")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Type 1 Diabetes Mellitus in Pediatric Patients and Its Impact on Relationships in the Family Environment
Authors Madrigal MA, López M, Sánchez A, Cao MJ, Castro MJ, Jiménez JM
Received 14 September 2020
Accepted for publication 29 October 2020
Published 15 December 2020 Volume 2020:13 Pages 4973—4980
DOI https://doi.org/10.2147/DMSO.S281949
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Miguel Angel Madrigal,1,2 María López,1 Alicia Sánchez,2 María José Cao,1 María José Castro,1 José María Jiménez1
1Faculty of Nursing, Universidad de Valladolid, Valladolid, Spain; 2Hospital Clínico Universitario de Valladolid, Valladolid, Spain
Correspondence: María López
Faculty of Nursing, Universidad de Valladolid, Avda Ramón y Cajal, Nº 7, Valladolid, Spain
Tel +34 983184056
Email [email protected]
Purpose: The aim of this study is to assess the impact of type 1 diabetes mellitus on family environment relationships, as well as the management and approach to this disease.
Patients and Methods: One hundred one children, 52.47% male and 47.52% female, with an average age of 8.55 ± 4.01 years, diagnosis of type 1 diabetes mellitus. Quantitative cross-sectional descriptive study was conducted using the validated questionnaires “Modified Diabetes Quality of Life” and “Questionnaire for the assessment of psychological impact in parents/guardians of diabetic children”.
Results: Most of the children (70.3% versus 29.7%) identified diabetes as unpleasant or not fun. The ≤ 5-year-olds expressed that they felt concerned about the consequences of being diabetic (8.1% by age group), as opposed to the 10-year-olds who did not feel concerned (85.1% by age group), P < 0.001. The family environment was affected in 98.1% (n=99) of the cases.
Conclusion: Self-care of type 1 diabetes mellitus in pediatric patients is a complex process that impacts the family environment and their relationship with their peers, especially for children under the age of 5. Fear, concern and insecurity were prevalent feelings in children suffering type 1 diabetes mellitus.
Keywords: chronic disease, adaptation, psychological, self-care, child health, psychology
Introduction
Type 1 diabetes mellitus (T1D) is one of the most remarkable health alterations in pediatric age, as it is one of the most common chronic diseases in childhood. Ineffective glycemic control can affect the growth and development of children and adolescents, and this is usually accompanied by acute and chronic complications that can impact their quality of life.1
A diagnosis of T1D leads to a significant change in the lifestyle of the child or adolescent and his/her family, associated with a situation of personal and family stress, whose impact on physical and mental health can be difficult to quantify.2
Parents experience high levels of stress and feelings of vulnerability.3 In this context, it is important that health professionals provide support tailored to the needs of each family in order to achieve psychological and medical benefits.4
The interventions conducted in these patients require tools that allow the objectivization of the actions performed,5 as well as the development of research that seeks the psychological benefit of pediatric patients diagnosed with T1D and their families.6
Healthcare professionals play an important role in T1D care when addressing sociodemographic and socioeconomic factors that influence diabetes therapies and programs.7
These issues make it essential to develop a questionnaire that includes aspects of disease management, including psychological coping and self-care capacity, partially adapting it to the pediatric patient.8–10 Due to the involvement of parents in the care of their children with T1D, it is necessary to identify their perspective in coping and managing the disease,11,12 including different aspects such as the resolution of complications13 and the correct daily follow-up of the treatment and care required.14
In pediatric healthcare, the dimensions of physical, emotional, and social healing need to be considered.15 The use of tools to quantify different aspects of the care, supervision and attention of parents, guardians and caregivers of children is very beneficial.16 The Spanish version of the Diabetes Quality of Life (DQOL), a validated tool in Spanish,8 has led to its choice over other questionnaires such as the Pediatric Quality of Life (PedsQL) to prevent cultural biases linked to translation.17
T1D has a direct impact on a child’s or adolescent’s daily life, as it affects their diet, physical activity, rest, academic performance and psychosocial environment; thus, health professionals play a key role in their care, support and health education.18 Self-management of diabetes by the pediatric patient and their environment is crucial. Some studies such as the one developed by Saoji et al reflect how barriers to self-management of T1D are associated with the quality of life of children and adolescents, and how the clinical setting can improve the life experience of these children and their families.14
Identifying psychosocial and quality of life issues in children with T1D and their parents will help health professionals in their psychosocial anamnesis and provide additional information to assist in the health approach.19 Improving the care of pediatric patients diagnosed with T1D and their families should be a goal for health personnel.20
The aim of this study is to assess the impact of type 1 diabetes mellitus on family environment relationships, as well as the management and approach to this disease.
