")
Back to Journals » Clinical Ophthalmology » Volume 15
Trends in Dry Eye Disease Management Worldwide
Authors Hantera MM
Received 22 September 2020
Accepted for publication 5 November 2020
Published 14 January 2021 Volume 2021:15 Pages 165—173
DOI https://doi.org/10.2147/OPTH.S281666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed Mostafa Hantera
Department of Ophthalmology, Umm AL Qura University, Jeddah, Saudi Arabia
Correspondence: Mohamed Mostafa Hantera
Medical Reference Center, King Road After Hiraa Crossing, Jeddah, Saudi Arabia
Tel +966552553322
Email [email protected]
Abstract: Dry eye disease (DED) is a condition frequently encountered in ophthalmology practice worldwide. The purpose of this literature review is to highlight the worldwide trends in DED diagnosis and therapy amongst practitioners and determine if a more uniform approach to manage this multifactorial condition has developed over the past two decades. A manual literature search utilizing PubMed was conducted to obtain papers with survey results relating to ophthalmology and optometry diagnosis and treatment of dry eye from January 2000 to January 2020. This did not include data from clinical trials as we were only interested in community clinical practice trends. The terms “dry eye” and “survey” were searched in combination with one or more of the following words or phrases: prevalence, diagnosis, treatment, therapy, etiology, risk factors, therapy, and quality of life. Papers were selected based on their direct applicability to the subject and were only included if they contained relevant survey data from community practitioners. The available literature suggests common trends worldwide in the diagnosis and treatment of DED. These trends have not modified substantially over the past two decades. Practitioner education on the benefits of measuring tear film homeostasis could increase its use as a diagnostic tool to complement current tools. Of the results found, 75% of the papers were published after 2006 and only one paper after 2017. More recent survey results are required to determine if research into DED pathophysiology is altering the current trend in DED management.
Keywords: dry eye disease, etiology, prevalence, therapy, survey
Introduction
This paper aims to investigate the trends among practitioners diagnosing and treating DED around the world over the last two decades. The literature search found 12 papers with survey results from eye care practitioners determining their diagnostic and/or therapeutic management of DED. The literature comprises research between January 2000 and November 2018 from 12 countries around the world; Australia, Canada, Ghana, Italy, Japan, Korea, New Zealand (NZ), Philippines, Spain, Switzerland, United Kingdom (UK) and the United States (US). The surveys were sent out to community practitioners. We did not investigate data from clinical trials as we felt there may be a bias towards different diagnostic tools that may not accurately represent the trends amongst community practitioners. The understanding of dry eye pathophysiology has advanced in the last decade and we wanted to determine if there has been a modified diagnostic and therapeutic approach among community practitioners to reflect this knowledge.
Overview of Dry Eye
The prevalence of dry eye disease in the population ranges from 5%-34% with large variations between countries.1–10 The large discrepancy in prevalence worldwide is presumed to be the result of a combination of factors; geographical location, study population variations and lack of consistent diagnostic criteria.10
Definition
