perceived stressors caregiver assessment, mediators factors and consequences of care were associated with resilience. We have developed a more integrated and operational conceptual model of resilience and care than previous models in our sociocultural environment.
Purpose: To assess the resilience of caregivers of people with AD and the related factors grouped according to an established operational conceptual model of Alzheimer´s caregivers stress.
Patients and Methods: A total of 120 primary informal caregivers of AD persons in Badajoz (Spain) were included in a cross-sectional design. The following variables have been measured on AD persons and caregivers: socio-demographic data, dependency level, cognitive decline, neuropsychiatric and behavioral symptoms, anxiety, depression, severity of somatic symptoms, level of burden, self-esteem, coping, social support, health-related quality of life (HRQOL) and resilience.
Results: Most of the caregivers reported symptoms of anxiety (63.3%) and depression (62.5%). We found out higher levels of resilience in caregivers with lower dependence caring (p=0.004). Higher resilience levels of caregivers were related to minor depressive (p=0.006) and anxiety symptoms (p=0.000), and higher HRQOL (p=0.000). Coping dimension mostly used was problem-based strategies such as active coping, positive reinterpretation and acceptance (p= 0.000).
Conclusion: Those caregivers reporting higher levels of resilience exhibited moderate to intense indicators of burden, fewer symptoms of depression and anxiety and fewer somatic symptoms. They also used adequate problem-focused coping strategies, showed higher levels of HRQOL and demonstrated an appropriate perception of social support. Despite the fact that the characteristics relating to the care context and to social support exert an undeniable influence on caregiver resilience, it would appear that the caregiver’s own intra-psychic resources reveal stronger correlations.
Relevance for Clinical Practice: The early and accurate identification of caregivers with lower levels of resilience could enable the implementation of vital psychological and educative support interventions to help caregivers to improve their well-being.
Keywords: adaptation, psychological, quality of life, social support, depression, anxiety, self-concept
Plain Language Summary
What is known on the subject?
- The primary caregiver endures a great burden owing to the nature of the disease and the specific needs of Alzheimer´s disease (AD) persons. Serious physical and mental health issues (depression, anxiety, high blood pressure, heart disease, etc) can arise in many cases as a result of the stress generated by this burden.
- However, a number of studies mention the different factors connected with the capacity to adapt and other positive effects on caregivers of AD persons, such as resilience, coping strategies and social support.
What this paper adds to existing knowledge?
- Despite the fact that the characteristics relating to the care context and to social support exert an undeniable influence on caregiver resilience, it would appear that the caregiver’s own intra-psychic resources reveal stronger correlations.
- The current study can contribute to existing literature and advance our understanding of resilience. In addition, the conceptual model of stress of Alzheimer’s caregivers may increase our knowledge of the factors and resources that are associated with resilience in families in which a member has been diagnosed with AD.
What are the implications for practice?
- In clinical practice we can use a holistic approach in the context of care that involves fostering psychological resilience, helping to manage their multiple responsibilities and prevent the caregiver’s symptoms from progressing to a diagnosable disorder.
- We can apply this model as a practical framework to provide caregivers of persons with AD with effective strategies to develop and improve resilience.
Introduction
The number of individuals suffering from dementia and in particular from Alzheimer’s disease (AD) is on the rise. In total, 50 million people worldwide are living with dementia since 2018. It is estimated that there will be 132 million cases in the world by 2050 and a new case of dementia every 3 seconds.1
The latest studies carried out in Spain estimate that there are around 800,000 people with dementia, of which approximately 60–80% correspond to AD.2 AD affects the lives of more than 3.5 million people in Spain, so that currently, one in four Spanish families has a member with the disease.3
The World Alzheimer Report 2019: Attitudes to dementia analyses findings of the world’s largest survey on attitudes to dementia.4 It established over 50% of caregivers said their health suffered as a result of their caring responsibilities and over 60% said the social life suffered as a result of their caring responsibilities. Help and support for caregivers should be a fundamental lynchpin of any national dementia plan. In the report, it is clear that even in high-income countries, most categories of survey respondents felt there were not enough services available.
The primary caregiver endures a great burden owing to the nature of the disease and the specific needs of AD persons.5,6 Serious physical and mental health issues (depression, anxiety, high blood pressure, heart disease, etc) can arise in many cases as a result of the stress generated by this burden.7–10
Furthermore, it has been proven that the health-related quality of life (HRQOL) of caregivers of persons with dementia is impaired.11 However, despite suffering health problems and a poorer quality of life, some caregivers extract great benefits and a sense of meaning from the care process, the gratifying nature of which provides a feeling of satisfaction.12 A number of studies mention the different factors connected with the capacity to adapt and other positive effects on caregivers of AD persons, such as resilience,7,8,13,14 coping strategies15 and social support.16 Resilience has been defined as “one’s capacity for successful adaptation when faced with the stress of adversity”.17,18 Although the HRQOL of AD person caregivers can be affected, it has been evidenced that highly resilient caregivers’ HRQOL is actually enhanced.19
Coping has been described as
The constantly evolving efforts, both behavioral and cognitive, that people employ to handle the specific external and/or internal demands which are considered to exceed or overwhelm an individual’s resources.20
Other protective factors which mediate negative health outcomes are social support, described as “the experience provided by others with resources that assist the person in everyday activities”,21 personal factors or faith,16,22 which also play a role in boosting resilience levels.13,14,16,23,24
Despite the fact that many studies have been performed to investigate both resilience levels in informal caregivers and the connection with other factors such as coping, social support and quality of life, several studies suggest the need for researchers to capture the heterogeneity of caregiver resilience when examining the longitudinal implications of informal long-term care, as well as the impact of resilience on physical health.7,8,25 The heterogeneity of resilience is found in its multidimensional nature and in the great heterogeneity existing among the population of caregivers that involves challenging interventions.
