")
Back to Journals » Cancer Management and Research » Volume 14
Treatment Outcomes and Its Associated Factors Among Adult Patients with Selected Solid Malignancies at Kenyatta National Hospital: A Hospital-Based Prospective Cohort Study
Authors Degu A , Terefe EM , Some ES, Tegegne GT
Received 7 February 2022
Accepted for publication 7 April 2022
Published 22 April 2022 Volume 2022:14 Pages 1525—1540
DOI https://doi.org/10.2147/CMAR.S361485
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Amsalu Degu,1 Ermias Mergia Terefe,1 Eliab Seroney Some,1 Gobezie T Tegegne2
1Department of Pharmaceutics and Pharmacy Practice, School of Pharmacy and Health Sciences, United States International University-Africa, Nairobi, Kenya; 2Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Amsalu Degu, United States International University-Africa, School of Pharmacy and Health Sciences, Nairobi, Kenya, Tel +254745063687, Email [email protected]
Introduction: The treatment outcome of cancer is poor in the African setting due to inadequate treatment and diagnostic facilities. However, there is a paucity of data on solid cancers in Kenya. Hence, this study aimed to investigate the treatment outcomes and its determinant factors among adult patients diagnosed with selected solid malignancies at Kenyatta National Hospital (KNH).
Materials and Methods: A prospective cohort study was employed at the Oncology Department of KNH from 1st July 2020 to 31st December 2021. All new patients with a confirmed diagnosis of lymphoma, prostate cancer and breast cancer were studied. A consecutive sample of 99 breast cancer, 50 lymphomas, and 82 prostate cancer patients was included in the study. Semi-structured questionnaires consisting of socio-demographics, clinical characteristics, and quality of life were employed to collect the data. All enrolled patients were followed prospectively for 12 months. Treatment outcomes were reported as mortality, cancer-specific survival and health-related quality of life. The data were entered and analyzed using the SPSS 20.0 statistical software. Survival outcomes and its predictors were evaluated using the Kaplan–Meier analysis and Cox regression analyses, respectively.
Results: The study showed that the mortality rate among breast and prostate cancer patients was 3% and 4.9%, respectively. In contrast, the mortality rate was 10% among lymphoma patients. Most of the patients had partial remission and a good overall global health-related quality of life. Older age above 60 years, co-morbidity, distant metastasis and advanced stages of disease were significant predictors of mortality.
Conclusion: Although the mortality was not high at 12 months, only a few patients had complete remission. For many patients, the disease was progressing, despite 12-month mortality was not high. Therefore, longer follow-up will be required to report cancer mortality accurately. In addition, most of the patients had a good overall global health-related quality of life.
Keywords: treatment outcomes, health-related quality of life, solid malignancies, Kenyatta National Hospital
Introduction
Cancer is characterized by the uncontrolled multiplication of cells inherited or acquired from environmental exposure and other factors.1 Cancers can be classified into two categories based on tissue origin (histological type) and the primary site of tumor development. Histologically, cancers can be categorized as carcinoma, sarcoma, leukaemia, myeloma, lymphomas, and mixed types.2 Colorectal, breast cancer, lymphoma, prostate cancer are the frequent solid malignancies.3
Globally, cancer cases are increasing, and 23.6 million new cancer cases are expected to be diagnosed in 2030.4 In 2020, around ten million deceased cancer patients were reported globally.3 This growing trend of cancer incidence has forced human beings to work more on cancer prevention and treatments.5
Although infectious diseases are the greatest burden for Sub-Saharan African Countries, cancer incidence is growing at an alarming rate.6 Around 70% of deaths in developing countries were due to cancer.7 In sub-Saharan Africa, prostate cancer, liver cancer, esophageal cancer, Kaposi sarcoma, and colorectal cancer are the most common solid malignancies in males. On the other hand, breast, cervical, and ovarian are the commonest cancers among the female population.6
Early detection and treatment of cancer have an immense contribution to reduce the survival and mortality of cancer patients.8 However, there are inadequate resources to diagnose and treat cancer in developing countries, resulting in poor treatment outcomes, significant morbidity and mortality, increased healthcare costs, and reduced quality of life.8,9 Furthermore, even with chemotherapy, patients experienced mild to life-threatening adverse effects. In addition, there is an enormous probability of not achieving the desired treatment outcomes due to the cytotoxicity of most anticancer agents and unpredictable treatment outcomes due to inter-individual pharmacokinetic variability.9,10 Despite a lack of comprehensive evidence about treatment outcomes in prostate cancer patients in the study setting, earlier research in Kenya on the survival of undifferentiated and poorly differentiated prostate cancer was poor irrespective of how it was treated.11 In addition, a previous systematic review reported that the survival rate of breast cancer patients was relatively low.12 Despite this, there is a paucity of evidence about the treatment outcome of breast cancer, prostate cancer and lymphoma patients in Kenya. Therefore, this study was envisioned to investigate the treatment outcomes and associated factors among adult patients diagnosed with selected solid malignancies at the Oncology Department of Kenyatta National Hospital.
Materials and Methods
Study Setting and Period
The study was conducted at the Oncology Department of Kenyatta National Hospital from 1st July 2020 to 31st December 2021. KNH is the biggest tertiary hospital in East & Central Africa, with an 1800 bed capacity. Currently, it has 50 inpatient wards, 22 clinics, and 24 theatres. Since it is the largest tertiary hospital in Kenya, it has a diversified patient population drawn from across the country.
Study Design
A single-arm prospective cohort study was employed to assess the treatment outcomes among adult patients with selected solid malignancies. Treatment outcome was measured at the end of the 12 months follow-up period for the respective cancer types.
Target Population
All treatment-naive hospitalized and ambulatory adult patients with a histologically confirmed diagnosis of prostate cancer, lymphoma, and breast cancer treated in the Oncology Department of KNH were targeted in the study. Those malignancies are targeted to study based on their higher prevalence and the possibility of having treatment outcome measuring parameters in the context of the study setting.
Eligibility Criteria
Inclusion Criteria
- All treatment-naive adult patients (≥18 years) with a histologically confirmed diagnosis of prostate cancer, lymphoma, and breast cancer treated in the hospital between 1st July 2020 to 31st December 2020 were enrolled for the follow-up study period.
- Patients who signed the informed written consent.
Exclusion Criteria
- Prostate cancer, lymphoma and breast cancer patients started and completed their treatment before the beginning of the study.
- Patients who were not willing to participate in the study.
- Unconscious patients who could not provide information during the data collection.
Sample Size and Sampling Techniques
All new eligible patients with a histologically confirmed diagnosis of solid malignancies (prostate cancer, lymphoma and breast cancer) during the study period were included. Hence, a consecutive sampling technique was employed since all eligible new patients were studied because of having a small population for the selected solid malignancies. Accordingly, 99 breast cancer patients, 50 lymphoma patients, and 82 prostate cancer patients were included in the study.
Data Collection Tool and Procedure
The principal investigator, co-investigators, oncology residents, Oncology Pharmacists and United States International University-Africa fourth-year Pharmacy students were involved in the data collection. In addition, relevant training was given for the data collectors regarding the appropriate use of the tool for data collection. A semi-structured questionnaire consisting of socio-demographics, clinical characteristics, ECOG (The Eastern Cooperative Oncology Group) performance scale,13 and The European Organization for Research and Treatment of Cancer Quality of life Questionnaire (EORTC QLQ 30)14 was employed to collect the data.
By interviewing patients and reviewing their medical records, pertinent data such as health-related quality of life, sociodemographics, histological type of cancer, co-morbidities, clinical stage of cancer, treatment regimens, and hormone receptor status were collected. Two measurements were done for each patient during the follow-up period. The first measurement (before the commencement of cancer treatment) was done as a baseline measurement to collect data on the ECOG performance scale, the stage of cancer, and other relevant socio-demographic, clinical characteristics and health-related quality of patients. The second follow-up measurement was conducted one year after the start of appropriate cancer therapy for each cancer type. In this last phase of data collection, mortality, cancer-specific survival time, remission status and health-related quality of data was collected to determine treatment outcomes.
Before initiating the actual study, a pre-test was performed on ten patients to confirm the reliability of the data collection instruments. Following the pre-test, all the required modifications were implemented on the tools before applying them in the actual research.
Study Variables
The outcome variable of interest was treatment outcome. The following possible outcomes were targeted; mean survival time, health-related quality of life, and disease metastasis after treatment. Besides, the following variables, such as age, presence of co-morbidity, type of co-morbidity, treatment regimen, stage of cancer, histological type of cancer, and hormone receptor status, were likely to influence the outcome variables.
Reliability and Validity of the Instruments
Standard tools such as the EORTC Quality of Life Questionnaire were used to ensure the replicability of the instruments. Besides, the Cronbach alpha test (α value should be > 0.7) was also employed to assess the reliability of the tools used for data collection.
Validity of the questionnaire was maintained by pre-testing the data collection instrument, expert opinion, or feedback (medical oncologists, oncology pharmacists, and epidemiologists) and recruiting representative samples of the target population. After reviewing expert opinion and pilot study, all necessary modifications were incorporated in the final questionnaire.