It is now widely understood that the cause for DED is multifactorial and directly affects the interpalpebral ocular surface and tear film, leading to discomfort and disturbance in vision. The updated report in 2017 from the Tear Film and Ocular Surface Society (TFOS) International Dry Eye Workshop II (DEWS II) defined DED as „a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.„11 The TFOS DEWS II best-practice guideline is designed to help facilitate a consistent approach among practitioners managing DED.12
Diagnosis
Symptoms
There is a poor correlation between DED signs and symptoms.13–16 For this reason a validated patient questionnaire may be more useful to observe any change in symptoms over time rather than as a tool for initial diagnosis.10
Signs
Clinical signs are assessed by evaluating the layers of the tear film, surrounding lids and interpalpebral zone. In 2010 Sullivan et al found the diagnostic tools most commonly used in grading severity were symptomatology, tear break up time (TBUT), fluorescein or lissamine green staining of the cornea and conjunctiva, meibomian secretion scoring and the Schirmer test.17 As early as 2006, Tomlinson et al concluded that the measurement of tear film osmolarity arguably offers the best means of capturing, in a single parameter, the balance of input and output of the lacrimal system.18 In April 2007 the TFOS DEWS report regarded tear hyperosmolarity as the central mechanism causing ocular surface inflammation and the initiation of compensatory events in dry eye, this was corroborated in 2017.11,19
This research supports a ‘tear-film oriented diagnosis’ (TFOD) that looks at the tear secretion volume, tear stability, lipid layer thickness and vital staining to evaluate the cause of DED.20 The Japanese Dry Eye Society (JDES) and Asia Dry Eye Society (ADES) base their diagnostic criteria on this concept.20 The TFOD focuses on which part of the tear film is abnormal so a' tear-film oriented therapy' (TFOT) can be initiated.20
Treatment
In mild DED the eye will often respond favourably to treatment.21 With prolonged damage goblet cell repair mechanisms can fail resulting in irregular mucin production. A so-called “Vicious Circle” will be established and lead to permanent damage if left untreated.21
The available treatments for DED have advanced over the past couple of decades, despite this, traditional methods of warm compresses and artificial tears remain a universal first line therapy.22 Second line treatments include tea tree oil therapy for Demodex, punctal plugs, moisture chamber devices, ointment overnight, intense pulsed light therapy, topical corticosteroids, antibiotics, non-glucocorticoid immunomodulators (cyclosporine), LFA-1 antagonist drugs (lifitegrast), purinergic P2Y2 receptor agonists (diquafosol), oral and topical hyaluronic acid (HA) and oral tetracycline antibiotics.23–25 (Table 1)
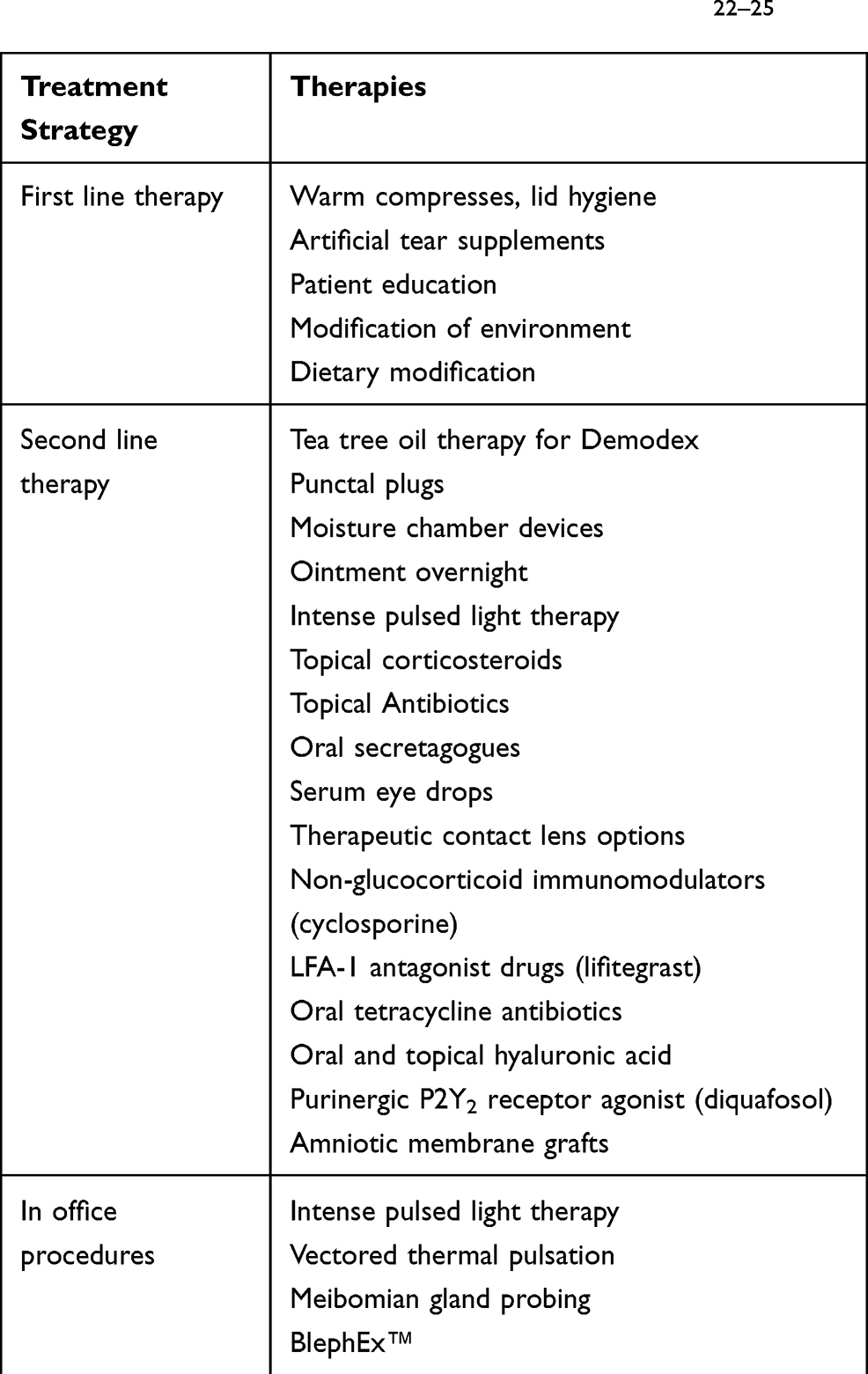 |
Table 1 Summary of Therapies for Dry Eye Disease22–25 |
Results
This paper looks at the current trends in diagnosis and management of DED among community eye care practitioners worldwide. Of the 12 papers we found with relevant survey results, 75% had been published since 2007 when the TFOS DEWS first reported tear hyperosmolarity as a central mechanism in DED. The surveys were sent out to community practitioners. In some cases the respondents reported an interest in dry eye and/or anterior segment. Some survey respondents were affiliated with a University but the majority were in private community practice. For this reason we did not obtain a grade or rank for the respondents. We did not want to include data from clinical trials where there may be a bias towards specific diagnostic tools. The survey results over the past two decades provide a summary of clinical practice preferences among practitioners in the community across 12 countries. (Table 2).