For this reason, the aim of this paper is to describe and analyze the resilience of informal caregivers of AD persons in Spain. Specifically, the study has a double objective. The main one, to evaluate the level of resilience of the caregivers and, secondly, to analyze the relationship with other variables, namely care context, stress factors, mediator variables and other variables connected to the emotional state of the caregiver (consequences of care) (Figure 1). All-in-one, it is intended to advance in the knowledge of the factors that influence certain caregivers to successfully adapt to one difficult situation and develop a more integrated and operational model of resilience and care than those previously mentioned.
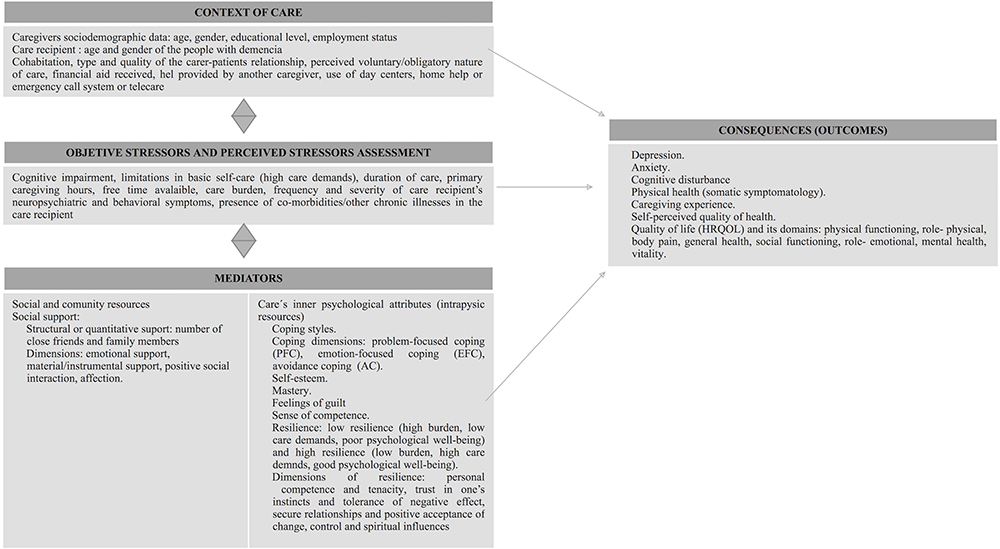 |
Figure 1 A conceptual model of Alzheimer´s caregivers stress. Source authors’ own elaboration (inspired by Gaugler et al (2007) and Joling et al (2016)).14,25 |
As a conceptual framework (Figure 1), the conceptual model of resilience of Gaugler et al,25 and the conceptual model of dementia caregiver resilience of Joling et al14 were fundamentally adopted, in which aspects such as context of care, objective stressors, perceived stressors assessment and mediators variables of the effects of stressors on the physical and psychological health of the caregiver, quality of life and self-perceived quality of health (consequences of care). Based on other previous research in our environment,23 resilience has been incorporated into the model as a mediator variable (in interaction with the other mediator variables), studying its role as a protection factor in chronic stress situations.
We hypothesize that high scores in resilience will be associated with exposure to a lower number of stressors derived from care, perceived stressors caregiver assessment, and adequate physical and psychological state of health and better quality of life. Furthermore, resilience, understood as a mediator variable between the stressors to which the person is exposed and their health status, will be related to other mediator variables, such as perceived social support and the intrapsychic resources of the caregiver (coping styles, self-esteem or sense of competence).
Patients and Methods
Participants
A total of 120 primary informal caregivers of AD persons in Badajoz (Spain) were included in a cross-sectional design. The participants were recruited through the Association of Relatives of AD persons and nursing consultations in Health Centers from the different healthcare areas, which form part of the Extremadura Health Service between 2018 and 2019. All of them fulfill the inclusion and exclusion criteria and were given an informed consent form, which they signed voluntarily.
Participants were selected through a non-probabilistic, intentional or convenience analysis on visiting the associations, institutions or specialized centers. Caregivers were invited to participate in the study and they were explained about the purpose and the characteristics of it. At the same time, they were also given the informed consent and the questionnaires. All the documents were fulfilled face-to-face at the primary healthcare center or by the home-visiting nurse. Clinical data of the patients with AD were collected from their electronic medical record.
Caregivers were defined as individuals providing daily care for a person diagnosed with AD. Inclusion criteria were that caregivers had to be at least 18 years of age, identify as the primary informal caregiver of the person with AD, that the AD person was not in a care facility, to have provided care for at least one year without financial remuneration and to have no history of serious psychiatric disorders or use of psycho-pharmaceuticals.
Measures
Socio-Demographic Data
On AD persons and caregivers such as factors relating to the care context were gathered using a structured questionnaire of our own design. It included gender, age, civil status, level of studies, employment status, relationship with the care-recipient, length of time as the primary caregiver, prior relationship, co-habitation and length of time with the patient, reason why they are caring for the patient, type and nature of assistance received (financial or help provided by another caregiver), number of hours dedicated to the patient and amount of free time available, using of day centers, emergency call system or telecare and home help.
Katz’s Instrumental Activities of Daily Living Index (IADL)26
Adapted to Spanish.27 It evaluates the autonomy/dependency level of the patient based on 6 dimensions (self-feeding, continence, dressing, transferring, toilet hygiene and bathing). It demonstrates appropriate levels of internal consistency and reliability.
Global Deterioration Scale (GDS)28
Adapted to Spanish.29 It assesses cognitive function and the global level of functioning of AD persons. This instrument describes 7 stages of global deterioration from no cognitive decline (stage 1) to very severe cognitive decline (stage 7). Test-retest and inter-rater reliability has proven to be good.
Neuropsychiatric Inventory Questionnaire (NPI-Q)30
Adapted to Spanish.31 Is an instrument that measures the severity and prevalence of 12 of the neuropsychiatric symptoms observed in AD persons. Higher scores indicate greater levels of neuropsychiatric symptoms (0–144). It has exhibited good test-retest reliability and positive convergent validity.