Materials and Methods
Study Design
Quantitative cross-sectional descriptive study using the validated questionnaires “Modified Diabetes Quality of Life”,8–10 and “Questionnaire for the assessment of psychological impact in parents/guardians of diabetic children”.16
Study Sample
The study population is constituted by 250 children diagnosed with T1D in the health area of Valladolid in July 2018. We conducted a non-random consecutive sampling among patients diagnosed with T1D in the health area of Valladolid and obtained the voluntary participation of 101 children. Since they were minors, it was necessary to obtain prior informed consent from at least one of the parents.
Research Process
All children diagnosed with T1D and their parents were invited to participate in the study after receiving information about the purpose and content of the research. Informed parental approval and child consent were obtained prior to completion of the questionnaires.
The two questionnaires were conducted in pediatric nursing consultations at health centers from April to June 2019.
The questionnaire “Modified Diabetes Quality of Life”, consists of 10 close-ended questions, related to how to cope with the disease in order to assess quality of life and self-care capacity in pediatric patients diagnosed with diabetes.
The “Questionnaire for the assessment of psychological impact in parents/guardians of diabetic children” consists of 10 closed-ended questions that analyze the effects of taking care of a child diagnosed with T1D in the family environment.
Both questionnaires were complemented with the sociodemographic variables gender and age of the children studied. They were classified into the following age groups: ≤5 years, ≥6 years and <10 years, ≥10 years.
Both questionnaires were carried out in the presence of the parents/guardians of the diabetic children at all times. The questionnaire “Modified Diabetes Quality of Life” was specifically addressed to the children; the youngest ones needed the help of their parents since their reading and comprehension abilities were still not developed enough to answer the questions by themselves. The “Questionnaire for the assessment of psychological impact in parents/guardians of diabetic children” was only addressed to the parents/guardians of children diagnosed with diabetes to assess the impact of their child’s disease on the family environment and the care of their children.
The variables studied in the children were sociodemographic: age and gender, besides those related to the management and quality of life of the disease in children and parents.
Reproducibility or reliability was assessed by internal consistency (Cronbach’s alpha) and test-retest by Pearson’s correlation coefficient. The overall internal consistency of the “Modified Diabetes Quality of Life” questionnaire was 0.848 and the “Questionnaire for the assessment of psychological impact on parents/guardians of diabetic children” was 0.688.
Ethical Considerations
This study was approved by the Ethics Committee for Scientific Research in the Valladolid Este Health Area, which belongs to the Health Service of Castilla y León, in March 2019 (reference number: PI 19-1239) and this study complied with the Declaration of Helsinki.
Statistical Analysis
Data were analyzed using IBM SPSS v. 24.0 software. Quantitative variables that followed a normal distribution were summarized as means ± standard deviations (SD). Medians and ranges were recorded for non-Gaussian variables. Qualitative variables were summarized by number and as percentage of cases. The paired t-test or Wilcoxon rank test were used to study the differences between means over time, and ANOVA or the Kruskal–Wallis test to compare changes in variables in more than two categories. Significance was set at P<0.05.