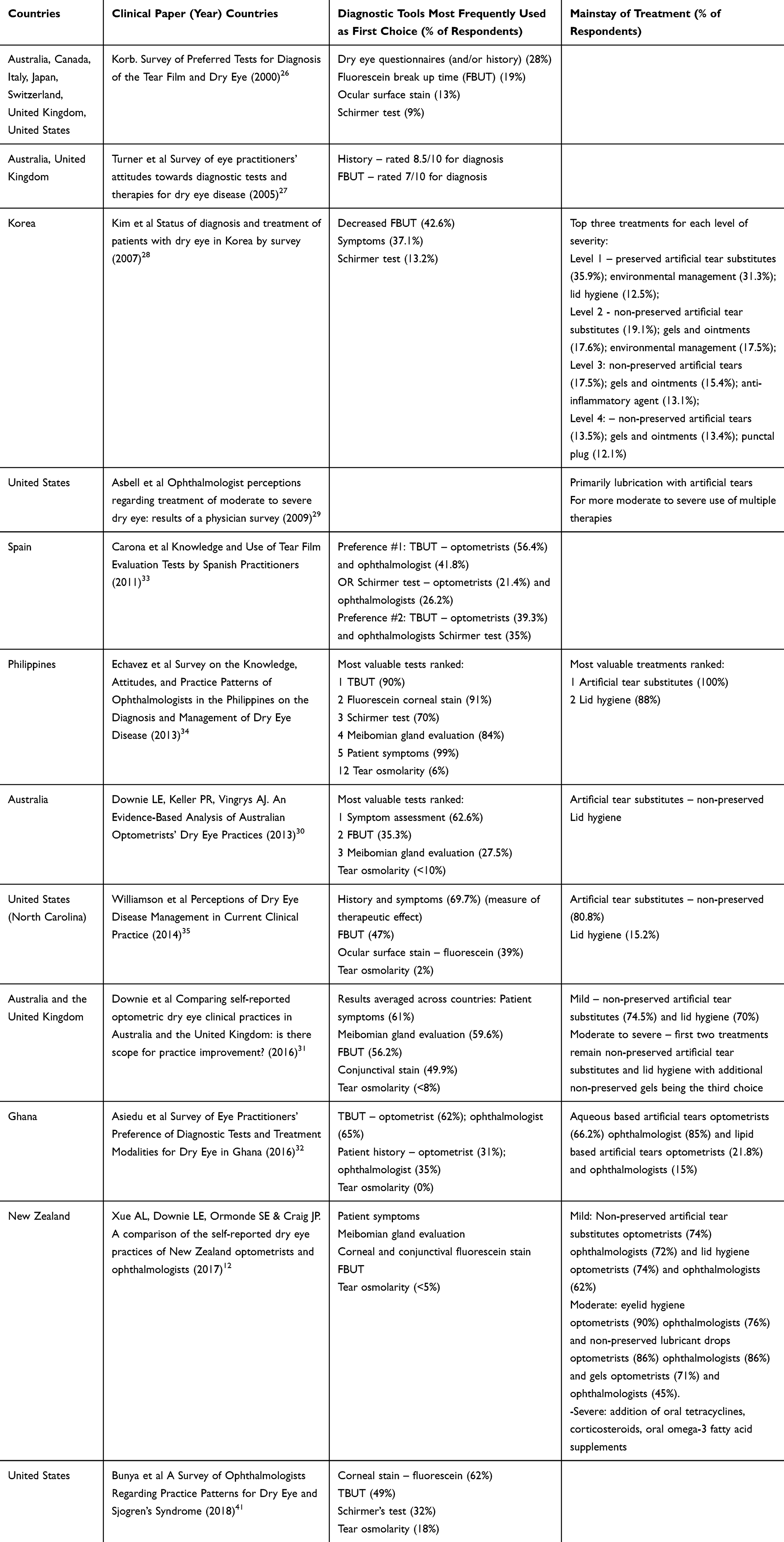 |
Table 2 Summary of Diagnostic and Therapeutic Trends Among Community Eye Care Practitioners Surveyed in the Past Two Decades |
Discussion
At the beginning of this century practitioner survey results indicated the use of multiple tools to evaluate DED.26 Largely there was poor satisfaction with the available diagnostic and therapeutic options for dry eye and research in 2005 recommended a systematic review into dry eye tools and their validity.27 Reinforcing this in 2007 Kim et al found 39.8% practitioners felt the need for a new diagnostic method to evaluate the stability of the tear film and its layers.28 More recently there remains consensus among practitioners that DED is multifactorial in nature and no one diagnostic tool suits all patients.12,29–31
History and Symptoms
Over the past two decades, we found an overwhelming diagnostic trend that placed clear emphasis on patient history and symptoms.12,27,28,30–35 A validated symptom questionnaire can be administered at the beginning of each examination to monitor the progression and efficacy of treatment.36 The Ocular Surface Disease Index (OSDI) is the most widely used questionnaire for DED clinical trials.36 The JDES/ADES consensus also confirms symptom assessment as a fundamental tool for diagnosis.37
A systematic review in 2018 of dry eye-specific questionnaires was conducted and despite identifying 13 validated questionnaires, they all had limitations and there was not one standardized DED-specific questionnaire.37 Consequently future research is required to formulate a DED questionnaire that focuses on normative data and can detect clinically significant changes in response to treatment.37
Survey Results
Patient history is an imperative diagnostic tool and our review confirms the majority of practitioners surveyed understand this and routinely use it for diagnosis.12,27,28,30–35 Perhaps education around the use of a DED questionnaire to document and more easily evaluate disease progression and management is warranted. Further research into a “gold standard” questionnaire that is routinely used around the world will likely provide a consistent approach to understanding symptoms and treatment response.
