")
Back to Journals » Clinical Interventions in Aging » Volume 14
Understanding experiences of patients and family caregivers in the Mayo Clinic Care Transitions program: a qualitative study
Authors Takahashi PY, Finnie DM, Quigg SM, Borkenhagen LS, Kumbamu A, Kimeu AK, Griffin JM
Received 14 August 2018
Accepted for publication 10 October 2018
Published 19 December 2018 Volume 2019:14 Pages 17—25
DOI https://doi.org/10.2147/CIA.S183893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Paul Y Takahashi,1 Dawn M Finnie,2 Stephanie M Quigg,1 Lynn S Borkenhagen,1 Ashok Kumbamu,2 Ashley K Kimeu,1 Joan M Griffin2,3
1Department of Internal Medicine, Division of Primary Care Internal Medicine, Mayo Clinic, Rochester, MN, USA; 2Robert D and Patricia E Kern Center for Science of Health Care Delivery, Mayo Clinic, Rochester, MN, USA; 3Department of Health Science Research, Division of Health Care Policy and Research, Mayo Clinic, Rochester, MN, USA
Background: Care transitions programs are increasingly used to improve care and reduce re-admission of patients after hospitalization. To learn from the experience of patients who have participated in the Mayo Clinic Care Transitions (MCCT) program and to understand the patient experience, we sought perspectives of patients, caregivers, and providers who worked with participants of the MCCT program.
Methods: Investigators interviewed 17 patients and nine of their caregivers about their experience with the MCCT program. Eight health care providers described provider experiences with the MCCT program. Data from semistructured interviews were audio recorded, transcribed, and evaluated through content analysis. Inductive coding methods were used to elicit themes about patient experience with the MCCT program.
Results: Patients, caregivers, and providers emphasized that the MCCT program prevented hospitalizations and contributed to the health and quality of life of participants. All three stakeholder groups emphasized the value of the home visit and provision of the visit on a patient’s “home turf” as central to the program. Patients appreciated speaking to a provider without the stress and exertion of a trip to the clinic. Caregivers appreciated improved communication provided in the home visit and felt that home visits gave them peace of mind. Patients, caregivers, and providers also identified the need for improved phone triage and communication.
Conclusion: Patients, caregivers, and providers acknowledged the care transitions problem and emphasized the benefits of seeing patients on their home turf rather than in an office visit. This qualitative study of patient, caregiver, and provider experiences further validates the importance of the MCCT program.
Keywords: geriatrics, home care, program evaluation, nurse practitioner, hospitalization
Background
Patients and family caregivers often face difficult issues following a hospitalization.1 Many have changes in medication regimens2,3 or have medical conditions with complex care routines.4 Health care systems have begun to pay closer attention to this transition period5 through the use of health coaches,6 standard hospital dismissals,7 or nurse practitioners (NPs) to assist patients.8 Patients must prepare for the physical challenges of going home from the hospital and the need to organize and plan for upcoming appointments in the medical health care system.9 Our practice started the Mayo Clinic Care Transitions (MCCT) program to assist with hospital aftercare for high-risk patients.10–12 By using a model in which a NP conducted home visits, we found a higher 30-day re-admission rate for control patients (20.1%) than MCCT patients (12.4%), with a 7.7% absolute reduction (P=0.002).12
Even with significant reduction in re-admission rates, acceptance of the program by patients and providers is critical for program sustainability and success. In one population of patients over 65 with cognitive impairment, investigators observed that patients and their caregivers desired information about posthospital needs and illness.13 They ascribed importance of care coordination for primary care communication and appointments and valued the importance of the family or friend caregiver experience.13 To better understand the experience of our patient population, we sought to evaluate the MCCT program’s strengths and weaknesses from the perspectives of the patients, their caregivers, and their health care providers. Although similar to other programs based on a home visit by NPs,8 our program differs from others described in the literature because of our patient population and the intensity of visits. Thus, the experiences of a care transitions program are unclear regarding stakeholders when patients are enrolled for shorter periods and when the stakeholders include patients with multiple morbidities. Our goal was to understand the experiences of patients and caregivers who currently or recently were in the MCCT program and to apply this knowledge to improve the clinical program. To fully explore these experiences, we conducted a qualitative study with patients and caregivers, as well as health care providers.