Data Analysis
The data were coded, inserted, cleaned and analyzed using the latest version of SPSS statistical software. Categorical patient characteristics were summarized using descriptive statistics, and continuous variables were reported using mean and standard deviation. Survival outcomes were evaluated using the Kaplan-Meier analysis, and a Log rank test was used to assess the difference in survival probability across different treatment regimens. Univariate and multivariate Cox regression analyses were used to investigate the predictors of survival outcomes. Statistical significance was considered at a p-value of ≤0.05.
Operational Definition of Terms
Adult patients: Cancer patients with selected diagnosis of malignancies 18 years and above.
Baseline data: The information collected before the beginning of treatment.
Cancer-specific survival: is defined as the time interval from the date of primary cancer diagnosis to the date of cancer related-death or last follow-up.
Cancer-specific survival after metastasis: defined as the time interval from the date of the first radiographic metastasis to the date of cancer related-death or last follow-up.
Complete remission: defined as no evidence of disease on repeat scanning after treatment.
Treatment outcome: is defined in terms of health-related quality of life, mortality, cancer-specific survival, metastasis-free survival, cancer-specific survival after metastasis, complete and partial remission.
Metastasis-free survival: defined as the time interval from the date of primary cancer diagnosis to the first radiographic metastasis.
Non-response: defined as failure to achieve partial remission.
Partial remission: defined as a reduction in tumor volume of at least 50% compared with pretreatment imaging.
Progressive disease: defined as increased size of the tumor despite therapy.
Selected solid malignancies: Adult patients with a histologically confirmed diagnosis of prostate cancer, breast cancer and lymphoma.
Treatment naive: A patient who will not start cancer therapy before the beginning of the study.
Good health-related quality of life: A high mean score (≥60) on the functional scale and a low mean score (<60) on the symptom scale of the EORTC QLQ 30 questionnaire.
Poor health-related quality of life: Represented by a low mean score (<60) on the functional scale and a high mean score (≥60) on the symptom scale of the EORTC QLQ 30 questionnaire.
Results
Socio-Demographic Characteristics of the Patients
A total of 231 patients, 99 breast cancer patients, 50 lymphoma patients, and 82 prostate cancer patients, were included in the study. The mean age of breast cancer patients was 49.2 ±12.1 years, while the mean age of prostate and lymphoma patients was 68.5 ±7.9 years and 37.8 ±16.4 years, respectively. Most of the patients completed secondary level education in all three types of cancers. Besides, most of the study participants had no family history of cancer in all the cancer types included in the study (Table 1).
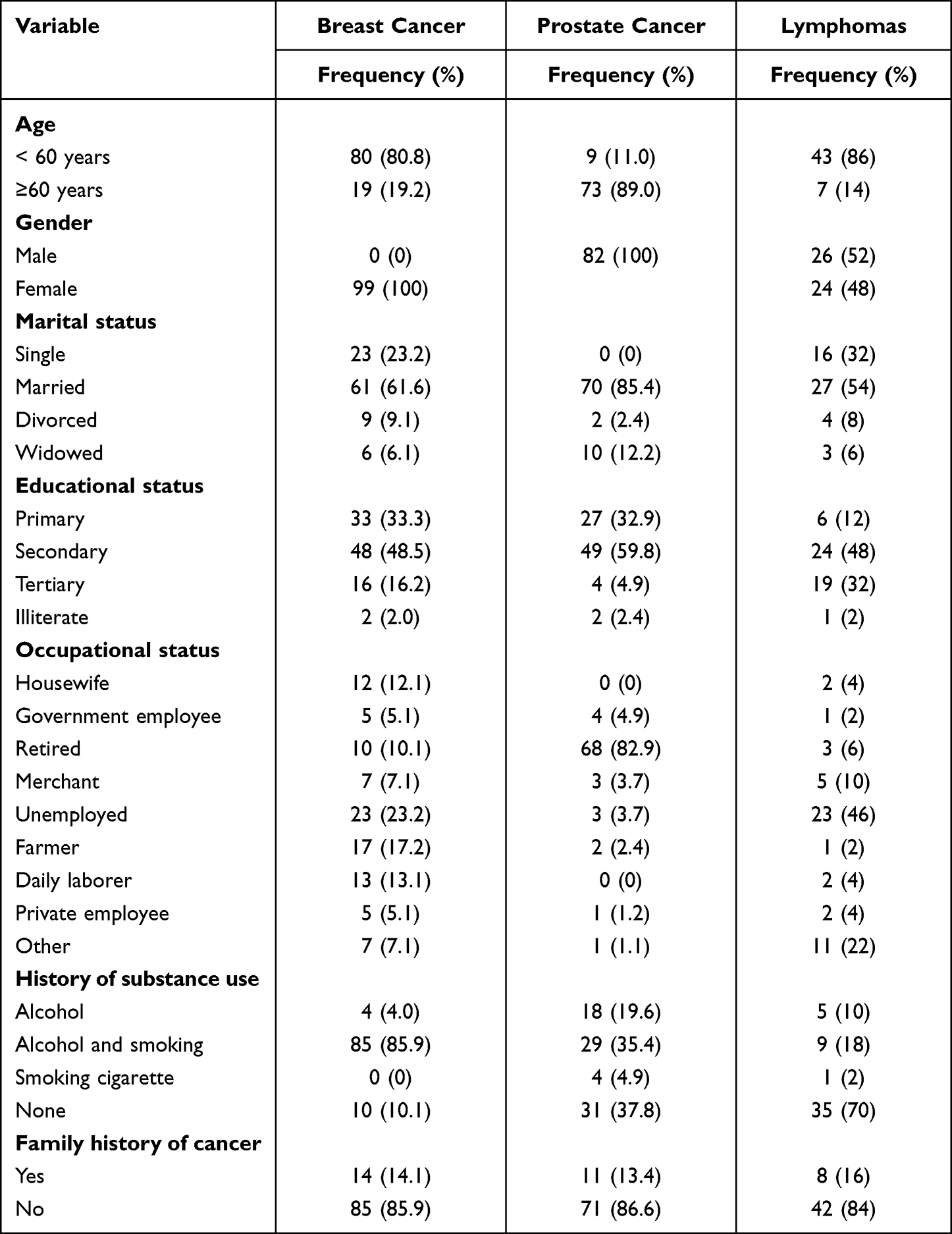 |
Table 1 Socio-Demographic Characteristic of the Study Participants |
Clinical Characteristics of the Study Participants
The present study showed that 48.5%, 50%, and 54% of breast cancer patients, prostate cancer patients, and lymphoma patients had comorbid conditions, respectively. Of those, hypertension accounted for 30.3% and 45.1% of co-morbidities in breast and prostate cancer patients, respectively. Nonetheless, deep vein thrombosis, hypertension and hepatitis were relatively the least prevalent co-morbidities in lymphoma patients. Most prostate cancer patients (74.4%) had distant metastasis at diagnosis (Table 2).
