")
Back to Journals » Infection and Drug Resistance » Volume 12
Treatment of severe ventriculitis caused by extensively drug-resistant Acinetobacter baumannii by intraventricular lavage and administration of colistin
Authors Chen F, Deng X , Wang Z , Wang L, Wang K, Gao L
Received 6 September 2018
Accepted for publication 14 December 2018
Published 21 January 2019 Volume 2019:12 Pages 241—247
DOI https://doi.org/10.2147/IDR.S186646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Eric Nulens
FuMei Chen,1,2,* Xianyu Deng,1,* Zhanpeng Wang,3 Li Wang,4 Ke Wang,1 Liang Gao1
1Department of Neurosurgery, Shanghai Tenth People’s Hospital, Tongji University, Shanghai 200072, China; 2Department of Emergency Surgery, The First Affiliated Hospital of Medical School of Zhejiang University, Hangzhou 360001, China; 3Department of Neurosurgery, Shanghai Clinical College, Anhui Medical University, Shanghai 200072, China; 4Intensive Care Unit, Sir Run Run Shaw Hospital, Zhejiang University, Hangzhou City 310016, China;
*These authors contributed equally to this work
Background: Severe ventriculitis (SV) caused by multidrug-resistant bacteria is associated with high morbidity and mortality in neurosurgical patients. This study assessed the outcomes of patients with SV caused by Acinetobacter baumannii who were treated by intraventricular (IVT) lavage and colistin administration.
Methods: This retrospective study included consecutive patients with SV caused by A. baumannii who were admitted at the Neurosurgical Department of Shanghai Tenth People’s Hospital from January 2014 to September 2017. Patients’ medical records, radiographic images, and surgical notes were reviewed. The patients were followed up for at least 6 months after discharge.
Results: A total of 25 patients, including 20 male and five female, were enrolled in this study; the average age was 45.6 years. All patients underwent neurosurgery before infection, and all A. baumannii cultures from cerebrospinal fluid (CSF) showed extensive resistance to the tested antibiotics except for tigecycline and colistin. All the patients underwent IVT lavage followed by daily administration of colistin after surgery; 24 patients received a daily colistin dose of 100,000 IU, while one received 50,000 IU. The patients also received tigecycline-based systemic antibiotic treatment. The mean duration of IVT colistin was 13.4±2.8 days. The time required to obtain a negative CSF culture was 8.9±4.0 days. Of the 20 patients who were cured, eight underwent shunt surgery due to hydrocephalus before they were discharged to a rehabilitation center. Five patients died, including one who was re-admitted due to recurrence 1 month after discharge.
Conclusions: IVT lavage and colistin treatment may be an effective treatment for SV caused by extensively drug-resistant A. baumannii. Future studies with a larger sample size may be needed to verify the findings in this study.
Keywords: severe ventriculitis, extensively drug resistant, intraventricular colistin, intraventricular lavage, Acinetobacter baumannii
Introduction
Ventriculitis is associated with high mortality and negatively affects the prognosis of neurosurgical patients. Procedures that can lead to post-neurosurgical ventriculitis include craniotomy, external ventricular drainage (EVD), ventriculostomy, lumbar puncture, and ventriculoperitoneal (VP) shunt insertion.1 Although prophylactic antibiotic therapy is commonly used before neurosurgical procedures, its effectiveness is uncertain.2 In recent years, the extensive use of antibiotics for the treatment of pneumonia and the increasing incidence of neurosurgery may have altered the epidemiology and clinical spectrum of ventriculitis.3–5 Acinetobacter baumannii is a common infectious agent in hospitals worldwide.6–8 This Gram-negative, non-fermentative coccobacillus of the Moraxellaceae family is characterized by a resistance island comprising 45 resistance genes against commercially available antibiotics. Thus, A. baumannii has been responsible for a massive increase in ventriculitis.7–10 Drugs used to treat A. baumannii infection include sulbactam, antipseudomonal cephalosporins, antipseudomonal carbapenems, monobactams, aminoglycosides, fluoroquinolones, tetracyclines, glycylcyclines, and polymyxins. However, the emergence of extensively drug-resistant (XDR) A. baumannii has reduced the therapeutic options for SV.11,12 XDR strains show no susceptibility to 15/17 types of antibiotic (at least one of each type of agent, including tigecycline and/or polymyxins).13,14
Colistin (formulated as colistimethate sodium) isolated from Bacillus polymyxa is a cationic antimicrobial peptide that is toxic to Gram-negative bacteria including A. baumannii and has been re-introduced into clinical practice to target XDR pathogens.13,15 Although colistin has never been through drug development programs or assessed in comparative clinical studies, it has shown favorable efficacy including in cases of central nervous system infection.15,16 Many studies have demonstrated that an extremely low level of colistin enters the cerebrospinal fluid (CSF) following intravenous (IV) administration; thus, intraventricular (IVT) and/or intrathecal (ITH) administration could be effective in the treatment of A. baumannii ventriculitis.17,18
In this study, we retrospectively analyzed our data on ventriculitis after neurosurgical procedures to evaluate the benefits and complications of colistin for treating infections caused by XDR A. baumannii.