Investigations
The most appropriate diagnostic tools currently recommended by the TFOS DEWS II are symptoms, NIBUT, osmolarity and ocular surface staining.36 In contrast the JDES/ADES diagnosis of dry eye relies on patient symptoms and a reduction in TBUT without the inclusion of the Schirmer’s value or the presence of epithelial damage.20,38 The new concept of TFOD and TFOT adopted in Asian countries is based on the dynamics of the precorneal tear film. This concept implies the use of FBUT is all that is needed to classify DED and to propose appropriate therapy based on the instability of the tear film.38 This view is very useful and practical for clinicians.
Tear Film Stability
The three-layer physiology of the tear film first described last century by Wolff is still utilized: a mucin layer covering the epithelial cells of the cornea; an aqueous layer to provide lubrication and nutrients to maintain osmolarity; and a lipid layer to prevent evaporation.39
The aqueous layer quantity can be evaluated using the Schirmer test, the strip meniscometry and anterior segment optical coherence tomography.20 Lipid interferometry is available to evaluate the lipid layer.20 There is no simple evaluation method readily available to evaluate mucins on the ocular surface.20 Vital staining using fluorescein and lissamine green can be used to evaluate the epithelial layer.20
In addition, lid wiper epitheliopathy (LWE) is observed as vital staining of the upper and lower lid margin directly in contact with the ocular surface. The primary cause for lid wiper epitheliopathy is thought to be friction between the ocular surface and the lid wiper related to inadequate lubrication.40 The presence of LWE in conjunction with reduced FBUT indicate a reduction in tear film quantity.
