")
Back to Journals » Patient Preference and Adherence » Volume 14
Trivial or Troublesome: Experience with Coronary Heart Disease Medication from the Patient’s Perspective
Authors Östbring MJ, Hellström L, Mårtensson J
Received 6 September 2019
Accepted for publication 11 January 2020
Published 27 February 2020 Volume 2020:14 Pages 411—424
DOI https://doi.org/10.2147/PPA.S230120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Malin Johansson Östbring,1,2 Lina Hellström,1,2 Jan Mårtensson3
1Pharmaceutical Department Region Kalmar County, Kalmar, Sweden; 2eHealth Institute, Department of Medicine and Optometry, Faculty of Health and Life Sciences, Linnaeus University, Kalmar, Sweden; 3Department of Nursing, School of Health and Welfare, Jönköping University, Jönköping, Sweden
Correspondence: Malin Johansson Östbring
Pharmaceutical Department Region Kalmar County, Building 2, House 2, Kalmar County Hospital, Kalmar SE-391 85, Sweden
Tel +46 70 289 32 55
Email [email protected]
Background: Living with coronary heart disease (CHD) usually means being prescribed several medications to help prevent new cardiac events. Using medicines for long-term conditions impacts on day-to-day life, and coping with medicines can be burdensome and can affect the quality of life. To enable better support of these patients, we need to understand their collective medicine-related experience.
Purpose: The purpose of this study was to describe patients’ medicine-related experience 1 year after the diagnosis of CHD.
Patients and Methods: A qualitative, descriptive study using semi-structured interviews was conducted in 19 patients in their homes or at Linnaeus University, Sweden. Interviews were recorded and transcribed verbatim. Qualitative content analysis with an inductive approach was used.
Results: Patients’ experiences with using their medicines after diagnosis of CHD differed considerably. Some patients found handling the medicines and administering their treatment very easy, natural and straightforward, while others found that it was distressing or troublesome, and influenced their lives extensively. There was a varied sense of personal responsibility about the treatment and use of medicines. The patients’ experiences were classified into one of seven categories: a sense of security, unproblematic, learning to live with it, taking responsibility for it, somewhat uncertain, troublesome, or distressing. Participants in the study who expressed an unproblematic view of medicine taking also often revealed that they had dilemmas or uncertainties.
Conclusion: Patients’ medicine-related experiences after CHD vary greatly. The findings of this study highlight a need for more individualized support for patients using medicines for secondary prevention. The patients often needed better dialogue with healthcare providers to optimally manage their medicines. Medicine-related support for these patients should encompass various aspects of medicine-taking.
Keywords: coronary artery disease, qualitative research, patient experience, medicine management
Introduction
An increasing number of people live with coronary heart disease (CHD) today because an aging population and the development of acute and secondary treatment options have resulted in more patients surviving and living longer.1–3 Improvements in the acute treatment of CHD, with the widespread use of percutaneous coronary interventions, have resulted in fast physical recovery of patients and shorter hospital stays. However, the time available for education about the disease and what is expected of the patient in terms of secondary prevention have also subsequently been limited. Successful rehabilitation after CHD presupposes that patients are provided with sufficient education, counselling and psychosocial support to cope with all consequences of the disease.4 However, short hospital stays have not usually been accompanied by correspondingly expanded out-patient follow-up services. Substantial deficits have been seen in patients’ knowledge and understanding of the disease and the required prevention measures, highlighting the need for revision of cardiac rehabilitation programs.5,6
Living with CHD usually means being prescribed a series of medications (eg, aspirin, antiplatelet agents, a statin, a beta-blocker, an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, nitroglycerin spray) for the prevention of new cardiac events.7 In order to obtain the full benefit of these medications, patients must adhere to the prescribed regimens; however, studies reveal that patients sometimes stop taking their medicines after the first few months and that nonadherence increases with time after the diagnosis.8,9 Poor adherence to secondary prevention is thought to be one of the reasons for treatment goals not being met despite established guidelines and widespread access to effective and inexpensive medicines,10,11 resulting in increased morbidity and mortality.12–14
Adherence to medical treatment regimens is a complex act requiring both motivation and ability; nonadherence can, therefore, be either intentional or unintentional.15–17 Unintentional nonadherence occurs if the patient wants to adhere but is unable to because of difficulties with understanding instructions, affording costs, or remembering to take the medication, or for other practical reasons. Intentional nonadherence occurs when the patient decides not to follow the recommendations. Depression is associated with lower levels of both unintentional and intentional nonadherence to cardiac medication and has been associated with increased risk of cardiac events.18,19 However, in general, factors influencing unintentional and intentional adherence are different and need different management.20
Adherence to medication regimens is influenced by the patient’s attitude towards their medications. This can be assessed using the Beliefs about Medicines Questionnaire-Specific (BMQ-S) instrument, which measures beliefs about the necessity for medicines or concerns about medicines, on two scales.21–23 The patient’s beliefs are important determinants of both intentional and unintentional adherence and changes in beliefs have been linked to changed adherence behavior.21,24–30 Based on the BMQ-S, patients can be classified as accepting, ambivalent, indifferent or skeptical in their attitudes, each having a specific effect on their likelihood of being adherent.31,32 Most patients, with various diseases, are accepting or ambivalent, believing their medications are necessary; ambivalent patients also having serious concerns about medicines. Indifferent or skeptical are less common attitudes.32,33 Patients with CHD become more concerned about their medications during the period after the event,34 which could explain the worsening adherence among these patients.8,16,35 Being discharged with more than seven medicines, not receiving a medication list, and believing that the healthcare provider did not listen to them were factors associated with a higher risk of increased concern.34
Using medicines for long-term conditions impacts on day-to-day life, and coping with medicines can be burdensome and can affect the quality of life.36 In the early recovery phase after an acute coronary event, patients might consider medicines as intrusive and as the cause of many of their symptoms.37 They can find it hard to understand their treatment and this can generate concerns about potential side effects.38 A study of medication-related perspectives among patients who had been using medications for an average of 2.5 years found that they thought about their medicines and wanted to understand their treatment, but the level of information they wanted differed among the participants. The beliefs they held about both the disease and the medicines also influenced their decisions about the treatment.39 A review of interview studies of patients with CHD, or patients receiving similar preventive treatment, explored concepts relating to how patients perceived their medicines and their perspectives on adherence. These perceptions about the disease and about taking their medication and the patients’ relationships with the clinicians were found to be central factors influencing medication-taking behavior.40 These studies have all had a general aim, covering medication-related experiences in general,37 studying patients’ experiences with chronic medicines in general,36 or focusing specifically on factors affecting medicine-taking and adherence.39,40 However, little is known about how patients with CHD reason about their medicines, what support they have and what affects their thinking about medicines.
Since we are currently developing an intervention for improving pharmaceutical care for patients with CHD, we require a better understanding of how patients in our setting experience medicine-taking so we can find ways to better support them.41,42 The purpose of this study was, therefore, to describe patients’ medication-related experiences over the first year after diagnosis of CHD.
Materials and Methods
Study Design and Setting
A qualitative study using a descriptive approach with semi-structured interviews was conducted. The participants were 19 patients who had been diagnosed with CHD and had their secondary prevention follow-up meeting at the cardiology clinic of a county hospital in the south of Sweden. The standard follow-up procedure for patients like these included an appointment with a cardiac specialist nurse within 3 weeks of discharge, and an appointment with an assistant physician or cardiologist about 2 months after discharge. All patients were also offered cardiac rehabilitation for about 4 months at the hospital or at a primary-care facility closer to home.
