")
Back to Journals » Clinical Ophthalmology » Volume 13
Twelve-week dosing with Aflibercept in the treatment of neovascular age-related macular degeneration
Authors Garweg JG
Received 25 March 2019
Accepted for publication 11 June 2019
Published 19 July 2019 Volume 2019:13 Pages 1289—1295
DOI https://doi.org/10.2147/OPTH.S185756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Justus G Garweg1,2
1Swiss Eye Institute, Rotkreuz, and Berner Augenklinik Am Lindenhofspital, Bern, Switzerland; 2Department of Ophthalmology, Inselspital, University of Bern, Bern, Switzerland
Purpose: To review published evidence for a treatment interval extension to ≥12-weeks in neovascular macular degeneration treated with intravitreal Aflibercept.
Methods: A systematic search was performed in the NCBI/PubMed database to identify pro- and retrospective studies retrieved by the key terms or and or AND AND and included all papers that used a treat-and-extend (T&E) protocol including a loading phase of 3 intravitreal anti-VEGF injections and a minimal follow-up of 2 years. Disease stability was defined as the absence of any intraocular and absence or stability of subretinal fluid and pigment-epithelial detachment.
Results: Four studies were identified that reported information pertaining to disease stability or treatment extension beyond 12 weeks under intravitreal Aflibercept therapy including 1,102 eyes in total. Following a T&E protocol, a mean of 62.9% achieved disease stability and a 6.9 letter gain based on 11.9 injections over 24 months of Aflibercept treatment. As much as 43.0% of all eyes or 64.1% of the eyes with stable disease were maintained on ≥12-weekly injection intervals.
Conclusions: A consequent treatment with a null tolerance for intraretinal fluid is prerequisite to induce stability and maintain visual gain after the loading phase. Using Aflibercept in a T&E protocol, disease stability and interval extension to ≥12 weeks were reported in 43% of the eyes by end of the second year with less injections, but similar results as under fix dosing. A lower treatment burden strongly argues for an individualized proactive treatment regimen.
Keywords: neovascular age-related macular degeneration, AMD, Aflibercept, intravitreal anti-VEGF injections, treat-and-extend, proactive treatment, long-term outcome, review
Introduction
Monthly treatment of exudative or neovascular age-related macular degeneration (nAMD) with intravitreal anti-vascular endothelial growth factor (anti-VEGF) agents typically goes along with an impressive short-term effect,1–3 if treated before neuroretinal atrophy and subretinal fibrosis have developed.4,5 This gain is, however, lost over the following years after the patients have been switched to an as needed or pro re nata (PRN) therapy.6–9 Compared to randomized clinical trials (RCTs), the initial visual gain is less pronounced whereas the mid- to long-term vision loss is more pronounced in real life because exclusion criteria or negative predictors for vision gain in RCTs such as subfoveal fibrosis or hemorrhage and systemic comorbidities limiting a regular access to treatment do not apply to real life.10–12 Obviously, functional stability in real life is related to regular clinical visits and the number of intravitreal injections13,14 as well as the individual response to treatment with 50% of the patients newly developing disease activity despite monthly intravitreal ranibizumab therapy.15
With the introduction of Aflibercept for the treatment of nAMD in late 2012,3 the discussion focused on the quality of response,16–18 terms such as insufficient response and treatment resistance were defined and used as reason for switching from one to the other therapy.19,20 This indicates a shift in the aim of treatment from prevention of a severe vision loss for a previously blinding disease21,22 to long-term disease stability which is only achieved in the absence of any intraretinal and stability of subretinal fluid and/or pigment-epithelial detachment.