Results
The study sample is composed by 101 children 53 males (52.47%) and 48 females (47.52%), with a mean age of 8.55 ± 4.01 years, females 8.22 ± 3.96 years and males 8.89 ± 4.06 years. The distribution of the sample is described in Table 1.
 |
Table 1 Distribution of the Study Sample |
Quality of Life
Regarding the coping and approach to the disease, most of the children (70.3% versus 29.7%) identified diabetes as something unpleasant or not fun: 86.5% of the ≤5-year-old group, 17.6% of the group between ≥6 years and <10 years, and 76.6% of the ≥10-year-old group P<0.001. Figure 1 shows the analysis of the responses to the questionnaire “Modified Diabetes Quality of Life” divided by age and gender groups.
 |
Figure 1 Analysis of the answers to the questionnaire “Modified Diabetes Quality of Life” divided by age and gender groups. *P<0.05 or **P<0.001 when comparing age groups. |
The 36.4% (n=64) of children did not feel concerned about the consequences of being diabetic, 30.7% (n=31) did not think about it, and 5.9% (n=6) were concerned. Analyzing the sample according to the classification by age group, the ≤5-year-olds expressed that they felt concerned (8.1% by age group) as opposed to the 10-year-olds who did not feel concerned (85.1% by age group). P<0.001. There were no significant gender differences, although the proportion of those who felt worried was greater in males than in females (7.5% versus 4.2%).
Regarding the severity of diabetes as a disease, 78.2% (n=79) of children responded that they did not think about it, 14.9% (n=15) considered it a serious disease, 5% (n=5) not serious and 2% (n=2) very serious. The group of ≤5-year-olds considered the disease very serious (5.4% by age group) and serious (27% by age group). Children over 10 years old answered that they did not think about it (87.2% by age group) followed by children from 6 to 10 years old (76.5% by age group). P=0.007.
A large percentage, 91.1% (n=92), said that there would be consequences of the disease in the future if they did not take care of themselves.
Three-quarters of the sample, 75.2% (n=76) responded that they were a little bit scared of having diabetes, seeing it as a punishment; 16.8% (n=17) were not scared and 7.9% (n=8) were scared. No significant differences were noted by gender, but there are differences by age group, the youngest of which responded that it did scare them (18.9% by age group) P<0.001.
Children diagnosed with diabetes did not find their relationships affected (87.1%. n=88) compared to those who stated that it did affect them (12.9%. n=13). No statistically significant differences by age group or gender were observed.
The 90.1% (n=91) of the children indicated that they could not follow a study plan similar to that of their classmates. There were statistically significant differences among age groups (P=0.03), with the youngest one answering that they could follow the same study program than the rest of their classmates (6.93%. N=7). On the other hand, in the group of 6–10 years old 16.83% (N=17) and 43.56% (n=44) of those over 10 years old answered that they could not follow the same study plan than the rest.
Diabetic children presented limitations in doing activities that others could do in a percentage of 79.2% (n=80). The 18.8%. (n=19) of them answered that they were never limited and 2% (n=2) answered that they were limited. No statistically significant differences by age or gender were observed.
Dietary compliance was assessed as part of treatment and good disease control. 62.4% (n=63) of the children responded that it was only partly, 33.7% (n=34) that it was, and 4% (n=4) that it was not. No statistically significant differences by age or gender were observed.
The 92.1% (n=93) did not consider that the use of insulin for the treatment of diabetes had harmful consequences for their health, while 7.9% (n=8) did. By age group, children ≤5 years old were the ones who mostly identified the harmful effects of insulin on their health (16.2% by age group). P<0.05.
Regarding the use of syringes and needles in the administration of insulin, it was considered neither difficult nor easy to do (56.4%. n=37), 34.7% (n=35) responded that it was relatively difficult to do, 5% (n=5) that it was very difficult and, lastly, that it was fairly easy to do 4% (n=4). The group of ≤5 years old answered that it was very difficult for them (10.8% by age group). P<0.001.