Methods
We retrospectively analyzed the medical records of all patients with XDR A. baumannii ventriculitis hospitalized at the Department of Neurological Surgery and Neurosurgical Intensive Care Unit (NICU) of Shanghai Tenth People’s Hospital between January 2014 and May 2017. This study was approved by the ethics committee of Shanghai Tenth People’s Hospital. Informed consent was obtained from the patients’ next of kin.
Inclusion and exclusion criteria
The inclusion criteria were as follows:
- Patients with XDR A. baumannii ventriculitis who underwent ventricular lavage.
- Patients who had received IVT colistin and had undergone successive drainage of infected CSF (ie, EVD, Ommaya reservoir, and lumbar drainage).
- Patients experiencing their first episode of A. baumannii infection.
- Patients diagnosed with IVT empyema by computerized tomography (CT) scans or magnetic resonance imaging (MRI).
Exclusion criteria were as follows:
- Patients had concomitant postoperative central nervous system infection with an organism other than XDR A. baumannii.
- There were others organism besides XDR A. baumannii.
- Had a history of intracranial infection before cranial operations.
- Had received IV colistin treatment for intracranial infection or infection at other locations.
Definitions
There is no established definition of severe ventriculitis (SV); we therefore defined this condition as IVT empyema according to the CT scan or MRI results. A definite diagnosis of SV had to meet at least one of the following criteria: 1) organisms were cultured from patient brain tissue, dura, and/or CSF samples; 2) the patient showed evidence of intracranial infection in the radiographic examination (eg, abnormal findings on ultrasound, CT scan, MRI, radionuclide brain scan, or arteriogram), surgical operation, or histopathological examination; 3) the patient had typical CSF findings of a glucose concentration <1.9 mmol/L, CSF glucose to blood glucose concentration ratio <0.23, protein level >2.2 g/L, white cell count >2,000 cells/mL, or CSF neutrophil count >1,180 cells/mL, and pleocytosis with predominantly polymorphonuclear cells; and 4) the patient had at least two of the following signs or symptoms without other identifiable cause: headache, dizziness, fever (>38°C), stiff neck, irritability, and altered level of consciousness.3,19–21
Colistin administration was initiated based on microbiological results. IVT colistin was administered in a 5-mL saline solution through a ventriculostomy tube following extraction of 5 mL CSF; thereafter, whole drainage was interrupted for 2 hours. If both EVD and Ommaya reservoir were used for a patient, we typically chose the former route for colistin. We installed the EVD channel on the side of ventricular pus and implanted the Ommaya reservoir in the opposite ventricle; if both ventricles had pus, the latter was typically inserted on the right side of the ventricles. The daily dose of colistin ranged from 50,000 to 100,000 international units (IU). Antimicrobial therapy is considered as competent if it includes at least one valid antibiotic. After receiving the antibiogram results, the treatment regimens were designed to include the following parenterally administered antibiotics: 2 g meropenem every 8 hours, 100 mg tigecycline every 12 hours, 1 g vancomycin every 12 hours, 600 mg amikacin every 24 hours, 3 g cefoperazone/sulbactam every 8 hours, 8 g fosfomycin every 12 hours, 0.6 g linezolid every 12 hours, and 2 g cefepime every 12 hours.
To monitor adverse events related to antibiotic therapy, any changes in clinical signs and symptoms and fluctuation in laboratory results that occurred after initiation of antimicrobial treatment were recorded.
IVT lavage
According to the head imaging results, either the pus side or the side with greater dilation was selected for ventricle entry. A long-tunnel EVD was inserted into the opposite ventricle and aspiration was performed with a 10-mL syringe attached to one terminal. Copious irrigation with colistin solution was carried out until the output was clear. Subsequently, a long-tunnel EVD was inserted into the ventricle with pus for IVT colistin and an Ommaya reservoir was inserted into the opposite ventricle.