Since the potential visual gain and safety outcomes were similar between prospective studies with different anti-VEGF agents,16,23 the burden of disease and its treatment for patients and caregivers became central24–26 and the number of visits and injections the most critical marker for treatment success.27–31
Real-life data pertaining to the long-term stability under treatment with Aflibercept beyond two to three years are still scarce,32–35 and few papers addressed predictive factors for long-term functional stability.36–41 Clinical experience has taught that independent of the anti-VEGF drug in use, the PRN treatment strategy in RCTs and clinical practice has an inherent risk of under-treatment since lesion activity indicated by intraretinal fluid triggers re-treatment. This results in progression of subretinal fibrosis and finally loss of vision in nAMD,10,11,42 whereas the risk of progression of geographic atrophy in response to over-treatment seems relatively low.41 Consequently, good responders maintaining a dry macula with less than an injection every 2 months did not meet major interest43 until recently, when the 12-month results from 2 new prospective randomized clinical trials (Harrier and Hawk)44 comparing the effects of the investigational drug Brolucizumab to Aflibercept indicated that the portion of eyes that demonstrated a complete resolution of intraretinal fluid was higher under the former therapy allowing a treatment extension to 12 weeks in half of the patients44 whereas Aflibercept was delivered per label at a fix dosing every 2 months. The underlying review therefore presents an overview of the few published data on treatment extension of Aflibercept to 12 or more weeks and possible predictors of this low treatment demand.
Patients and methods
A systematic search was performed in the NCBI/PubMed database from the National Institute of Health, USA (https://www.ncbi.nlm.nih.gov/pubmed), to identify pro- and retrospective studies retrieved by the key terms <exudative> or <neovascular> and <AMD> or <age-related macular degeneration> AND <intravitreal therapy> AND <anti-VEGF> or Ranibizumab> or <Aflibercept>. Based on this set of manuscripts, all abstracts were selected that had been published in the last 10 years (since 2008), used a loading phase of 3 intravitreal Aflibercept injections (2mg/50ul) and a minimal follow-up of 2 years. Case reports and series with less than 50 patients were excluded, whereas cross-references identified during the literature search were included if they provided new information. For the purpose of this review, disease stability was defined as the absence of any intraretinal and absence or stability of subretinal fluid and pigment-epithelial detachment while data pertaining to the change in lesion size were not found.
Results
A total of four studies, one randomized clinical trial and three real-life studies, reported information pertaining to treatment extension beyond 12 weeks under intravitreal Aflibercept therapy. Following a T&E protocol, disease stability was achieved in 62.9% (50.1–92.0) of 1,102 eyes, and 43.0% (24.0–52.8) of eyes reached ≥12-weekly injection intervals (Table 1).9,33,35,45 Because the corresponding RCT and real-world clinical studies did not use comparable outcome measures and identical treatment regimes, an evidence-based analysis of prognostic markers is not available, but few prognostic factors have consistently been reported in the different studies for disease stability, beyond these patient age, duration between first symptoms and treatment initiation, lesion size, absence or presence of intraretinal fluid after end of the loading phase and after 12 months, and the number of injections needed during the first year under an individualized therapy. A presenting visual acuity below 70 letters (20/40) resulted in a larger visual gain, but a lower final visual acuity than a visual acuity of ≥70 letters.46–49
Discussion
Clinical experience20,50 and the aforementioned head-to-head studies indicate that approximately half of the eyes respond equally well to Ranibizumab and Aflibercept treatment,51 indicating that these eyes might maintain functional and morphological stability of their exudative age-related macular degeneration (AMD) with a less intensive treatment35,51 than fix anti-VEGF dosing which was monthly for Ranibizumab or bi-monthly for Aflibercept in the VIEW studies.51,52 The dry AMD component, the involutive process of the retinal pigment epithelium and choriocapillaris, will progress independently in the long term, lately resulting in vision loss despite anti-exudative therapy.11,41,42 Nevertheless, 98% of the eyes with early nAMD indicated by a good presenting best-corrected visual acuity (BCVA; 70 ETDRS letters or driving vision) will maintain their function over 2 years despite a reduced number of injections in the second year according to the individual treatment demand.45 This is owed to a shift from a reactive to a proactive re-treatment strategy using not only functional but also anatomic disease activity criteria, namely intraretinal fluid on OCT.43 A good early functional response may, however, precede the anatomic response and go along with excellent long-term functional results: Attaining a satisfying functional 3-year outcome was closer (OR 9.8) correlated to a BCVA of ≥70 compared to <70 letters than to absence or presence of lesion activity (OR 1.6) by end of the loading phase following a treat-and-extend protocol.49 This is supported by another recently published study which found that independent of the number of injections, eyes with good initial BCVA had a good functional outcome over up to 4 years whereas eyes with poor initial BCVA despite a good initial visual gain deteriorated during the follow-up which was associated to the presence of intra- and subretinal fluid and subretinal fibrosis.48 Today, virtually no retina expert would delay intravitreal treatment in nAMD until a five-letter loss of vision despite the presence of intra- or subretinal fluid. A vision loss of ≥5 letters (1 line) was postulated as a re-treatment criterion for most prospective studies by the FDA and EMA. And likewise, virtually nobody would nowadays judge treatment necessary in the absence of any disease activity (no intra- or subretinal fluid on OCT) because of a five-letter loss.43,53 The OCTAVE study, designed to compare the sensitivity of a BCVA-driven to a combined BCVA/OCT-driven re-treatment, was terminated early because it had become evident by then that a re-treatment decision driven by morphological parameters adding to BCVA results in better macular long-term stability (Staurenghi G, personal communication, March 2019).