Assessment of Psychological Impact in Parents/Guardians of Diabetic Children
The “Questionnaire for the assessment of psychological impact in parents/guardians of diabetic children” reflected that the family environment was affected in 98.1% (n=99) of the cases. In 55.4% (n=56) of the cases, it affected their couple relationship, and in 94% (n=95) it had a direct impact in their work environment and social relations. The responses recorded by gender followed a homogeneous distribution without presenting any statistically significant differences.
The analysis by age group is presented in Figure 2. It was observed that the group of ≤5 years presented a greater dependence on care than the rest of the groups. In the group of ≥10 years, alterations in the family environment were more prevalent.
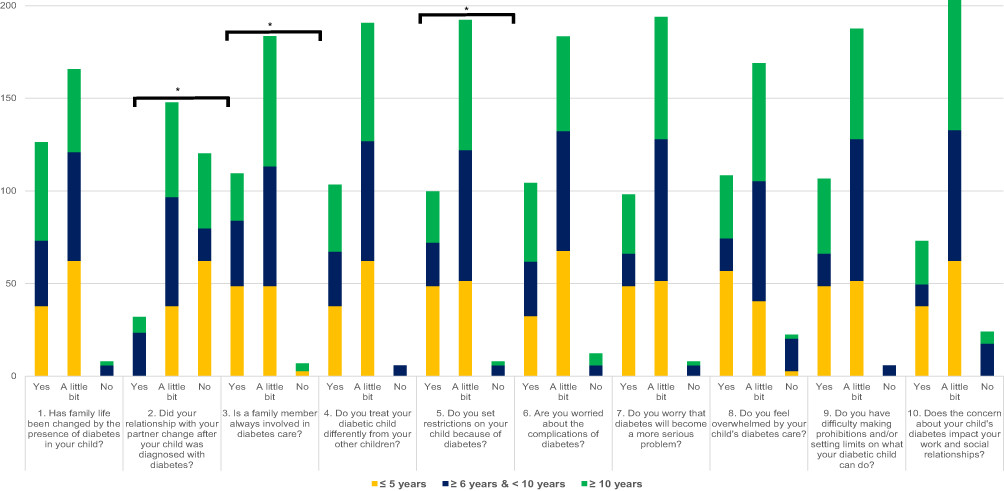 |
Figure 2 Assessment of psychological impact in parents/guardians of diabetic children by age groups. *P<0.05. |
Discussion
The proper management of T1D by children and parents is critical to achieve an effective disease control. Our study reflects the concern that both children and parents have about the best approach to the disease.
Children Facing T1D
T1D has a profound impact on the child’s environment and daily life. In our study, most of the children identified the disease as being unpleasant or unfunny: they were afraid of the disease, which they saw as a punishment, and believed that if they did not take care of themselves, the disease would have negative consequences for their health in the future. The ≤5-year-old group was the most concerned about the disease, considering it severe and declaring fear of its consequences. The cognitive ability of younger children to understand the chronicity and severity of the disease and the future perspective may favor this poor adaptation to T1D.21 Before that, the learning process leads to moments of doubt and embarrassment, with a clear dependence on their parents.22 The self-care process is a combination of knowledge and skills, in which children learn from their own experience, their parents and health professionals. As they grow up, their level of development and maturity increases, and so do their knowledge and skills, encouraging them to assume more responsibility for their self-care.23
For most children, T1D did not impact their relationship with other people, although it did have an impact on them in terms of following the same curriculum as their peers, and sometimes also limited them in certain activities. In this regard, the school environment is crucial to ensure that children feel safe.24 A positive environment is also important, including friendships, since they affect the management of the disease25 and leisure activities. T1D can be a barrier to physical activity, sometimes favouring sedentarism,26 and therefore translating in a negative impact on quality of life and metabolic control of the disease.27 Diet plays an essential role in glycemic control and the long-term consequences of diabetes,28 so it is essential that children learn to manage it properly. In this study, most of them reported that diet only helped them to comply partially with the treatment, while for the youngest it was not worthwhile to comply with the treatment with a proper diet.