Methods
Care transitions program
The MCCT program has been described previously.12 This program is staffed by advanced practice registered nurses (APRNs). To be a licensed APRN, a person must be an NP with a graduate degree in nursing and have completed 2,080 hours of supervised or collaborative practice.14
Patients enroll in the MCCT program on the basis of their scores on the Elder Risk Assessment Index (ERAI), which stratifies for risk of hospitalization.15 Among older patients, scores greater than 16 indicate that the top 10% is at risk for hospitalization and an emergency department visit.15 Patients are initially approached in the hospital by a registered nurse (RN) for possible enrollment in the MCCT program. After a patient’s hospital dismissal, an MCCT-affiliated NP evaluates the patient at home within five business days. The NP performs a comprehensive geriatric assessment, including medication reconciliation, evaluation of community needs, an action plan for acute issues, and long-term care plans for chronic health conditions. The patient is subsequently either seen or called at least once a week for 30 or more days. The total number of contacts, by phone or in person, varies depending on the length of program enrollment and the complexity, with all participants receiving a minimum of 4. Approximately six visits are made either by phone or face to face. Patients or their caregivers maintain phone access with the primary care team and are dismissed from the MCCT program when their medical condition stabilizes, as determined by the NP and the patient’s geriatrician.
Patient population
The initial estimate for patient accrual before initiation of the study was 18 patients based on the general numbers of patients in the program. Patients eligible for the present study had ERAI scores exceeding 16, had their first home visit of the MCCT program between January 9 and August 31, 2015, and had completed the program. All patients who met inclusion criteria were sent a letter asking whether they would participate in a study about the MCCT. The patients who returned signed consent forms were contacted by the study coordinator to set up an interview. Patients were excluded from the study if they were unable to provide informed consent, did not sign the form for the Health Insurance Portability and Accountability Act requirements, or did not have a proxy to provide informed consent. Caregivers of eligible patients who gave consent were also qualified for participation. The patients identified their own caregivers for participation.
Health care providers involved in the MCCT were asked to participate in this study. The providers, including medical doctors, RNs, and the NPs engaged in the program, were contacted through email. The medical doctors could have been the primary physician of the participants prior to the study. The RNs and NPs were staff who worked exclusively with MCCT. The Mayo Clinic Institutional Review Board approved the study protocol, informed consent, and interview guides. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.16
Qualitative data collection
In-depth telephone interviews with 17 study-eligible patients were conducted over 6 months (interviews were conducted from March 12, 2015, through September 29, 2015). During nine patient interviews, caregivers participated in the interview alongside the patients; sometimes, the caregiver responded with the patient to the same question and sometimes responded to questions directed specifically to the caregiver. Because caregivers, often familial, play an important role in the care of these frail, complex patients, particularly during times of care transition,5,17 we felt that it was appropriate to include their voice in this conversation. Although they were not the focus of this study, these caregivers provide valuable context about the patient experience during and after hospitalization as well as experience with the MCCT program. The iterative interview process allowed the research team to fully explore patient and caregiver experiences. This study followed the standards for reporting qualitative research guidelines.18
Health care providers were interviewed during the same time frame as patients and caregivers but were interviewed during a telephone call at a time convenient for the provider. Interviews were conducted by two members of the research team with expertise in qualitative methods (DMF and SMQ) using a semistructured interview guide. Interviews ranged from 13 to 50 minutes for patients and caregivers and from 18 to 44 minutes for providers. All interviews were audio recorded, transcribed, de-identified, and stored on a secure server.