Both eyes of an individual must not respond similarly to treatment.54–56 Usually, the second eye is treated earlier resulting in a better long-term outcome.57 Several factors independent of the anti-VEGF drug in use and disease activity are related to the response to treatment, which is beyond the scope of this review.28,37,48,56–60 To summarize these studies, the portion of eyes achieving a good BCVA (≥70 compared), a complete absence of any intra- and subretinal fluid by end of the first and second year of treatment and allowing a treatment extension to 12 or more weeks after 1 and 2 years may become more relevant as markers of treatment efficacy.44,49 According to these parameters, approximately half of the eyes in the VIEW studies achieved stability in the second year under a capped PRN (reactive treatment on an as-needed basis for all eyes presenting disease activity, and a complimentary proactive Aflibercept treatment every 12 weeks in eyes with a stable functional and morphological situation), whereas the other half of still active lesions and treated as needed lost 5 letters.9 In a recently published large real-life cohort study, on the other hand, 82% of the eyes became inactive within the first year after a median time of only 71 days and 3 intravitreal Aflibercept injections,9 respectively, which meets well with preclinical pharmacological data.61,62 A visual gain of +3.9 letters at 24 months of follow-up was encountered under a treat-and-extend protocol while the portion of eyes requiring an Aflibercept injection at an interval of longer than 10 weeks was only 24%45 which is half of the portion reported by other studies.35,51 The remarkable differences with regard to achieving disease stability and treatment extension to ≥12 weeks between the single studies indicate obviously a large inter-individual variability in the treatment demand and the presence of other impact factors such as lesion size, visual acuity at diagnosis and duration of symptoms until treatment initiation which may have to be taken into account.47,63–65 Only a consequent suppression of lesion activity will result in a 10-letter or two-line better 2-year outcome using a treat-and-extend protocol9,35,45 than reported with the “capped PRN arm” with a loss of 3.1–3.8 letters in the VIEW study.9 Interestingly, 47.6% of the eyes in the “capped PRN arm” in VIEW 1 and 2 achieved disease stability by end of year 1 qualifying them for a proactive treatment every 12 weeks. These eyes widely maintained the vision gain encountered by the end of year 1 (−0.6 letters; Table 1).