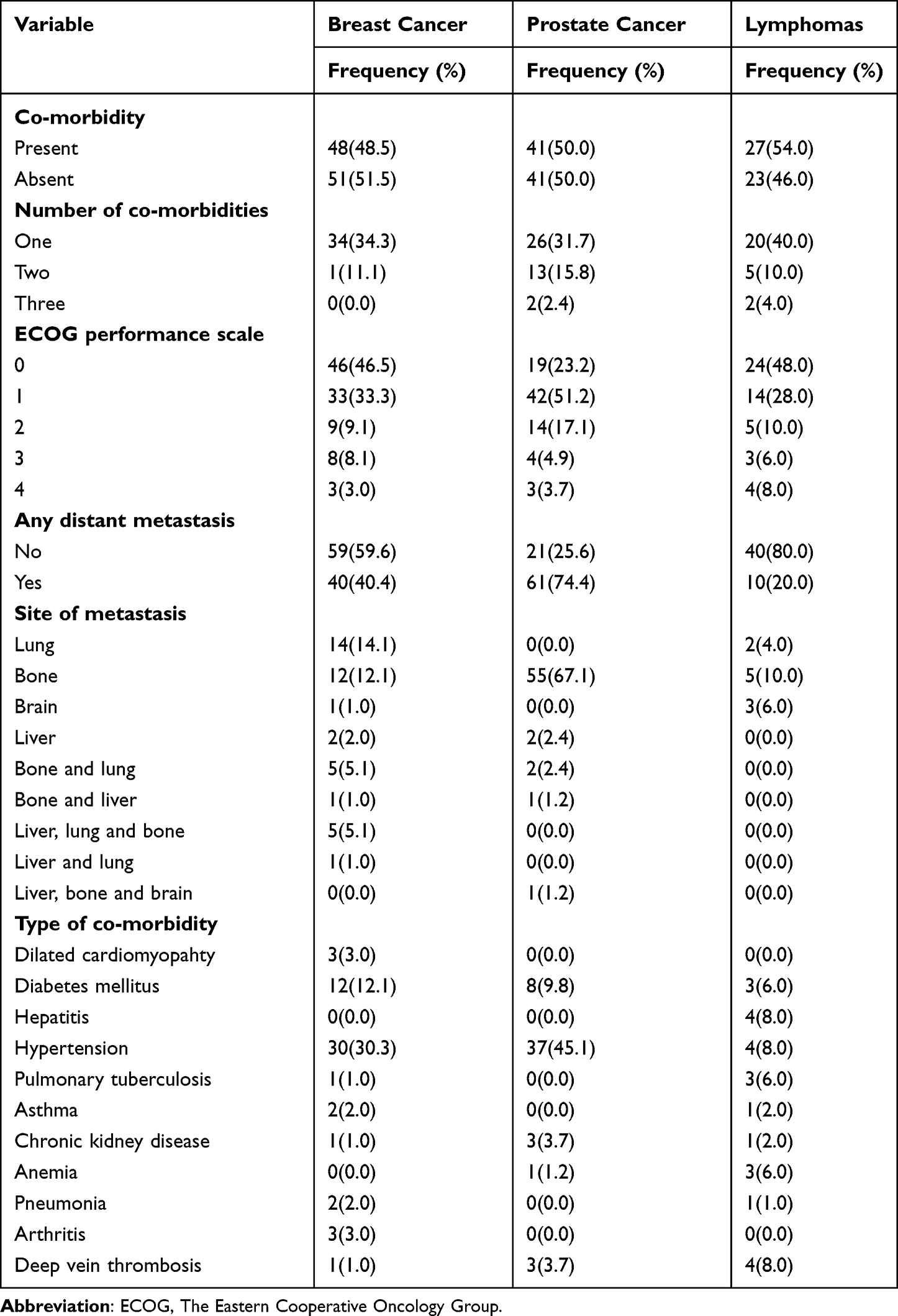 |
Table 2 Clinical Characteristics of the Study Participants |
The present study showed that most breast cancer and lymphoma patients had stage III tumor, nodes, and metastases (TNM) staging of the disease. Nonetheless, the predominant proportion of prostate cancer patients (73%) had an advanced stage of the disease (Figure 1).
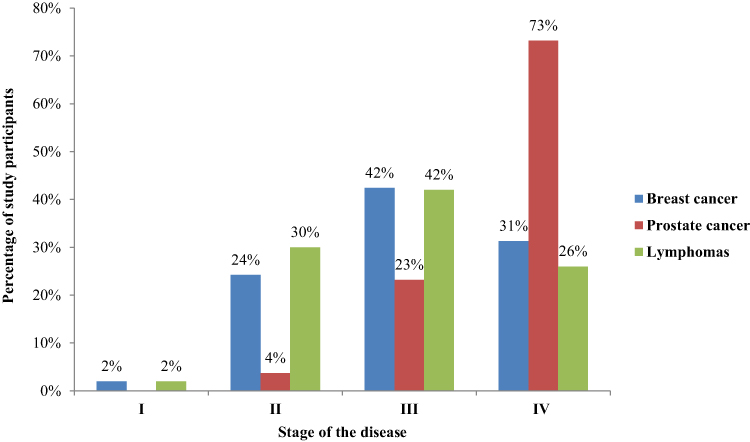 |
Figure 1 TNM staging of the disease among the study participants. |
The present study showed that 29.3% of breast cancer patients had estrogen and progesterone receptor-positive while 17.2% had triple receptor-negative hormone receptor status. In addition, 16.2% of the study participants had human epidermal growth factor receptor 2 Positive cancer (Appendix I).
Histologically, invasive ductal carcinoma accounted for the most prevalent (97%) types of breast cancer. In contrast, invasive lobular carcinoma and non-invasive ductal carcinoma were the least prevalent histological types of breast cancer. In prostate cancer patients, adenocarcinoma was the most commonly diagnosed histologically. Among lymphoma patients, non-Hodgkin’s lymphoma accounted for 62% of cases (Appendix II).
The current study demonstrated that most breast cancer, prostate cancer, and lymphoma patients had no significant change in serum creatinine, liver function test, or hematological parameters during the last follow-up period. Despite this, 51.5% of breast cancer and 28% of lymphoma patients had a low hemoglobin level in the last follow up period. Furthermore, 20% of lymphoma patients had a significantly abnormal liver function test (Appendix III).
In terms of treatment, 29.3% of breast cancer patients had been treated with the combination of radiotherapy, chemotherapy, surgery and endocrine therapy in the study setting. In prostate cancer patients, endocrine therapy (26.8%) was the mainstay of treatment. Nonetheless, chemotherapy was the least commonly used treatment regimen among prostate cancer patients. Contrastingly, chemotherapy was the principal treatment approach (80%) among lymphoma patients (Table 3).
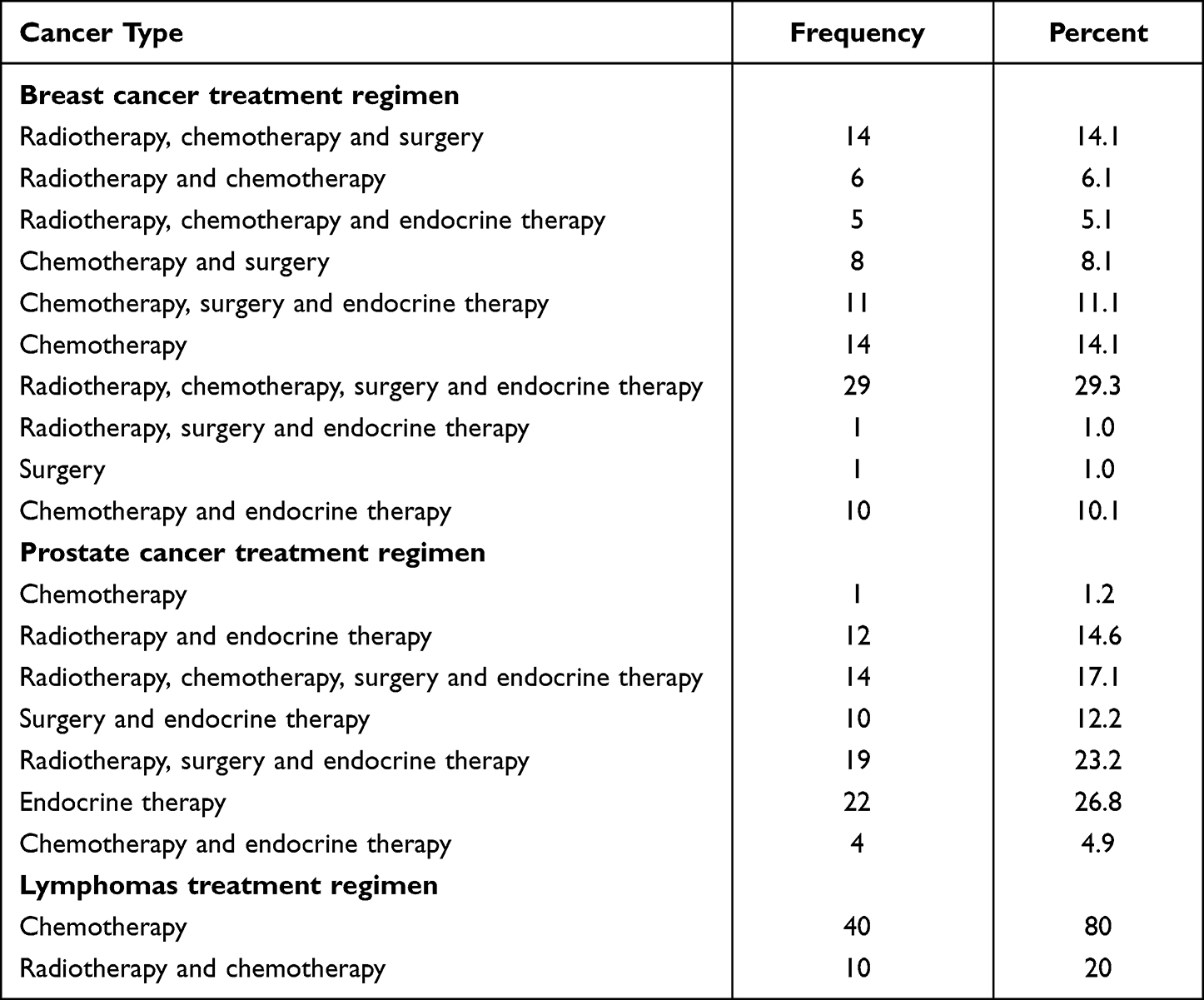 |
Table 3 Treatment Regimens Used for the Study Participants |
In breast cancer patients, tamoxifen accounted for 34.5% of endocrine therapy used in the study setting. In contrast, letrozole was the least (1%) prevalent endocrine therapy among breast cancer patients in the study setting. In addition, the combination of doxorubicin, cyclophosphamide, and paclitaxel was the most commonly used chemotherapy regimen (40.4%) in breast cancer patients. In prostate cancer patients, the combination of goserelin and bicalutamide was the most prevalent endocrine therapy used in the study setting. In lymphoma patients, ABVD (doxorubicin, bleomycin, vinblastine and dacarbazine) regimen accounted for 38% of cases in the study setting (Table 4).