Qualitative analysis
Members of the research team (DMF and SMQ) used a phenomenologic approach to analyze and understand the experience of patients in the MCCT program, followed by a thematic content analysis to analyze the final transcripts. This approach involved reading all transcripts to achieve immersion in the transcript data and to obtain a sense of the data as a whole.19 Transcripts were read word for word to derive themes that captured key thoughts or concepts from the data.20,21 Themes were then organized into codes. A code book was developed on the basis of these coding schemes, and definitions were applied to each code by researchers. These themes were applied back to the transcripts, and line-by-line inductive coding was used to structure data thematically. This approach was an interpretive process whereby themes were identified through review of the data to elicit common themes without generating theory. The approach is common for qualitative interview data derived from the health care research. Knowledge generated from content analysis was based on the patient, caregiver, and provider perspectives about their experiences with the MCCT program.
The team’s two qualitative researchers (DMF and SMQ) each coded all data to ensure that the open coding was consistent and reproducible (thereby improving reliability). Analytical software for the qualitative data (NVivo 10; QSR International Pty Ltd., Doncaster, VIC, Australia) provided structure to the coding and the data to ensure proper coding. This software provided an audit trail for decisions made on coding throughout the process. The team used triangulation of data from the patients, caregivers, and providers to ensure consistency of the themes, thus improving validity. The individual experience of the patient was the primary information source; however, experiences of caregivers and providers were considered. We also used investigator triangulation of the primary analysis team, with two analysts versed in qualitative techniques but not related to the MCCT program.
Sampling and recruitment of patients and caregivers
Of 91 patients who met the eligibility criteria and were contacted to participate, 55 did not respond, 15 stated that they were not interested, and three returned the signed consent after the target accrual was met. Eighteen of the 91 patients sent invitation letters back with signed consent forms, indicating their interest in study participation. One patient later declined to be interviewed because of time constraints. Thus, 17 patients were interviewed.
Sampling and recruitment providers
Fifteen invitations were sent through email between March 5, 2015, and June 24, 2015, to health care providers of the MCCT patients. Of the 15 recipients, eight gave verbal consent to participate and completed a qualitative interview. For provider interviews, two physicians, two advanced practice providers, and four RNs participated.
Results
Patient cohort
Seventeen patients were recruited for the study (10 men and seven women). Median (range) overall age was 82 (60–95) years. Median (range) ERAI score was 18 (16–21). As designed, the sample was at high risk for hospitalization.15 Among the patients, 12 patients (71%) had heart failure and five (29%) had COPD. Nine patients (53%) had caregivers who were interviewed.
The home visit
The inherent value of patients being at home for the care visits was consistent among the three groups. One patient referred to this as being on home turf. Patients and caregivers valued the home visit with feeling more comfortable conversing about their needs in their own environment. It gave them freedom to talk about their concerns and situation. They felt that NPs took the time to understand their needs. Medication discussions were important to patients, caregivers, and providers and allowed NPs to understand medication issues that may not be discussed in an office visit. Patients and NPs discussed diet and food. The ability to ask specific questions about foods that were in their cupboards was particularly valuable. The NPs provided patients with education or information that the patients felt they did not get while in the hospital or were too confused or overwhelmed to absorb (Boxes 1 and S1).