Data Collection
Patients who had been diagnosed with CHD during June–December 2014 were recruited from the healthcare register of the county council. Patients were included if they had a coronary angiography accompanied by a diagnosis of angina pectoris, myocardial infarction, or another acute or chronic ischemic disease. This yielded a list of 131 patients, identified only by their social security numbers. Patients were subsequently excluded if they had had prior CHD, lived outside the area, had a coronary artery bypass graft (CABG), had dementia, had a record of drug abuse, had not attended the follow-up meetings, or seemed too ill with other diagnoses. This left 75 patients, 45 of whom were selected as possible candidates using purposeful sampling. The aim of this sampling method was to ascertain variation in age, marital status, type of CHD, presence of co-morbidities and discharge date. The selected patients were contacted by a letter which described the study and informed them that the interviewer would contact them via telephone within a week to ask for their participation. Letters were first sent to 16 patients who had had a CHD event in the summer of 2014, and these patients were then contacted by phone. Some could not be reached by phone and a few did not want to participate in the interviews because they did not feel they had enough to share, or they had other priorities. Letters were then sent to more patients, those who had had a CHD event later in 2014, bringing the total to 35 patients contacted by letter and 19 who consented to participate. After the interview, the participants were asked to complete the BMQ-S. This questionnaire was used to control for variations in the attitudes of the sample; it was applied after the interview so that it would not influence data collection for the study. The characteristics of the participants are presented in Table 1.
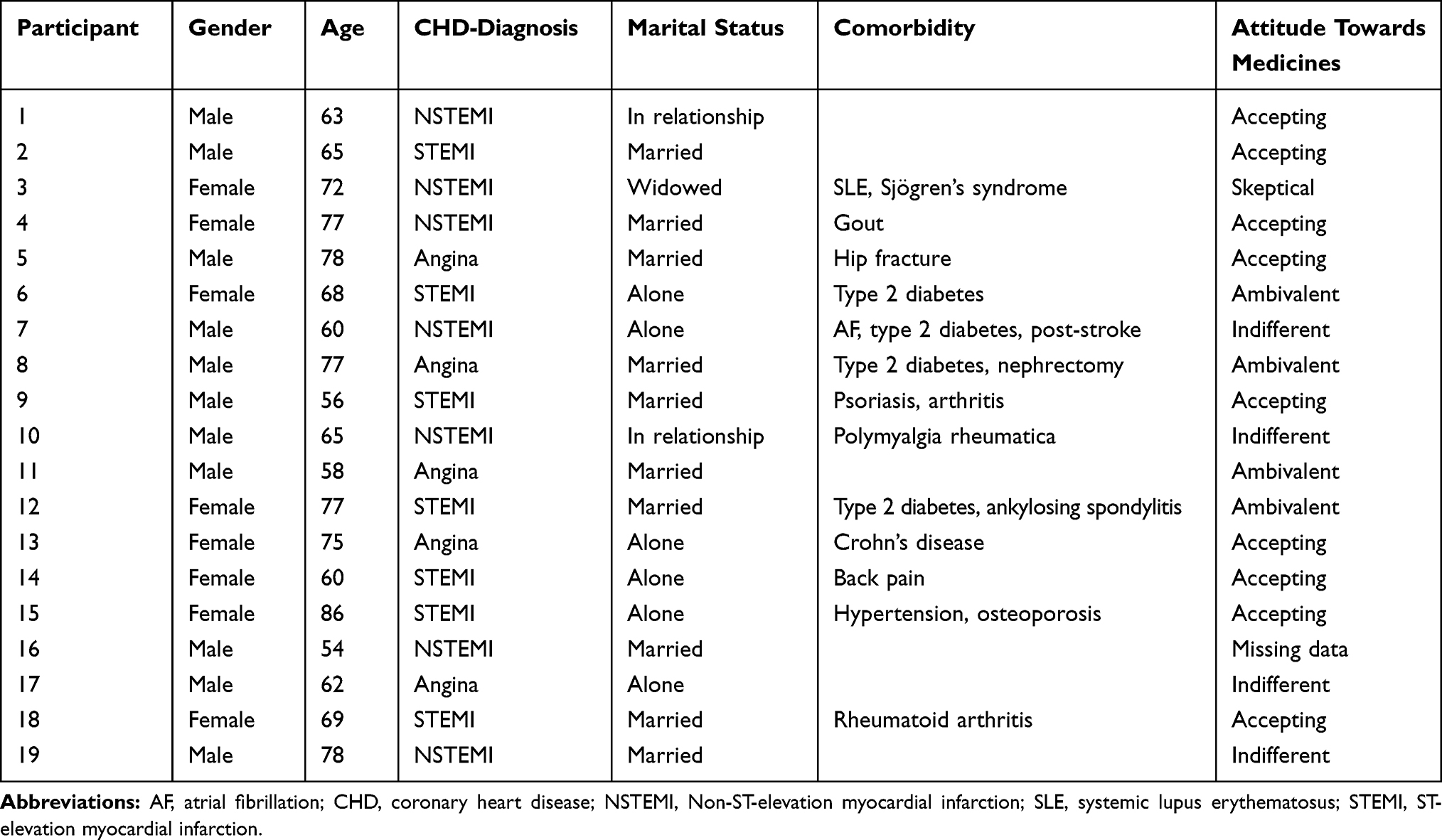 |
Table 1 Characteristics of the Participants |
Interviews
Interviews were conducted by the first author in the participant’s home (16) or in the first author’s office (3), whichever was desired by the participant. The interviewer introduced the aim of the study and asked the participant to put their medicines on the table in front of them so that pill boxes would give cues for the interview. The first three interviews were recorded and transcribed so that the interview guide and the researcher’s performance could be reviewed with the last author. After this review, the semi-structured interview guide was supplemented by the addition of examples of follow-up questions and probes to get more in-depth responses during the interviews (Table 2). Another 16 interviews were then conducted during September–November 2015 and these were then analyzed together with the first three. Interviews took between 20 and 110 min. The interviews were recorded and later transcribed verbatim. One recording failed because of technical error, so 18 interviews were transcribed, three by a research assistant and 15 by the first author. The collected data then constituted 240 pages of interview transcripts.