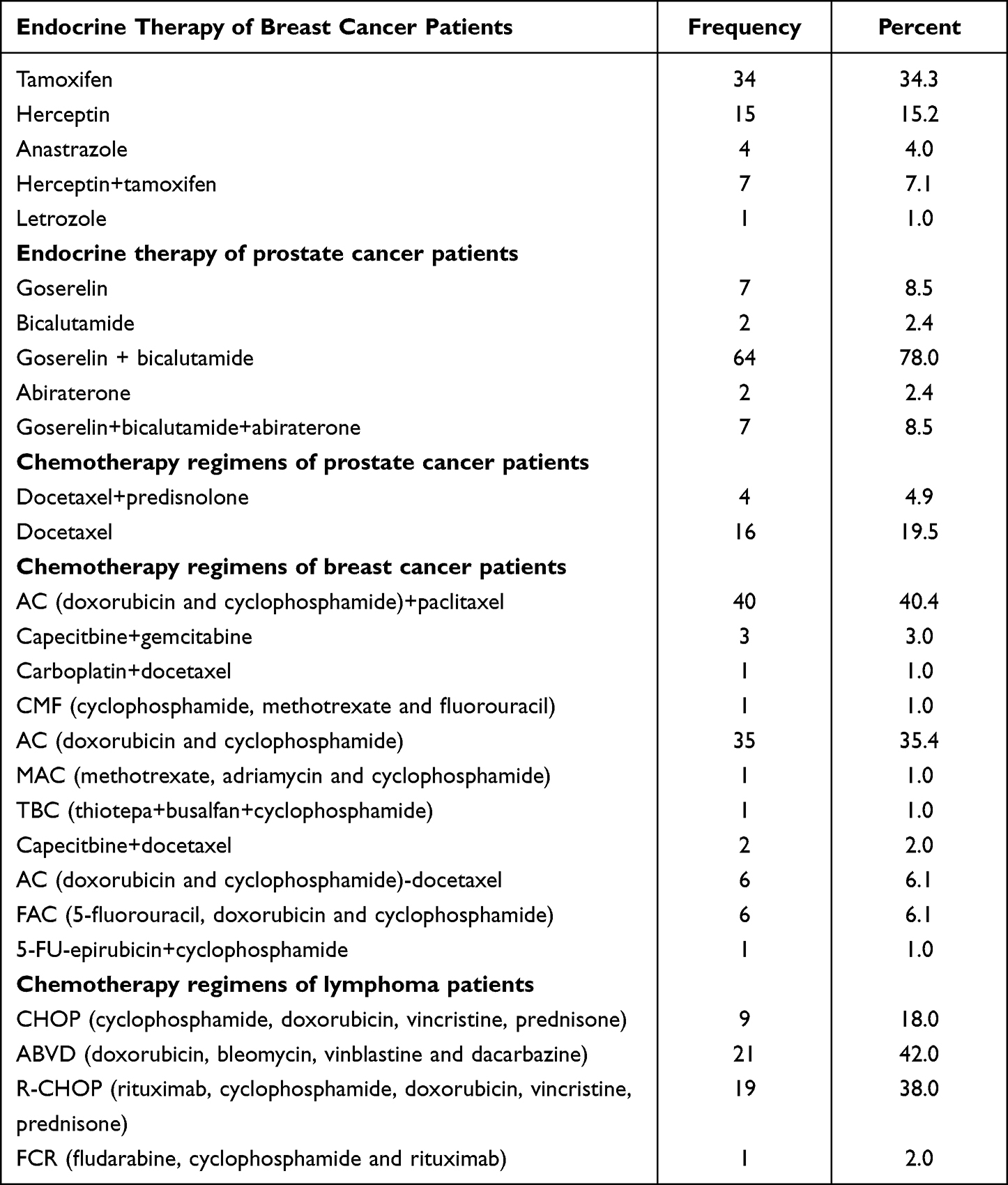 |
Table 4 Types of Endocrine Therapy and Chemotherapy Regimens Used Among the Study Participants |
Survival Outcomes Among the Study Participants
The mortality rate among breast and prostate cancer patients was 3% and 4.9%, respectively, in the last follow up period. In contrast, the mortality rate was 10% among lymphoma patients, while the other 90% of patients had censured outcomes. Most patients with breast cancer (45.5%), prostate cancer (45.1%), and lymphoma (42%) experienced partial remission during the most recent follow-up period. Nonetheless, only a small percentage of prostate cancer and lymphoma patients had complete remission in the last follow up period. Twenty-four percent of breast cancer, 36.6% prostate cancer and 20% lymphoma patients had disease progression in the last follow up (Table 5).
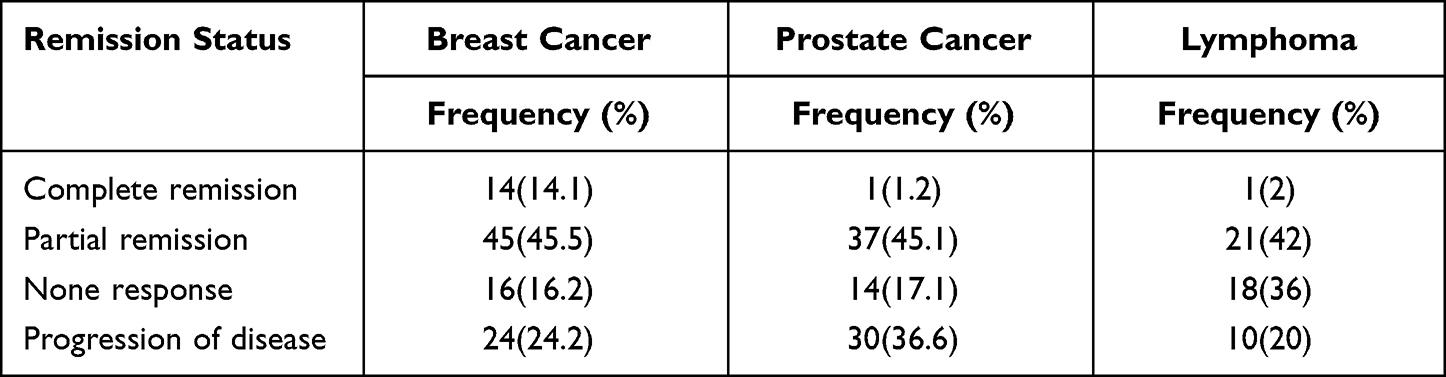 |
Table 5 Status of Remission of the Patients During the Last Follow-Up Period |
According to the findings of the current study, the mean cancer-specific survival was 11.4 months, 11.5 months, and 10.7 months for breast cancer, lymphoma, and prostate cancer patients, respectively. In addition, the mean metastasis-free survival time was 10.8 months, 10.2 months, and 11.2 months among breast cancer, lymphoma and prostate cancer patients, respectively (Table 6).
 |
Table 6 Mean Cancer-Specific Survival Outcomes Among the Study Participants |
The Kaplan Meier analysis of the present study demonstrated that breast cancer, lymphoma and prostate cancer patients with co-morbidity, distant metastasis, advanced stage of the disease and older than 60 years had a shorter mean survival estimate than their respective counterparts. In addition, the Log rank test revealed a statistically significant mean difference in the mean survival estimate among all cancer patients with 60 years and above, distant metastasis, advanced stage of the disease and comorbid conditions as compared to their counters parts as described in Table 7.