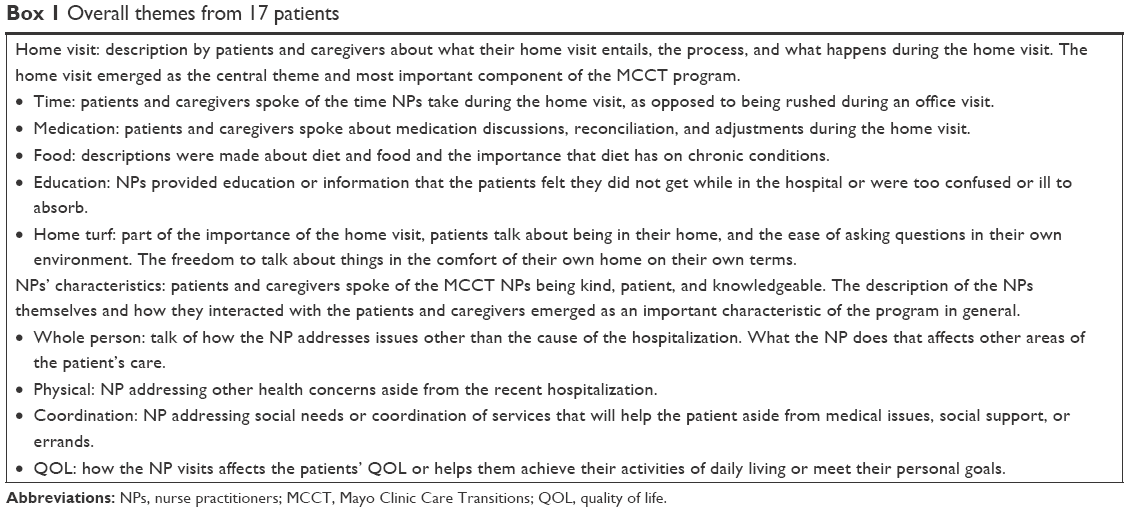 | Box 1 Overall themes from 17 patients |
Patient 4 commented, “Well, I think I feel more comfortable and it gives me the opportunity to ask questions back. You know, a lot of times I have, ah, questions about something that I don’t fully understand, and I can enter that into the conversation and it’s just, it’s more I think the conversation’s more complete when we’re together and talking. You gotta have feedback, both ways, and I don’t do that on the telephone.” Patient 14 noted, “I think that I’m more relaxed in my own home, and I can think better.”
The providers, and specifically the NPs, also described how invaluable it was to be able to visibly see the patients’ home environment; talk to them on their own terms; and identify environmental, social, or medical factors that may not be related to their recent hospitalization but are important to their health and recovery. The providers felt that the home visit was more personal, gave the patients more opportunity to ask questions, and helped them understand their situation. Following is a comment from Provider 101.
Yeah, that it’s invaluable that they can go out there and, for instance, they see [the patients] within 2 days. They have a hospital dismissal so they can take a look at their dismissal summary, and all like the list of their medications, and they can go in their house and pull all their pill bottles and say, “These don’t match”. Or the patient may say, “Well I’m taking my husband’s.” Or, “I can only afford ___ and I’m only taking it every other day.” Things that you wouldn’t pick up on. Or they could say, “Oh, I see you have a throw rug there on your floor, that’s not a good idea,” or things like, look in the bathroom, and see, “Maybe some safety bars would be helpful in your bathroom”. And they go through all their screening tools. I’d like to think an RN could probably do that and help them with their visit, but, yeah, I think that the time that they spend in the home in their first visit, maybe 2 hours in the home, a really thorough exam, well, more can get pulled out of that instead of a 15-minute visit in the office.
Patients and caregivers spoke about the characteristics of the NP and the patient-centered care provided, as well as the ability to navigate the health and non-health-related issues that affect the quality of life and care of the whole person (Box 2). The comfort and connection built by an NP visiting a patient’s home are the key components of that home visit. Patient 10 reported,
 | Box 2 Themes from nine caregivers of patients |
Well it’s the fact that they, that they come to the home … We don’t have to make the trip to the clinic. When they come to the home, they make us feel like we’re important … They’re very concerned about our welfare.
The convenience of being at home and not having to travel, especially given the challenging health conditions the patients face, was also discussed frequently. Patients reported challenges with getting to and from appointments. Physically, travel to the outpatient clinic was taxing and difficult, particularly after a hospital stay. Participation in the MCCT allowed patients to avoid travel. Caregiver 18 said,
So, um, I thought there the convenience of [an NP] coming in ’cause there’s no way my dad would have been able to get into a car and then tolerate driving down there, finding, you know, a parking space, being transported around. I mean, with the combination of his heart failure and his lungs, you know, he’s a double-whammy so to speak, so it makes it hard.