Measurement of the tear break up time with a non-invasive technique (NIBUT) is considered preferable to fluorescein break up time (FBUT). The JDES/ADES consensus concludes FBUT is a useful tool for evaluating tear film stability and can easily be performed.20 Fluorescein break up time can be used to analyse the aqueous layer, lipid layer, and epithelial layer, and the fluorescein breakup pattern can also be used to confirm the abnormalities in each component of the tear film.20 FBUT is easy to perform but due to the potential introduction of water to the ocular surface at the time of measurement, lipid layer interferometry, grid xeroscope, and tear stability analysis systems may result in a more accurate tear film assessment.20
Tear Osmolarity
Research indicates tear osmolarity demonstrates the highest correlation to disease severity of all clinical DED tools.36 In six out of seven papers published since 2012 tear osmolarity was included as a diagnostic tool but less than 10% of respondents used it to aid their diagnosis.12,30–32,34,35 In 2018 Bunya et al confirmed 18% of surveyed practitioners reported evaluating tear osmolarity for diagnosis.41 However corroborating with Korb in 2000 they found that practitioners still preferred traditional dry eye tests.41 Technology for assessing tear osmolarity is becoming widely available and we may see practitioners adopting this modality for in-office diagnosis.
It is hoped that survey data in the years to come will determine if practitioners are now routinely including tear osmolarity measurements in their battery of diagnostic tests.
Ocular Staining
Ocular surface staining may be considered a late sign of DED and an indication of disease severity in severe DED. The current TFOS DEWS II recommendation is to use a combination of fluorescein and lissamine green to indicate ocular surface damage in severe DED. More recent papers found Lissamine green staining was rarely used for DED severity detection despite the fact that it is part of the TFOS DEWS II severity grading scale.12,41
Our review highlights patient symptoms, a combination of FBUT, meibomian gland evaluation and ocular surface stain continue to be the predominant clinical tools used to diagnose dry eye.12,28,30–35,41,42 This aligns with TFOS DEWS II and JDES/ADES guidelines. However assessment of tear performance in its natural state was not frequently utilized with practitioner responses from a survey in 2017 in New Zealand reporting only 2% used LWE, corneal topography mire quality and non-invasive TBUT.12
Treatment
Effective treatment of dry eye is reliant on an accurate diagnosis. Targeting each abnormality in the TFOD approach will enhance treatment. The 2017 TFOS DEWS II provides guidelines for a stepped management and treatment protocol for dry eye.43
Step one involves patient education, modification of environment, dietary modification, ocular lubricants (if MGD then lipid containing supplements) and lid hygiene.43 If these first line treatments are inadequate then in step two non-preserved lubricants, tea tree oil for Demodex, punctal occlusion, moisture chamber googles, in-office physical heating and expression of the meibomian glands, IPL, topical antibiotic and/or corticosteroids, secretagogues, immunomodulatory drugs, oral tetracyclines and topical LFA-1 antagonist drugs should be considered.43 Step three includes oral secretagogues, serum eye drops and therapeutic contact lens options. In severe unresponsive DED then step 4 of the guidelines indicates topical corticosteroids for longer duration, amniotic membrane grafts, surgical punctal occlusion or other surgical approaches.43
Drug Therapy
Topical corticosteroids have been used for years to treat the inflammation associated with dry eye.44 Topical cyclosporine A is a common second line therapy for those that have had little success with the first line more conservative measures.22 In July 2016, lifitegrast 5% became the second FDA approved topical ocular anti-inflammatory drug for the treatment of DED.
Although there has been a link between low dietary intake of omega-3 essential fatty acids and DED, there are only a limited number of random controlled trials confirming supplementation improves tear break up times and Schirmer scores.44
Hyaluronic acid has been proven to promote corneal epithelial wound healing.45 A pilot study by Kim et al in 2019 indicated both oral and topical HA were effective at reducing corneal fluorescein staining especially when used in combination.24
Aqueous secretagogue eye drops, topical 3% diquafosol have become widely available for dry eye patients.25 They have been found to improve tear production, tear break up time, and reduce corneal fluorescein and rose bengal staining and subjective symptoms.25
Procedures
Alongside drug therapies in-office procedures have evolved targeting meibomian gland expression and restoration of the natural flow of meibum (intense pulse light, vectored thermal pulsation, meibomian gland probing, BlephEx™).22
Survey Results
Given the extensive research and development into new therapeutic options for the treatment of DED we anticipated a modified treatment approach among practitioners. Where the more traditional treatments work to address the symptoms and restore the ocular surface, the newer therapeutic modalities endeavour to reverse the primary cause of the DED (such as inflammation).