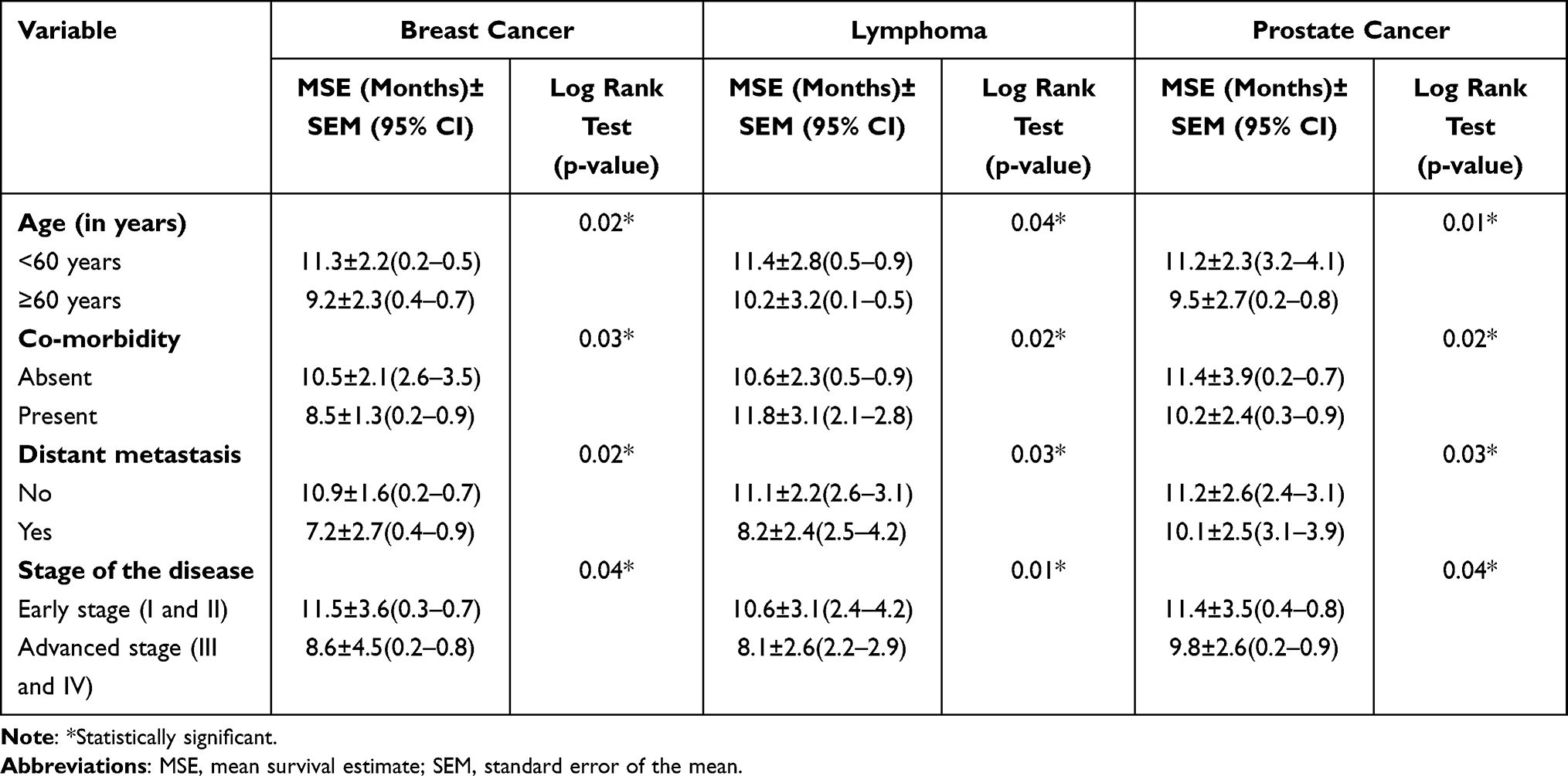 |
Table 7 Mean Survival Estimate Among the Study Participants |
Predictors of Mortality Among the Study Participants
The multivariate cox-regression analysis showed that breast cancer patients above 60 years had 2.8 times more risk of dying than those below 60 years of age (AHR:2.8, 95% CI: 0.2–0.7, p=0.001). In addition, breast cancer patients who had co-morbidity, distant metastasis, and advanced stage of disease had 2.2 (AHR: 2.8, 95% CI: 0.2–0.7, p=0.001), 3.1 (AHR: 2.8, 95% CI: 0.3–0.8, p=0.002) and 2.1 (AHR: 2.8, 95% CI: 1.5–2.3, p=0.01) times more risk of dying than their counterparts, respectively.
In lymphoma patients, the multivariate cox-regression analysis depicted that the risk of dying was 2.4 (AHR:2.4, 95% CI: 3–5, p=0.002), 2.3 (AHR:2.3, 95% CI: 0.5–0.9, p=0.04), 3.1 (AHR: 3.1, 95% CI: 0.3–0.9, p=0.02) and 2.5 (AHR:2.5, 95% CI: 1.3–2.9, p=0.03) times more among patients who had co-morbidity, distant metastasis, and advanced stage of disease as compared to their counterparts, respectively. Furthermore, older age above 60 years, presence of co-morbidity, distant metastasis and advanced stages of disease were statistically significant predictors of mortality among prostate cancer patients (Table 8).
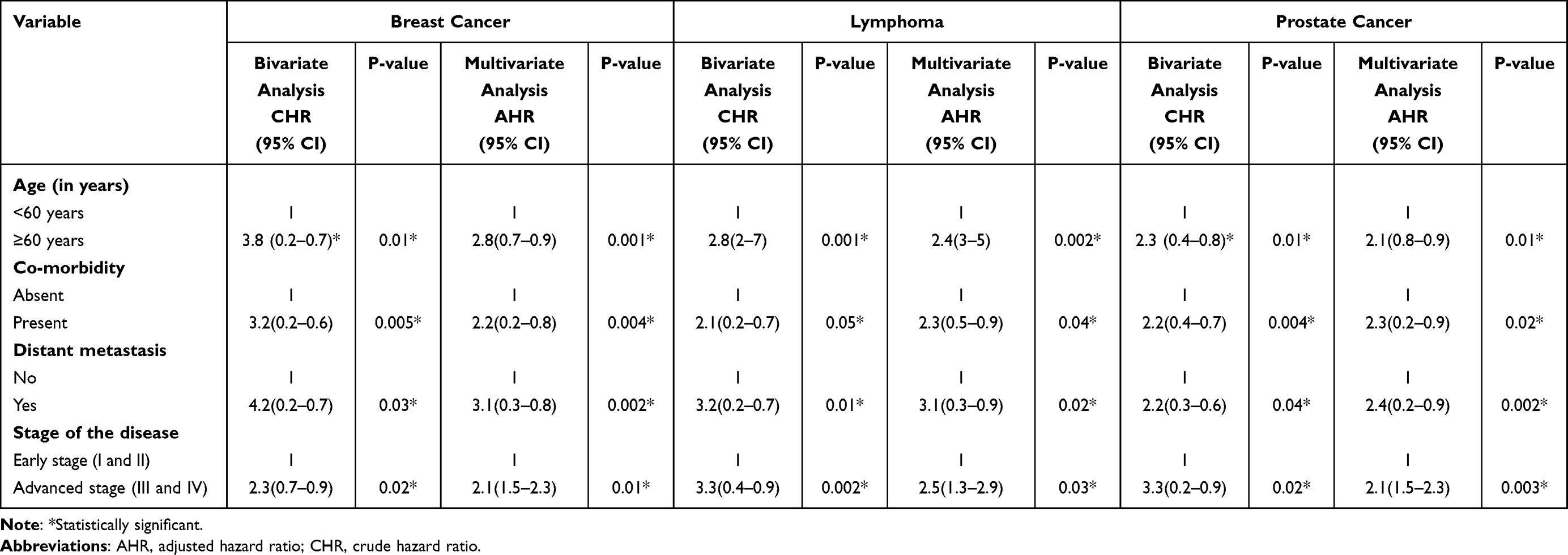 |
Table 8 Predictors of Mortality Among the Study Participants |
Health-Related Quality of Life Among the Study Participants
The study’s findings showed a significant improvement in all domains of health-related quality of life after initiation of treatment among breast cancer, lymphoma, and prostate cancer patients (Table 9). Besides, most breast cancer (64%), lymphoma (58%) and prostate cancer (85%) patients had a good overall global health-related quality of life in the last follow up period (Figure 2).