In an unexpected benefit of the home visit, patients were able to forego telephone follow-up calls because they would have issues addressed by their NPs. Many patients and caregivers reported issues before MCCT participation of having to wait extended periods on the telephone triage system and being redirected frequently when they called. Similarly, patients reported preferring the face-to-face conversation of the home visit because they were unable to hear well (n=6) or to hold the phone receiver because of arthritis (n=1); the timing of the phone calls also was inconvenient (n=3). As Patient 4 described,
Well, I think it’s, for 1 thing for me, I’m so hard of hearing, I have trouble on the telephone. And I’m doing fairly well with you right now, but a lot of times, when they call in, I don’t even know who I’m talking to and it seems like they all talk too fast for people that are hard of hearing.
The NP role
Patients and caregivers described the NP as being knowledgeable, a good listener, and a systems navigator. The patients also stated that the NP respected people’s lives. For example, Patient 12 said,
Well, she seemed very interested in what was going on with me and my family, if anything was botherin’ me, what questions I had for her, and seemed to always listen really well to anything I was talking about … Yeah, it sounded like she had really read probably all about me from Mayo papers and so forth, so she seemed to be very knowledgeable about almost everything that has happened with my health.
Care of the whole person
Patients and caregivers described the MCCT care as treating the whole person, having a connection to everything they need, and being able to address their needs and goals. They described this care as going beyond the posthospital recovery and addressing other needs, both medical and nonmedical. Some study participants described the improvement to their quality of life and their ability to transition back to their normal life. Providers described being able to improve the quality of life of some patients and, for others, keeping the patient out of the hospital and addressing end-of-life needs.
MCCT program evaluation
The patients and caregivers described challenges with the care team phone triage system. The providers expressed their passion for taking care of the care transition program population. They also voiced the advantages of end-of-life discussions and palliative care (Box 3).
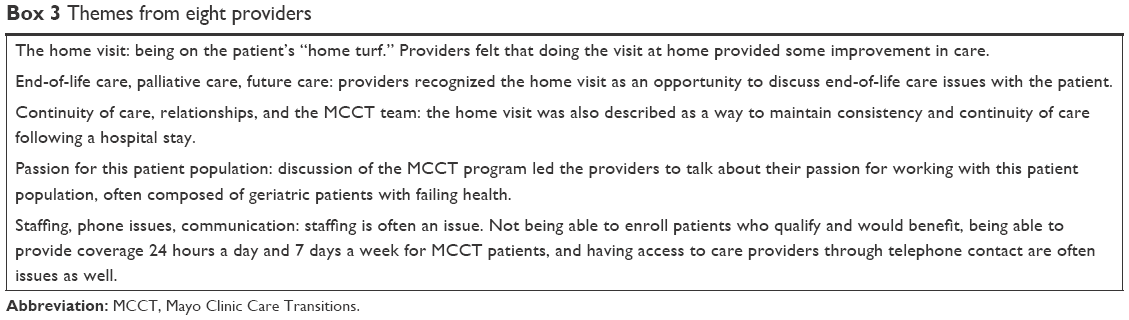 | Box 3 Themes from eight providers |
Discussion
In this qualitative study of 17 patients, nine caregivers, and eight providers, we learned the importance of providing care on the home turf and the comfort of visits with the NP in the home. For the ill patients in this transition population, being comfortable meant that they talked more openly at home. Caregivers were able to communicate with the NP directly. Other studies have evaluated similar high-risk populations and sought some evaluation of the patient’s experience. Our study focused in the community, whereas other studies sought input from patients in residential facilities or Programs of All-Inclusive Care for the Elderly after hospital dismissal.22
One identified barrier involved the phone triage system and the difficulty of getting access to care when they needed it. The providers mentioned the importance of the telephone in the communication challenge. Patients, caregivers, and providers all identified that the MCCT program helped to reduce the need to call the phone triage. They also mentioned that home visits eliminated the burden of the journey to the medical clinic. Difficulty in communication with the telephone was the biggest limitation within the program. Some patients could not use the telephone because they had hearing loss. Different patient groups experience different feelings after hospital dismissal. Among cancer patients and caregiver groups, the patients expressed themes of timely care, issues with ongoing concerns, needing to regain control, and appreciating care transitions.23 Among patients with heart failure, aspects that continue to be important are an understanding of heart failure, how to work with it, getting control of the situation, and end-of-life care.24 There is comfort of communicating at home that is not seen in the hospital or office setting.