Patient Health Questionnaire (PHQ-15)32
Adapted to Spanish.33 A screening instrument of the intensity and severity of somatic symptoms. A global score ranging from 0 to 30 points is obtained from the summation of the scores from the 15 items. Thereafter, the patients are classified into two groups: patients not showing significant physical symptoms (from 0 to 4 points) and patients showing significant physical symptoms (>4 points). The PHQ-15 showed adequate internal consistency and there are strong correlations with other measures.
Beck Depression Inventory (BDI-II)34
Adapted to Spanish.35 It assesses the symptoms of depression. It is a 21-item scale. The standard cut-off score is 13 (score range 0–63) and the presence and degree of symptoms of depression can be detected. The Spanish adaptation exhibits high levels of reliability and validity and an internal consistency.
Goldberg Anxiety and Depression Scale (GADS)36
Adapted to Spanish.37 Only the anxiety scale (9 items) was used for the purpose of this paper to evaluate the presence and intensity of symptoms (cut-off score of > 4). The Spanish adaptation exhibits adequate sensitivity, specificity and positive predictive value.
Zarit Burden Inventory (ZBI)38
Adapted to Spanish.39 The 22-item version of this instrument measures the subjective level of burden experienced by caregivers in a caring situation. In the Spanish validation, the cut-off scores were determined: “lack of burden” (<46), “light burden” (47–55) and “heavy burden” (>56). The data obtained supports the high level of validity and reliability.
Rosenberg Self-Esteem Scale (RSES)40
Adapted to Spanish.41 It measures the degree of satisfaction with oneself by estimating the actual difference between the individual’s ideal self and real self. It is a 10-item scale. The total score ranges from 10 (low self-esteem) to 40 (high self-esteem). The adaptation to Spanish exhibits a high level of internal consistency, a high test-retest reliability and appropriate validity.
Coping Orientations to Problems Experienced Questionnaire (COPE-28, Brief COPE)42
Adapted and psychometric validation translated into Spanish.43 An inventory to assess the strategies caregivers employ in response to the care situation. This 28-item scale aims to determine 14 coping strategies. It has been possible to group these strategies into three main factors: problem-focused coping, emotion-focused coping and avoidance coping.44 The data available thus far supports the internal validity and reliability of the original version.
Connor-Davidson Resilience Scale (CD-RISC)45
Adapted to Spanish by.46 This instrument comprises 25 structured items for the assessment of the individual’s perceived hardiness over the previous month. The ratings give a number between 0 and 100 where higher scores indicate greater resilience. The CD-RISC consists of 5 factors which are believed to be significant components of resilience; 1) personal competence, 2) trust in one’s instincts and tolerance of negative effect, 3) positive acceptance of change, 4) control and 5) spiritual influences. It exhibits a high level of internal consistency convergent validity and a high test-retest reliability.
MOS Social Support Survey (MOS-SSS)47
Adapted to Spanish.48 It evaluates perceived social support, consisting of a total of 20 items based on four dimensions: emotional/informational, instrumental, positive social interaction and affection. The Spanish adaptation establishes the validity, reliability and appropriate, psychometric properties.
Short Form-36 Health Survey Questionnaire (SF-36)49,50
Adapted to Spanish.51 It is an instrument for the assessment of HRQOL with eight different health domains: Physical Functioning (PF), Role-Physical (RP), Body Pain (BP), General Health perceptions (GH), Social Functioning (SF), Role-Emotional (RE), Mental Health (MH) and Vitality (VT). For each domain is used a scale ranging from 0 (the worst state of health) to 100 (the best state of health), prior codification, aggregation and transformation of the items contained in each domain. The Spanish adaptation provides solid evidence of its acceptability and validity.
Statistical Analysis
The socio-demographic and clinical characteristics of the caregiver and person with AD were analyzed with descriptive statistics. The independent t-test, the chi-square test and the ANOVA test were used to assess the relationship between resilience (dependent variable) (DV) and socio-demographic, clinical and care context variables (independent variables) (IV) (Table 1).
 |
Table 1 Socio-Demographic, Clinical and Care Context Characteristics of Caregivers and People with AD and Correlations with Resilience |
Matrices of Pearson’s correlations were created to investigate correlations between resilience (DV) and objective stress (dependency level, cognitive decline, months of care, hours per day of care, free time available, neuropsychiatric and behavioral symptoms and co-morbidities), perceived stressors assessment (subjective burden), mediator variables (self-esteem, coping and social support) and those relating to the state of caregiver (anxiety, depression, severity of somatic symptoms and HRQOL (IV)) (Tables 2–4).
 |
Table 2 Objective Stress Variables, Perceived Stressors Assessment and Correlations with Resilience |
 |
Table 3 Variables Associated with the State of the Caregiver (Consequences of Care) |
 |
Table 4 Mediator Variables and Correlations with Resilience |
Based on the significant correlations, multivariate linear regressions were performed to determine the factors related to the caregivers’ resilience. The best models were selected on the basis of a trade-off between the highest explained variance (R2). To detect multicollinearity, we checked collinearity diagnosis in SPSS the Inflation Factor Variance (IFV <15) and the Condition Index (CI<10).
All statistical analyses were performed with IBM®SPSS® Statistics 22. For all analyses, the α-level was less than 0.05.
Results
Participants Characteristics
Socio-demographic, clinical and care context characteristics of caregivers and people with AD are shown in Table 1. The sample comprised 120 subjects, all primary caregivers of persons with AD, with an average age of 50.5±4.2. The majority were female (86.7%), married (74.25%) and a direct family member of the care recipient (90.8%).
More than half the sample of caregivers lived with the care recipient (56.7%). Of this group, 41.7% had been doing so since their relative began to require assistance, the vast majority defining their relationship with the patient as good with a high level of intimacy and affection (81.7%). Furthermore, over half the sample of caregivers (55.8%) were assisting their relative of their own accord.