Most of the children did not consider insulin as a treatment harmful to their health, except for the ≤5-year-old group. The majority of the sample indicated that using insulin syringes and needles were neither difficult nor easy, although the younger children did report that they found it difficult. Fear, anxiety and pain during insulin injections may be factors that complicate their proper management.29 Tasks related to blood glucose control may generate stress,30 although the study sample did not consider this type of healthcare to be difficult.
Parents Facing T1D
Parents of children with T1D revealed some psychological burden and stress, being the parents of patients ≤5 years old the ones who had more overload and stress. Family functioning had been modified for the parents by the new situation of having a child diagnosed with T1D. A child with T1D is dependent on his or her parents to receive proper treatment; they are responsible of supporting the child and carrying out the treatment.31
Most parents reported that they treated their diabetic child “a little bit” differently than the others. It is complex to establish a life that is as normal as possible for your child; this involves adjusting to daily diabetes management tasks and routines that benefit your child’s health and life.3
Parents were concerned about the complications of diabetes, along with the fact that the disease was becoming a more severe problem. They also noted that they were overwhelmed by the care of their child, especially the ≤5-year olds. This may be because as intensive insulin regimens become the standard of care for young people with T1D, the burdens on the routines and relationships of young people and their families also increase.30 In addition to psychological distress, it has been shown that symptoms of exhaustion are more common in parents of children with T1D than in parents of healthy children.31 The state of alertness and concern for the health of their child does not allow them to relax, which leads to fatigue.3
Drawing boundaries for their diabetic child was found challenging by most parents, combined with their concern about their child’s diabetes impacting on their work and social relationships. This is understandable as parents also need specific support to cope with the high levels of stress around their child’s T1D diagnosis.4 This can be complicated in adolescence, when the patients have to assume responsibility for most of their care, and discrepancies may arise with their parents and the proper management of T1D.32 In this context, health professionals should favor self-management skills in patients.33
By involving children in the decision-making process of their health care, they become more knowledgeable, thus facilitating and benefiting the work of health professionals. This is why specific interventions by medical staff are needed to encourage the active participation of children and their involvement in self-care.34
Among the limitations of this work is the lack of randomness of the analyzed sample, as well as the difficulty of communicating with the children, especially the younger ones, in some of the questions, in which the participation of the parents was required.
Conclusion
Managing T1D disease is a complex process, mainly in patients under 5 years of age, who have the greatest difficulty in self-care. The management of self-care associated with T1D was better in the older age groups.
T1D caused feelings of fear, worry and uncertainty not only among the children suffering from it, but also among their parents and guardians. The family environment was affected both personally and professionally.
Nurses should promote healthy styles and routines in the management of T1D to encourage self-care and minimize the negative consequences of the disease from childhood, involving also the family in the whole process.
Abbreviations
T1D, diabetes mellitus; DQOL, diabetes quality of life; PEDSQL, the pediatric quality of life.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fortins RF, Lacerda EMA, Silverio RNC, et al. Predictor factors of glycemic control in children and adolescents with type 1 diabetes mellitus treated at a referral service in Rio de Janeiro, Brazil. Diabetes Res Clin Pract. 2019;154:138–145. doi:10.1016/j.diabres.2019.05.027
2. Mills SA, Hofman PL, Jiang Y, et al. Health-related quality of life of Taranaki children with Type 1 diabetes. N Z Med J. 2015;128:25–32.