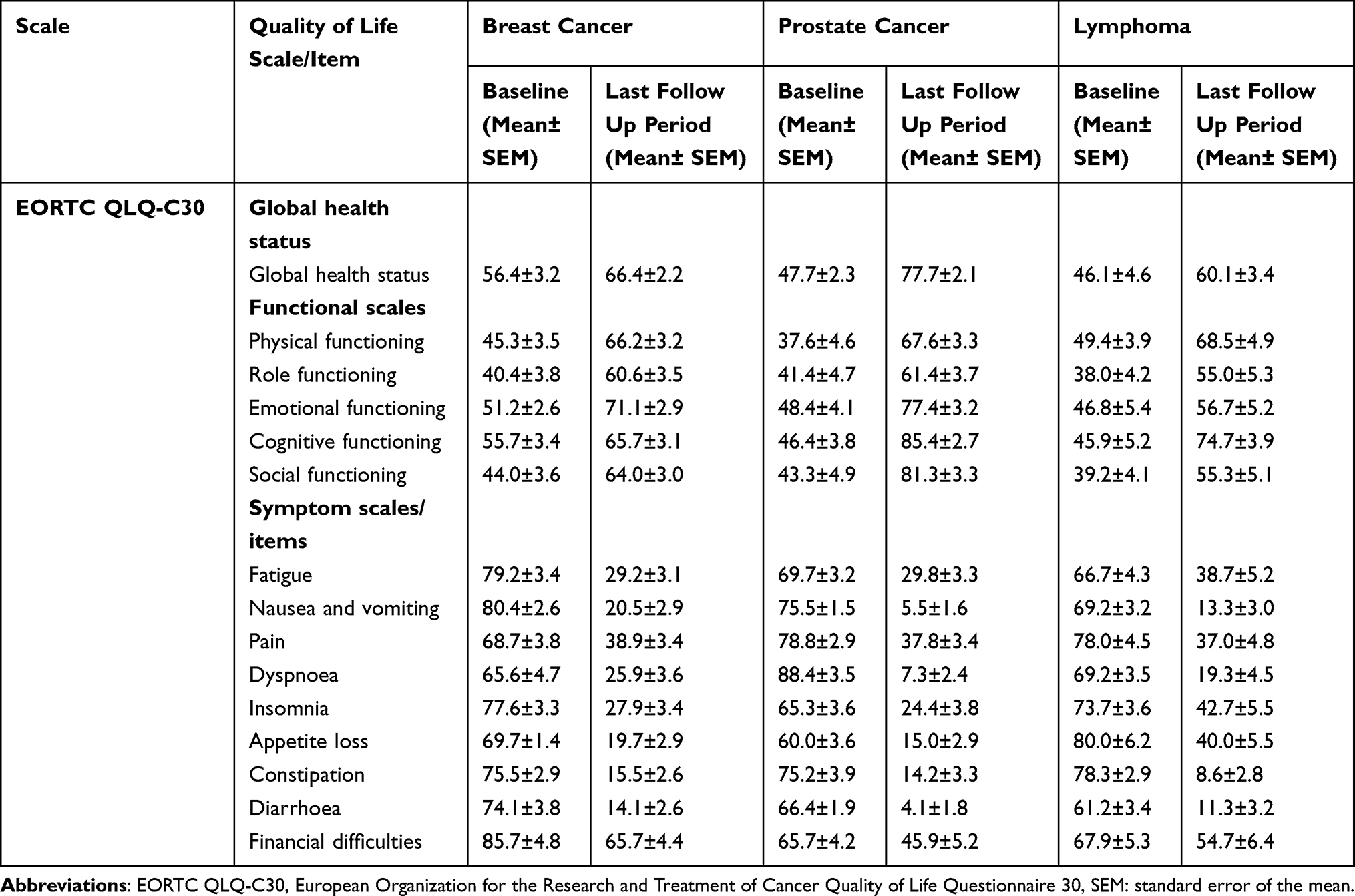 |
Table 9 Health-Related Quality of Life Among the Study Participants |
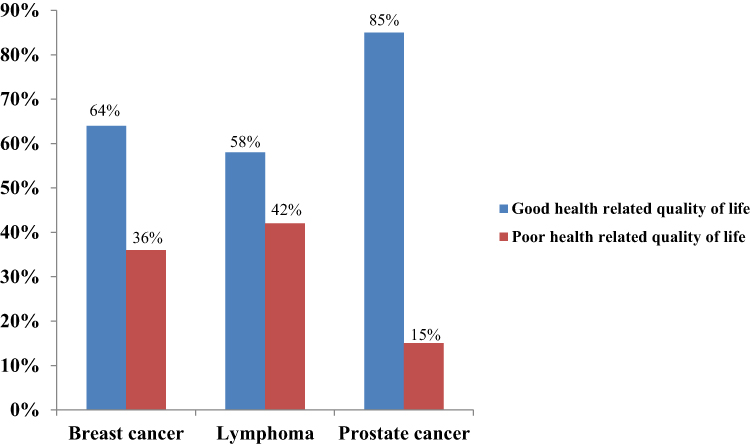 |
Figure 2 Overall health-related quality of life of the study participants in the last follow up period. |
Discussion
The study assessed treatment outcomes and associated factors among breast cancer, lymphoma and prostate cancer patients. The mean ages of the study participants were 49.2 ±12.1, 68.5 ±7.9 and 37.8 ±16.4 years in breast cancer, prostate and lymphoma patients, respectively. A global study reported a higher frequency of early-onset breast cancers in developing countries than in developed countries.15 Similarly, other studies showed that the mean age of breast and prostate cancer patients was 52.57, 68.4 and 66 years, respectively.16–18 In contrast to our study, the median age of diagnosis among lymphoma patients was 67.2 years, as reported by Smith et al study.19 However, the mean age of lymphoma patients in our setting is in agreement with the American Cancer Society report, which showed that the average age of diagnosis in Hodgkin lymphoma patients was 39 years.20 This similarity could be probably due to the high prevalence of lymphoma in early adulthood in both settings.
The present study showed that most breast cancer and lymphoma patients had stage III tumor, nodes, and metastases (TNM) staging of the disease, which reflects the lack of adequate awareness of early cancer screening in our setting. In contrast, Japanese, Chinese and Ethiopian studies showed that most breast cancer patients had clinical stage II and III cancer.21–23 Nonetheless, the predominant proportion of prostate cancer patients (73%) had an advanced stage of the disease. This urges the implementation of public awareness strategies of prostate cancer’s early signs and symptoms in our setting to circumvent the high prevalence of advanced-stage prostate cancer patients. These findings agree with the Rwandese and Nigerian study, which showed that most (85%) prostate cancer patients had an advanced and were locally advanced (88.9%) stage at the time of diagnosis, respectively.16,24 Such differences may be due to differences in literacy level and health-seeking behaviour of patients.
In addition, a significant proportion of breast cancer patients had estrogen and progesterone receptor-positive (29.3%) and human epidermal growth factor receptor 2 Positive cancer (16.2%). Likewise, previous systematic reviews and meta-analyses in East African countries reported an overall high (55%) prevalence of estrogen receptor-positive breast cancer subtypes.25 A Chinese study also revealed a higher proportion of ER-positive (79.5%) and HER-2 positive breast cancer (70.8%) among the study participants.22 Despite this fact, a sub-Saharan Africa study demonstrated that many patients did not initiate treatment (17%) one year after diagnosis due to financial constraints.26 Therefore, a collaborative effort is indispensable at the national level for equitable access to cancer treatment to effectively control the prevalent breast cancer subtypes in the study setting.
Histologically, invasive ductal carcinoma was the most prevalent (97%) type of breast cancer. Similarly, an Ethiopian study demonstrated that 95.63% of breast cancer patients had invasive ductal carcinoma.23 In prostate cancer patients, adenocarcinoma was the most commonly diagnosed histologically. Among lymphoma patients, non-Hodgkin’s lymphoma accounted for 62% of cases.
Previous studies showed that bone-only metastasis accounted for most breast cancer patients.27–29 Contrastingly, metastasis to the lung (14.1%) was the major site of metastasis among breast cancer patients in our setting, which is in line with a study reported by Chen et al in metastatic breast cancer patients.30 In addition, bone (67.1%) and brain (6%) was the frequent metastasis site for prostate cancer and lymphoma, respectively. Due to the unique genetic characteristics of metastatic tumors, they might be highly resistant to standard treatments. Hence, adequate strategies should be designed to promote early screening and provide efficient cancer treatment at the national level.
In our study, there are relatively higher percentages of mortality due to prostate cancer (4.9% vs 3.8%) and lymphoma (10% vs 3.2%) than GLOBOCAN estimates in 185 countries.31 Further, the mortality rate of breast cancer was slightly higher than the Taiwanian study (0.9% one year after treatment) and lower than GLOBOCAN estimates in the East African countries (10.8%).17,32 This variation may be due to the differences in the age of the study population, stage of cancer, level of metastasis, duration of follow up time and healthcare setting. In addition, the findings are higher than a study conducted by Vargas et al in Colombia.33 Although the mortality was not high at 12 months, only a few patients had complete remission. For many patients, the disease was progressing, although 12-month mortality was not high. Therefore, longer follow up will be required to accurately report cancer mortality among the study participants.
Due to the advent of rituximab, the relative survival outcomes of lymphoma patients was improved significantly.34 Similarly, most lymphoma patients (38%) in our setting were treated with an R-CHOP regimen. Therefore, a lower mortality rate (10%) in the one year follow up period in the study setting could probably be due to the frequent use of the R-CHOP regimen as a first-line treatment modality in lymphoma patients.
According to this study, patients with co-morbidity, distant metastasis, advanced stage of the disease, and older than 60 years had a shorter mean survival estimate. Jung et al found that history of hypertension, ER/PR status, HER2 status, metastasis-free interval, metastatic location (including brain, bone and liver), and body mass index at diagnosis with metastatic breast cancer was the most relevant prognostic factors for survival after metastatic disease diagnosis.35 On the other hand, Chaturvedi et al reported that venous thromboembolic disease was a predictor of poor survival in patients with prostate cancer, especially those with advanced disease.36
Concerning associated factors of mortality, breast cancer patients with old age, presence of co-morbidity, distant metastasis, and advanced disease had a relatively higher risk of death. Tiruneh et al revealed that age, stage of breast cancer, menopausal status, and surgical therapy were significant predictors of death.37 In addition, another study conducted in Ethiopia showed that age, educational status, residence, baseline tumor size and pathology type were influential factors affecting the time to death of breast cancer patients at the hospital.38
Regarding predictors of prostate cancer associated with death, our study found that age above 60 years, presence of co-morbidity, distant metastasis, and advanced stages of disease were statistically significant risk factors of mortality. On the other hand, the study in Brazil reported that only age and the presence of co-morbidity were significant risk factors.39 Another study revealed that higher cancer prostate risk assessment scores and primary treatment with radiation were associated with an increased risk of death.40
Further, this study found that the presence of co-morbidity, distant metastasis, and advanced stage of disease were predictors of mortality due to lymphoma. Lin et al reported that age ≥ 80 years and involvement of the basal ganglia were identified as independent risk factors of early mortality.41 On the other hand, the study conducted in Brazil revealed that older age, male gender and white race were associated with higher mortality in lymphoma patients.42 Therefore, effective interventional strategies should be implemented among comorbid and advanced-stage patients to reduce mortality and extend survival time among all the selected malignancies in the study setting.