Regarding formal support resources, more than two thirds of the sample (72.6%) stated that they used them. A total of 34.2% made use of day centers to help a family member and 3.7% called upon some kind of home assistance. In total, 6.7% had installed an emergency call system or a home telecare system. On an informal level, 72.5% stated that they received help from other relatives to care for the patient, qualifying this help as very useful in all cases. Only 20% of the caregivers received some kind of institutional, financial aid and this was preemptively linked to the existing dependency level.
Objective Stress Variables and Perceived Stressors Assessment
AD persons recorded mean IADL scores of 3.30±0.95 and GDS scores of 4.89±0.70, indicating the presence of moderate to high levels of ADL dependency and cognitive decline, along with co-morbidity (other chronic illnesses suffered by the care recipient) with an average of 1.88±0.86. A total of 95% of the sample group of care recipients showed evidence of psychiatric and behavioral disorders. Of the 12 domains of the scale, apathy/indifference was the most prevalent (85.8%) followed by anxiety and depression with the same percentage (61.7%) and eating disorders (appetite/nutrition) with 60.8% (n=73) (Table 2). The caregivers attend to their relative for an average of 13.48±6.9 hours a day, a considerable proportion of their day, and they had been giving this care for an average of 48.80±27.46 months.
As regards perceived stressors assessment, caregivers scored an average of 60.72± 13.70 for perceived care burden. It can be seen that 61.6% of the primary informal caregivers face a severe burden in subjective sub-dimension (Table 2).
The following scores were obtained for the two sub-dimensions of the primary informal caregivers’ burden (subjective and objective): the mean subjective burden score was 26.25± 7.88 and the mean objective burden score was 16.43 ± 4.56. It was discovered that the most affected dimensions are impact of care (mean 16.43±3.90) and interpersonal relationships (mean 13.18±4.52) (Table 2).
Variables Associated with the State of the Caregiver
Our sample revealed symptoms of anxiety in 63.3% of the cases, the mean being 7.59±1.21. These levels are considered moderate to severe. In addition, 62.5% of the sample showed symptoms of depression, the mean being 15.05±9.15 (Table 3).
A mean of 10.91± 4.90 was obtained for the primary informal caregiver’s perception of the severity of the somatic symptoms. The two subgroups in the sample reveal that 91.7% of the somatic symptoms are relevant. The most frequently observed sets of somatic symptoms are sleep disorders (95.8%) followed by pain in arms, legs and joints (95%), fatigue (90.9%), back pain (73.3%), headaches (72.5%), constipation or diarrhea (68.4%) and stomach pain (57.5%).
As regards self-perceived quality of health, 56.7% deemed their level of health to be average, 11.7% viewed it as poor but 31.7% (n=38) considered their health to be good.
When the HRQOL of caregivers sufferers is assessed (Table 3), the highest-scoring domain was PF, followed by MH, RP and GH, whereas the lowest score was obtained by BP. In descending order of points, the results are PF>MH>RP>GH>RE>VT>SF>BP.
Mediator Variables
The level of self-esteem obtained was 24.19± 2.45. The most frequently used coping strategies were the following: active coping, positive reappraisal and acceptance. On the contrary, the least used coping strategies revealed to be behavioral disengagement, humor and substance use. Thus, it can be observed that the sample group made greater use of problem-focused coping strategies (3.02±0.93) as opposed to emotion-focused strategies (2.26±1.01) or avoidance (1.97±1.24) (Table 4).
The structural or quantitative support had mean values of 3.3 ± 2.23 for close friends and 4.14 ± 2.51 for close family members; the qualitative support revealed the data represented in Table 4. The results obtained revealed a stronger perception of emotional support (31.39±6.32) as opposed to the other dimensions: social (15.53±4.08), material (14.75±4.11) and affection (12.60±2.92).
As regards levels of resilience, the caregivers obtained a mean score of 69.24±14.07 on the CD-RISC scale (Table 5). Half the subjects can be considered to have an average level of resilience. A cut-off score of 70 (Connor & Davidson, 2003) was determined to identify highly resilient caregivers and it can be seen that 51.66% equaled this score or obtained a higher score. In descending order, the highest points per factor were as follows: feeling of having control over one’s own life, personal competence and tenacity followed by establishing secure relationships and positive acceptance of change, trust and tolerance of negative effect, and finally, spiritual influences.
 |
Table 5 Resilience Scores for the Sample Group of Caregivers |
Influential Factors of Resilience Capacity
An analysis was performed on the correlation between the resilience scores obtained by the CD-RISC and the variables relating to socio-demographic and clinical characteristics and the care context (Table 1). Findings reveal that those subjects who were unemployed or doing unpaid work reported lower levels of resilience than those in gainful employment (p=0.016). The situation is different when correlating the cohabitation with the AD person, in so far as individuals who were living with the AD sufferer reported higher levels of resilience (p=0.008). Also, the highest levels of resilience can be linked to the following situations: when the caregiver is a direct relative (p=0.045), receiving financial support (p=0.001) and extra help (p= 0.000).
As regards the stress variables relating to the situation of assistance (Table 2), the highest resilience scores correlated with a lower level of dependency (p= 0.004) and with the care recipient’s cognitive decline (p= 0.007), but not with the rest of objective stressors. In the assessment of stressors by the caregiver, resilience correlated negatively with subjective levels of burden (p= 0.000) and with the component of the caregiver’s objective burden (p= 0.043); therefore, the most resilient caregivers showed a more objective evaluation of these stressors.
Significant correlations were found between resilience and a set of the variables considered to be indicative of consequences of care (Table 3). Specifically, resilience is inversely correlated with the caregiver’s symptoms of depression (p = 0.006) and their anxiety (p = 0.000). Furthermore, the caregivers reporting the highest scores for resilience also obtain the highest scores in HRQOL (p= 0.000). In addition, when resilience was compared with HRQOL, the only strong correlation was with role-physical, so an adequate level of resilience diminished the perception of work-related or other day-to-day problems (p= 0.032). Also, high scores on the CD-RISC correlate with a reduction in the presence of sets of somatic symptoms in the caregiver (p= 0.004) and higher level of self-perceived quality of health.