Microbiological assays
CSF samples were obtained through an IVT catheter. The hospital’s microbiology laboratory evaluated the antimicrobial susceptibility of isolates by the disk diffusion and microbiological methods. The susceptibility of A. baumannii to colistin was determined by the disk diffusion method, which is widely used for colistin susceptibility testing. However, according to the definition of XDR, it does not affect our research results.13,22
Data collection
Demographic, clinical, radiographic, and laboratory data were collected using a standardized case report form. The information thus collected was added to a database. The following data were extracted: age, sex, admission criteria to NICU and the Department of Neurological Surgery, primary diagnosis, surgeries before infection, time period, and main systemic antibiotics. Data from laboratory findings such as CSF white cell count, CSF glucose, ratio of CSF glucose to blood glucose concentration, and CSF protein level on the day of admission as well as on the first and last days of colistin treatment were also collected.
Follow-up and evaluation of outcome
Treatment outcome was evaluated based on CSF cultures, laboratory findings, colistin toxicity, and complications. Treatment success was defined as recovery of laboratory findings and negative CSF cultures of SV at the end of colistin treatment and during follow-up. Treatment failure was defined as persistence or deterioration of laboratory findings, presentation of symptoms and/or signs of SV during IVT colistin administration, and/or persistence of positive CSF cultures. All patients were followed up for at least 12 months.
Statistical analyses
SPSS v.16.0 software was used for statistical analyses. The results are mainly presented as simple descriptive statistics. Continuous data are expressed as the mean ± standard deviation and categorical data are expressed as the median value (IQR). A paired-point Student’s t-test or the Wilcoxon test was used to compare laboratory findings before IVT initiation and after its discontinuation, with P<0.05 considered as statistically significant.
Results