In this literature review the general trend among practitioners did follow a stepwise treatment approach. Mild dry eye was treated with non-preserved artificial tear substitutes combined with lid hygiene.12,28,30,31,34,35 Therapeutics for moderate to severe dry eye meant the addition of non-preserved gels or ointments and topical anti-inflammatories.12,28,30,31, In addition, it was found that the proportion of anti-inflammatory drugs used increased with the treatment of moderate to dry eye.28 There seems to be consensus over the last twenty years that therapeutic management is based on disease severity.12,28,31,34 Successful management can be determined by improvement of patient-reported symptoms and a reduction in ocular signs.
Conclusion
Our literature search identified 12 published papers surveying eye care practitioners in clinical practice about their diagnostic and/or therapeutic approach to dry eye. This limited number highlights the need for additional worldwide research to determine practitioner trends. Furthermore all but two of the surveys were extracted from research conducted prior to 2017 indicating a need for current worldwide practitioner survey responses to accurately determine trends in the coming years.
The definition and classification of DED has advanced considerably over the past two decades due to an enhanced understanding of the pathophysiology of the disease. The TFOS DEWS II and JDES/ADES provide definitions and guidelines for practitioners to follow. Both definitions share the similar concept that disruption of the tears and ocular surface epithelia results in the development of DED. The TFOS DEWS II definition included multiple pathogeneses including ocular surface inflammation, tear film instability, hyperosmolarity and neurosensory abnormalities. It focuses on the pathophysiology of DED. In contrast the JDES/ADES report highlights the importance of observations made by the practitioner. Despite differences, the consensus remains that careful consideration of symptoms and tear film status is required to accurately diagnose DED.
Internationally there seems to be a common trend for practitioners to routinely use the more traditional methods of diagnosis. Subjectively patient symptoms remain a critical tool for diagnosis and assessment of treatment effectivity. Research and education into the use of a “gold standard” patient questionnaire will likely provide a consistent approach to understanding symptoms and response to treatment.
Objectively corneal staining with fluorescein and fluorescein tear break up time are the mainstay tools used among the majority of practitioners surveyed worldwide. Less consistency is seen with the use of non-invasive procedures to assess tear quality and osmolarity despite advice from the TFOS DEWS II and JDES/ADES reports. Latest research is focusing on tear film biomarkers for dry eye disease, with tear osmolarity being one such biomarker. It is thought that this may give a more quantitative measure of disease severity and therapeutic effectivity. Enhanced education about these newer diagnostic tools identifying an imbalance in the tear film may alter DED management over time.
Further tools measuring tear film quality such as LWE and non-invasive TBUT may become common practice as education continues to signify the importance of the assessment of tear film performance in its natural state.
Therapeutic advancements in the treatment of DED have not necessarily correlated with a modified treatment regime. Artificial tear supplements and lid hygiene continue to be the first line treatment strategy, followed by anti-inflammatory therapy for more moderate to severe DED. In office treatments for meibomian gland expression and restoration were not commonly reported in the management strategy among surveyed respondents.
Practitioner surveys are a sound way to gauge trends in the professional population. Our literature review confirms that the majority of community practitioners surveyed understand the multifactorial nature of DED and because of this use multiple tools to form an accurate diagnosis. The more recent literature also indicates an overall understanding that inflammation plays a critical role in DED and the therapy for moderate to severe dry eye reflects this. But the reliable assessment of DED severity remains problematic with often limited correlation between disease severity and clinical signs.
Future practitioner surveys will determine if DED management is changing with time. Education on the importance of widespread use of the TFOS DEWS II and JDES/ADES guidelines and algorithms in clinical practice along with advancements in clinical research into tear film biomarkers will further enhance the management strategy for dry eye disease.
Acknowledgments
I wish to acknowledge the assistance provided by Louise Wood, of EyeWrite Communications, in writing and editing this paper.
Disclosure
The author reports no conflicts of interest for this work.
References
1. Bakkar MM, Shihadeh WA, Haddad MF, Khader YS. Epidemiology of symptoms of dry eye disease (DED) in Jordan: a cross-sectional non-clinical population-based study. Cont Lens Anterior Eye. 2016;39(3):197–202. doi:10.1016/j.clae.2016.01.003
2. Hashemi H, Khabazkhoob M, Kheirkhah A, et al. Prevalence of dry eye syndrome in an adult population. Clin Exp Ophthalmol. 2014;42(3):242–248. doi:10.1111/ceo.12183
3. Lee AJ, et al. Prevalence and risk factors associated with dry eye symptoms: a population based study in Indonesia. Br J Ophthalmol. 2002;86(12):1347–1351. doi:10.1136/bjo.86.12.1347
4. Moss SE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118(9):1264–1268. doi:10.1001/archopht.118.9.1264
5. Onwubiko SN, Eze BI, Udeh NN, Arinze OC, Onwasigwe EN, Umeh RE. Dry eye disease: prevalence, distribution and determinants in a hospital-based population. Cont Lens Anterior Eye. 2014;37(3):157–161. doi:10.1016/j.clae.2013.09.009
6. Sendecka M, Baryluk A, Polz-Dacewicz M. Prevalence and risk factors of dry eye syndrome. Przegl Epidemiol. 2004;58:227–233.