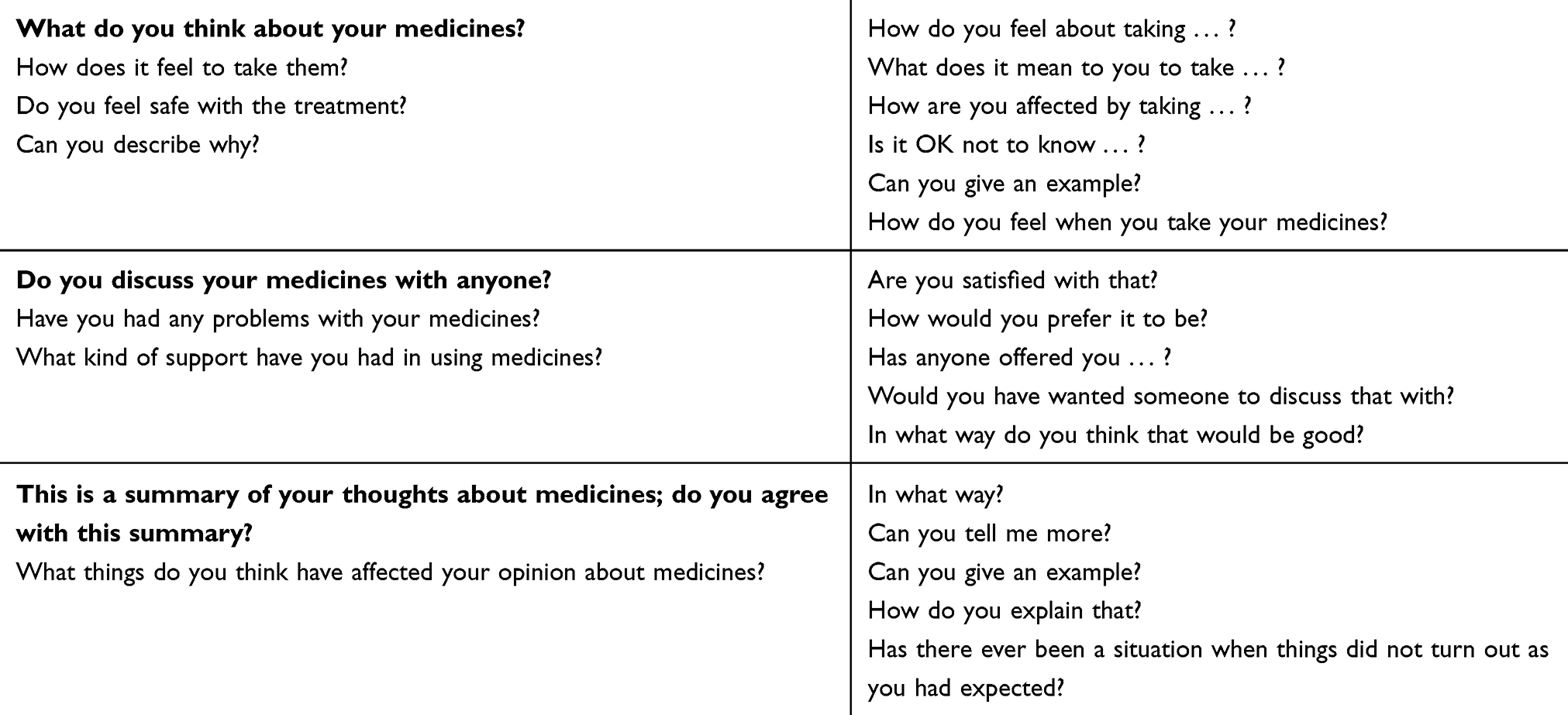 |
Table 2 Interview Guide Used for Interviews 4–19, Main Questions in Bold |
Data Analysis
Qualitative content analysis with an inductive approach has been previously described by Elo and Kyngäs.43 The recordings were listened to carefully, in order to proof-read the transcripts, and to get a sense of the whole. The transcripts were then read through to find the meaning units that corresponded with the study aim. The initial codings for, or condensed summaries of, the meaning units were written in the margin of the transcript as a form of open coding. The context of the whole interview or a typical area of content was considered when deciding on the codes.44 Each interview resulted in between 10 and 50 codes, which were collected in an Excel spreadsheet (500 codes in total). Similar codes were combined to form about 50 groups, which were then compared for differences and similarities before being regrouped and merged to form sub-categories, based on their meanings. The abstraction process was guided by the concept of a code belonging to a sub-category more than just being similar in content.43 Sub-categories were freely formed from the groups in this manner, and later categories emerged from the sub-categories (Table 3). All the steps in this collection and analysis process were performed by the first author, with insights from the actual interviews in mind but also with ongoing dialogue with the last author for guidance in the methodology. The first author has 10 years’ experience as a clinical pharmacist talking to patients about their medicines in clinics, wards and educational groups and is familiar with the research field. The last author has extensive experience as a nurse in cardiology and in using qualitative methods.
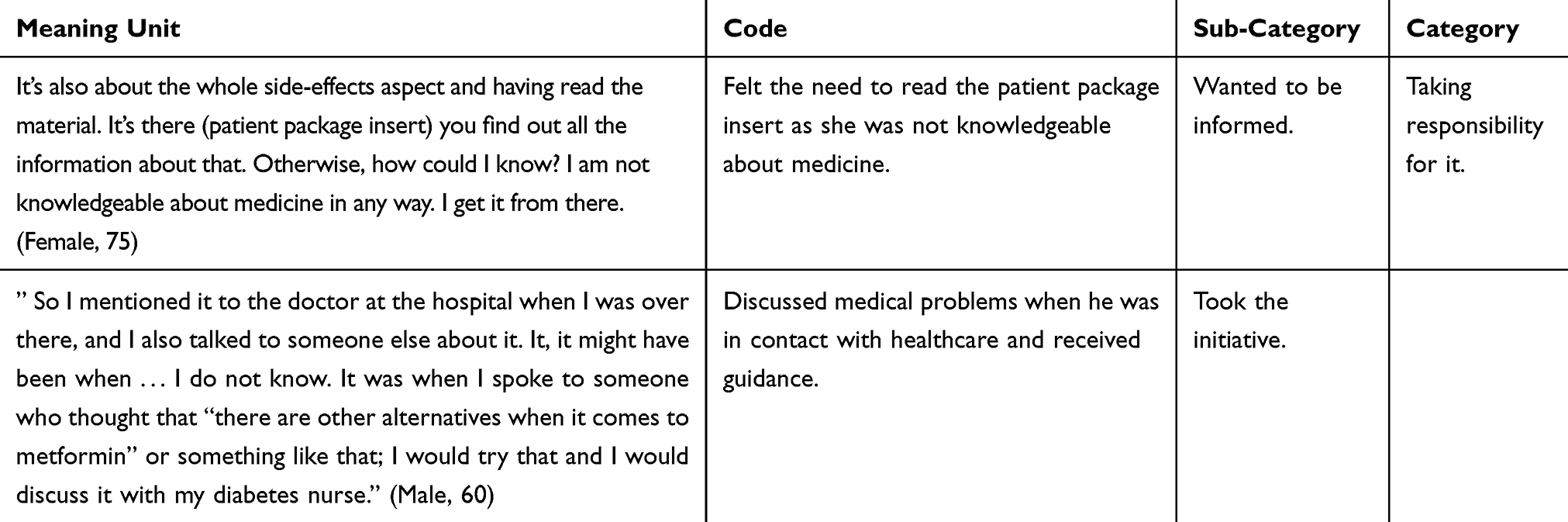 |
Table 3 Example of the Analytical Process |
Ethical Considerations
The investigation conformed to the standards described in the Declaration of Helsinki. The study was approved by the Regional Ethics Committee in Linköping (Dnr 2014/506-31). Participants were given written and oral information about the study and gave written consent to participate. Participation was voluntary and participants could at any time and without explanation choose to withdraw from the study. Codes were used instead of personal data in all audio files, transcripts and analyses to ensure confidentiality.
Results
Analysis of the interviews revealed that the participants varied in their response to the handling of and treatment with medicines after diagnosis of CHD, finding it very easy, natural and straightforward, or distressing, or mostly troublesome. Participants also had different feelings about taking responsibility for their treatment and the use of medicines. Some felt concerned about taking medicines and some felt secure in taking them, but no one mentioned that they had noticed a positive therapeutic effect from taking them. These responses associated with medicine-taking after CHD were characterized into seven categories (Table 4).
 |
Table 4 Categorization of Medication-Related Experiences from the Perspective of 19 Patients After a Coronary Heart Disease Event |
Sense of Security
The category “sense of security” describes participants’ experience of feeling secure with their medicines, because they trusted the doctors and the health system, and trusted that they were being treated in the best way. They also felt safe because they thought that the medicines protected them from worsening of their condition and because they felt that the treatment had been individualized for them in some way. They knew they could discuss any dilemmas with someone, which also made them feel secure to be taking medicines as part of everyday life.