Pooled data of 25 patients (five women and 20 men) who were treated for SV by IVT colistin were included in the analysis. A total of 16 patients with SV required extracranial drainage; the remaining nine were infected as a result of a poorly healed incision. The mean duration from the last surgery to confirmed infection was 19.3±10.1 days (range: 3–48 days). The basic information of the patients is shown in Table 1.
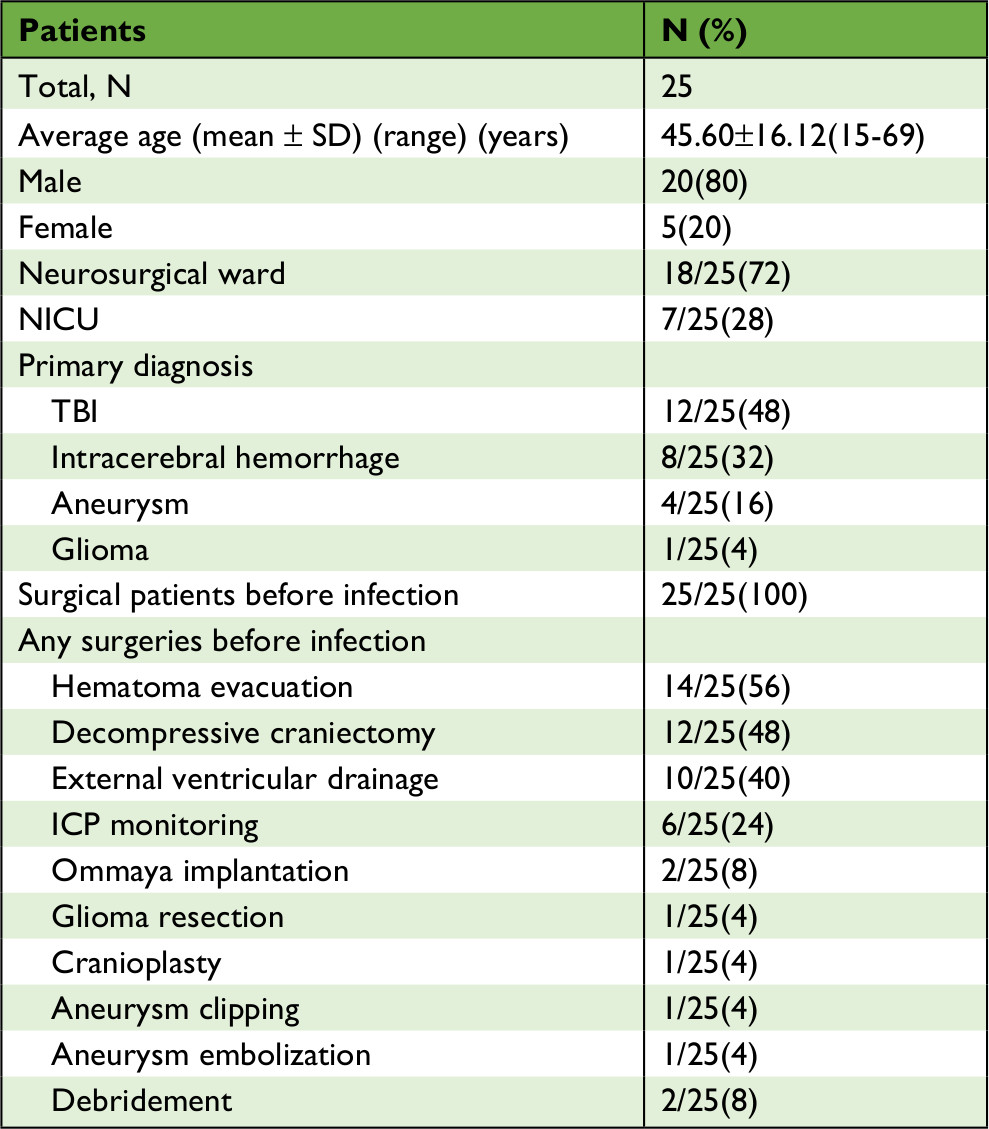 | Table 1 Demographics of the patients Abbreviations: CSF, cerebrospinal fluid; ICP, intracranial pressure; IVT, intraventricular; NICU, neurosurgical intensive care unit; TBI, traumatic brain injury; VP, ventriculoperitoneal. |
All patients underwent operations after diagnosis of SV; 25 (100%) underwent IL, 19 (76%) underwent Ommaya implantation, 18 (72%) underwent lumbar drainage, and 14 (56%) underwent EVD. The 25 patients received treatment with IVT colistin at 100,000 IU once daily, except for one patient who was administered a dose of 50,000 IU once daily; the median colistin dose was 100,000 IU (range: 50,000–100,000 IU) administered once daily. The mean duration of IVT colistin treatment was 13.4±2.8 days (range: 8–23 days). The 25 patients had CSF cultures positive for XDR A. baumannii and received systemic antibiotic treatment, including meropenem-tigecycline (n=7), tigecycline-cefoperazone/sulbactam (n=4), meropenem-vancomycin (n=3), cefoperazone/sulbactam-amikacin (n=2), meropenem-cefoperazone/sulbactam (n=2), tigecycline-cefoperazone/sulbactam-fosfomycin (n=2), cefoperazone/sulbactam-vancomycin (n=1), cefepime-vancomycin (n=1), meropenem-linezolid (n=1), tigecycline-fosfomycin (n=1), and cefoperazone/sulbactam-amikacin (n=1). The mean duration of the systemic antibiotic treatment was 19.2±9.2 days (range: 9–40 days) (Tables 1 and 2).
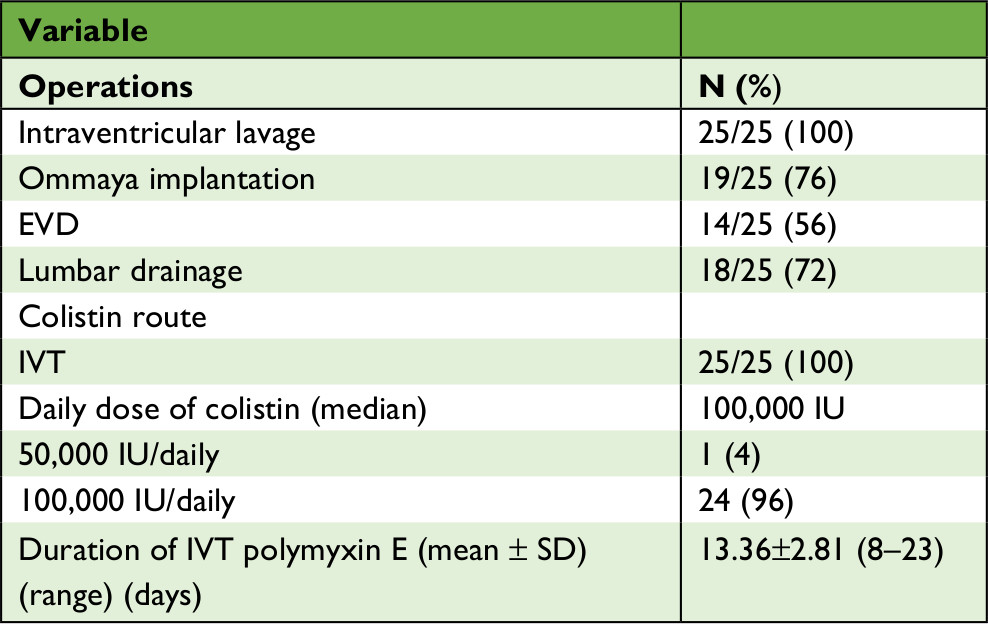 | Table 2 Surgical treatment and local administration of intracranial infection Abbreviations: EVD, external ventricular drainage; IVT, intraventricular; IU, international units. |
Clinical symptoms and CSF laboratory data of patients before and after treatment are shown in Table 3. The mean time from initiation of IVT colistin until a negative CSF culture was obtained was 8.9±4.0 days (range: 3–19 days).
