")
Back to Journals » International Journal of General Medicine » Volume 12
Two-year results of a community-based randomized controlled lifestyle intervention trial to control prehypertension and/or prediabetes in Thailand: a brief report
Authors Pengpid S , Peltzer K , Jayasvasti I , Aekplakorn W, Puckpinyo A , Nanthananate P , Mansin A
Received 1 January 2019
Accepted for publication 20 February 2019
Published 25 March 2019 Volume 2019:12 Pages 131—135
DOI https://doi.org/10.2147/IJGM.S200086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supa Pengpid,1,2 Karl Peltzer,3,4 Isareethika Jayasvasti,1 Wichai Aekplakorn,5 Apa Puckpinyo,1 Pheeraya Nanthananate,6 Anutsara Mansin7
1ASEAN Institute for Health Development, Mahidol University, Salaya, Thailand; 2Department of Research Development and Innovation, University of Limpopo, Polokwane, South Africa; 3Department for Management of Science and Technology Development, Ton Duc Thang University, Ho Chi Minh City, Vietnam; 4Faculty of Pharmacy, Ton Duc Thang University, Ho Chi Minh City, Vietnam; 5Department of Community Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 6Faculty of Nursing, Bangkok-Thonburi University, Bangkok, Thailand; 7Department Surgical Nursing, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Abstract: The aim of the study was to assess the 2-year effect of a community-based randomized controlled lifestyle intervention on glucose and blood pressure levels in Thailand. Participants (N=443, with prediabetes and/or prehypertension) received a six 2-hr group sessions lifestyle intervention (physical activity and nutrition) over 6 months. Measurements were at baseline, 12 months (89%) and at 24 months (84.7%). Statistically significant interaction effects on fasting plasma glucose and DBP at 12 months were not maintained at 24 months, while significant interaction effects were found on high-density lipoprotein and low-density lipoprotein cholesterol at 24 months. Improvements were found for fasting plasma glucose, SBP, DBP and total cholesterol, but no significant interaction effect was detected. The development of type 2 diabetes was higher in the control than in the intervention group, but it was not reaching significance (P=0.181), while 3.0% in the intervention group and 2.6% in the control group developed hypertension at 24 months. No significant group differences were found in psycho-behavioral variables. The lifestyle intervention did not provide additional benefits compared to the control group at 24-month follow-up.
Trial registration number: TCTR20170721001
Keywords: community-based intervention, lifestyle intervention, prediabetes, prehypertension, Thailand
Introduction
Lifestyle interventions have been found to be effective to prevent the progression of prehypertension to hypertension and prediabetes to diabetes.1–5 In a 12-month follow-up study, partial effectiveness of a community (Buddhist temple)-based lifestyle intervention program to control prehypertension and/or prediabetes in temple members was found in Thailand,6 showing the potential effectiveness of such a community intervention. In order to assess longer term effects of this intervention trial, we report findings on the results of this study at 24-month follow-up.
Materials and methods
The study is a cluster randomized controlled evaluation of a group-based program in community settings (12 Buddhist temples) in Nakhon Pathom province; more detail.6 The study protocol was approved by the “Committee for Research Ethics (Social Sciences), Mahidol University (MU-SSIRB: 2016/053-B1).” Written informed consent was obtained from all participants. This study was in compliance with the ethical principles of the Declaration of Helsinki.
The intervention consisted of six group lifestyle (diet and physical activity) counseling sessions (on average 60–90 mins) over a period of 6 months conducted by trained study nurses in the temple premises and/or the adjacent health facility.
Participants were followed-up at 12 and 24 months following baseline assessment. A detailed study description, including intervention content, study flow chart, sample characteristics and assessment measures, has been published previously.6 The study sample consisted of 443 participants (220 in intervention and 223 in the control group) aged 35–65 years with prediabetes and/or prehypertension, of which 394 participants (89%) were retained at 12 months and 375 (84.7%) (179 in the intervention and 196 in the control group) at 24 months.