Due to the advancement of breast cancer treatment, the overall quality of life has been enhanced in breast cancer patients in the past ten years.43 In terms of health-related quality of life, there was a significant improvement in all domains of quality of life after 12 months of treatment among breast cancer patients in our setting. Besides, most breast cancer (64%) patients had a good overall global health-related quality of life in the last follow up period. The finding of this study is in agreement with a previous study by Zamel et al which depicted a better overall global health status of breast cancer patients after chemotherapy.44 A Moroccan study also reported a higher mean score of overall global health status in breast cancer patients.45 Contrastingly, radiotherapy treatment did not substantially improve the health-related quality of life in early-stage breast cancer patients.46 However, endocrine therapy with aromatase enzyme inhibitors had a significant positive association with most health-related quality of life domains.47 Previous systematic reviews reported that breast cancer patients with metastatic disease had a worse health-related quality of life.48 In line with this report, a significant proportion (14.1%) of breast cancer patients who had an advanced disease in our setting had a poor overall quality of life on a global scale.
A previous study showed that most non-Hodgkin’s lymphoma patients had a good quality of life.49,50 Likewise, the findings of our study also revealed that most lymphoma (58%) patients had a good overall health-related quality of life. Another study also reported a significant improvement in the symptom scales of quality of life among Non-Hodgkin Lymphoma survivors.51 A German study demonstrated a considerable improvement in the mean scores of all functioning and symptom scales after treatment in Hodgkin Lymphoma patients.52
The present study showed that most (85%) prostate cancer patients had a good overall global health-related quality of life in the last follow up period, although a recent systematic review reported a poor overall health-related quality of life in various domains. Of which, sexual function was the most grossly affected domain.53 Similarly, a previous cohort study showed a significant improvement in most health-related quality of life domains 12 months after treatment of prostate cancer.54 In contrast, another study by Klein et al reported a lower health-related quality of life on an overall global scale and all functional domains of quality of life.55 In addition, a Korean study revealed a lack of improvement in urinary and sexual outcomes in prostate cancer patients after 12 months of treatment.56 Further, Kang et al found that 40–50% of prostate cancer survivors were not happy or satisfied with their life.51 Overall, there was a promising improvement in the health-related quality of life among all the study cancer types. Hence, further interventional strategies should be implemented to enhance all domains of health-related quality of life in the study setting.
Strengths and Limitations of the Study
The strength of our study was the involvement of a variety of cancers, absence of lost to follow up and completeness of the data collected from both medical records and interviewing the patients. However, it was a single centre study with a smaller sample size that could not be generalized to all populations.
Conclusions
Although the mortality was not high at 12 months, only a few patients had complete remission. For many patients, the disease was progressing, although 12-month mortality was not high. Therefore, longer follow up will be required to accurately report cancer mortality among the study participants. In addition, most of the patients had partial remission and a good overall global health-related quality of life in the last follow up period. Age above 60 years, co-morbidity, distant metastasis, and advanced stages of disease were statistically significant predictors of mortality among the study participants.
Abbreviations
AHR, adjusted hazard ratio; CHR, crude hazard ratio; ECOG, The Eastern Cooperative Oncology Group; EORTC QLQ 30, The European Organization for Research and Treatment of Cancer Quality of life Questionnaire; KNH, Kenyatta National Hospital.
Data Sharing Statement
The soft copy of the data is available from the corresponding author upon a reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by Kenyatta National Hospital, University of Nairobi, Ethics and Research Committee (Approval Number: P83/02/2020). After receiving ethical clearance, an official letter was presented to the Cancer Treatment Centre of the hospital to collect data from the patients and their medical records. The name and other identities of the patients were not recorded during the data collection to ensure the confidentiality of the data. Before the commencement of the study, written informed consent was obtained from all the study participants of the study to collect information from them and use their medical records. The study was conducted in compliance with the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge the United States International University-Africa for their financial support in this project. We also extend our gratitude to the patients and all the oncology staff members of Kenyatta National Hospital for their assistance in completing this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the United States International University-Africa [grant number: 102855].
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. National Cancer Institute. What is cancer? [Internet]; 2015 [cited October 3, 2018]. Available from: https://www.cancer.gov/about-cancer/understanding/what-is-cancer.
2. National Cancer Institute. Cancer classification [Internet]; 2018 [cited October 10, 2018]. Available from: https://training.seer.cancer.gov/disease/categories/classification.html.
3. World Health Organization. Cancer [Internet]; 2021 [cited January 23, 2022]. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer.
4. Cancer Research UK. Worldwide cancer statistics [Internet]; 2018 [cited May 20, 2018]. Available from: http://www.cancerresearchuk.org/health-professional/cancer-statistics/worldwide-cancer.
5. Gavhane Y, Shete A, Bhagat A, et al. Solid tumors: facts, challenges and solutions. Int J Pharma Sci Res. 2011;2(1):1–12.
6. Olaleye O, Ekrikpo U. Epidemiology of cancers in Sub-Saharan Africa. In: Cancer in Sub-Saharan Africa: Current Practice and Future. Springer International Publishing; 2017:3–19.
7. World Health Organization. Cancer key facts [Internet]; 2018 [cited May 20, 2018]. Available from: http://www.who.int/news-room/fact-sheets/detail/cancer.
8. Neal RD. Do diagnostic delays in cancer matter? Br J Cancer. 2009;101(S2):S9–12. doi:10.1038/sj.bjc.6605384
9. Cagan R, Meyer P. Rethinking cancer: current challenges and opportunities in cancer research. Dis Model Mech. 2017;10(4):349–352. doi:10.1242/dmm.030007
10. Undevia SD, Gomez-Abuin G, Ratain MJ. Pharmacokinetic variability of anticancer agents. Nat Rev Cancer. 2005;5(6):447–458. doi:10.1038/nrc1629
11. Magoha GA. Management and survival in advanced prostate cancer in Nairobi. East Afr Med J. 2000;77(5):260–263. doi:10.4314/eamj.v77i5.46630
12. Rezaianzadeh A, Jalali M, Maghsoudi A, Mokhtari AM, Azgomi SH, Dehghani SL. The overall 5-year survival rate of breast cancer among Iranian women: a systematic review and meta-analysis of published studies. Breast Dis. 2017;37(2):63–68. doi:10.3233/BD-160244
13. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655. doi:10.1097/00000421-198212000-00014
14. Cocks K, King MT, Velikova G, Fayers PM, Brown JM; The European Organization for Research and Treatment of Cancer Quality of life. Quality, interpretation and presentation of European Organisation for Research and Treatment of Cancer quality of life questionnaire core 30 data in randomised controlled trials. Eur J Cancer. 2008;44(13):1793–1798. doi:10.1016/j.ejca.2008.05.008
15. Bidoli E, Virdone S, Hamdi-Cherif M, et al. Worldwide age at onset of female breast cancer: a 25-year population-based cancer registry study. Sci Rep. 2019;9(1):1–8. doi:10.1038/s41598-019-50680-5
16. Ajape A, Ibrahim KOO, Fakeye JA, Abiola OO. An overview of cancer of the prostate diagnosis and management in Nigeria: the experience in a Nigerian tertiary hospital. Ann Afr Med. 2010;9(3):113–117. doi:10.4103/1596-3519.68353
17. Liu FC, Lin HT, Kuo CF, See LC, Chiou MJ, Yu HP. Epidemiology and survival outcome of breast cancer in a nationwide study. Oncotarget. 2017;8(10):16939–16950. doi:10.18632/oncotarget.15207
18. Rawla P. Epidemiology of prostate cancer. World J Oncol. 2019;10(2):63. doi:10.14740/wjon1191
19. Smith A, Crouch S, Lax S, et al. Lymphoma incidence, survival and prevalence 2004–2014: sub-type analyses from the UK’s Haematological Malignancy Research Network. Br J Cancer. 2015;112(9):1575–1584. doi:10.1038/bjc.2015.94
20. American Cancer Society. Key Statistics for Hodgkin Lymphoma [Internet]; [cited February 4, 2022]. Available from: https://www.cancer.org/cancer/hodgkin-lymphoma/about/key-statistics.html.
