")
Back to Journals » International Medical Case Reports Journal » Volume 8
Treatment with sodium hyaluronate eye drops in a patient who had early-onset bleb leakage after trabeculectomy with mitomycin C
Authors Sagara H, Sekiryu T , Noji H, Ogasawara M, Imaizumi K, Yago K
Received 28 August 2015
Accepted for publication 15 October 2015
Published 27 November 2015 Volume 2015:8 Pages 301—304
DOI https://doi.org/10.2147/IMCRJ.S95334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hideto Sagara,1,2 Tetsuju Sekiryu,2 Hiroki Noji,2 Masashi Ogasawara,2 Kimihiro Imaizumi,2 Keiko Yago3
1The Marui Eye Clinic, Minamisoma, 2Department of Ophthalmology, School of Medicine, Fukushima Medical University. 3Northern Fukushima Medical Center, Fukushima, Japan
Abstract: We present the case of a 47-year-old man who had bilateral proliferative diabetic retinopathy and neovascular glaucoma. Schirmer I test revealed tear secretions of 5 mm and 3 mm in the right and left eyes, respectively. Tear breakup times in the right and left eyes were 7 and 8 seconds, respectively. The ocular surface staining in both eyes was scored as Grade 1 as per the Oxford scheme. Retinal photocoagulation was performed for correction of the proliferative diabetic retinopathy and rubeosis iridis, which resolved with treatment. However, the intraocular pressure in the left eye could not be adequately controlled. Therefore, trabeculectomy with mitomycin C using limbal-based conjunctival flap was performed. Three hours after the surgery, the patient developed a large and diffuse filtering bleb, but no leakage occurred from the conjunctival scar. However, on the first postoperative day, leakage was noted and the conjunctiva was at the leakage point. The leakage resolved transiently, but recurred the next day. Severe keratoconjunctival epithelial failure was detected, and the patient was administrated 0.1% sodium hyaluronate eye drops six times daily. The epithelial failure improved, and many microcysts were detected on the bleb surface where the epithelial failure improved. The leakage resolved 2 days after initiation of the sodium hyaluronate eye drops. The microcysts disappeared and the bleb surface became smooth 1 month later.
Keywords: trabeculectomy, bleb, bleb leak, microcyst, sodium hyaluronate
Introduction
The study adhered to the tenets of the Declaration of Helsinki principles. Treatment was administered after the purpose of the study was explained to the patient and they provided informed consent. Doctors explained that sodium hyaluronate eye drops effectively treat dry eye and rarely cause severe side effects. Moreover, the patient was told that the sodium hyaluronate eye drops prevent complications of trabeculectomy with mitomycin C (MMC).
Patients with a history of trabeculectomy may occasionally present with early-onset bleb leakages, which is difficult to treat in some cases.1,2 Treatment with sodium hyaluronate eye drops has been reported to be efficacious for dry eye3 and prevents late-onset bleb leakage after trabeculectomy with MMC.4 Epithelial failure of the bleb wall caused by tear dysfunction could contribute to late-onset bleb leakage after trabeculectomy with MMC,4,5 and dry eye was suspected as one cause of late-onset bleb leakage.5 Reports indicate that late-onset bleb leaks in patients with ocular surface diseases can be treated effectively by using a combination of sodium hyaluronate and autologous serum eye drops.6 Considering these findings, we speculated that tear dysfunction and/or epithelial failure of the bleb surface impedes wound healing and contributes to early-onset bleb leakage. In this report, we present a case of early-onset bleb leakage, tear dysfunction, and epithelial failure of the bleb surface after trabeculectomy with MMC that was treated using sodium hyaluronate eye drops.
Case report
The patient was a 47-year-old man who had bilateral proliferative diabetic retinopathy, neovascular glaucoma, and tear dysfunction. Schirmer I test revealed tear secretion levels of 5 and 3 mm in the right and left eyes, respectively. Tear breakup times were 7 and 8 seconds for the right and left eye, respectively. The ocular surface staining with fluorescein dye7 was scored as Grade 1 in both eyes. Accordingly, retinal photocoagulation was performed to treat the proliferative diabetic retinopathy and rubeosis iridis; the latter resolved completely with treatment.