All clinical and psycho-behavioral questionnaire data at baseline, 12 months and 24 months were collected by study nurses. Outcomes included changes in SBP and blood glucose levels from baseline to year 2.
The analyses conducted used intention-to-treat, participants and clusters (temples) were analyzed according to the group they were allocated to. The intervention effects on continuous 24-month outcomes (ie, fasting plasma glucose, SBP and DBP, triglyceride, low-density lipoprotein=LDL, high-density lipoprotein=HDL, BMI and waist circumference) and diabetes and hypertension incidence outcomes and psycho-behavioral outcomes were analyzed using linear, gamma and logistic mixed-effect models adjusted for clustering (ie, a random effect of temple community), and baseline covariates, namely age, gender, education, smoking, alcohol use and depression. Fixed effects in these analyses consisted of time, condition, a time-by-condition interaction (ie, between-group changes) and baseline covariates. The data were analyzed using IBM-SPSS for Windows, version 24 (Chicago, IL, USA).
Results
Table 1 presents the physical study outcomes at each data assessed and results of multilevel mixed modeling. At 24-month follow-up, mixed modeling found significant interaction effects on HDL cholesterol (P=0.037) and LDL cholesterol (P<0.011). Improvements were found for fasting plasma glucose, SBP, DBP and total cholesterol,, but no significant interaction effect was detected. Further, there were no significant changes in terms of BMI, waist circumference, body fat and muscle mass (Table 1).
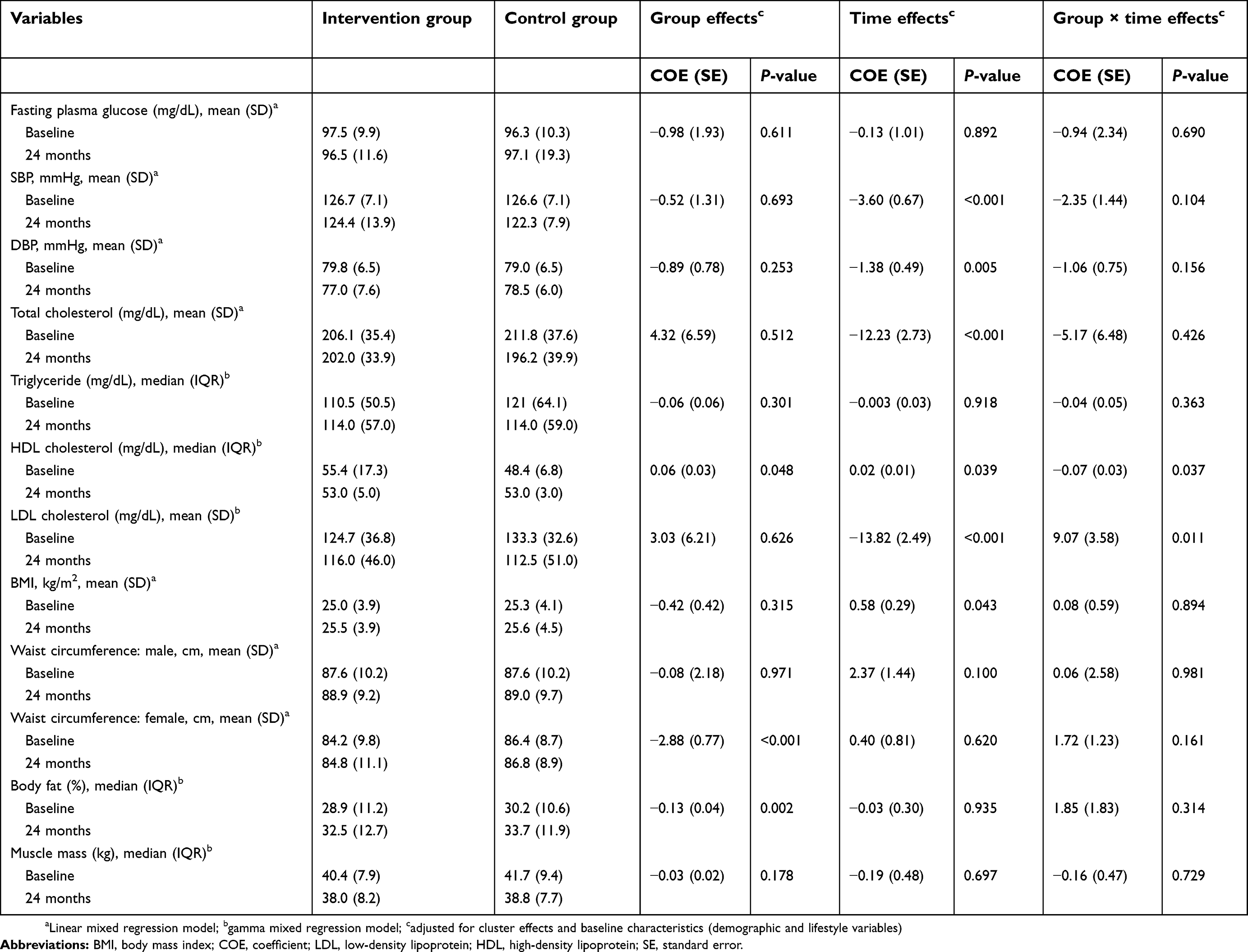 | Table 1 Clinical study outcomes of the intervention and control groups at baseline and 24 months |
Finally, Table 2 shows the development of diabetes and hypertension at 24 months. The development of type 2 diabetes was higher in the control than in the intervention group, but it was not reaching significance (P=0.181), while 3.0% in the intervention group and 2.6% in the control group developed hypertension at 24 months (Table 2).
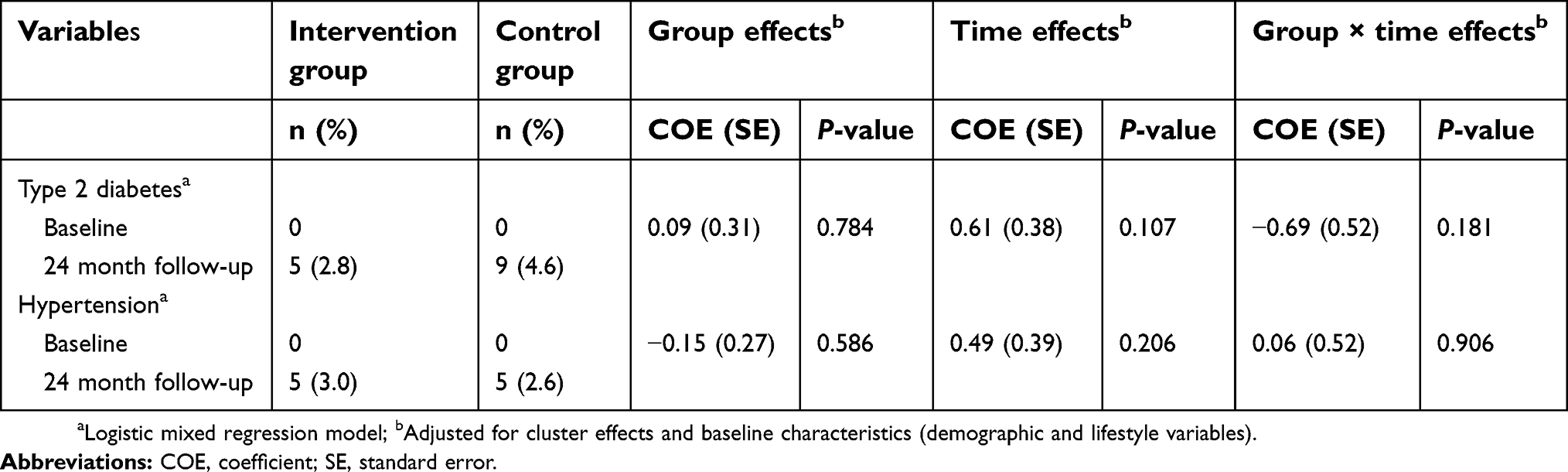 | Table 2 Changes to type 2 diabetes and/or hypertension |
Table 3 shows the changes in psycho-behavioral variables by study group at 24 months. Compared with the control group participants, intervention group participants were less likely to have a general anxiety disorder and were less likely to engage in hazardous or harmful drinking, but this did not reach significance. No group differences were found for fruit and vegetable consumption, smoking, physical activity and major depressive disorder (Table 3).