Patients provided positive comments on the professionalism and help of the NPs and the RNs. They commented on the role of the NP as the center of the care transitions team. These comments reinforce the importance of both the NP as the center of the medical home after hospital discharge and the use of medical teams.25 Previous studies have emphasized the importance of medical care after a hospital stay. In a Department of Veterans Affairs study of care transitions, patients felt that medication education, home health nursing, prompt visits, and improved communication helped prevent hospital readmission.26 Similarly, the importance of continuity of care with a care transitions team was emphasized in a study from UK,27 and other studies have shown that NPs are seen positively by patients in other care transitions programs.13 We, too, found that the link from patient to NP was strong and important in comfort, knowledge, and communication.
Consistent with previous research, the caregivers in our study reported the importance of communication and relationships with the NPs. In previous studies, caregivers have reported the need to have their situation understood, to be involved with the process, to obtain practical information, to be in harmony with formal caregivers, and to have both personal time and emotional readiness.28 Communication between patients and the medical team or discharge team has also been reported as important.29 In our study, the caregivers felt that they had better communication and some consistency with the NPs. This natural communication is one method to fostering improved care. Caregivers and patients were empowered to provide and use self-assessment of medical conditions, which was also an important concept to have them involved with the care plan.
The providers confirmed many of the feelings and sentiments of both the patients and the caregivers. They appreciated the importance of the home as a center of providing care. They had a sense that lowering the barriers of access might help to provide better medical care. The providers who work in the MCCT program reported being committed to the population generally and to the care for patients and caregivers. Similar to patients and caregivers, providers in other qualitative studies have expressed the importance of communication and the need for education as central to successful care transitions.30
There are many practical implications from our research. Placing patients at the center of care and meeting them at their own home have a powerful effect for both patient and caregiver. Meeting at someone’s home may take a relationship to a different level and may improve the satisfaction of the patient. For many patients with multimorbidities who were dismissed from the hospital, the home visit from the MCCT enhances care beyond medication reconciliation, medical action plans, and safety evaluations.
This qualitative study has weaknesses and strengths. We triangulated the assessment of the program through three different groups and found similar responses. Our goal was to describe a broad set of experiences until we found commonalities across those experiences. Nevertheless, a possibility is that the MCCT patients who participated in the study had a different set of experiences than the MCCT patients who did not participate; thus, the possibility of volunteer bias exists. This is particularly important for this older, frail population, where persons with severe chronic illness may not have participated. In a similar manner, the providers who responded could be different from the general provider population. A volunteer bias may have existed for the providers as well as the patients. In addition, recall bias is a possible factor in the study. Participants were enrolled in the study after their enrollment in the program. There is a possibility of social desirability bias from the participants. In another limitation, the caregivers were present with the participants, which could influence the answers of the caregivers. A study that specifically assesses caregiver experiences may be appropriate in the future. Despite these weaknesses, the experiences of patients, caregivers, and providers shed light on the importance of home visits after hospital dismissal. In particular, they reinforce the utility of the home as the center of the health care visit.
Conclusion
We observed that patients, caregivers, and providers embraced the MCCT program and found aspects of the program valuable. Central to this care was the importance of seeing the patient in the home environment, as opposed to the office. Patients reported the comfort of talking in the home and felt that fewer barriers to receiving care occurred with home visits than with clinic visits, especially for patients with physical difficulties or hearing problems. As medical complexity increases, providers and caregivers value the ability to spend time in an environment that is relaxing for patients. Communication and patient-centered care were important in this venue. Possibly, the home is a better place than the office to communicate with patients and caregivers.
Abbreviations
APNP, advanced practice registered nurse; ERAI, Elder Risk Assessment Index; MCCT, Mayo Clinic Care Transitions; NP, nurse practitioner; RN, registered nurse.