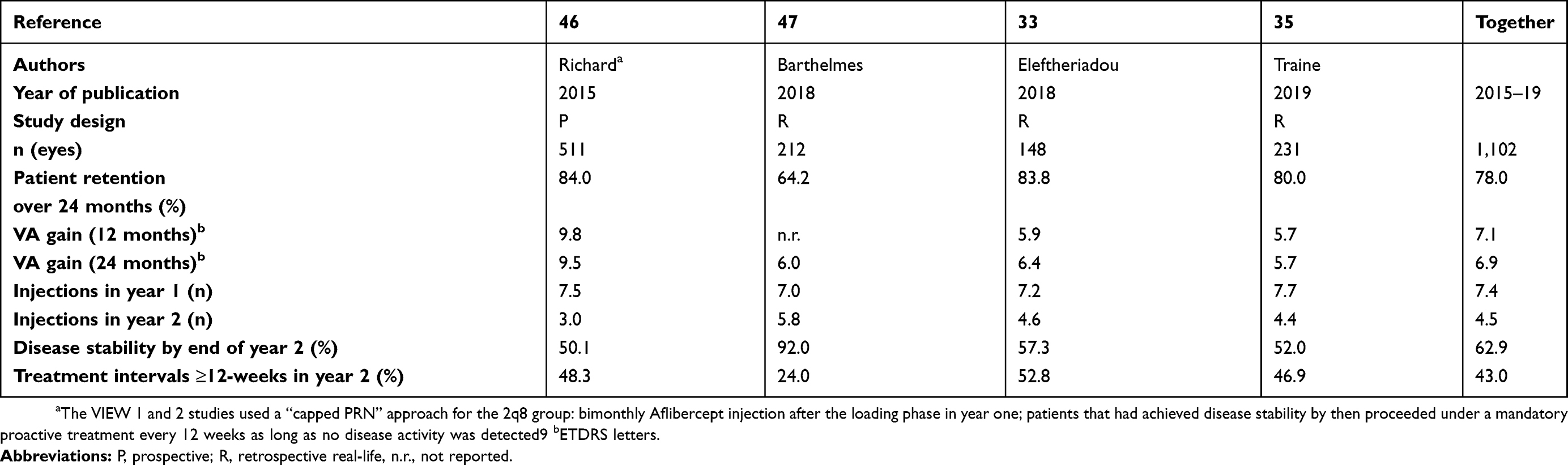 |
Table 1 Overview of published data |
The favorable outcomes of a null-tolerance against intraretinal fluid, moreover, have recently received support from prospective clinical trial, the Altair study.66 According to the interim analysis of the as yet not fully published study in a Japanese population under a treat-and-extend regimen, the Aflibercept treatment interval was extended to 12 weeks in 42.3% (2-week treatment extension arm) to 49.6% (4-week extension arm) by week 52,66 and 62.1–62.7% of the eyes experienced a treatment interval extension to 12 weeks and a visual gain of 6.1 and 7.6 ETDRS letters by week 96.67 In response to such favorable outcomes, the US FDA has recently approved a change of the treatment label allowing a treatment interval extension up to 12 weeks for Aflibercept.
In conclusion, consequently following a treat-and-extend protocol using Aflibercept treatment according to individual needs was reported to result in morphological and functional stability in two-thirds of eyes after 2 years and allows a treatment interval extension to ≥12 weeks in 43% of the eyes based on a patient retention of 78% indicating a high patient satisfaction with this protocol.
Disclosure
JGG acts as an advisor for several pharmaceutical companies (AbbVie, Alcon, Allergan, Bayer, Novartis) and contributes to several international industry-sponsored clinical studies. The underlying manuscript is independent of these activities. The author received no direct or indirect support for this study nor has he conflicting interests with the data that are presented herein. The author reports no other conflicts of interest in this work.