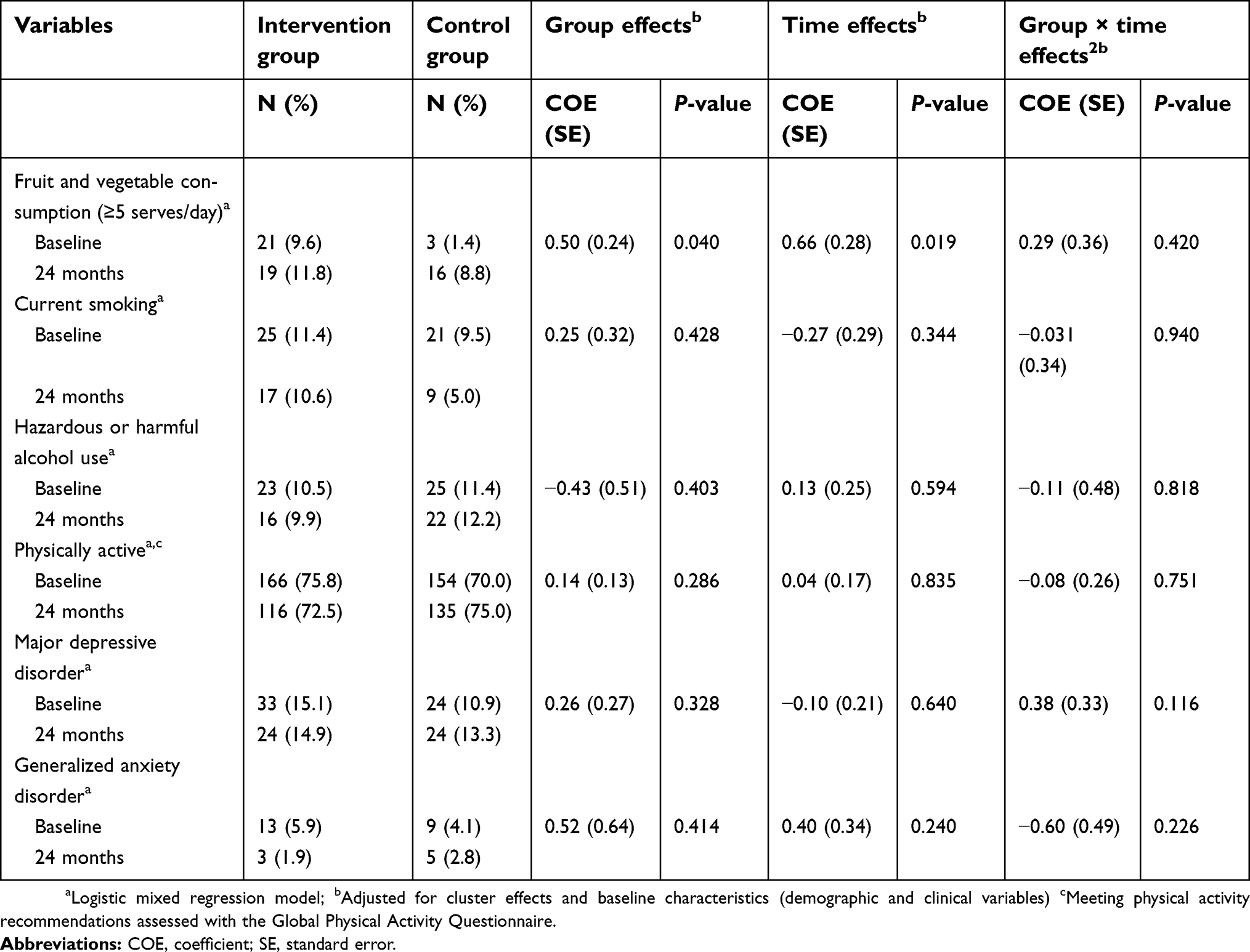 | Table 3 Psycho-behavioral study outcomes of the intervention and control groups at baseline and 24 months |
Conclusion
The aim of this community (Buddhist temple)-based lifestyle intervention programme was to control prehypertension and/or prediabetes in temple members. Previously, we showed that the intervention model was partially effective at 12-month follow-up.6
In this longer term follow-up, however, the lifestyle intervention did not provide additional benefits compared to the control group at 24-month follow-up. This finding seems to confirm that although the target was six intervention sessions only 3.8 sessions were on overage attended,6 more intervention sessions are needed to make this lifestyle programme effective. Even in a 15 session lifestyle intervention for prediabetics in India non-significant reduction in diabetes incidence was found at 24-month follow-up.7 The original PREMIER lifestyle intervention to control blood pressure included 18 session,8 and in a lifestyle intervention to prevent type 2 diabetes (DE-PLAN) in primary care included eleven counselling sessions, “six motivational phone calls and two letters followed by organized physical activity sessions.”9
Data sharing statement
The dataset used in the current study are available from the corresponding author on reasonable request.
Acknowledgment
The project was supported by the National Research Council of Thailand.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dagogo-Jack S, Egbuonu N, Edeoga C. Principles and practice of nonpharmacological interventions to reduce cardiometabolic risk. Med Princ Pract. 2010;19(3):167–175. doi:10.1159/000285280
2. Hedayati SS, Elsayed EF, Reilly RF. Non-pharmacological aspects of blood pressure management: what are the data? Kidney Int. 2011;79(10):1061–1070. doi:10.1038/ki.2011.46