7. Uchino M, Nishiwaki Y, Michikawa T, et al. Prevalence and risk factors of dry eye disease in Japan: koumi study. Ophthalmology. 2011;118(12):2361–2367. doi:10.1016/j.ophtha.2011.05.029
8. Vehof J, Kozareva D, Hysi PG, Hammond CJ. Prevalence and risk factors of dry eye disease in a British female cohort. Br J Ophthalmol. 2014;98(12):1712–1717. doi:10.1136/bjophthalmol-2014-305201
9. Asbell P, Messmer E, Chan C, et al. Defining the needs and preferences of patients with dry eye disease. BMJ Open Ophthalmol. 2019;4(1):e000315. doi:10.1136/bmjophth-2019-000315
10. Shanti Y, Shehada R, Bakkar MM, et al. Prevalence and associated risk factors of dry eye disease in 16 northern West bank towns in Palestine: a cross-sectional study. BMC Ophthalmol. 2020;20(1):26. doi:10.1186/s12886-019-1290-z
11. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
12. Xue AL, Downie LE, Ormonde SE, Craig JP. A comparison of the self-reported dry eye practices of New Zealand optometrists and ophthalmologists. Ophthalmic Physiol Opt. 2017;37(2):191–201. doi:10.1111/opo.12349
13. Nichols KK, Nichols JJ, Mph GL, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23(8):
14. Aggarwal S, Galor A. What’s new in dry eye disease diagnosis? Current advances and challenges. Faculty Rev. 2018;7:1952.
15. Holland EJ, Darvish M, Nichols KK, Jones L, Karpecki PM. Efficacy of topical ophthalmic drugs in the treatment of dry eye disease: A systematic literature review. Ocul Surf. 2019;17(3):412–423. doi:10.1016/j.jtos.2019.02.012
16. Messmer EM. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch Arztebl Int. 2015;112(5):
17. Sullivan BD, Whitmer D, Nichols KK, et al. An Objective Approach to Dry Eye Disease Severity. Invest Opthalmology Visual Sci. 2010;51(12):6125–6130. doi:10.1167/iovs.10-5390
18. Tomlinson A, Khanal S, Ramaesh K, Diaper C, McFadyen A. Tear film osmolarity: determination of a referent for dry eye diagnosis. Invest Ophthalmol Vis Sci. 2006;47(10):4309–4315. doi:10.1167/iovs.05-1504