Those factors considered to be mediators correlate with the level of resilience (Table 4). A higher level of resilience correlates with a higher level of self-esteem (p= 0.001). Higher levels of perceived social support had a positive effect on the resilience of the subjects (p= 0.013), the results reporting a significant link with the dimension of emotional support (p= 0.000) and leisure and distraction (positive social interaction) (p= 0.024).
Furthermore, coping styles have an impact on resilience levels, so the most appropriate responses when faced with stressful situations were directly related to the subject’s adaptation to these situations (p<0.000). Specifically, there was a link between resilience and a greater use of problem-based strategies (p= 0.000).
Predictors Factors of Resilience
The linear regression model examined the relationship of the resilience and the variables that were significantly correlated (Tables 1–4). The linear regression indicated that resilience was significantly related to the anxiety symptoms (p < 0.001), caregivers burden (p=0.012), coping (p=0.001), social support (p=0.008), cohabitation with care recipient (p=0.038), help provided (financial or by another caregiver) (p=0.001) and the HRQOL (p < 0.01). The final model with factors associated with resilience explained 76.1% of the observed variance (p < 0.05). The adjusted R2 values and the standardized regression weights are presented in Table 6.
 |
Table 6 Regression Model of Factors Related to Caregivers Resilience |
Discussion
We hypothesize that high scores in resilience will be associated with exposure to a lower number of stressors derived from care, perceived stressors caregiver assessment, and adequate physical and psychological state of health and better quality of life. Furthermore, resilience, understood as a mediator variable between the stressors to which the person is exposed and their health status, will be related to other mediator variables, such as perceived social support and the intrapsychic resources of the caregiver (coping styles, self-esteem or sense of competence).
In this sense, this paper demonstrates that many caregivers possess an extraordinary capacity of adaptation in the face of highly demanding situations and a heavy burden of care. Resilience and its adaptive capacity are not so much to do with the inherent stressors or the objective characteristics of the care context, but primarily with subjective aspects relating to internal resources and the caregiver’s concept of them.
Various studies confirm the presence of moderate to high levels of resilience in a substantial percentage of AD person caregivers even though they are subject to severe stressors, and this is also reflected in our research.16,18,23 This fact proves that, although the resilience of caregivers is affected by the care situation (they report lower mean scores than the population in general, 80.4),45 not all caregivers respond in the same way to the stress variable of caring and a significant percentage of these caregivers could be considered highly resilient.52
Caregivers obtain the highest scores in certain dimensions of resilience, such as the feeling of control over one’s own life, personal competence and tenacity as well as positive acceptance of change and secure relationships. This would seem to indicate that they perceive a significant degree of control over their own lives, trusting their strengths and the affective bonds they create and showing a tendency to adapt and give meaning to the situation in which they find themselves.23 The fact that the majority of caregivers perform their duties of their own accord may help to explain why the caregiver’s perception of their capacity to tackle stressful situations is positive.
When the relationship between resilience levels and the care context is taken into consideration, links are established between lower levels of resilience and the following factors; being unemployed or in unpaid employment, bearing no family relationship with the AD person and a lack of financial assistance or support from other caregivers. It can be confirmed that specific factors increase the degree of vulnerability of caregivers and clearly impact on their resilience. The relationship factor can be explained by the fact that when a family bond exists, the perception of intimacy and affection acts as a coping strategy thus modifying the interconnection between the stress undergone and the consequences on the caregiver’s health, and so there is a positive impact on resilience.23 Other studies discovered a greater likelihood that caregivers who benefited from a substantial degree of family support would score more highly in resilience.16,53
In this same care context, our findings showed the caregivers who lived with their patients reported higher levels of resilience. Sustaining the burden of care presumably involves a long-term commitment which inevitably offers new challenges to the individual.54 It can be supposed that these caregivers manage to be resilient and are therefore able to deal with stressors, demonstrating successful coping in the face of the stress generated by adversity.55 However, other studies have concluded that living independently from the patient was linked to higher levels of resilience.14,25
On the whole, correlations with resilience were not found when objective caregiver stress was taken into consideration. Only the cognitive state of the patient and consequently, their degree of dependency show an inverse correlation with resilience in accordance with other studies.25,56 Resilience is independent from the frequency and gravity of the problems (as far as the patient’s neuropsychiatric symptoms are concerned), the duration of care, the hours per day dedicated to care, the free time available and the presence of other chronic illnesses in the care recipient. It has been demonstrated the lack of a relationship between the perceived benefits of care and the objective stressors of the situation, which suggests that perceived benefits depend on other aspects of the caregiver-care recipient relationship. Mutual closeness, motivation or characteristics of the caregiver’s personality are just some of those aspects.56
In addition, it has been found that resilience was more closely linked to the characteristics and abilities of the individual and that resilient caregivers might not perceive the clinical symptoms of AD as uncontrollable.18 On the contrary, the presence of burden is likely to depend pre-emptively on subjective factors. The most resilient caregivers might be more accepting in the face of the behavior changes of AD persons because resilience presumably enables a better psychological adjustment and the development of new coping strategies in response to the demands of dementia care.57
The subjective perception of a greater burden of care was associated with lower resilience, which is consistent with other previous studies.18,52,55,58 This situation could be interpreted in the following way; individuals reporting lower levels of resilience might be more concerned by and tend to be more susceptible to situations which provoke stress. They can have stronger reactions to stressful daily events and focus more on the negative aspects of care which leads to a tendency to select dysfunctional coping strategies.54 On the other hand, individuals possessing higher levels of resilience might have a positive self-image, self-efficacy and a healthy attitude to life.59
Furthermore, our findings revealed significant differences in the negative repercussions of care on the emotional state of the caregiver. The presence of higher levels of symptoms of depression and anxiety in the family caregiver has been correlated with lower levels of resilience.14,55,58 Resilience can be conceived as a feature of personality54 which acts as a protector against depression and is linked to stress reduction.25 On the contrary, other authors suggest that resilience is not a feature of personality but a set of behaviors, beliefs and actions that can be nurtured throughout life establishing appropriate emotional connections.23 High scores in resilience are also linked to lower levels of somatic symptoms in the caregiver. Resilience could be considered a significant predictor of the caregiver’s state of health.23,60
In this study, the significant link between resilience and caregiver HRQOL is confirmed. The caregivers reporting the highest levels of resilience also showed the highest levels of HRQOL. It has been reported the interrelationship between HRQOL and personal strengths such as resilience, sense of coherence and optimism.16,19 Resilience acts as a protector by improving quality of life, coping and general adaptability to care-related difficulties.19 Specifically, our findings revealed a correlation with role-physical, therefore the most resilient caregivers perceived fewer work or other day-to-day problems and a better HRQOL. Meanwhile, Trapp et al (2015) discovered that personal strength was associated with caregiver HRQOL, although the effect was substantially stronger for mental HRQOL than for physical HRQOL.