"Trusting the doctors", and the health system, was the reason participants felt safe with their medicines. The extensive research behind this type of treatment, and the fact that all patients receive the same medicines was also mentioned as good reasons for putting trust in the treatment. The participants who expressed a sense of being "protected by the medicines" said they knew that they had medicines that reduced the risk of new events. One participant commented that the medicines were like a lifeline and explained: “Yeah, if I stop, if I stop taking them, this problem, this thing with my coronary arteries will get even worse and then the risk that I’ll have another heart attack will be higher I think.” (18) Some participants mentioned that they had had confirmation of the effects of their medicines on, for example, their cholesterol levels. Having the nitroglycerin spray nearby also felt like being protected by a life guard. Being "treated as a partner" and deciding on the treatment together, taking individual factors into consideration, helped participants to trust that the medicines were right for them. “So he thought my blood pressure was too low. So it was because of that; yes, we spoke about that too, and together we decided to reduce the enalapril.” (10) Having "someone to talk to" and discuss the treatment with, a relative working in healthcare, or another doctor, made participants feel safe when managing their drugs. Some used this as a sort of second opinion which made them feel sure of the treatment; for others, it was more the sense that they had someone to turn to that gave a sense of security. “So I choose the channel that is easiest and that’s my siblings really, because they’re in healthcare.” (16)
Unproblematic
The category “unproblematic” describes participants’ experience of accepting medicines into their life with ease. When something came up it was easily taken care of, medicines were not on their mind, they just took them and got on with their lives. They had not noticed anything different in their health; they felt well, so they guessed everything was all right. They might not know so much about their medicines but they were confident, they were happy not knowing because decisions were not up to them. Falling ill and having a bunch of medicines was something that just happened to them and they accepted it easily.
Some participants said "I just take them", and that they never thought of it as anything special. It was no big deal, because they had accepted that they needed them. “I don’t really think anything about them at all (the medications); they’re just part of my life right now.” (16) It was also experienced as a" straightforward process"; when something occurred it was easily taken care of and then put in the past. A new status quo was instantly found, so even though they had had complications they did not consider the medicines as problematic. When they needed new prescriptions they knew where to turn and the pharmacy had the medicines they needed in stock. Participants expressed that they were "still feeling well", the medicines had not made them tired, drowsy or nauseated, which they thought characterized the side effects of medicines. They thought that because they felt the same as before, the medicines could not be bad for them in any way. “Yeah, when you don’t get any side effects or anything, no nausea or … anything like that … that I notice.” (12) Participants said that they "knew all they needed" because they felt comfortable with their medicines even though they did not know all there is to know. Some participants even acknowledged that they did not know much at all but they were happy that way because they trusted others and they did not want to take any more responsibility. Participants said that the medicines had been "easy to accept" because they were instantly convinced about their need for them. They might have to live with a few side effects but that was not a problem in the bigger picture.
Yes, but now I’ve been given that (warfarin). Yes, now I think that way (that I need it). In any case, they have explained how it’s related and why I should have it. And it’s no problem that it (the blood) runs a little easier. It works for me. (7)
Learning to Live with It
The category “learning to live with it” describes the experience of participants in adapting, ie getting used to thinking of health and medicines in a new way, and making medicines a part of every-day life. Some participants described this as a process that had ended, they had adapted their way of life and thinking. Others might still be learning because they thought of their medicines as a necessary evil, but they did live with them. This was an experience of accepting the medicines and the new state of health, of overcoming difficulties, in a thoughtful, conscious way. Some participants also decided not to read about side effects because they sensed that this might make them too attentive to them.
"Coming to terms with medicines" describes the experience of adapting to a new routine or adapting to a life with medicines, accepting the situation after initial hesitation. It took some time to get used to the thought of having to take medicines, but then they found a routine and got on with it. “It took a while before I knew what to do, to remember to take them, you know.” (14) The experience also sometimes involved learning how to relate to side effects or feelings of insecurity, but all these experiences ended up as some sort of acceptance of a new situation. Participants said that "reflecting on medicines is a part of everyday life"; that they had been thinking about their medicines sometimes without taking any action. They reflected in a more general sense on what the medicines did for them, or thought about how to best take them. A "necessary evil" was how some participants described their medicines as something they were not keen on, because they knew they could cause side effects or they had always thought that you should take as few medications as possible, but they understood that they had to take these medicines because of their disease. “I think it’s a bit scary with all the medication you take of course, but well … sometimes it’s necessary and so you just have to do it.” (15) "Creating a routine of ones own" describes participants’ experience of making medicine-taking a routine, or organizing medicines in the best way for them.
Well yes, I take them out of the packaging but … both yes and no … I have a smaller box that I use … One sheet of pills, the various sheets in it. So I don’t have to deal with the boxes every time. They are very big after all.//And then I put it on the kitchen table in the evening so I don’t forget to take them. (13)
It was also expressed how they managed their medicines as a habit, both the habit of taking them with breakfast and the habit of filling the pill dispenser with what they were used to, without the list of prescribed medicines as an aid. Participants said that if they forgot their medicine it was usually because their routine was disrupted. For some participants, this happened often, usually with the pills to be taken in the evening.
Taking Responsibility for Their Own Treatment
The category “taking responsibility for it” describes the participants’ experiences with respect to taking responsibility for their own treatment in some way. This experience could be a conscious sense of responsibility for the treatment or the experience that they had to take the initiative for something to happen. It could also be the experience of making their own decisions about the treatment, for instance deciding not to take a medicine that they felt bad about.
Some participants "wanted to be informed" about side effects, and actively sought information about this in order to have a sense of control over what they might be faced with. “Yes, that I have a certain control. And don’t just say that I’m feeling terrible, so terrible. Instead, I know what the deal is.” (18) "Taking the initiative" describes the experience of deciding to discuss or change medicines. This covered how participants had acted upon various cues to handle problems, like contacting their primary-care physician when they suspected a side effect, or arranging for their prescribed medicines not to be exchanged for a generic version. Problems were handled and solved because of their own initiative. Participants could also "feel in charge of their own health" because they sensed that the quality of their treatment was their responsibility too, not just that of the doctor. They thought that it was up to them to decide about the balance of risk and safety, or that they had to take responsibility for their body because they knew it best. “I take on that responsibility myself. I have to assume responsibility for myself, so to speak. It is too important for someone else to take that responsibility.” (10) Some participants said that they had "decided for themselves" about the treatment. This did not necessarily mean that they were disobeying the doctor’s prescription, they just saw it as the natural consequence of taking responsibility for themselves, and thought that the doctor would probably agree with the decision if they had had the possibility to discuss it. Participants sometimes solved a problem regarding their medicines by acting on their own and they knew that they were doing this outside of the doctor’s prescription. Problems managed this way included contraindications, interactions, or the feeling of having too many medicines, so the participant decided to skip or take fewer medicines that they felt were not prioritized, like antidepressants or analgesics.
The doctor actually told me, I need to take it all the time if it’s going to have an effect. And I thought that there’s so much here that I … So I have sort of forgotten (put away) this tablet. (12)
Side effects were managed by one patient by slightly lowering the dose of the beta-blocker. One participant had received a prescription for sildenafil to take for only 2 months, from his primary-care physician, but since he had not heard of any time restraints from the cardiologist, and this medicine was so important for his quality of life he had decided to use it for longer periods. He said that he had not inquired further about possible restraints because he did not want to know more, he had made his own decision.