19. Avialble from: https://www.tearfilm.org/dewsreport/pdfs/TOS-0502-DEWS-noAds.pdf. Accessed June 8, 2020.
20. Kojima T, Dogru M, Kawashima M, Nakamura S, Tsubota K. Advances in the diagnosis and treatment of dry eye. Prog Retin Eye Res. 2020;78:100842. doi:10.1016/j.preteyeres.2020.100842
21. Baudouin C, Aragona P, Van Setten G, Rolando M, Irkeç M. Diagnosing the severity of dry eye: a clear and practical algorithm. Br J Ophthalmol. 2014;98(9):1168–1176. doi:10.1136/bjophthalmol-2013-304619
22. O’Neil E, Henderson M, Massaro-Giordano M, Bunya VY. Advances in dry eye disease treatment. Curr Opin Ophthalmol. 2019;30(3):166–178. doi:10.1097/ICU.0000000000000569
23. Şimşek C, Doğru M, Kojima T, Current Management TK. Treatment of dry eye disease. Turk J Ophthalmol. 2018;48(6):
24. Kim Y, Moon CH, Kim B-Y, Jang SY. Oral hyaluronic acid supplementation for the treatment of dry eye disease: a pilot study. J Ophthalmol. 2019;2019:5491626. doi:10.1155/2019/5491626
25. Nam K, Kim H, Yoo A. A: efficacy and safety of topical 3% diquafosol ophthalmic solution for the treatment of multifactorial dry eye disease: meta-analysis of randomized clinical trials. Ophthalmic Res. 2019;61(4):188–198. doi:10.1159/000492896
26. Korb DR. Survey of preferred tests for diagnosis of the tear film and dry eye. Cornea. 2000;19(4):483–486. doi:10.1097/00003226-200007000-00016
27. Turner AW, Layton CJ, Bron AJ. Survey of eye practitioners‘ attitudes towards diagnostic tests and therapies for dry eye disease. Clinical and Experimental Ophthalmology. 2005;33(4):351–355. doi:10.1111/j.1442-9071.2005.01026.x
28. Kim WJ, Kim HS, Kim MS. Current trends in the recognition and treatment of dry eye: a survey of ophthalmologists. J Korean Ophthalmological Soc. 2007;48(12):1614–1622. doi:10.3341/jkos.2007.48.12.1614
29. Asbell PA, Spiegel S. Ophthalmologist perceptions regarding treatment of moderate to severe dry eye: results of a physician survey. Trans Am Ophthalmol Soc. 2009;107:
30. Downie LE, Keller PR, Vingrys AJ. An evidence-based analysis of australian optometrists’ dry eye practices. Optom Vis Sci. 2013;90(12):1385–1395. doi:10.1097/OPX.0000000000000087
31. Downie LE, Rumney N, Gad A, Keller PR, Purslow C, Vingrys AJ. Comparing self-reported optometric dry eye clinical practices in Australia and the United Kingdom: is there scope for practice improvement? Ophthalmic Physiol Opt. 2016;36(2):140–151. doi:10.1111/opo.12280
32. Asiedu K, Kyei S, Ayobi B, Agyemang FO, Ablordeppey RK. Survey of eye practitioners’ preference of diagnostic tests and treatment modalities for dry eye in ghana. Cont Lens Anterior Eye. 2016;39(6):411–415. doi:10.1016/j.clae.2016.08.001
33. Cardona G, Serés C, Quevedo L, Augé AM. Knowledge and use of tear film evaluation tests by spanish practitioners. Optom Vis Sci. 2011;88(9):1106–1111. doi:10.1097/OPX.0b013e3182231b1a
34. Echavez M. Lim bon siong r. survey on the knowledge, attitudes, and practice patterns of ophthalmologists in the philippines on the diagnosis and management of dry eye disease. Philip J of Ophthal. 2013;44:2.
35. Williamson JF, Huynh K, Weaver MA, Davis RM. Perceptions of dry eye disease management in current clinical practice. Eye Contact Lens. 2014;40(2):111–115. doi:10.1097/ICL.0000000000000020
36. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;544–579.
37. Shiraishi A, Sakane Y. Assessment of dry eye symptoms: current trends and issues of dry eye questionnaires in Japan. Invest Opthalmology Visual Sci. 2018;59(14):DES23–DES28. doi:10.1167/iovs.18-24570
38. Shimazaki J. Definition and diagnostic criteria of dry eye disease: historical overview and future directions. Invest Opthalmology Visual Sci. 2018;59(14):DES7–DES12. doi:10.1167/iovs.17-23475
39. Willcox MDP, Argüeso P, Georgiev GA, et al. TFOS DEWS II tear film report. Ocul Surf. 2017;15(3):366–403. doi:10.1016/j.jtos.2017.03.006
40. Efron N, Brennan N, Morgan P, Wilson T. Lid wiper epitheliopathy. Progress Retinal Eye Res. 2016;53:140–174. doi:10.1016/j.preteyeres.2016.04.004
41. Bunya VY, Fernandez KB, Ying G-S, et al. Survey of Ophthalmologists Regarding Practice Patterns for Dry Eye and Sjogren Syndrome. Eye Contact Lens. 2018;44(2):196–201. doi:10.1097/ICL.0000000000000448
42. Nichols KK, Nichols JJ, Zadnik K. Frequency of dry eye diagnostic test procedures used in various modes of ophthalmic practice. Cornea. 2000;19(4):
43. Jones L, Downie L, Korb D, et al. TFOS DEWS II management and therapy report. Ocular Surface. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
44. Buckley R. Assessment and management of dry eye disease. Eye. 2018;32(2):200–203. doi:10.1038/eye.2017.289
45. Ho W, Chiang T, Chang S, Chen Y, Hu F, Wang I. Enhanced corneal wound healing with hyaluronic acid and high-potassium artificial tears. Clinical and Experimental Optometry. 2013;96(6):536–541. doi:10.1111/cxo.12073
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.