Acknowledgments
All authors contributed toward data analysis, drafting, and revising the paper and agree to be accountable for all aspects of the work. Portions of the manuscript were published in abstract form in J Am Geriatr Soc. 2016;64:S68.
Disclosure
PYT serves on a medical advisory board for Axiall, LLC. The other authors report no conflicts of interest in this work.
References
Makaryus AN, Friedman EA. Patients’ understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80(8):991–994. | ||
Cochrane RA, Mandal AR, Ledger-Scott M, Walker R. Changes in drug treatment after discharge from hospital in geriatric patients. BMJ. 1992;305(6855):694–696. | ||
Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429. | ||
Krumholz HM. Post-hospital syndrome – an acquired, transient condition of generalized risk. N Engl J Med. 2013;368(2):100–102. | ||
Coleman EA, Smith JD, Frank JC, Min SJ, Parry C, Kramer AM. Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention. J Am Geriatr Soc. 2004;52(11):1817–1825. | ||
Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828. | ||
Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187. | ||
Naylor MD, Brooten DA, Campbell RL, Maislin G, Mccauley KM, Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc. 2004;52(5):675–684. | ||
Neiterman E, Wodchis WP, Bourgeault IL. Experiences of older adults in transition from hospital to community. Can J Aging. 2015;34(1):90–99. | ||
Syed H, Chen CJ, Crane S. Hospital readmission and the value of a care transitions program for the elderly: a retrospective cohort study. Primary Health Care: Open Access. 2012;2:113. | ||
Takahashi PY, Haas LR, Quigg SM, et al. 30-day hospital readmission of older adults using care transitions after hospitalization: a pilot prospective cohort study. Clin Interv Aging. 2013;8:729–736. | ||
Takahashi PY, Naessens JM, Peterson SM, et al. Short-term and long-term effectiveness of a post-hospital care transitions program in an older, medically complex population. Health c (Amst). 2016;4(1):30–35. | ||
Bradway C, Trotta R, Bixby MB, et al. A qualitative analysis of an advanced practice nurse-directed transitional care model intervention. Gerontologist. 2012;52(3):394–407. | ||
Minnesota Board of Nursing [webpage on the Internet]. Advanced practice registered nurse (APRN) licensed general information. Available from: https://mn.gov/boards/nursing/advanced-practice/advanced-practice-registered-nurse-(aprn)-licensure-general-information/. Accessed October 4, 2018. | ||
Crane SJ, Tung EE, Hanson GJ, Cha S, Chaudhry R, Takahashi PY. Use of an electronic administrative database to identify older community dwelling adults at high-risk for hospitalization or emergency department visits: the elders risk assessment index. BMC Health Serv Res. 2010;10:338. | ||