References
1. Rosenfeld PJ, Brown DM, Heier JS; MARINA Study Group, et al.. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1419–1431. doi:10.1056/NEJMoa054481
2. Brown DM, Kaiser PK, Michels M; ANCHOR Study Group, et al.. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1432–1444. doi:10.1056/NEJMoa062655
3. Heier JS, Brown DM, Chong V; VIEW 1 and VIEW 2 Study Groups, et al.. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119:2537–2548. doi:10.1016/j.ophtha.2012.09.006
4. Zandi S, Weisskopf F, Garweg JG, et al. Pre-existing RPE atrophy and defects in the external limiting membrane predict early poor visual response to ranibizumab in neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging Retina. 2017;48:326–332. doi:10.3928/23258160-20170329-07
5. Sadda SR, Tuomi LL, Ding B, Fung AE, Hopkins JJ. Macular atrophy in the HARBOR study for neovascular age-related macular degeneration. Ophthalmology. 2018;125:878–886. doi:10.1016/j.ophtha.2017.12.026
6. Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology. 2012;119:1175–1183. doi:10.1016/j.ophtha.2011.12.016
7. Rofagha S, Bhisitkul RB, Boyer DS, Sadda SR, Zhang K; SEVEN-UP Study Group. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology. 2013;120:2292–2299. doi:10.1016/j.ophtha.2013.03.046
8. Martin DF, Maguire MG, Fine SL; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, et al.. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119:1388–1398. doi:10.1016/j.ophtha.2012.03.053
9. Richard G, Monés J, Wolf S, et al. Scheduled versus pro re nata dosing in the VIEW trials. Ophthalmology. 2015;122:2497–2503. doi:10.1016/j.ophtha.2015.08.014
10. Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99:220–226. doi:10.1136/bjophthalmol-2014-305327
11. Garweg JG, Zirpel JJ, Gerhardt C, Pfister IB. The fate of eyes with wet AMD beyond four years of anti-VEGF therapy. Graefes Arch Clin Exp Ophthalmol. 2018;256:823–831. doi:10.1007/s00417-018-3907-y
12. Ehlken C, Helms M, Böhringer D, Agostini HT, Stahl A. Association of treatment adherence with real-life VA outcomes in AMD, DME, and BRVO patients. Clin Ophthalmol. 2017;12:13–20. doi:10.2147/OPTH.S151611
13. Holz FG, Tadayoni R, Beatty S, et al. Key drivers of visual acuity gains in neovascular age-related macular degeneration in real life: findings from the AURA study. Br J Ophthalmol. 2016;100:1623–1628. doi:10.1136/bjophthalmol-2015-308166
14. Holz FG, Tadayoni R, Beatty S, et al. Determinants of visual acuity outcomes in eyes with neovascular AMD treated with anti-VEGF agents: an instrumental variable analysis of the AURA study. Eye (Lond). 2016;30:1063–1071. doi:10.1038/eye.2016.90
15. Droege KM, Caramoy A, Kersten A, et al. Patient preference of ranibizumab treatment regimen for neovascular age-related macular degeneration - monthly injections versus pro re nata. Graefes Arch Clin Exp Ophthalmol. 2014;252:31–34. doi:10.1007/s00417-013-2412-6
16. Ba J, Peng RS, Xu D, et al. Intravitreal anti-VEGF injections for treating wet age-related macular degeneration: a systematic review and meta-analysis. Drug Des Devel Ther. 2015;9:5397–5405. doi:10.2147/DDDT.S86269
17. Szabo SM, Hedegaard M, Chan K, et al. Ranibizumab vs. aflibercept for wet age-related macular degeneration: network meta-analysis to understand the value of reduced frequency dosing. Curr Med Res Opin. 2015;31:2031–2042. doi:10.1185/03007995.2015.1084909
18. Stewart MW. Individualized treatment of neovascular age-related macular degeneration: what are patients gaining? Or losing? J Clin Med. 2015;4:1079–1101. doi:10.3390/jcm4051079
19. Garweg JG, Niderprim SA, Russ HM, Pfister IB. Comparison of strategies of treatment with ranibizumab in newly-diagnosed cases of neovascular age-related macular degeneration. J Ocul Pharmacol Ther. 2017;33:773–778. doi:10.1089/jop.2017.0006