A factor which might have a positive impact on caregiver resilience is social support. The findings of some studies indicate that social support has a positive impact on resilience and that caregivers who received strong family support were more likely to be highly resilient.16,53 It can be suggested that social support should mediate the effects of the stressors caregivers face and explain the individual differences in the well-being of caregivers,53 serving as a buffer between the effects of stress and the emotional state of the caregiver.13,18,23,55 Resilience is that of a mediator variable of the effects of stress and its consequences. Individuals reporting high levels of resilience tend to evaluate the stressors they deal within a more positive manner, as well as the social support available to them. In addition, they are less likely to suffer psychological problems.52
Still on the topic of resilience mediator variables, our findings pointed to a correlation between high scores in resilience and high levels of self-esteem. It is safe to assume that this is a two-way relationship and this is consistent with other studies.23 Furthermore, it has been demonstrated that the development of coping strategies is fundamental to the caregiver’s ability to deal with psychological distress and this factor is recognized as being paramount in the development of high levels of resilience.15 The findings of this study reveal that problem-focused and emotion-focused strategies are the most used by caregivers, as opposed to dysfunctional strategies. Our results are consistent with those of the systematic review published by Monteiro et al (2018). They demonstrated that problem-focused strategies (active coping, positive reinterpretation, instrumental support and planning) are effective when dealing with specific problems and dysfunctional coping strategies can have negative consequences when dealing with an AD person.15 Thus, dysfunctional coping strategies and depression seem to be the most significant predictors of caregiver anxiety. Resilience is positively correlated with problem-focused coping styles, while avoidance-coping would seem to have a negative impact on resilience.22
The contributions of this study are evident, but it is not without its limitations. As this is a transversal study, changes in the population cannot be detected given that a causal conclusion cannot be reached, especially as regards those phenomena, which are sensitive to change such as the improvement of clinical variables.
Conclusions
In general, our findings offer a number of clinical contributions to the positive aspects of care as however challenging and stressful caring for a family member with AD may be, a group of caregivers can manage to handle the situation relatively well given that the majority of caregivers report average to high levels of resilience. Resilience is linked to a variety of factors, which confirms its multidimensional nature.
Those caregivers reporting higher levels of resilience exhibited moderate to intense indicators of burden, fewer symptoms of depression and anxiety and fewer somatic symptoms. They also used adequate problem-focused coping strategies, showed higher levels of HRQOL and demonstrated an appropriate perception of social support. However, and despite the fact that the characteristics relating to the care context and to social support exert an undeniable influence on caregiver resilience, it would appear that the caregiver’s own intra-psychic resources (self-esteem, hope, optimism, coping) reveal stronger correlations. A connection can be assumed to exist between resilience and the individual’s characteristics and abilities whereas the links with both the clinical status of the AD sufferer and the objective care stressors seem weaker. In this regard, the way the stressors are evaluated and the coping style employed by the caregiver have become established as factors of paramount importance in the development of high levels of resilience.
Greater insight into caregiver resilience and its determining factors could facilitate the early and accurate identification of caregivers with lower levels of resilience. This could enable the implementation of vital psychological and educative support interventions to help caregivers to improve their well-being and serve as a basis for the design of intervention programs. To that end, a standardized measure of resilience in the care context would enable a more precise measurement across populations and it could also facilitate the adaptation of interventions which aim to promote caregiver resilience, to improve both their physical and mental health and to ensure that the care of AD persons continues to be manageable in the future.
Relevance for Clinical Practice
The current study can contribute to existing literature and advance our understanding of resilience. In addition, the conceptual model of stress of Alzheimer’s caregivers may increase our knowledge of the factors and resources that are associated with resilience in families in which a member has been diagnosed with AD.
The protection and increase of the resilience of caregivers is a priority for mental health nursing. The promotion of resilience is based on the recognition of strengths beyond vulnerability. It is of key importance because it involves responding to the challenges that affect the individual in their health behavior.
It is important to identify the processes by which resilience is formed and to develop predictive and intervention models that decide which individuals are most likely to benefit from specific mental health interventions aimed at increasing resilience factors.
In clinical practice we can use a holistic approach in the context of care that involves fostering psychological resilience, helping to manage their multiple responsibilities and prevent the caregiver’s symptoms from progressing to a diagnosable disorder.
We can apply this model as a practical framework to provide caregivers of persons with AD with effective strategies to develop and improve resilience.
Ethical Statement
Permission was obtained from the Ethics in Clinical Investigation Committee of Badajoz. Confidentiality of the information was maintained at all times in accordance with Declaration of Helsinki and current legislation (Spanish Organic Law 3/2018, of December 5, on Protection of Personal Data and guarantee of digital rights).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was partially financed by a grant of the Regional Government of Extremadura. European Regional Development Fund (FEDER) (GR18045).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patterson C. World Alzheimer Report 2018: The State of the Art of Dementia Research: New Frontiers. London, UK: Alzheimer’s Disease International (ADI); 2018.