However, despite the administration of the maximum tolerated doses of topical antiglaucoma medications, intraocular pressure (IOP) continued to remain high, with the level in the left eye exceeding more than 25 mmHg. Therefore, trabeculectomy with MMC using limbal-based conjunctival flap was performed; during surgery, 0.04% MMC was applied for 5 minutes. Tenon’s capsule was not excised, and the conjunctival flap and the underlying Tenon’s capsule were closed tightly with shoelace 10–0 nylon sutures. Three hours after the operation, a large and diffuse filtering bleb was detected; however, no leakage of the conjunctival scar was noticed. However, leakage was detected on the first postoperative day, and the IOP was 7 mmHg with noncontact tonometer. Resuturing the conjunctiva at the point of leakage stopped the leakage transiently, but it resumed the next day even though the subject was treated with a compression bandage after resuturing. On examination, severe keratoconjunctival epithelial failure (Figure 1) was detected, and the patient was treated with 0.1% sodium hyaluronate eye drops (Hyalein; Santen Pharmaceutical Co Ltd, Osaka, Japan) administered six times daily with the patient lying supine to allow the drops to spread onto the upper blebs. With this treatment, improvement in the epithelial failure was seen at some sites, which showed the presence of many microcysts on the bleb surface; the leakage resolved completely 2 days after starting the sodium hyaluronate eye drops without using compression bandage (Figure 2). One month after starting this treatment, the microcysts disappeared; the bleb surface was smooth; and the IOP was 10 mmHg (Figure 3). However, subsequently, 18 months after starting the application of sodium hyaluronate eye drops, the bleb was found to be flat and IOP was poorly controlled despite administration of maximum tolerated doses of topical antiglaucoma medications and exceeded 22 mmHg in the left eye. Therefore, trabeculotomy was performed, and thereafter, IOP has remained in control, at less than 15 mmHg, over a period of 5 years.
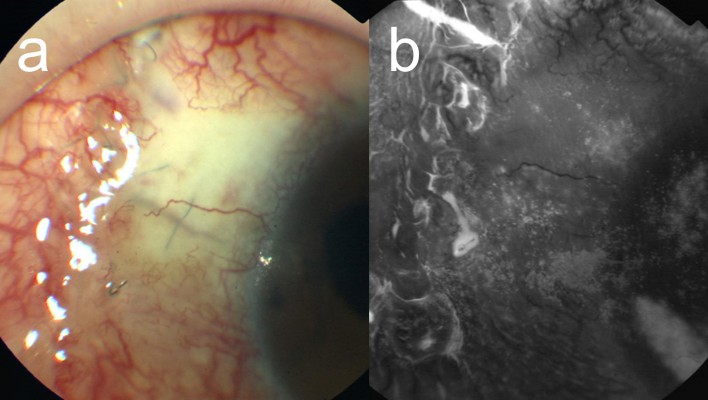
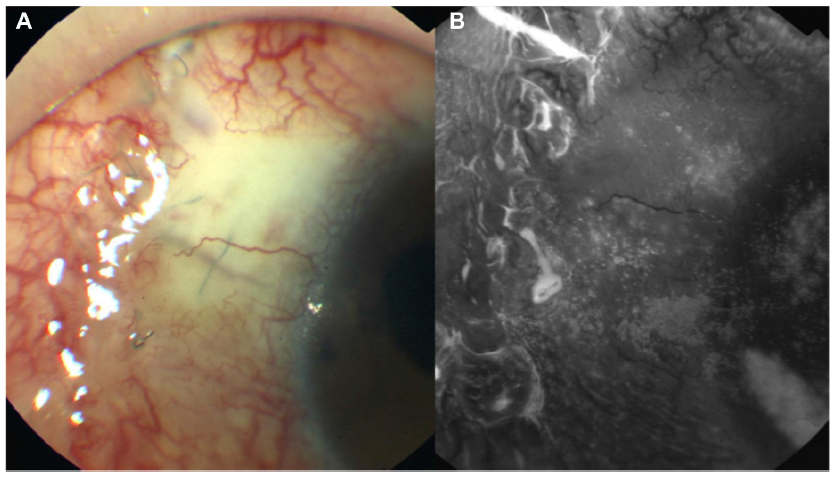
 | Figure 1 Apparent point leakage with severe ocular surface failure. |
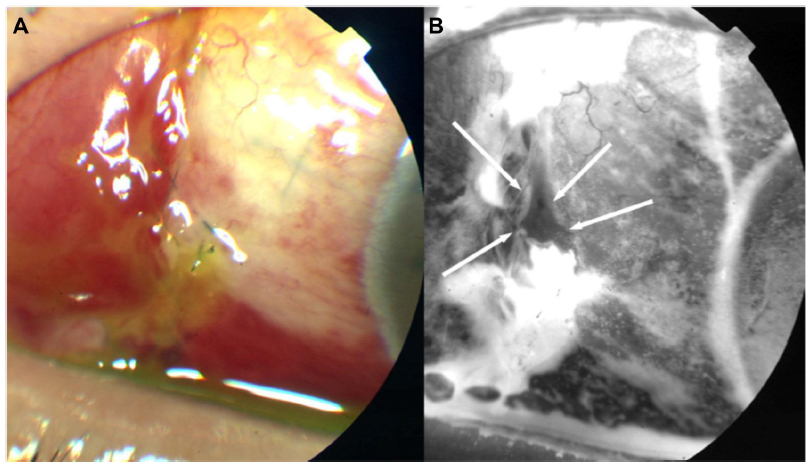
 | Figure 2 (A and B) Photographs obtained 2 days after the initiation of sodium hyaluronate eye drops. |
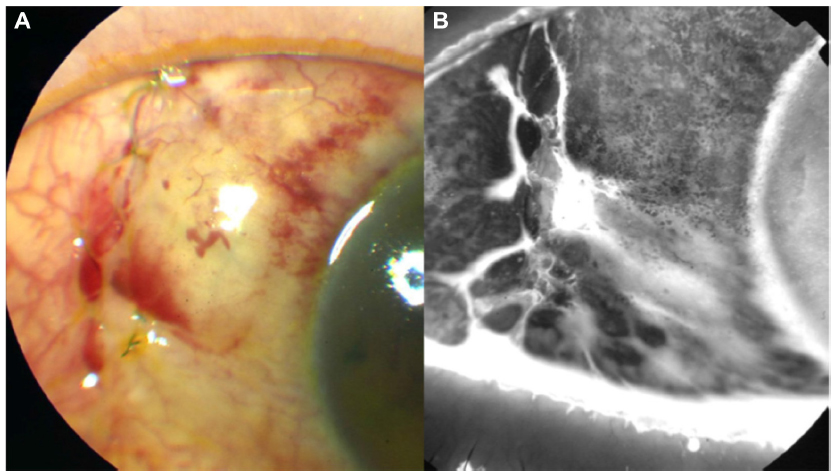