20. Garweg JG, Gerhardt C, Kodjikian L, Pfister IB. Real-life experience with aflibercept and ranibizumab in the treatment of newly diagnosed neovascular age-related macular degeneration over 24 months. J Ocul Pharmacol Ther. 2017;33:567–572. doi:10.1089/jop.2017.0031
21. Regillo CD, Brown DM, Abraham P, et al. Randomized, double-masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER Study year 1. Am J Ophthalmol. 2008;145:239–248. doi:10.1016/j.ajo.2007.10.004
22. Kim LN, Mehta H, Barthelmes D, Nguyen V, Gillies MC. Metaanalysis of real-world outcomes of intravitreal ranibizumab for the treatment of neovascular age-related macular degeneration. Retina. 2016;36:1418–1431. doi:10.1097/IAE.0000000000001142
23. Nguyen CL, Oh LJ, Wong E, Wei J, Chilov M. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration: a meta-analysis of randomized controlled trials. BMC Ophthalmol. 2018;18:130. doi:10.1186/s12886-018-0785-3
24. Hernandez L, Lanitis T, Cele C, Toro-Diaz H, Gibson A, Kuznik A. Intravitreal aflibercept versus ranibizumab for wet age-related macular degeneration: a cost-effectiveness analysis. J Manag Care Spec Pharm. 2018;24:608–616. doi:10.18553/jmcp.2018.24.7.608
25. van Asten F, Michels CTJ, Hoyng CB, et al. The cost-effectiveness of bevacizumab, ranibizumab and aflibercept for the treatment of age-related macular degeneration-A cost-effectiveness analysis from a societal perspective. PLoS One. 2018;13:e0197670. doi:10.1371/journal.pone.0197670
26. Schmid MK, Reich O, Faes L, et al. Comparison of outcomes and costs of ranibizumab and aflibercept treatment in real-life. PLoS One. 2015;10:e0135050. doi:10.1371/journal.pone.0135050
27. Martin DF. Evolution of intravitreal therapy for retinal diseases-from CMV to CNV: the LXXIV Edward Jackson Memorial Lecture. Am J Ophthalmol. 2018;191:xli–lviii. doi:10.1016/j.ajo.2017.12.019
28. Hussain RM, Hariprasad SM, Ciulla TA. Treatment burden in neovascular AMD:visual acuity outcomes are associated with anti-VEGF injection frequency. Ophthalmic Surg Lasers Imaging Retina. 2017;48:780–784. doi:10.3928/23258160-20170928-01
29. Saxena N, George PP, Hoon HB, Han LT, Onn YS. Burden of wet age-related macular degeneration and its economic implications in Singapore in the year 2030. Ophthalmic Epidemiol. 2016;23:232–237. doi:10.1080/09286586.2016.1193617
30. Prenner JL, Halperin LS, Rycroft C, Hogue S, Williams Liu Z, Seibert R. Disease burden in the treatment of age-related macular degeneration: findings from a time-and-motion study. Am J Ophthalmol. 2015;160(725–731.e1). doi:10.1016/j.ajo.2015.06.023
31. Mantel I. [Age-related macular degeneration – a challenge for public health care]. Ther Umsch. 2016;73:79–83. doi:10.1024/0040-5930/a000760
32. Neves Cardoso P, Pinheiro AF, Meira J, et al. Switch to aflibercept in the treatment of neovascular AMD: long-term results. J Ophthalmol. 2017;2017:6835782. doi:10.1155/2017/6835782
33. Eleftheriadou M, Gemenetzi M, Lukic M, et al. Three-year outcomes of aflibercept treatment for neovascular age-related macular degeneration: evidence from a clinical setting. Ophthalmol Ther. 2018;7:361–368. doi:10.1007/s40123-018-0139-5
34. Bakri SJ, Thorne JE, Ho AC, et al. Safety and efficacy of anti-vascular endothelial growth factor therapies for neovascular age-related macular degeneration: a Report by the American Academy of Ophthalmology. Ophthalmology. 2019;126:55–63. doi:10.1016/j.ophtha.2018.07.028
35. Traine PG, Pfister IB, Zandi S, Spindler J, Garweg JG. Long-term outcome of intravitreal aflibercept treatment for neovascular age-related macular degeneration using a „treat-and-extend“ regimen. Ophthalmol Retina. 2019;3:393–399. doi:10.1016/j.oret.2019.01.018
36. Zhang X, Lai TYY. Baseline predictors of visual acuity outcome in patients with wet age-related macular degeneration. Biomed Res Int. 2018;2018:9640131. doi:10.1155/2018/9640131
37. Ashraf M, Souka A, Adelman RA. Age-related macular degeneration: using morphological predictors to modify current treatment protocols. Acta Ophthalmol. 2018;96:120–133. doi:10.1111/aos.13565