2. Soto-Gordoa M, Arrospide A, Moreno-Izco F, Martinez-Lage P, Castilla I, Mar J. Projecting burden of dementia in spain, 2010–2050: impact of modifying risk factors. J Alzheimers Dis. 2015;48(3):721–730. doi:10.3233/JAD-150233
3. Martínez-Lage P, Martín-Carrasco M, Arrieta E, Rodrigo J, Formiga F. Mapa de la enfermedad de alzheimer y otras demencias en españa. proyecto MapEA. Rev Esp Geriatr Gerontol. 2018;53(1):26–37. doi:10.1016/j.regg.2017.07.006
4. Alzheimer’s Disease International. World Alzheimer Report 2019: Attitudes to Dementia. 2019.
5. Allegri RF, Sarasola D, Serrano CM, et al. Neuropsychiatric symptoms as a predictor of caregiver burden in alzheimer’s disease. Neuropsychiatr Dis Treat. 2006;2(1):105.
6. Peña-Longobardo LM, Oliva-Moreno J. Caregiver burden in alzheimer’s disease patients in spain. J Alzheimers Dis. 2015;43(4):1293–1302. doi:10.3233/JAD-141374
7. Harmell AL, Chattillion EA, Roepke SK, Mausbach BT. A review of the psychobiology of dementia caregiving: a focus on resilience factors. Curr Psychiatry Rep. 2011;13(3):219–224. doi:10.1007/s11920-011-0187-1
8. Bull MJ. Strategies for sustaining self used by family caregivers for older adults with dementia. J Holist Nurs. 2014;32(2):127–135. doi:10.1177/0898010113509724
9. Novais T, Dauphinot V, Krolak-Salmon P, Mouchoux C. How to explore the needs of informal caregivers of individuals with cognitive impairment in alzheimer’s disease or related diseases? A systematic review of quantitative and qualitative studies. BMC Geriatr. 2017;17(1):86. doi:10.1186/s12877-017-0481-9
10. O’Rourke N, Kupferschmidt AL, Claxton A, Smith JZ, Chappell N, Beattie BL. Psychological resilience predicts depressive symptoms among spouses of persons with alzheimer disease over time. Aging Ment Health. 2010;14(8):984–993. doi:10.1080/13607863.2010.501063
11. Gusi N, Prieto J, Madruga M, Garcia JM, Gonzalez-Guerrero JL. Health-related quality of life and fitness of the caregiver of patient with dementia. Med Sci Sports Exerc. 2009;41(6):1182–1187. doi:10.1249/MSS.0b013e3181951314
12. Mitchell LA, Hirdes J, Poss JW, Slegers-Boyd C, Caldarelli H, Martin L. Informal caregivers of clients with neurological conditions: profiles, patterns and risk factors for distress from a home care prevalence study. BMC Health Serv Res. 2015;15(1):350. doi:10.1186/s12913-015-1010-1
13. Cherry MG, Salmon P, Dickson JM, Powell D, Sikdar S, Ablett J. Factors influencing the resilience of carers of individuals with dementia. Rev Clin Gerontol. 2013;23(4):251–266. doi:10.1017/S0959259813000130
14. Joling KJ, Windle G, Dröes R, et al. Factors of resilience in informal caregivers of people with dementia from integrative international data analysis. Dement Geriatr Cogn Disord. 2016;42(3–4):198–214. doi:10.1159/000449131
15. Monteiro AMF, Santos RL, Kimura N, Baptista MAT, Dourado MCN. Coping strategies among caregivers of people with alzheimer disease: a systematic review. Trends Psychiatry Psychother. 2018;40(3):258–268. doi:10.1590/2237-6089-2017-0065
16. Wilks SE, Croom B. Perceived stress and resilience in alzheimer’s disease caregivers: testing moderation and mediation models of social support. Aging Ment Health. 2008;12(3):357–365. doi:10.1080/13607860801933323
17. Dias R, Santos RL, Sousa MFBD. Resilience of caregivers of people with dementia: a systematic review of biological and psychosocial determinants. Trends Psychiatry Psychother. 2015;37(1):12–19. doi:10.1590/2237-6089-2014-0032
18. Dias R, Simões-Neto JP, Santos RL, et al. Caregivers’ resilience is independent from the clinical symptoms of dementia. Arq Neuropsiquiatr. 2016;74(12):967–973. doi:10.1590/0004-282x20160162
19. Trapp SK, Perrin PB, Aggarwal R, et al. Personal strengths and health related quality of life in dementia caregivers from latin america. Behav Neurol. 2015;2015.
20. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. Springer publishing company; 1984.
21. Rayle AD. Mattering to others: implications for the counseling relationship. J Couns Dev. 2006;84(4):483–487. doi:10.1002/j.1556-6678.2006.tb00432.x
22. Garity J. Caring for a family member with alzheimer’s disease: coping with caregiver burden post-nursing home placement. J Gerontol Nurs. 2006;32(6):39–48. doi:10.3928/00989134-20060601-07
23. Fernández-Lansac V, López MC, Cáceres R, Rodríguez-Poyo M. Resiliencia en cuidadores de personas con demencia: estudio preliminar. Rev Esp Geriatr Geronto. 2012;47(3):102–109. doi:10.1016/j.regg.2011.11.004
24. O’Dwyer S, Moyle W, Van Wyk S. Suicidal ideation and resilience in family carers of people with dementia: a pilot qualitative study. Aging Ment Health. 2013;17(6):753–760. doi:10.1080/13607863.2013.789001
25. Gaugler JE, Kane RL, Newcomer R. Resilience and transitions from dementia caregiving. J Gerontol B Psychol Sci Soc Sci. 2007;62(1):P38–P44. doi:10.1093/geronb/62.1.P38
26. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185(12):914–919. doi:10.1001/jama.1963.03060120024016
27. Cruz AJ. El índice de katz. Rev Esp Geriatr Gerontol. 1991;26(5):338–348.
28. Reisberg B, Ferris SH, de Leon MJ, Crook T. The global deterioration scale for assessment of primary degenerative dementia. Am J Psychiatry. 1982.