Somewhat Uncertain
The category “somewhat uncertain” describes participants’ experiences of not being entirely sure about the treatment without any objective facts or real worries. These participants took the medicines even though they had some doubts about actually needing them. They may also have felt that they did not have all the necessary information or knowledge to feel confident in managing their medicines. They felt that there were uncertainties surrounding their treatment.
"I take them but I am not sure I need them" describes the experience of not really committing to the need for medicines. They might have thought there were other alternatives but had accepted the prescription, or they might not have understood or known their purpose.
I still function after all. Like today, when I forgot to take them. I have kept functioning either way. I know that I have forgotten them once in a while, and I’ll be walking down town. I feel tired, for sure, but that could be due to something else, after all. But I don’t feel like I miss them, you know (when I’ve forgotten them). (6)
"Missing information" describes how participants’ have experienced a lack of knowledge or have wanted more information so as to feel certain about their medicines. "Lack of someone to discuss with" was expressed by participants who wished their doctor could be more accessible for discussing their treatment. “And you have a lot, possibly too much, personal responsibility if you ask me. Because even if you get it, that’s not enough, you need to discuss things sometimes.” (7)
Troublesome
The category “troublesome” describes participants’ experience of the medicines as something that caused them trouble. This could have been that they were hard to manage, that it was just a tricky job to get them in the pill dispenser, or that the medicines were a nuisance because their side effects impaired their quality of life; they felt that they had to adapt their way of living because of the effects of the medicines.
Participants sometimes experienced the actual managing and handling of medicines as "inconvenient and fussy"; it was bothersome because it required detail, and pills were small, numerous, and similar looking. “I guess I just felt that there were a lot to keep track of to get it right … There are so many pills, so it’s … I understand if people get it mixed up.” (4) Renewing prescriptions could be troublesome when participants did not feel confident of whom to turn to, or when they were unexpectedly faced with referrals to primary care. Some participants said that they were "disturbed by the generic exchange" because they had to keep track of the names, because of the inflexible system and because of the fuss in the pharmacy. It was also "annoying to easily bleed" because it resulted in a fuss, either related to applying plaster and dealing with blood stains, or because of having to request particular care, or justify bruises. Participants felt that they were "restricted in every-day life" when they avoided activities because of the risk of bleeding, when they had felt fatigued or impeded by the effects of a beta-blocker, or because they could no longer relieve their pain with non-steroidal anti-inflammatory drugs. They also felt restricted in a sense because they could not just take their pills in the morning and get on with their life, because they also had to take pills in the evening.
Yes, it’s easier to just have one thing that you …, you get up, get dressed, eat breakfast and then just take it. And then … Then you get on with living. It doesn’t matter where you are at night, if you are out dancing or whatever, you don’t need to check the clock. (17)
Some participants said that they had "experienced side effects" like having nightmares, gastrointestinal problems and feelings of dizziness, some also had to seek acute care because of this. Some had put this in the past by changing medicines and others had to live with the side effects.
Distressing
The category “distressing” describes participants’ experiences of concern about their medicines, of feeling unsafe about them. The sense that something was not quite right, either with how the medicines affected the body, or with distrust in the encounter with healthcare representatives or pharmacy. Worries also arose from the exchange of medications for a different generic version at the pharmacy, with some receiving different brands each time. Participants could "feel bad about taking the medications". This entailed concerns about taking too many medicines, about the combination of medicines, or about how medicines would affect the body in the long run, and some participants also had symptoms which they thought could have been caused by the medicines. "Distrust of healthcare or pharmacy" could arise in encounters related to medicine taking, which gave participants a feeling of insecurity, not knowing who to rely on, and doubts about the medicines. “Never heard of it, he said, the vaginal thing that is. That it could give (cardiac side effects). But why does it say that, I ask you as well, why does it say that?” (13) Some participants described how it was "worrisome to get new generics" because they worried about different effects and side effects when they received a new brand. “And you think: will I tolerate this one, or will I not? What will happen?” (6) An "unwelcome reminder of ill health" was how some participants described the medicines: they reminded them that they were no longer free from disease. This could be in the sense that they were reminded of their disease each time they had to take their medicines. “It’s a constant reminder. What you want to do is leave all that stuff behind you, that you have had a heart attack, but you actually end up being reminded of it every day.” (14) It could also be in a more general sense that when they thought of their medicines they got a negative feeling because medicines reminded them of illness.
Discussion
The aim of this study was to describe the experience of using medicines from the perspective of patients with CHD. The findings showed that the use of medicines could be viewed as trivial or natural, but it could also influence day-to-day life, routines and thoughts extensively. Some participants truly live with their medicines, they think about them, they might be distressed or troubled by them; and others just take them. Feeling a sense of security with medicines, ie, putting trust in the knowledge of doctors and the rigor of the health system, did not necessarily mean that the participants were untroubled or not distressed by their medicines. Participants in the study who expressed an unproblematic view of medicine taking also often revealed that they had had dilemmas or uncertainties. Altogether, the findings of the study highlight the need for more individualized support for patients who use medicines for the secondary prevention of CHD. Based on our findings, this support needs to encompass various aspects of medicine-taking.
Relationships and Interactions with Clinicians
In line with what others have found in more general studies of the same population,40 the participants’ medicine taking was influenced by their perceptions about the disease and the medication, and their encounters or relationships with health professionals. When the participants felt secure, it was partly because they trusted the doctors and felt that they were listened to and treated as a partner. This trust in the doctor and satisfaction with the relationship has been linked to medication beliefs and patient adherence.34,39,40,45,46 Considering the low fulfillment of treatment goals in secondary prevention10,11 it is of great concern that many patients with cardiovascular medication mistrust that their doctors will choose the right treatment for them or perceive that their concern about the drugs has not always been taken seriously.47 Several studies support the notion that patients often experience a reluctance in doctors or other healthcare professionals to discuss the risk of adverse effects.48–51 In our study, a feeling of uncertainty, as opposed to security, was connected to a lack of information. Participants were not asked about the specific information they had been given or what they did not have, but they nonetheless mentioned missing information or not knowing enough about their need for drugs, as in a recent study of patients who had undergone percutaneous coronary interventions (PCI) in Norway.48 Several other studies have also mentioned a lack of information and, perhaps more importantly, have found that patients need very different types of information, adapted to their own personal situations, and that the kind of information needed varies over time.39,49,50,52–54
The findings in our study associated with the active experience of learning to live with medicines, and taking or feeling responsibility, reflect how medicines are included in the everyday life of patients. Being active in this sense also meant that participants considered themselves to be active partners with healthcare personnel in treating or preventing the disease. Perhaps most importantly, the participants differed in the way they wanted to take responsibility for their treatment. Some said that they relied on their doctors to give them the right treatment and wanted to refrain from engaging, while others saw themselves as valuable partners in the management of their own health. This is not a new finding,36,39,40,46 but we still do not have a follow-up management plan ready to meet these differing needs. This is reflected in the participants who felt that they were missing information and someone to discuss things with, because they needed the health professionals to be easily accessible if they were to feel like an active partner. The health professionals must be able to individualize the information and, through the continuing relationship, be ready to repeat information and adapt it to their patients’ experiences.36,46,54 It is also evident from the literature that health professionals need to be more interested in the patients’ views on health, the risks of medicines and how they feel about taking them.36,39,40,47,54 Participants in this study who experienced medicine-taking as troublesome and distressing might have been relieved of some of these burdens if health professionals had opened a dialogue and questioned them about their perspective. Other participants did not explicitly report that they wanted someone to discuss their medications with but they did say that they had solved problems by themselves. They were left alone with decisions that they ought to have discussed with a doctor (or other healthcare professional). Like the old woman who decided not to take her antidepressant, because she had so many medicines now. Patients make decisions that seem rational to them, within their knowledge and context, but that might have been better if their knowledge and perspective had widened through a respectful discussion with a health professional.45,54,55