3. Iversen AS, Graue M, Haugstvedt A, et al. Being mothers and fathers of a child with type 1 diabetes aged 1 to 7 years: a phenomenological study of parents’ experiences. Int J Qual Stud Health Well-Being. 2018;13(1):1487758. doi:10.1080/17482631.2018.1487758
4. Hilliard ME, Tully C, Monaghan M, et al. Design and development of a stepped-care behavioral intervention to support parents of young children newly diagnosed with type 1 diabetes. Contemp Clin Trials. 2017;62:1–10. doi:10.1016/j.cct.2017.08.009
5. Pickup JC, Harris A. Assessing quality of life for new diabetes treatments and technologies: a simple patient-centered score. J Diabetes Sci Technol. 2007;1(3):394–399. doi:10.1177/193229680700100312
6. Smith LB, Liu X, Johnson SB, et al. Family adjustment to diabetes diagnosis in children: can participation in a study on type 1 diabetes genetic risk be helpful?. Pediatr Diabetes. 2018;19(5):1025–1033. doi:10.1111/pedi.12674
7. Visekruna S, McGillis Hall L, Parry M, et al. Intersecting health policy and the social determinants of health in pediatric Type 1 diabetes management and care. J Pediatr Nurs. 2017;37:62–69. doi:10.1016/j.pedn.2017.06.001
8. Millan M. [Quality-of-life questionnaire designed for diabetes mellitus (EsDQOL)]. Aten Primaria. 2002;29(8):517–521. doi:10.1016/S0212-6567(02)70623-9. Spanish.
9. Burroughs TE, Desikan R, Waterman BM, et al. Development and validation of the diabetes quality of life brief clinical inventory. Diabetes Spectr. 2004;17(1):41–49. doi:10.2337/diaspect.17.1.41
10. Dudzińska M, Tarach JS, Burroughs TE, et al. Validation of the polish version of Diabetes Quality of Life – Brief Clinical Inventory (DQL-BCI) among patients with type 2 diabetes. Arch Med Sci. 2014;5:891–898. doi:10.5114/aoms.2014.46210
11. Hansen JA, Weissbrod C, Schwartz DD, et al. Paternal involvement in pediatric Type 1 diabetes: fathers’ and mothers’ psychological functioning and disease management. Fam Syst Health. 2012;30(1):47–59. doi:10.1037/a0027519
12. Teasdale A, Limbers C. Avoidant coping moderates the relationship between paternal involvement in the child’s type 1 diabetes (T1D) care and parenting stress. J Child Health Care. 2018;22(4):606–618. doi:10.1177/1367493518767068
13. Pate T, Klemenčič S, Battelino T, et al. Fear of hypoglycemia, anxiety, and subjective well-being in parents of children and adolescents with type 1 diabetes. J Health Psychol. 2019;24(2):209–218. doi:10.1177/1359105316650931
14. Saoji N, Palta M, Young HN, et al. The relationship of Type 1 diabetes self-management barriers to child and parent quality of life: a US cross-sectional study. Diabet Med. 2018;35(11):1523–1530. doi:10.1111/dme.13760
15. Anderson YC, Wynter LE, Treves KF, et al. Assessment of health-related quality of life and psychological well-being of children and adolescents with obesity enrolled in a New Zealand community-based intervention programme: an observational study. BMJ Open. 2017;7(8):e015776. doi:10.1136/bmjopen-2016-015776
16. Malerbi FE, Negrato CA, Gomes MB. Assessment of psychosocial variables by parents of youth with type 1 diabetes mellitus. Diabetol Metab Syndr. 2012;4:48. doi:10.1186/1758-5996-4-48
17. D´Annunzio G, Gialetti S, Carducci C, et al. Italian translation, cultural adaption and validation of the PedsQLTM3.0mdiabetes module questionnaire in children with type diabetes and their parents. Health Qual Life Outcomes. 2014;12(1):115. doi:10.1186/s12955-014-0115-2
18. Saylor J, Hanna KM, Calamaro CJ. Experiences of college students who are newly diagnosed with Type 1 diabetes mellitus. J Pediatr Nurs. 2019;44:74–80. doi:10.1016/j.pedn.2018.10.020
19. Boogerd EA, Damhuis AMA, van Alfen-van der Velden JA, et al. Assessment of psychosocial problems in children with type 1 diabetes and their families: the added value of using standardised questionnaires in addition to clinical estimations of nurses and paediatricians. J Clin Nurs. 2015;24(15–16):2143–2151. doi:10.1111/jocn.12789
20. Kim SH, Lee A. Health-literacy-sensitive diabetes self-management interventions: a systematic review and meta-analysis. Worldviews Evid Based Nurs. 2016;13(4):324–333. doi:10.1111/wvn.12157
21. Hoey H, Lange K, Skinner TC, et al. For Hvidoere International Study Group. Hvidoere smiley faces: international diabetes quality of life assessment tool for young children. Pediatr Diabetes. 2018;19(3):553–558. doi:10.1111/pedi.12602
22. Orenstein GA, Lewis L. Eriksons stages of psychosocial development. In: StatPearls. 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556096/. Accessed September 14, 2020.
