")
Back to Journals » Transplant Research and Risk Management » Volume 8
Tumor-resected kidney transplant – a quality of life survey
Authors Sundararajan S, He B , Delriviere L
Received 21 August 2015
Accepted for publication 19 November 2015
Published 2 May 2016 Volume 2016:8 Pages 9—13
DOI https://doi.org/10.2147/TRRM.S94868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qing Yi
Siva Sundararajan,1 Bulang He,1,2 Luc Delriviere,1,2
1WA Liver and Kidney Surgical Transplant Service, Department of General Surgery, Sir Charles Gairdner Hospital, Perth, WA, Australia; 2School of Surgery, The University of Western Australia, Perth, WA, Australia
Background: To overcome the organ shortage, a program to use kidney grafts after excision of a small renal tumor (tumor resected kidney [TRK]) was implemented in February 2007. All recipients were over 55 years old according to the selection criteria. The aim of this study is to assess the quality of life after kidney transplant in this cohort.
Methods: From February 2007 to July 2013, 27 patients received a kidney graft after excision of the small kidney tumor. All patients were given the modified 36-Item Short Form Survey (SF-36) questionnaire with additional information regarding concerns about tumor recurrence and whether they would choose TRK transplantation or prefer to stay on dialysis if they have an option again.
Results: Of them, 20 returned the completed questionnaire. There is no tumor recurrence on a mean follow-up of 38 months. The mean scores in all eight domains of the SF-36 were higher posttransplantation. The differences were statistically significant. Ninety-five percent of recipients would prefer to have TRK transplantation rather than remain on dialysis. Eighty percent of patients had no or minimal concerns regarding tumor recurrence.
Conclusion: The patients who had kidney transplantation by using the graft after excision of a small tumor have achieved excellent quality of life. It is an important alternative for the solution of organ shortage in kidney transplantation. The concern of tumor recurrence is minimal. Performing a further study is worthwhile, with prospective data collection and a control group.
Keywords: quality of life, kidney transplant, tumor, small renal cell carcinoma
Introduction
Kidney transplant is the best treatment for patients with end-stage renal failure (ESRF). The number of patients with ESRF and consequently the number of patients on the transplant waitlist is increasing.1 These patients have a poor quality of life (QoL) and are vulnerable to other medical complications. There is a significant improvement to the health related quality of life (HRQoL) of end-stage renal disease patients posttransplantation.2–4 However, increase in the number of patients needing transplant outweighs the supply, leading to a shortage in the organs available. Alternate methods to increase the organ transplant pool have been explored including ABO incompatibility and extended criteria and paired donor exchange.5–8 These are still inadequate to meet the demands.1
Restoring kidney grafts from patients who have a small renal cell carcinoma, which is excised ex vivo and then transplanted, is an alternate option. This method has been described previously but as far as we are aware of, our unit is the first to implement a formal program to use tumor resected kidneys (TRK) grafts.9,10 The details of this program have been described previously.11 The aim of this study was to investigate the HRQoL and concerns patients had about recurrence of tumor.
Materials and methods
A cohort study was done between October 2007 and December 2012 on 27 patients who received a TRK graft. Appropriate ethics approval was obtained from the Human Research Ethic Committee of Sir Charles Gairdner Hospital. Written information was provided to all patients and written consent was obtained. Selection of tumor-excised kidney graft from a donor and potential candidate for acceptance of the graft has already been described.11 Briefly, the decision for radical or partial nephrectomy for a potential donor patient with a small renal mass is purely a discussion between the patient and his/her treating urologist. The donor patient is fully informed that the kidney may be used for transplantation if radical nephrectomy is considered. The transplant team is informed only after the decision for radical nephrectomy is made. The tumor size should be no more than 3 cm in diameter. Frozen section is routinely performed on the back table following excision of the tumor. The histopathology of the tumor is obtained, and it is ensured that the margin is clear prior to transplantation. The potential candidates for acceptance of the tumor-excised kidney are those aged over 60 years with comorbidities who are otherwise unlikely to be accepted for the usual deceased waiting list or patients who are running out of dialysis access. The potential candidates are fully informed of the nature of the tumor excised kidney graft and aware of the risk of tumor recurrence after transplantation prior to being listed on this special waiting list. Immunosuppression is a basic triple regimen that consists of steroids, mycophenolate mofetil, and tacrolimus or cyclosporin. Sirolimus is always considered for these recipients who are suitable. A modified 36-Item Short Form Survey (SF-36) questionnaire was sent out to all patients who have received tumor excised kidney graft. The SF-36 is a validated, standardized self-report measure of the HRQoL. It measures eight domains: physical functioning, role limitations as a result of physical health problems, bodily pain, general health, vitality, social functioning, role limitations as a result of emotional health problems, and mental health. Scores range from 0 to 100 in each domain, with a higher score indicating better function. Two summary scores are also derived from the eight domains: the physical health component and the mental health component scores. The SF-36 was modified based on this study. So each patient assessed their HRQoL before and after transplantation, their concerns regarding recurrence of tumor, and whether they would opt to have the transplant again or continue with dialysis if they had to start over again. Demographic data, dialysis vintage (duration of dialysis treatment prior to kidney transplantation), level of concern regarding tumor recurrence, and the SF-36 scores were obtained. Twenty participants returned the completed questionnaire (91% response rate). Five patients were deceased (for reasons as summarized in Table 1). Two patients had migrated overseas and were lost to follow-up.