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. | ||
Levine C, Halper D, Peist A, Gould DA. Bridging troubled waters: family caregivers, transitions, and long-term care. Health Aff (Millwood). 2010;29(1):116–124. | ||
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. | ||
Tesch R. Qualitative Research: Analysis Types and Software Tools. New York, NY: Falmer Press; 1995. | ||
Miles MB, Huberman M. Qualitative Data Analysis: An Expanded Source Book. 2nd ed. Thousand Oaks: Sage Publications; 1994. | ||
Morse J, Field PA. Qualitative Research Methods for Healthcare professionals. Thousand Oaks, CA: Sage Publications; 1995. | ||
Toles MP, Abbott KM, Hirschman KB, Naylor MD. Transitions in care among older adults receiving long-term services and supports. J Gerontol Nurs. 2012;38(11):40–47. | ||
Ang WH, Lang SP, Ang E, Lopez V. Transition journey from hospital to home in patients with cancer and their caregivers: a qualitative study. Support Care Cancer. 2016;24(10):4319–4326. | ||
Jones J, Nowels CT, Sudore R, Ahluwalia S, Bekelman DB. The future as a series of transitions: qualitative study of heart failure patients and their informal caregivers. J Gen Intern Med. 2015;30(2):176–182. | ||
Reckrey JM, Soriano TA, Hernandez CR, et al. The team approach to home-based primary care: restructuring care to meet individual, program, and system needs. J Am Geriatr Soc. 2015;63(2):358–364. | ||
Spehar AM, Campbell RR, Cherrie C. Seamless Care: Safe Patient Transitions From Hospital to Home. In: Kerm Henriksen, James B Battles, Eric S Marks, and David I Lewin, editors. Ft. Belvoir: Defense Technical Information Center; 2005. Available from: http://handle.dtic.mil/100.2/ADA433720. A ccessed November 21, 2018. | ||
Cowie L, Morgan M, White P, Gulliford M. Experience of continuity of care of patients with multiple long-term conditions in England. J Health Serv Res Policy. 2009;14(2):82–87. | ||
Giosa JL, Stolee P, Dupuis SL, Mock SE, Santi SM. An examination of family caregiver experiences during care transitions of older adults. Can J Aging. 2014;33(2):137–153. | ||
Chapin RK, Chandran D, Sergeant JF, Koenig TL. Hospital to community transitions for adults: discharge planners and community service providers’ perspectives. Soc Work Health Care. 2014;53(4):311–329. | ||
Fuji KT, Abbott AA, Norris JF. Exploring care transitions from patient, caregiver, and health-care provider perspectives. Clin Nurs Res. 2013;22(3):258–274. |
Supplementary material
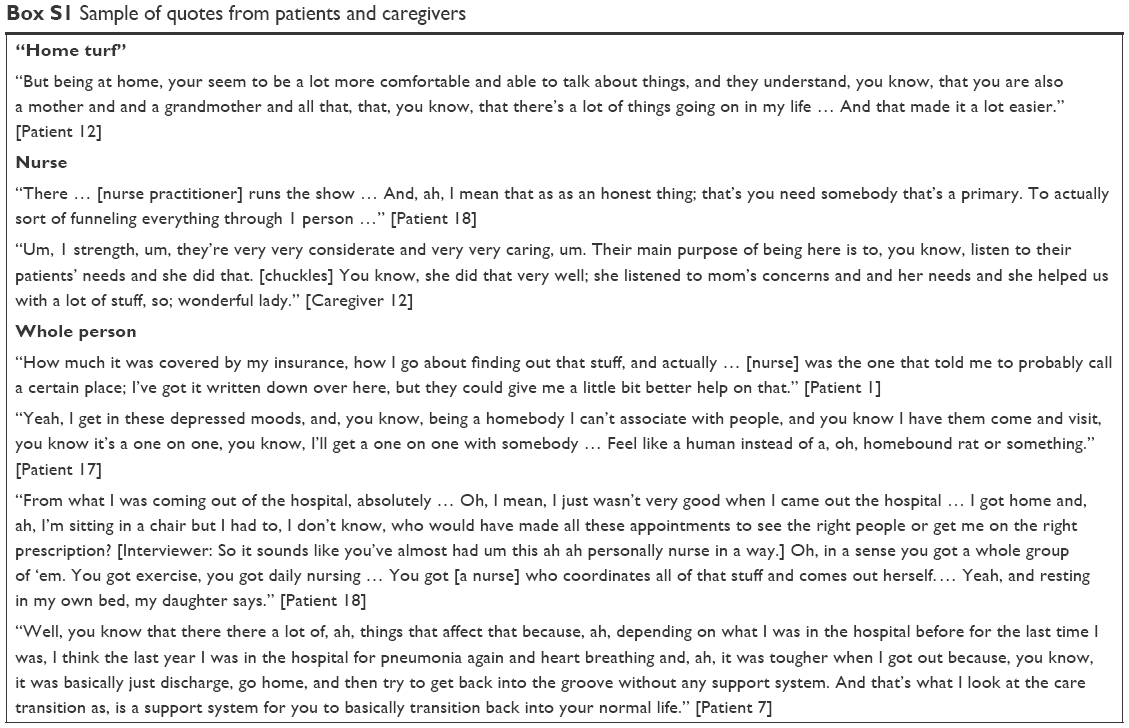 | Box S1 Sample of quotes from patients and caregivers |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.