38. Tsilimbaris MK, López-Gálvez MI, Gallego-Pinazo R, Margaron P, Lambrou GN. Epidemiological and clinical baseline characteristics as predictive biomarkers of response to anti-VEGF treatment in patients with neovascular AMD. J Ophthalmol. 2016;2016:4367631. doi:10.1155/2016/4367631
39. Ying GS, Maguire MG, Daniel E; Comparison of Age-Related Macular Degeneration Treatments Trials (CATT) Research Group, et al.. Association of baseline characteristics and early vision response with 2-year vision outcomes in the comparison of AMD Treatments Trials (CATT). Ophthalmology. 2015;122(2523–31.e1). doi:10.1016/j.ophtha.2015.08.015
40. Kwon YH, Lee DK, Kim HE, Kwon OW. Predictive findings of visual outcome in spectral domain optical coherence tomography after ranibizumab treatment in age-related macular degeneration. Korean J Ophthalmol. 2014;28:386–392. doi:10.3341/kjo.2014.28.5.386
41. Garweg JG. Atrophy of the macula in the context of its wet, age-related degeneration: an inescapable consequence of anti-VEGF therapy? Ophthalmologe. 2016;113:1036–1045. doi:10.1007/s00347-016-0306-9
42. Munk MR, Ceklic L, Ebneter A, Huf W, Wolf S, Zinkernagel MS. Macular atrophy in patients with long-term anti-VEGF treatment for neovascular age-related macular degeneration. Acta Ophthalmol. 2016;94:e757–e764. doi:10.1111/aos.13157
43. Amoaku WM, Chakravarthy U, Gale R, et al. Defining response to anti-VEGF therapies in neovascular AMD. Eye (Lond). 2015;29:721–731. doi:10.1038/eye.2015.48
44. Dugel PU, Jaffe GJ, Sallstig P, et al. Brolucizumab versus aflibercept in participants with neovascular age-related macular degeneration: a randomized trial. Ophthalmology. 2017;124:1296–1304. doi:10.1016/j.ophtha.2017.03.057
45. Barthelmes D, Nguyen V, Daien V; Fight Retinal Blindness Study Group, et al.. Two year outcomes of “Treat and extend” intravitreal therapy using aflibercept preferentially for neovascular age-related macular degeneration. Retina. 2018;38:20–28. doi:10.1097/IAE.0000000000001496
46. Regillo CD, Busbee BG, Ho AC, Ding B, Haskova Z. Baseline predictors of 12-month treatment response to ranibizumab in patients with wet age-related macular degeneration. Am J Ophthalmol. 2015;160(5):1014–1023.e2. doi:10.1016/j.ajo.2015.07.034
47. Finger RP, Wickremasinghe SS, Baird PN, Guymer RH. Predictors of anti-VEGF treatment response in neovascular age-related macular degeneration. Surv Ophthalmol. 2014;59:1–18. doi:10.1016/j.survophthal.2013.03.009
48. Sagiv O, Zloto O, Moroz I, Moisseiev J. Different clinical courses on long-term follow-up of age-related macular degeneration patients treated with intravitreal anti-vascular endothelial growth factor injections. Ophthalmologica. 2017;238:217–225. doi:10.1159/000479437
49. Nguyen V, Daien V, Guymer R; Fight Retinal Blindness! Study Group, et al.. Projection of long-term visual acuity outcomes based on initial treatment response in neovascular age-related macular degeneration. Ophthalmology. 2019;126:64–74. doi:10.1016/j.ophtha.2018.08.023
50. Gillies MC, Nguyen V, Daien V, Arnold JJ, Morlet N, Barthelmes D. Twelve-month outcomes of ranibizumab vs. Aflibercept for neovascular age-related macular degeneration: data from an observational study. Ophthalmology. 2016;123:2545–2553. doi:10.1016/j.ophtha.2016.08.016
51. Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology. 2014;121:193–201. doi:10.1016/j.ophtha.2013.08.011
52. Wykoff CC, Clark WL, Nielsen JS, Brill JV, Greene LS, Heggen CL. Optimizing anti-VEGF treatment outcomes for patients with neovascular age-related macular degeneration. J Manag Care Spec Pharm. 2018;24(2–a Suppl):S3–S15. doi:10.18553/jmcp.2018.24.2-a.s3
53. Pron G. Optical coherence tomography monitoring strategies for A-VEGF-treated age-related macular degeneration: an evidence-based analysis. Ont Health Technol Assess Ser. 2014;14:1–64.