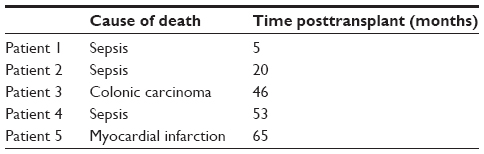 | Table 1 The cause of recipient death after tumor resected kidneys transplant |
Statistical analysis
All statistical analysis was performed using IBM SPSS Statistics Version 2.0 (SPSS Inc., Chicago, IL, USA), and P<0.05 indicates statistical significance. The pre- and posttransplant scores were compared using the paired Wilcoxon signed-rank test. Pearson correlation test was done to analyze relationship to age, sex, and level of concern regarding tumor recurrence. Spearman correlation test was used to analyze the relationship to dialysis vintage.
Results
In this cohort of 27 patients, 5 patients died during follow-up (Table 1). Twenty patients completed the questionnaire for analysis. Fifty percent of the patients were men. Mean age was 64.3 years (range: 52–80 years). The mean follow-up duration was 38 months (range: 13–74 months). There have been no tumor recurrences in any of the patients. The mean scores for all eight domains of the SF-36 were higher posttransplantation. The physical and mental component scores were also higher posttransplantation. The results are statistically significant (Tables 2 and 3). There was no significant correlation between age and any of the domain scores. Men appeared to have higher pretransplant scores for all domains except for bodily pain and emotional well-being. The correlation scores were statistically significant. Posttransplant, the scores between men and women were more even but did not reach statistical significance. Eighty percent of patients had minimal or no concerns about tumor recurrence. Ninety-five percent of patients would have the transplant again rather than remain on dialysis. Patients who had less concerns regarding tumor recurrence had higher scores. However, this result did not reach statistical significance. Dialysis vintage was negatively correlated with both physical and mental scores posttransplantation, which was statistically significant for majority of the domains (Tables 4 and 5).
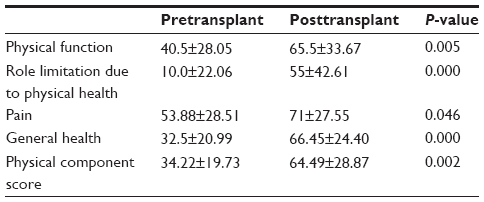 | Table 2 Physical domain scores |
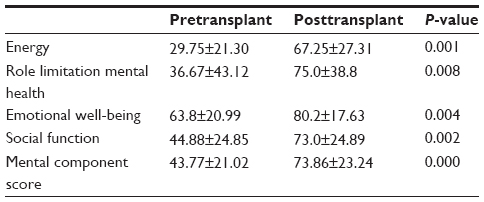 | Table 3 Mental domain scores |
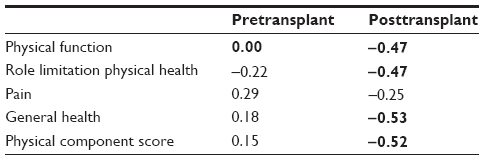 | Table 4 Physical domain scores with duration of pretransplant dialysis |
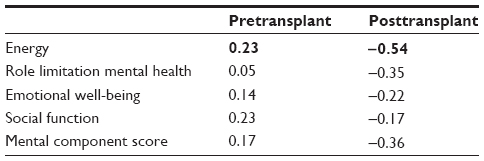 | Table 5 Mental domain scores with duration of pretransplant dialysis |
Discussion
The incidental finding of small renal lesions is increasing.12 Although most are benign, differentiating benign from malignant lesions is difficult.13 The choice of definitive treatment is between radical and partial nephrectomy. Although there is an increasing trend toward partial nephrectomy, radical nephrectomy is still significantly more common. In 2012, in Australia, there were 1,401 procedures performed for renal lesions less than 10 cm in size. Of these, 876 (63%) were radical nephrectomies.14 Although not all of these kidneys will be suitable as TRK grafts, it can be envisaged that a proportion of these, which would end up in the pathology laboratory otherwise, will be suitable for transplantation. A small renal cell carcinoma is less likely to have tumor recurrence and cause metastatic disease. There was no tumor recurrence encountered during median follow-up of 38 months. Therefore, utilization of a small tumor-excised kidney graft could allow more elderly people, who are otherwise unlikely to be offered normal deceased donor, kidney transplant. However, care needs to be taken during selection of potential recipients and acceptance of the kidney graft with a small tumor. A further study with a large number of patients and longer follow-up is necessary to confirm the safety by using tumor excised kidney graft for transplantation.