21. Sawaki M, Yamada A, Kumamaru H, et al. Clinicopathological characteristics, practical treatments, prognosis, and clinical issues of older breast cancer patients in Japan. Breast Cancer. 2021;28(1):1–8. doi:10.1007/s12282-020-01188-8
22. Qianxin C, Yixin Z, Ke L, et al. Characteristics and prognosis of female breast cancer in Guangzhou, 2008–2017. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(11):1831–1835. doi:10.3760/cma.j.cn112338-20191012-00731
23. Dagne S, Abate SM, Tigeneh W, Engidawork E. Assessment of breast cancer treatment outcome at Tikur Anbessa specialized hospital adult oncology unit, Addis Ababa, Ethiopia. Eur J Oncol Pharm. 2019;2(2):e13. doi:10.1097/OP9.0000000000000013
24. Nzeyimana I, Nyirimodoka A, Ngendahayo E, et al. Diagnosis of advanced prostate cancer at the community level in Rwanda. Int Urol Nephrol. 2021;53(10):1977–1985. doi:10.1007/s11255-021-02921-8
25. Popli P, Gutterman EM, Omene C, Ganesan S, Mills D, Marlink R. Receptor-defined breast cancer in five East African Countries and its implications for treatment: systematic review and meta-analysis. JCO Glob Oncol. 2021;7(7):289–301. doi:10.1200/GO.20.00398
26. Foerster M, Anderson BO, McKenzie F, et al. Inequities in breast cancer treatment in sub-Saharan Africa: findings from a prospective multi-country observational study. Breast Cancer Res. 2019;21(1):1–11. doi:10.1186/s13058-019-1174-4
27. Hamaoka T, Madewell JE, Podoloff DA, Hortobagyi GN, Ueno NT. Bone imaging in metastatic breast cancer. J Clin Oncol. 2004;22(14):2942–2953. doi:10.1200/JCO.2004.08.181
28. Tahara RK, Brewer TM, Theriault RL, Ueno NT. Bone metastasis of breast cancer. Adv Exp Med Biol. 2019;1152:105–129.
29. Wang R, Zhu Y, Liu X, Liao X, He J, Niu L. The Clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer. 2019;19(1):1091. doi:10.1186/s12885-019-6311-z
30. Chen MT, Sun HF, Zhao Y, et al. Comparison of patterns and prognosis among distant metastatic breast cancer patients by age groups: a SEER population-based analysis. Sci Rep. 2017;7(1):9254. doi:10.1038/s41598-017-10166-8
31. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
32. Global Cancer Incidence Mortality and Prevalence. Globocan 2020: Eastern Africa [Internet]; 2020 [cited March 24, 2022]. Available from: https://gco.iarc.fr/today/data/factsheets/populations/910-eastern-africa-fact-sheets.pdf.
33. Hernández Vargas JA, Ramírez Barbosa PX, Gil Quijano AM, Valbuena AM, Acuña L, González JA. Patterns of breast, prostate and cervical cancer incidence and mortality in Colombia: an administrative registry data analysis. BMC Cancer. 2020;20(1):1–9. doi:10.1186/s12885-020-07611-9
34. Wright F, Hapgood G, Loganathan A, et al. Relative survival of patients with lymphoma in Queensland according to histological subtype. Med J Aust. 2018;209(4):166–172. doi:10.5694/mja17.00937
35. Jung SY, Rosenzweig M, Sereika SM, Linkov F, Brufsky A, Weissfeld JL. Factors associated with mortality after breast cancer metastasis. Cancer Causes Control. 2012;23(1):103–112. doi:10.1007/s10552-011-9859-8
36. Chaturvedi S, Sidana S, Elson P, Khorana AA, McCrae KR. Symptomatic and incidental venous thromboembolic disease are both associated with mortality in patients with prostate cancer. PLoS One. 2014;9(8):e94048. doi:10.1371/journal.pone.0094048
37. Tiruneh M, Tesfaw A, Tesfa D. Survival and predictors of mortality among breast cancer patients in Northwest Ethiopia: a retrospective cohort study. Cancer Manag Res. 2021;13:9225–9234. doi:10.2147/CMAR.S339988
38. Tesfay B, Getinet T, Derso EA. Survival analysis of time to death of breast cancer patients: in case of Ayder comprehensive specialized hospital Tigray, Ethiopia. Cogent Med. 2021;8(1):1908648. doi:10.1080/2331205X.2021.1908648
39. Braga SFM, da Silva RP, Junior AAG, Cherchiglia ML. Prostate cancer survival and mortality according to a 13-year retrospective cohort study in Brazil: competing-risk analysis. Rev Bras Epidemiol. 2021;24:1–13. doi:10.1590/1980-549720210006
40. Kutikov A, Cooperberg MR, Paciorek AT, Uzzo RG, Carroll PR, Boorjian SA. Evaluating prostate cancer mortality and competing risks of death in patients with localized prostate cancer using a comprehensive nomogram. Prostate Cancer Prostatic Dis. 2012;15(4):374–379. doi:10.1038/pcan.2012.21
41. Lin CH, Yang CF, Yang HC, et al. Risk prediction for early mortality in patients with newly diagnosed primary CNS lymphoma. J Cancer. 2019;10(17):3958–3966. doi:10.7150/jca.32467
42. De Sá Gouveia M, Batista JKM, Passos TS, Prado BS, Siqueira CE, Almeida-Santos MA. Comparison of factors associated with leukemia and lymphoma mortality in Brazil. Cad Saude Publica. 2020;36(8):e00077119. doi:10.1590/0102-311x00077119
43. Mokhatri-Hesari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes. 2020;18(1):338. doi:10.1186/s12955-020-01591-x
44. Zamel ON, Inocian EP, Alshehry AS, Tumala RB, Patalagsa JG, Alsaleh KA. Quality of life among breast and colon cancer patients before and after first-cycle chemotherapy. J Holist Nurs. 2021;39(2):116–125. doi:10.1177/0898010120958859
45. El Fakir S, El Rhazi K, Zidouh A, et al. Health-related quality of life among breast cancer patients and influencing factors in Morocco. Asian Pacific J Cancer Prev. 2016;17(12):5063–5069.
46. Jacobs DHM, Charaghvandi RK, Horeweg N, et al. Health-related quality of life of early-stage breast cancer patients after different radiotherapy regimens. Breast Cancer Res Treat. 2021;189(2):387–398. doi:10.1007/s10549-021-06314-4
47. Dibble KE, Bellizzi KM, Taxel P, et al. Physical activity and health-related quality of life among postmenopausal women with breast cancer treated with aromatase inhibitors. Support Care Cancer. 2021;29(5):2385–2394. doi:10.1007/s00520-020-05741-1
48. Gonzalez L, Bardach A, Palacios A, et al. Health-related quality of life in patients with breast cancer in Latin America and the Caribbean: a systematic review and meta-analysis. Oncologist. 2021;26(5):e794–806. doi:10.1002/onco.13709
49. Ariestine DA, Sari NK, Rinaldi I, Abdullah M. Quality of life in older survivors of non-Hodgkin’s lymphoma who received chemotherapy and related factors. J Geriatr Oncol. 2021;12(2):326–331. doi:10.1016/j.jgo.2020.09.002
50. Ellis S, Brown RF, Thorsteinsson EB, Pakenham KI, Perrott C. Quality of life and fear of cancer recurrence in patients and survivors of non-Hodgkin lymphoma. Psychol Health Med. 2021:1–12. doi:10.1080/13548506.2021.1913756
51. Kang D, Cho J, Kim IR, Kim MK, Kim WS, Kim SJ. Health-related quality of life in non-Hodgkin lymphoma survivors: a prospective cohort study. Cancer Res Treat. 2018;50(4):1051–1063. doi:10.4143/crt.2017.207
52. Kreissl S, Müller H, Goergen H, et al. Health-related quality of life in patients with Hodgkin lymphoma: a longitudinal analysis of the German Hodgkin Study Group. J Clin Oncol. 2020;38(25):2839–2848. doi:10.1200/JCO.19.03160
53. Odeo S, Degu A. Factors affecting health-related quality of life among prostate cancer patients: a systematic review. J Oncol Pharm Pract. 2020;26(8):1997–2010. doi:10.1177/1078155220959414
54. Shin DW, Lee SH, Kim TH, et al. Health-related quality of life changes in prostate cancer patients after radical prostatectomy: a longitudinal cohort study. Cancer Res Treat. 2019;51(2):556–567. doi:10.4143/crt.2018.221
55. Klein J, Lüdecke D, Hofreuter-Gätgens K, Fisch M, Graefen M, von Dem Knesebeck O. Income and health-related quality of life among prostate cancer patients over a one-year period after radical prostatectomy: a linear mixed model analysis. Qual Life Res. 2017;26(9):2363–2373. doi:10.1007/s11136-017-1582-9
56. Pak S, Kim M, Ahn H. Changes in health-related quality of life after radical prostatectomy for prostate cancer: a longitudinal cohort study in Korea. Investig Clin Urol. 2018;59(5):313–320. doi:10.4111/icu.2018.59.5.313
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.