3. Lindström J, Peltonen M, Eriksson JG, et al. Improved lifestyle and decreased diabetes risk over 13 years: long-term follow-up of the randomised finnish Diabetes Prevention Study (DPS). Diabetologia. 2012;56(2):284–293. doi:10.1007/s00125-012-2752-5
4. Márquez-Celedonio FG, Téxon-Fernández O, Chávez-Negrete A, Hernández-López S, Marín-Rendón S, Berlín-Lascurain S. Clinical effect of lifestyle modification on cardiovascular risk in prehypertensives: PREHIPER I study. Rev Esp Cardiol. 2009;62(1):86–90.
5. Yoon U, Kwok LL, Magkidis A. Efficacy of lifestyle interventions in reducing diabetes incidence in patients with impaired glucose tolerance: a systematic review of randomized controlled trials. Metabolism. 2012;62(2):303–314. doi:10.1016/j.metabol.2012.07.009
6. Pengpid S, Peltzer K, Puckpinyo A, Jayasvasti Chantarasongsuk I. Effectiveness of a cluster randomized controlled trial community-based lifestyle intervention program to control prehypertension and/or prediabetes in Thailand. Int J Diabetes Dev Ctries. 2018. doi:10.1007/s13410-018-0641-2
7. Thankappan KR, Sathish T, Tapp RJ, et al. A peer-support lifestyle intervention for preventing type 2 diabetes in India: a cluster-randomized controlled trial of the Kerala diabetes prevention program. PLoS Med. 2018;15(6):e1002575. doi:10.1371/journal.pmed.1002575
8. Funk KL, Elmer PJ, Stevens VJ, et al. PREMIER – a trial of lifestyle interventions for blood blood pressure control: intervention design and rationale. Health Promot Pract. 2008l;9(3):271–280. doi:10.1177/1524839906289035
9. Gilis-Januszewska A, Lindström J, Tuomilehto J, et al. Sustained diabetes risk reduction after real life and primary health care setting implementation of the diabetes in Europe prevention using lifestyle, physical activity and nutritional intervention (DE-PLAN) project. BMC Public Health. 2017;17(1):198. doi:10.1186/s12889-017-4104-3
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.