Kidney transplant has undisputedly improved the QoL in patients with ESRF. In 2012, there were 1,080 patients on the transplant waitlist in Australia. Only 606 patients received a deceased donor kidney transplant. The average time that patients are on the waitlist for a deceased donor kidney transplant was 3.8 years.1 The TRK program was implemented to address some of the issues highlighted above. Our patients were predominantly elderly with medical comorbidities, and without the TRK graft, they would still be on dialysis.
In this cohort, the recipients are selected from elderly people who are on dialysis. Age did not appear to have any significant impact on the QoL scores in a previous study.15 Although our study supports this, the age range in this study was possibly not wide enough to reflect a true result. There were also no significant differences between men and women in our study. Ogutmen et al2 found men to have better QoL than women. This could be due to cultural differences between the Australian and Middle Eastern populations. They postulated that Turkish women are thought to be more reliant on men and be confined to the house. In Australia, women are brought up to be as independent as men. This could account for the lack of difference in QoL between men and women in our study population. In addition, a limitation of this study was the small number of patients in the cohort. A recent study in France also found women to have decreased scores in HRQoL assessments. However, they did not offer any explanation for that observation.16
Not surprisingly, dialysis vintage was associated with worse scores for both physical and mental domains. Most of the physical domains and the energy component of the mental domains were statistically significant. The QoL has significantly improved after kidney transplantation and after the patient was off the dialysis. In particular, some of these recipients had never met the criteria for usual deceased waiting list. TRK grafting provides an opportunity for them to have kidney transplantation. Other studies have also found dialysis vintage to be associated with worse outcomes posttransplantation. Overbeck et al3 found that patients on the transplant waitlist for longer than 3 years had lower social functioning and support. They hypothesized that this could be due to loss of relationships and being more isolated. It is possible that patients on dialysis for longer duration are more depressed, and hence the general chronicity of their illness would cause them to have lower QoL scores.17 Prevalence of depression in transplant patients can be up to 76.5%.18 Patients may also have expectations that are not met by the transplantation.19
Patients with higher level of concern regarding tumor recurrence had worse HRQoL scores. This was not statistically significant. These patients could have restricted their social interactions as a result of their concerns. One patient addressed his willingness to be on dialysis if he had an option again as a result of his bad experience with the immunosuppressive agents, but he has expressed no concern of tumor recurrence. Most patients had minimal or no concerns regarding tumor recurrence. In our cohort, the follow-up range was from 13 to 74 months, and no tumor recurrences have occurred to date. All these patients are still under regular surveillance by our protocol.
This study has demonstrated that, in elderly people, the QoL has improved after kidney transplantation by utilization of a small tumor excised kidney graft. As selection criteria indicated, these recipients are otherwise unlikely to be offered kidney transplantation. The risk of tumor recurrence is minimal for a small renal carcinoma (≤3 cm). The recipients have almost no concern of tumor recurrence in the questionnaire survey. The limitation of this study is obvious as it is of a retrospective nature. The study cohort only had a small group of patients with limited follow-up time. Further study is necessary to continue the follow-up of these patients and extend the study cohort.