29. Cacabelos R. Neurobiología y genética molecular de la enfermedad de alzheimer: marcadores diagnóticos y terapéutica. Med Clin. 1990;95:502–516.
30. Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The neuropsychiatric inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44(12):2308. doi:10.1212/WNL.44.12.2308
31. Boada M, Cejudo JC, Tàrraga L, López OL, Kaufer D. Neuropsychiatric inventory questionnaire (NPI-Q): validación española de una forma abreviada del neuropsychiatric inventory (NPI). Neurología. 2002;17(6):317–323.
32. Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64(2):258–266. doi:10.1097/00006842-200203000-00008
33. Montalban SR, Vives AC, Garcia-Garcia M. Validation of the spanish version of the PHQ-15 questionnaire for the evaluation of physical symptoms in patients with depression and/or anxiety disorders: DEPRE-SOMA study. Actas Esp Psiquiatr. 2010;38(6):345–357.
34. Beck AT, Steer RA, Brown GK. Beck depression inventory-II. San Antonio. 1996;78(2):490–498.
35. Sanz J, Navarro ME, Vázquez C. Adaptación española del inventario para la depresión de beck-II (BDI-II): 1. propiedades psicométricas en estudiantes universitarios. Anál Modif Conducta. 2003;29(124):239–288.
36. Goldberg D, Bridges K, Duncan-Jones P, Grayson D. Detecting anxiety and depression in general medical settings. BMJ. 1988;297(6653):897–899. doi:10.1136/bmj.297.6653.897
37. Montón C, Pérez Echeverría MJ, Campos R, García Campayo J, Lobo A. Escalas de ansiedad y depresión de goldberg: una guía de entrevista eficaz para la detección del malestar psíquico. Aten Primaria. 1993;345–349.
38. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649–655. doi:10.1093/geront/20.6.649
39. Martın M, Salvadó I, Nadal S, et al. Adaptación para nuestro medio de la escala de sobrecarga del cuidador (caregiver burden interview) de zarit. Rev Gerontol. 1996;6:338–346.
40. Rosenberg M. Rosenberg self-esteem scale (SES). Soc Adolesc Self Image. 1965.
41. Vázquez-Morejón Jiménez R, Jiménez García-Bóveda R, Vázquez Morejón AJ. Escala de autoestima de rosenberg: fiabilidad y validez en población clínica española. Apunt Psicol. 2004;22(2):247–255.
42. Carver CS. You want to measure coping but your protocol’s too long: consider the brief cope. Int J Behav Med. 1997;4(1):92. doi:10.1207/s15327558ijbm0401_6
43. Moran C, Landero R, González MT. COPE-28: a psychometric analysis of the spanish version of the brief COPE. Univ Psychol. 2010;9(2):543–552.
44. Reich M, Costa-Ball CD, Remor E. Estudio de las propiedades psicométricas del brief COPE para una muestra de mujeres uruguayas. Av En Psicol Latinoam. 2016;34(3):615–636. doi:10.12804/apl34.3.2016.13
45. Connor KM, Davidson JR. Development of a new resilience scale: the Connor‐Davidson resilience scale (CD‐RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
46. Crespo M, Fernández-Lansac V, Soberón C. Spanish version of the CDRISC resilience scale for chronic stress situations. behavioral psychology. Psicol Conductual. 2014;22:219–238.
47. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32(6):705–714. doi:10.1016/0277-9536(91)90150-B
48. De la Revilla L, Luna J, Bailón E, Medina I. Validación del cuestionario MOS de apoyo social en atención primaria. Med Fam. 2005;6(1):10–18.
49. McHorney CA, Ware JE, Raczek AE. The MOS 36-item short-form health survey (SF-36): II. psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31(3):247. doi:10.1097/00005650-199303000-00006
50. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
51. Alonso J, Prieto L, Antó JM. La versión española del SF-36 health survey (cuestionario de salud SF-36): un instrumento para la medida de los resultados clínicos. Med Clin. 1995;104(20):771–776.
52. Crespo M, Fernández-Lansac V. Resiliencia en cuidadores familiares de personas mayores dependientes. An Psicol. 2015;31(1):19–27.
53. Clay OJ, Roth DL, Wadley VG, Haley WE. Changes in social support and their impact on psychosocial outcome over a 5‐year period for african american and white dementia caregivers. Int J Geriatr Psychiatry. 2008;23(8):857–862. doi:10.1002/gps.1996
54. Rohr MK, Wagner J, Lang FR. Effects of personality on the transition into caregiving. Psychol Aging. 2013;28(3):692. doi:10.1037/a0034133
55. Rosa R. Caregivers’ resilience in mild and moderate alzheimer’s disease. Aging Ment Health. 2018;1–9.
56. Pinquart M, Sörensen S. Differences between caregivers and noncaregivers in psychological health and physical health: a meta-analysis. Psychol Aging. 2003;18(2):250. doi:10.1037/0882-7974.18.2.250
57. Deist M, Greeff AP. Living with a parent with dementia: a family resilience study. Dementia. 2017;16(1):126–141. doi:10.1177/1471301215621853
58. Pessotti CFC, Fonseca LC, Tedrus GMDAS, Laloni DT. Family caregivers of elderly with dementia relationship between religiosity, resilience, quality of life and burden. Dement Neuropsychol. 2018;12(4):408–414. doi:10.1590/1980-57642018dn12-040011
59. Contador I, Fernández-Calvo B, Palenzuela DL, Miguéis S, Ramos F. Prediction of burden in family caregivers of patients with dementia: a perspective of optimism based on generalized expectancies of control. Aging Ment Health. 2012;16(6):675–682. doi:10.1080/13607863.2012.684666
60. Violeta F-L, María L. Resiliencia, personalidad resistente y crecimiento en cuidadores de personas con demencia en el entorno familiar: una revisión. Clin Salud. 2011;22(1):21–40. doi:10.5093/cl2011v22n1a2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.