Personal Beliefs, Routines and Experiences
Most of the participants in this study reported high necessity beliefs (BMQ-S), but in the interviews, no one mentioned that they had had any positive effects from them. This is not surprising, as most of the relevant medicines are preventive rather than for treating symptoms. Participants in this study reported that they felt protected by their medicines; this has previously been described as a safety net.39 But it is still interesting to note that the participants did not mention an experienced need for the medications. This finding could perhaps explain why adherence to treatment among patients with CHD, as opposed to other chronic diseases, is not strongly correlated with a belief in the necessity for treatment.56 Thus, for patients with CHD, the correlation between beliefs and adherence is mainly linked to patients’ concerns. It could be that when asked about the necessity for the drugs in the BMQ-S, patients’ answer according to the information they have received and what they know, but this may not be an emotional belief, since they do not experience a need/necessity for the medication. Thus, because it is not an emotional belief, it would not influence their behavior with respect to adherence as much as it otherwise would.39
Participants in the study had created their own routines or systems for taking their medications, consistent with other studies.39,48,57 The participants used different systems but all related some system which they used to remember to take their medicines. Many used a pill dispenser, which they filled every one or 2 weeks. Taking the pills this way in the morning with breakfast was considered easy: “I just take them.” These participants had made it a habit and did not reflect on their medicines as they took them. The role of habit has been highlighted in adherence research58,59 and it is evident that forming a habit around taking medicines is important to avoid missing doses (unintentional nonadherence). However, this habit could also facilitate intentional adherence, because the description of the dispenser as an easy way of taking daily medicine implies that there is some ambivalence about taking the medicines on a daily basis. Ambivalent patients (according to the BMQ-S) hold strong necessity beliefs, which make them want to take the medicines (intention), but also have strong concerns, which discourage them from taking the medicines. Using a pill dispenser perhaps limits the ambivalence to the day of organizing the tablets: this is when they make a new decision on whether to adhere to the regimen for the next period. This is one way that beliefs about medicines and forming habits might interact and influence adherence.
For some participants, their medicines were no more than an unproblematic routine, while others found it bothersome to take medicines even though they had routines for it and used a pill box. Having a complex regimen with administration more than once a day is associated with lower adherence46 and participants in our study found that multiple administrations restricted them in their everyday life and, in line with others, that the evening doses were more likely to be forgotten.36,47,48 This shows the significance of tailoring medicine dosages for individual patients, and indicates that it is often worth questioning the therapeutic need for twice-daily dosages, or any absolute dosage regimen. Some participants also said that the medicines themselves were a reminder of their disease and that having to take medicines more than once a day made them live with the disease more than if they could just take their medicines with breakfast and go on with their lives. This is an important example of how medicines and patient adherence cannot be isolated from the whole experience of becoming ill and the emotions connected with this.48,55 This is part of the medication experience described by Shoemaker as an individual’s subjective experience of taking a medication in his daily life, captured in four themes.60 The theme “a meaningful encounter” describes how the encounter with a medication is filled with meaning such as the sense of losing control (of health).
The patient’s medication experience, as well as their different personality traits, will influence their beliefs and how they perceive medicines, and will, therefore, affect how they are best supported. The term concordance has been described as “a new way to define the process of successful prescribing and medicine taking, based on partnership.”61 It is based on the notion that consultation between patient and prescriber is a negotiation between equals, who might have differing views. In this sense, it is equivalent to person-centered care because it endorses the patient as an expert.54,62 Concordance is about achieving constructive and respectful partnerships.61 As concordance was proposed and welcomed twenty years ago,63 but can hardly be said to have hit the scene yet, perhaps it will be outrun by person-centered care and “What matters to you?”.64–66 Post-discharge follow-up and cardiac rehabilitation are now in need of revision because treatment goals are unmet (34, 37) and patients’ knowledge is found to be limited (5). However, care must be taken not to impose our goals as healthcare professionals onto the patients without regard to their personal perspective.
Methodological Considerations
The trustworthiness of qualitative content analysis can be described in terms of credibility, dependability, conformability and transferability.44 Choosing interviewees with different genders, ages and experiences contributes to an increase in credibility. To ensure broad variability, we used purposeful sampling and made sure that the participants differed in their demographic characteristics (see Table 1). It also strengthens the credibility of the study that the participants had different attitudes to their medicines according to the BMQ. Transferability was supported by the purposeful sampling of participants from diverse backgrounds and was confirmed by “a rich and vigorous presentation of the findings together with appropriate quotations.”44 Since all participants were recruited from the same hospital, however, transferability beyond the local study area may be limited. To ensure dependability, three pilot interviews were conducted by the first author and reviewed by the last author before the remaining interviews were conducted. To strengthen dependability, the first author was the only one who conducted the interviews, transcribed them verbatim, and proof-read the transcripts, thus making this aspect consistent.
Conformability was achieved by following the recommended steps in the analytical process, as suggested by Elo.67 The first author’s previous clinical experience and understanding of the participants’ contexts might have influenced the interpretation of the data. However, open dialogue among the authors helped to reduce any potential bias and our different perspectives as pharmacists and nurse helped to increase comprehensiveness and contribute to the sound interpretation of the data. Analyses were carried out in close collaboration with the last author, who has extensive experience with qualitative research methods. Categories and sub-categories were also discussed with LH, who is a pharmacist in cardiac care.
Clinical Implications
In this study of patients’ experiences of medical secondary preventive care, we found that patients often need better interactions with healthcare providers to manage their medicines in the best way. This improved dialogue should be based on either concordance or person-centered care, both of which focus on relational aspects. Our findings particularly emphasize that when medicines are managed with the patients, the offered support should encompass all the relevant aspects of medicine-taking.
A follow-up program for patients with CHD based on person-centered care could use knowledge of the patients’ challenges with medicines, and their experience of them, to improve the treatment experience for each individual patient.48,68,69 Poor adherence to treatment is only one of the many problems that can arise to make the treatment outcome suboptimal. Understanding that the patient’s experience of taking medicines can be a factor behind many drug-related problems also indicates that their personal information is valuable, and can help provide effective support for them.68
Knowledge of the patient’s beliefs about their medicines can guide healthcare professionals in how to approach them at the first appointment and how to plan the follow-up. Using the BMQ in clinical practice is also a way to ensure that these more personal aspects of medicine-taking are taken into account.
Patients need personally tailored medicine regimens, where the dose and dosage of the medicine is guided not just by the effects and side-effects of the drug but also by how it is experienced by the patient. Patients also need personally tailored information, where the amount of information and the way it is communicated are adapted to the patient’s need.
Healthcare professionals who support patients in secondary prevention need to assess patients’ thoughts about and feelings for their medicines, and also to understand that patients feel different levels of responsibility with regard to their treatment.
Conclusions
The experiences of patients using medicines after CHD vary greatly. The findings of this study highlight the need for more individualized support for patients using medicines for secondary prevention. We found that patients often need better dialogue with healthcare providers to manage their medicines in the best way. Our findings emphasize that when support in managing medications is offered to patients, it should encompass various aspects of medicine-taking.