54. Silva R, Cachulo ML, Fonseca P, et al. Age-related macular degeneration and risk factors for the development of choroidal neovascularisation in the fellow eye: a 3-year follow-up study. Ophthalmologica. 2011;226:110–118. doi:10.1159/000329473
55. Mann SS, Rutishauser-Arnold Y, Peto T, et al. The symmetry of phenotype between eyes of patients with early and late bilateral age-related macular degeneration (AMD). Graefes Arch Clin Exp Ophthalmol. 2011;249:209–214. doi:10.1007/s00417-010-1483-x
56. Chevreaud O, Semoun O, Blanco-Garavito R, et al. Visual acuity at presentation in the second eye versus first eye in patients with exudative age-related macular degeneration. Eur J Ophthalmol. 2016;26:44–47. doi:10.5301/ejo.5000649
57. Lee AY, Lee CS, Butt T; UK AMD EMR Users Group, et al.. UK AMD EMR USERS GROUP REPORT V: benefits of initiating ranibizumab therapy for neovascular AMD in eyes with vision better than 6/12. Br J Ophthalmol. 2015;99:1045–1050. doi:10.1136/bjophthalmol-2014-306229
58. Li J, Xu J, Chen Y, Zhang J, Cao Y, Lu P. Efficacy comparison of intravitreal anti-VEGF therapy for three subtypes of neovascular age-related macular degeneration: a systematic review and meta-analysis. J Ophthalmol. 2018;2018:1425707. doi:10.1155/2018/1425707
59. Muftuoglu IK, Tsai FF, Gaber R, Alam M, Meshi A, Freeman WR. High-frequency aflibercept injections in persistent neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2017;255:709–717. doi:10.1007/s00417-016-3547-z
60. Abdelfattah NS, Zhang H, Boyer DS, et al. Drusen volume as a predictor of disease progression in patients with late age-related macular degeneration in the fellow eye. Invest Ophthalmol Vis Sci. 2016;57:1839–1846. doi:10.1167/iovs.15-18572
61. Fauser S, Schwabecker V, Muether PS. Suppression of intraocular vascular endothelial growth factor during aflibercept treatment of age-related macular degeneration. Am J Ophthalmol. 2014;158:532–536. doi:10.1016/j.ajo.2014.05.025
62. Stewart MW, Rosenfeld PJ. Predicted biological activity of intravitreal VEGF trap. Br J Ophthalmol. 2008;92:667–668. doi:10.1136/bjo.2007.134874
63. Muether PS, Hoerster R, Hermann MM, Kirchhof B, Fauser S. Long-term effects of ranibizumab treatment delay in neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2013;251:453–458. doi:10.1007/s00417-012-2038-0
64. Rasmussen A, Brandi S, Fuchs J, et al. Visual outcomes in relation to time to treatment in neovascular age-related macular degeneration. Acta Ophthalmol. 2015;93:616–620. doi:10.1111/aos.12781
65. Cazet-Supervielle A, Gozlan J, Cabasson S, Boissonnot M, Manic H, Leveziel N. Intravitreal ranibizumab in daily clinical practice for age-related macular degeneration: treatment of exudative age-related macular degeneration in real life. Ophthalmologica. 2015;234:26–32. doi:10.1159/000430470
66. Ohji M, Okada AA, Takahashi K, Kobayashi M, Terano Y. Two Different Treat and Extend Dosing Regimens of Intravitreal Afibercept for wAMD in Japanese Patients: 52 Week Results of the ALTAIR Study. Barcelona: Euretina Meeting; 2017.
67. Ohji M, Okada AA, Takahashi K, Kobayashi M, Terano Y. Two Different Treat-And-Extend Dosing Regimens of Intravitreal Aflibercept in Japanese Patients with Wet Age-Related Macular Degeneration: 96-Week Results of the ALTAIR Study. Vienna: Euretina Meeting; 2018.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.