 | Figure 3 (A and B) Photograph taken 1 month after initiation of treatment with sodium hyaluronate eye drops. |
Discussion
Severe, early-onset bleb leakage causes various serious complications, including choroidal effusions, suprachoroidal hemorrhage, hypotonous maculopathy, and endophthalmitis. In addition, the resulting flat bleb may promote the formation of adhesions between the roof and the base of the bleb, thereby hampering bleb evolution and increasing the risk of bleb scarring and failure. Early bleb leakage (caused by wound leak or conjunctival button holes) may be related to deficient wound closure, patent stitch tracts, or surgical trauma to the conjunctiva.1,8 In addition, the use of augmenting antimetabolites may suppress wound healing and further increase the risk of bleb leak.9 Severe, early-onset bleb leakage must be promptly treated to prevent the occurrence of these serious complications. However, in some cases, it is difficult to detect the exact reason for the leak, and it can continue to persist for more than 100 days.2 On the other hand, ocular surface complications following trabeculectomy with MMC are fairly common.10
In this case, we observed severe epithelial failure of the bleb wall, and the leakage recurred soon after resuturing. The severe epithelial failure on the bleb wall hindered the reepithelialization of the conjunctival scar, thereby contributing to the development of early leakage after trabeculectomy with MMC. Many microcysts were detected on the bleb surface at sites where the epithelial failure showed improvement. Similar microcysts are frequently observed on the surface of the cornea with bullous keratopathy and in the presence of stromal edema of the cornea.11 These microcysts frequently appear on functional, thin bleb surfaces.4 This case reiterates the findings of Sagara et al,4 who reported that microcysts occur on the avascular bleb surface when the defective epithelial area of the bleb wall showed improvement following the use of sodium hyaluronate eye drops. They speculated that stromal edema of the conjunctiva, which is caused by the aqueous humor within the bleb, induced the formation of microcysts in the presence of a thin conjunctival epithelium.4 Therefore, in this case, the microcysts may have appeared as a result of the reepithelialization of the bleb wall because the leakage from the defective epithelial area was suppressed by the presence of the thin conjunctival epithelium.