Acknowledgment
This work was partially funded by the Medical Research Council of Southeast Sweden.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bhatnagar P, Wickramasinghe K, Wilkins E, Townsend N. Trends in the epidemiology of cardiovascular disease in the UK. Heart. 2016;102:1945–1952. doi:10.1136/heartjnl-2016-309573
2. Socialstyrelsen. Myocardial Infarctions in Sweden 1994-2014; 2015.
3. Roth GA, Forouzanfar MH, Moran AE, et al. Demographic and epidemiologic drivers of global cardiovascular mortality. N Engl J Med. 2015;372(14):1333–1341. doi:10.1056/NEJMoa1406656
4. Piepoli MF, Corra U, Adamopoulos S, et al. Secondary prevention in the clinical management of patients with cardiovascular diseases. Core components, standards and outcome measures for referral and delivery: a policy statement from the cardiac rehabilitation section of the European Association for Cardiovascular Prevention & Rehabilitation. Endorsed by the committee for practice guidelines of the European Society of Cardiology. Eur J Prev Cardiol. 2014;21(6):664–681. doi:10.1177/2047487312449597
5. Karner A, Goransson A, Bergdahl B. Patients’ conceptions of coronary heart disease–a phenomenographic analysis. Scand J Caring Sci. 2003;17(1):43–50. doi:10.1046/j.1471-6712.2003.00113.x
6. Perk J, Hambraeus K, Burell G, Carlsson R, Johansson P, Lisspers J. Study of patient information after percutaneous coronary intervention (SPICI): should prevention programmes become more effective? EuroIntervention. 2015;10(11):e1–7. doi:10.4244/EIJV10I11A223
7. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
8. Kramer JM, Hammill B, Anstrom KJ, et al. National evaluation of adherence to beta-blocker therapy for 1 year after acute myocardial infarction in patients with commercial health insurance. Am Heart J. 2006;152(3):454e451–458. doi:10.1016/j.ahj.2006.02.030
9. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125(9):882–887.e881. doi:10.1016/j.amjmed.2011.12.013
10. Libungan B, Stensdotter L, Hjalmarson A, et al. Secondary prevention in coronary artery disease. Achieved goals and possibilities for improvements. Int J Cardiol. 2012;161(1):18–24. doi:10.1016/j.ijcard.2011.04.025
11. Hambraeus K, Lindhagen L, Tyden P, Lindahl B, Lagerqvist B. Target-attainment rates of low-density lipoprotein cholesterol using lipid-lowering drugs one year after acute myocardial infarction in sweden. Am J Cardiol. 2014;113(1):17–22. doi:10.1016/j.amjcard.2013.09.007
12. Ho PM, Magid DJ, Shetterly SM, et al. Medication nonadherence is associated with a broad range of adverse outcomes in patients with coronary artery disease. Am Heart J. 2008;155(4):772–779. doi:10.1016/j.ahj.2007.12.011
13. Ho PM, Spertus JA, Masoudi FA, et al. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch Intern Med. 2006;166(17):1842–1847. doi:10.1001/archinte.166.17.1842
14. Jackevicius CA, Li P, Tu JV. Prevalence, predictors, and outcomes of primary nonadherence after acute myocardial infarction. Circulation. 2008;117(8):1028–1036. doi:10.1161/CIRCULATIONAHA.107.706820
15. Wroe AL. Intentional and unintentional nonadherence: a study of decision making. J Behav Med. 2002;25(4):355–372. doi:10.1023/A:1015866415552
16. Molloy GJ, Messerli-Burgy N, Hutton G, Wikman A, Perkins-Porras L, Steptoe A. Intentional and unintentional non-adherence to medications following an acute coronary syndrome: a longitudinal study. J Psychosom Res. 2014;76(5):430–432. doi:10.1016/j.jpsychores.2014.02.007
17. Pakpour AH, Gellert P, Asefzadeh S, Updegraff JA, Molloy GJ, Sniehotta FF. Intention and planning predicting medication adherence following coronary artery bypass graft surgery. J Psychosom Res. 2014;77(4):287–295. doi:10.1016/j.jpsychores.2014.07.001
18. Gehi AK, Ali S, Na B, Whooley MA. Self-reported medication adherence and cardiovascular events in patients with stable coronary heart disease: the heart and soul study. Arch Intern Med. 2007;167(16):1798–1803. doi:10.1001/archinte.167.16.1798
19. Gehi A, Haas D, Pipkin S, Whooley MA. Depression and medication adherence in outpatients with coronary heart disease: findings from the Heart and Soul Study. Arch Intern Med. 2005;165(21):2508–2513. doi:10.1001/archinte.165.21.2508
20. Sabate M. Adherence to Long-Term Therapies - Evidence for Action. Geneva: World Health Organization; 2003.
21. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
22. Allen LaPointe NM, Ou FS, Calvert SB, et al. Association between patient beliefs and medication adherence following hospitalization for acute coronary syndrome. Am Heart J. 2011;161(5):855–863. doi:10.1016/j.ahj.2011.02.009
23. Clifford S, Barber N, Horne R. Understanding different beliefs held by adherers, unintentional nonadherers, and intentional nonadherers: application of the necessity-concerns framework. J Psychosom Res. 2008;64(1):41–46. doi:10.1016/j.jpsychores.2007.05.004
24. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
25. Unni E, Shiyanbola OO, Farris KB. Change in medication adherence and beliefs in medicines over time in older adults. Glob J Health Sci. 2015;8(5):39–47. doi:10.5539/gjhs.v8n5p39
26. Sirey JA, Greenfield A, Weinberger MI, Bruce ML. Medication beliefs and self-reported adherence among community-dwelling older adults. Clin Ther. 2013;35(2):153–160. doi:10.1016/j.clinthera.2013.01.001
27. Gadkari AS, McHorney CA. Unintentional non-adherence to chronic prescription medications: how unintentional is it really? BMC Health Serv Res. 2012;12:98. doi:10.1186/1472-6963-12-98
28. Berglund E, Lytsy P, Westerling R. Adherence to and beliefs in lipid-lowering medical treatments: a structural equation modeling approach including the necessity-concern framework. Patient Educ Couns. 2013;91(1):105–112. doi:10.1016/j.pec.2012.11.001
29. Unni EJ, Farris KB. Unintentional non-adherence and belief in medicines in older adults. Patient Educ Couns. 2011;83(2):265–268. doi:10.1016/j.pec.2010.05.006
30. Byrne M, Walsh J, Murphy AW. Secondary prevention of coronary heart disease: patient beliefs and health-related behaviour. J Psychosom Res. 2005;58(5):403–415. doi:10.1016/j.jpsychores.2004.11.010
31. Horne R, Parham R, Driscoll R, Robinson A. Patients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflamm Bowel Dis. 2009;15(6):837–844. doi:10.1002/ibd.20846
32. Tibaldi G, Clatworthy J, Torchio E, Argentero P, Munizza C, Horne R. The utility of the necessity–concerns framework in explaining treatment non-adherence in four chronic illness groups in Italy. Chronic Illn. 2009;5(2):129–133. doi:10.1177/1742395309102888
33. Kim SB, Kim KO, Jang BI, et al. Patients’ beliefs and attitudes about their treatment for inflammatory bowel disease in Korea. J Gastroenterol Hepatol. 2016;31(3):575–580. doi:10.1111/jgh.2016.31.issue-3
34. Allen LaPointe NM, Ou FS, Calvert SB, et al. Changes in beliefs about medications during long-term care for ischemic heart disease. Am Heart J. 2010;159(4):561–569. doi:10.1016/j.ahj.2009.12.025
35. Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119(23):3028–3035. doi:10.1161/CIRCULATIONAHA.108.768986
36. Krska J, Morecroft CW, Poole H, Rowe PH. Issues potentially affecting quality of life arising from long-term medicines use: a qualitative study. Int J Clin Pharm. 2013;35(6):1161–1169. doi:10.1007/s11096-013-9841-5
37. Attebring MF, Herlitz J, Ekman I. Intrusion and confusion–the impact of medication and health professionals after acute myocardial infarction. Eur J Cardiovasc Nurs. 2005;4(2):153–159. doi:10.1016/j.ejcnurse.2005.02.001
38. Roebuck A, Furze G, Thompson DR. Health-related quality of life after myocardial infarction: an interview study. J Adv Nurs. 2001;34(6):787–794. doi:10.1046/j.1365-2648.2001.01809.x
39. Lehane E, McCarthy G, Collender V, Deasy A. Medication-taking for coronary artery disease - patients’ perspectives. Eur J Cardiovasc Nurs. 2008;7(2):133–139. doi:10.1016/j.ejcnurse.2007.08.003
40. Rashid MA, Edwards D, Walter FM, Mant J. Medication taking in coronary artery disease: a systematic review and qualitative synthesis. Ann Fam Med. 2014;12(3):224–232. doi:10.1370/afm.1620
41. Johansson Östbring M, Eriksson T, Petersson G, Hellstrom L. Motivational interviewing and medication review in coronary artery disease (MIMeRiC) - study protocol for a randomized, controlled trial investigating effects on clinical outcomes, adherence and quality of life. J Med Internet Res. 2018;7(2):e57.