Conclusion
In conclusion, this study has shown that the patient’s QoL has improved significantly after kidney transplantation. There is almost no concern of tumor recurrence among these recipients. The limitations of our study are that first, we had a small cohort of patients. The study also relied on patient’s ability to recall their QoL retrospectively. Despite the small number of patients, our results clearly show an improvement in the QoL of these patients posttransplant. HRQoL is emerging as an important outcome measure in assessing the success of organ transplantation. The patients in this study form a unique cohort, which to our knowledge has not been studied before. We hope to do a prospective study on a larger cohort in the future.
Disclosure
The authors report no conflicts of interest in this work.
References
Leonie E, Stephen MD. Stock and flow. ANZDATA Registry 2009 Report. Adelaide, South Australia: ANZDATA; 2013. Available from: http://www.anzdata.org.au/anzdata/AnzdataReport/32ndReport/Ch01.pdf. Accessed December 12, 2015. | |
Ogutmen B, Yildirim A, Sever MS, et al. Health-related quality of life after kidney transplantation in comparison intermittent hemodialysis, peritoneal dialysis, and normal controls. Transplant Proc. 2006;38(2):419–421. | |
Overbeck I, Bartels M, Decker O, Harms J, Hauss J, Fangmann J. Changes in quality of life after renal transplantation. Transplant Proc. 2005;37(3):1618–1621. | |
Shrestha A, Shrestha A, Basarab-Horwath C, McKane W, Shrestha B, Raftery A. Quality of life following live donor renal transplantation: a single centre experience. Ann Transplant. 2010;15(2):5–10. | |
Ferrari P, de Klerk M. Paired kidney donations to expand the living donor pool. J Nephrol. 2009;22(6):699–707. | |
Fraser SM, Rajasundaram R, Aldouri A, et al. Acceptable outcome after kidney transplantation using “expanded criteria donor” grafts. Transplantation. 2010;89(1):88–96. | |
Mannami M, Mannami R, Mitsuhata N, et al. Last resort for renal transplant recipients, ‘restored kidneys’ from living donors/patients. Am J Transplant. 2008;8(4):811–818. | |
Montgomery RA, Locke JE, King KE, et al. ABO incompatible renal transplantation: a paradigm ready for broad implementation. Transplantation. 2009;87(8):1246–1255. | |
Nicol DL, Preston JM, Wall DR, et al. Kidneys from patients with small renal tumours: a novel source of kidneys for transplantation. BJU Int. 2008;102(2):188–192; discussion 192–193. | |
Buell JF, Hanaway MJ, Thomas M, et al. Donor kidneys with small renal cell cancers: can they be transplanted? Transplant Proc. 2005;37(2):581–582. | |
He B, Mitchell A, Lim W, Delriviere L. Restored kidney graft from urologist referrals for renal transplantation. Transplant Proc. 2013;45(4):1343–1346. | |
Jayson M, Sanders H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology. 1998;51(2):203–205. | |
Patard JJ. Incidental renal tumours. Curr Opin Urol. 2009;19(5):454–458. | |
Medicare Australia Statistics [webpage on the Internet]. ACT, Australia: Australian Government Department of Human Services. Available from: http://medicarestatistics.humanservices.gov.au/statistics/do.jsp?_PROGRAM=%2Fstatistics%2Fmbs_item_standard_report& DRILL=ag&group=36522%2C+36525%2C+36526%2C+36528& VAR=services&STAT=count&RPT_FMT=by+state&PTYPE=calyear &START_DT=201201&END_DT=201212. Accessed December 12, 2015. | |
Cetingok M, Winsett RP, Hathaway DK. A comparative study of quality of life among the age groups of kidney transplant recipients. Prog Transplant. 2004;14(1):33–38. | |
Gentile S, Beauger D, Speyer E, et al. Factors associated with health-related quality of life in renal transplant recipients: results of a national survey in France. Health Qual Life Outcomes. 2013; 11(1):88. | |
Zelle DM, Dorland HF, Rosmalen JG, et al. Impact of depression on long-term outcome after renal transplantation: a prospective cohort study. Transplantation. 2012;94(10):1033–1040. | |
Palmer S, Vecchio M, Craig JC, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. 2013;84(1):179–191. | |
Schulz T, Niesing J, Homan van der Heide JJ, Westerhuis R, Ploeg RJ, Ranchor AV. Great expectations? Pre-transplant quality of life expectations and distress after kidney transplantation: a prospective study. Br J Health Psychol. 2014;19(4):823–838. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.