23. Kelo M, Martikainen M, Eriksson E. Self-care of school-age children with diabetes: an integrative review. J Adv Nurs. 2011;67(10):2096–2108. doi:10.1111/j.1365-2648.2011.05682.x
24. Holmström MR, Häggström M, Söderberg S. Being facilitators in a challenging context-school personnel’s experiences of caring for youth with diabetes Type 1. J Pediatr Nurs. 2018;43:e114–e119. doi:10.1016/j.pedn.2018.08.007
25. Sparapani V, Borges ALV, Dantas IRDO, et al. Children with Type 1 diabetes mellitus and their friends: the influence of this interaction in the management of the disease. Rev Lat Am Enfermagem. 2012;20(1):117–125. doi:10.1590/S0104-11692012000100016
26. Czenczek-Lewandowska E, Leszczak J, Weres A, et al. Sedentary behaviors in children and adolescents with type 1 diabetes, depending on the insulin therapy used. Medicine (Baltimore). 2019;98(19):e15625. doi:10.1097/MD.0000000000015625
27. Yayan EH, Zengin M, Erden Karabulut Y, et al. The relationship between the quality of life and depression levels of young people with type I diabetes. Perspect Psychiatr Care. 2019;55(2):291–299. doi:10.1111/ppc.12349
28. Kummer S, Stahl-Pehe A, Castillo K, et al. Health behaviour in children and adolescents with type 1 diabetes compared to a representative reference population. PLoS One. 2014;9(11):e112083. doi:10.1371/journal.pone.0112083
29. Canbulat Sahiner N, Turkmen AS, Acikgoz A, et al. Effectiveness of two different methods for pain reduction during insulin injection in children with Type 1 diabetes: buzzy and shotBlocker. Worldviews Evid Based Nurs. 2018;15(6):464–470. doi:10.1111/wvn.12325
30. Anderson BJ, Laffel LM, Domenger C, et al. Factors associated with diabetes-specific health-related quality of life in youth with Type 1 diabetes: the Global TEENs Study. Diabetes Care. 2017;40(8):1002–1009. doi:10.2337/dc16-1990
31. Lindström C, Åman J, Norberg AL, et al. “Mission Impossible”; the mothering of a child with Type 1 diabetes - from the perspective of mothers experiencing burnout. J Pediatr Nurs. 2017;36:149–156. doi:10.1016/j.pedn.2017.06.002
32. Savin KL, Hamburger ER, Monzon AD, et al. Diabetes-specific family conflict: informant discrepancies and the impact of parental factors. J Fam Psychol. 2018;32(1):157–163. doi:10.1037/fam0000364
33. Dagan E, Dubovi I, Levy M, et al. Adherence to diabetes care: knowledge of biochemical processes has a high impact on glycaemic control among adolescents with type 1 diabetes. J Adv Nurs. 2019;75(11):2701–2709. doi:10.1111/jan.14098
34. Quaye AA, Coyne I, Söderbäck M, et al. Children´s active participation in decisión-making processes during hospitalisation: an observational study. J Clin Nurs. 2019;28(23–24):4525–4537. doi:10.1111/jocn.15042
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.