42. Johansson Östbring M, Eriksson T, Petersson G, Hellström L. Development of an adherence intervention and a protocol for the process evaluation - Motivational interviewing and medication review in coronary heart disease (MIMeRiC). J Med Internet Res. 2018;7(2):e57.
43. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
44. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
45. Svensson S, Kjellgren KI, Ahlner J, Saljo R. Reasons for adherence with antihypertensive medication. Int J Cardiol. 2000;76(2–3):157–163. doi:10.1016/S0167-5273(00)00374-0
46. Moen J, Bohm A, Tillenius T, Antonov K, Nilsson JL, Ring L. “I don’t know how many of these [medicines] are necessary.” - a focus group study among elderly users of multiple medicines. Patient Educ Couns. 2009;74(2):135–141. doi:10.1016/j.pec.2008.08.019
47. van der Laan DM, Elders PJM, Boons C, Nijpels G, Krska J, Hugtenburg JG. The impact of cardiovascular medication use on patients’ daily lives: a cross-sectional study. Int J Clin Pharm. 2018;40(2):412–420. doi:10.1007/s11096-018-0601-4
48. Pettersen TR, Fridlund B, Bendz B, et al. Challenges adhering to a medication regimen following first-time percutaneous coronary intervention: A patient perspective. Int J Nurs Stud. 2018;88:16–24. doi:10.1016/j.ijnurstu.2018.07.013
49. Carter SR, Moles R, White L, Chen TF. Medication information seeking behavior of patients who use multiple medicines: how does it affect adherence?. Patient Educ Couns. 2013;92(1):74–80. doi:10.1016/j.pec.2013.01.019
50. van Geffen EC, Philbert D, van Boheemen C, van Dijk L, Bos MB, Bouvy ML. Patients’ satisfaction with information and experiences with counseling on cardiovascular medication received at the pharmacy. Patient Educ Couns. 2011;83(3):303–309. doi:10.1016/j.pec.2011.04.004
51. Stevenson FA, Cox K, Britten N, Dundar Y. A systematic review of the research on communication between patients and health care professionals about medicines: the consequences for concordance. Health Expect. 2004;7(3):235–245. doi:10.1111/hex.2004.7.issue-3
52. Kohlmann S, Kilbert MS, Ziegler K, Schulz KH. Supportive care needs in patients with cardiovascular disorders. Patient Educ Couns. 2013;91(3):378–384. doi:10.1016/j.pec.2013.01.002
53. Barber N, Parsons J, Clifford S, Darracott R, Horne R. Patients’ problems with new medication for chronic conditions. Qual Saf Health Care. 2004;13(3):172–175. doi:10.1136/qshc.2003.005926
54. Gordon K, Smith F, Dhillon S. Effective chronic disease management: patients’ perspectives on medication-related problems. Patient Educ Couns. 2007;65(3):407–415. doi:10.1016/j.pec.2006.09.012
55. Pound P, Britten N, Morgan M, et al. Resisting medicines: a synthesis of qualitative studies of medicine taking. Soc Sci Med. 2005;61(1):133–155. doi:10.1016/j.socscimed.2004.11.063
56. Foot H, La Caze A, Gujral G, Cottrell N. The necessity-concerns framework predicts adherence to medication in multiple illness conditions: A meta-analysis. Patient Educ Couns. 2016;99(5):706–717. doi:10.1016/j.pec.2015.11.004
57. Granas AG, Bates I. Patients’ understanding and management of their illnesses and prescribed medicines–a descriptive study. Pharm World Sci. 2005;27(4):321–328. doi:10.1007/s11096-005-5999-9
58. Reach G. Role of habit in adherence to medical treatment. Diabet Med. 2005;22(4):415–420. doi:10.1111/dme.2005.22.issue-4
59. Alison Phillips L, Leventhal H, Leventhal EA. Assessing theoretical predictors of long-term medication adherence: patients’ treatment-related beliefs, experiential feedback and habit development. Psychol Health. 2013;28(10):1135–1151. doi:10.1080/08870446.2013.793798
60. Shoemaker SJ. Ramalho de Oliveira D. Understanding the meaning of medications for patients: the medication experience. Pharm World Sci. 2008;30(1):86–91. doi:10.1007/s11096-007-9148-5
61. Felzmann H. Adherence, compliance, and concordance: an ethical perspective. Nurse Prescribing. 2012;10(8):406–411.
62. Bell JS, Airaksinen MS, Lyles A, Chen TF, Aslani P. Concordance is not synonymous with compliance or adherence. Br J Clin Pharmacol. 2007;64(5):710–711. (). doi:10.1111/j.1365-2125.2007.02971_1.x
63. Mullen PD. Compliance becomes concordance. BMJ. 1997;314(7082):691–692. doi:10.1136/bmj.314.7082.691
64. Barry MJ, Edgman-Levitan S. Shared decision making–pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781. doi:10.1056/NEJMp1109283
65. Ekman I, Swedberg K, Taft C, et al. Person-centered care–ready for prime time. Eur J Cardiovasc Nurs. 2011;10(4):248–251. doi:10.1016/j.ejcnurse.2011.06.008
66. Barnett NL, Sanghani P. A coaching approach to improving concordance. Int J Pharm Pract. 2013;21(4):270–272. doi:10.1111/ijpp.2013.21.issue-4
67. Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative content analysis: a focus on trustworthiness. SAGE Open. 2014;4(1):2158244014522633. doi:10.1177/2158244014522633
68. Shoemaker SJ, Ramalho de Oliveira D, Alves M, Ekstrand M. The medication experience: preliminary evidence of its value for patient education and counseling on chronic medications. Patient Educ Couns. 2011;83(3):443–450. doi:10.1016/j.pec.2011.02.007
69. Fors A, Swedberg K, Ulin K, Wolf A, Ekman I. Effects of person-centred care after an event of acute coronary syndrome: two-year follow-up of a randomised controlled trial. Int J Cardiol. 2017;249:42–47. doi:10.1016/j.ijcard.2017.08.069
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.