Sodium hyaluronate can suppress the breakup of the preocular tear film.12 The tear fluid contains various cytokines, such as epidermal growth factor and vitamin A, which help maintain the normal histology of the conjunctiva.13,14 Therefore, in our case, the application of sodium hyaluronate eye drops may have suppressed the breakup of the tear film and promoted the reepithelialization of the bleb surface.
However, the incidence of flattening or encapsulation of the bleb tends to be greater when sodium eye drops are administered immediately after trabeculectomy and continued for a long time.4 Sodium hyaluronate eye drops may advance fibrosis of the bleb wall and decrease bleb function when administered immediately after trabeculectomy. In the present case, the bleb was eventually rendered flat, and reoperation had to be performed to suppress the IOP. To avoid this, it is necessary to stop administration of the drops before the bleb becomes flat.
Conclusion
Close monitoring of the bleb surface after trabeculectomy is important, particularly in the presence of tear dysfunction and/or ocular surface disorder. Our experience in this case suggests that the application of sodium hyaluronate eye drops may effectively resolve posttrabeculectomy early-onset bleb leaks that are caused by epithelial failure of the bleb wall.
Disclosure
The authors report no conflicts of interest in this work.
References
Alwitry A, Rotchford A, Patel V, Abedin A, Moodie J, King AJ. Early bleb leak after trabeculectomy and prognosis for bleb failure. Eye. 2009;23(4):858–863. | |
Henderson HW, Ezra E, Murdoch IE. Early postoperative trabeculectomy leakage: incidence, time course, severity, and impact on surgical outcome. Br J Ophthalmol. 2004;88(5):626–629. | |
Mengher LS, Pandher KS, Bron AJ, Davey CC. Effect of sodium hyaluronate eye drops (0.1%) on break-up time (NIBUT) in patients with dry eyes. Br J Ophthalmol. 1986;70(6):442–447. | |
Sagara H, Iida T, Suzuki K, Fujiwara T, Koizumi H, Yago K. Sodium hyaluronate eye drops prevent late-onset bleb leakage after trabeculectomy with mitomycin C. Eye. 2008;22(4):507–514. | |
Sagara H, Yago K. Dry eye and bleb leaks after trabeculectomy with mitomycin C. Folia Ophthalmol Jpn. 2004;55:18–21. Japanese. | |
Sagara H, Iida T, Saito K, Noji H, Ogasawara M, Oyamada H. Conservative treatment for late-onset bleb leaks after trabeculectomy with mitomycin C in patients with ocular surface disease. Clin Ophthalmol. 2012;6:1273–1279. | |
Methodologies to diagnose and monitor dry eye disease. Report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):108–152. | |
Rand Allingham R, editor. Shields’ Textbook of Glaucoma. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. | |
Cohen JS, Greff LJ, Novack GD, Wind BE. A placebo-controlled, double-masked evaluation of mitomycin C in combined glaucoma and cataract procedures. Ophthalmology. 1996;103(11):1934–1942. | |
Ono T, Yuki K, Ozeki N, Shiba D, Tsubota K. Ocular surface complications after trabeculectomy: incidence, risk factors, time course and prognosis. Ophthalmologiaca. 2013;230(2):93–99. | |
Tuft S. The cornea. In: Spalton DJ, Hitchings RA, Hunter PA, Tan JCH, Harry J, editors. Atlas of Clinical Ophthalmology. 3rd ed. Philadelphia, PA: Elsevier-Mosby; 2005:147–186. | |
Hamano T, Horimoto K, Lee M, Komemushi S. Sodium hyaluronate eye drops enhance tear film stability. Jpn J Ophthalmol. 1996;40(1):62–65. | |
Watanabe H, Ohashi Y, Kinoshita S, Manabe R, Ohshiden K. Distribution of epidermal growth factor in rat ocular and periocular tissues. Graefes Arch Clin Exp Ophthalmol. 1993;231(4):228–232. | |
Huang AJ, Tseng SC, Kenyon KR. Change of paracellular permeability of ocular surface epithelium by vitamin A deficiency. Invest Ophthalmol Vis Sci. 1991;32(3):633–639. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.