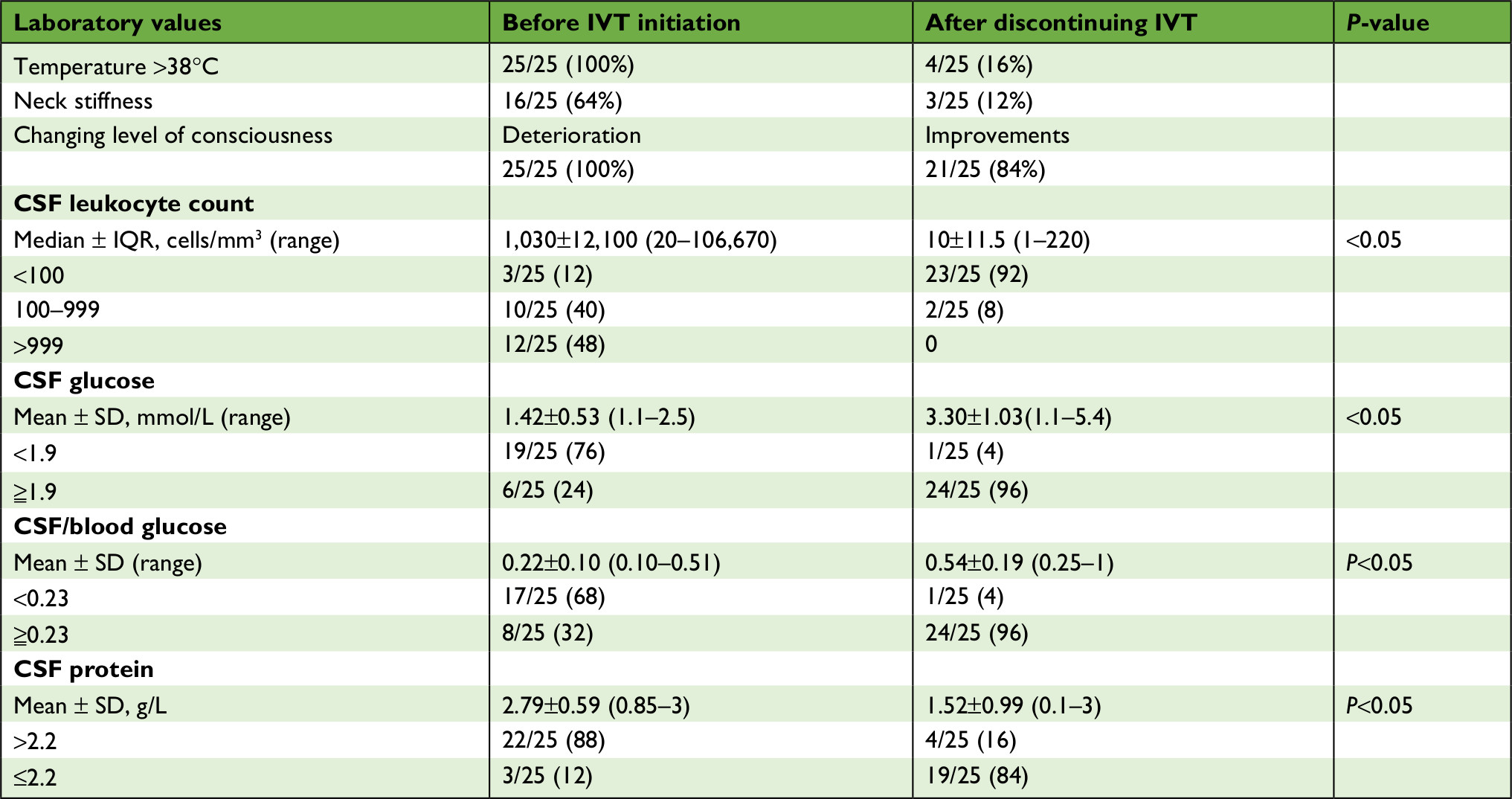 | Table 3 Clinical symptoms and laboratory data in patients Abbreviations: CSF, cerebrospinal fluid; IVT, intraventricular; IQR, interquartile. |
Treatment was successful in 20 patients (80%); five patients died, including one who was re-admitted due to recurrence 1 month after discharge. During treatment and follow-up, 15 patients (60%) presented with hydrocephalus. One (4%) had a relapse without other complications such as epilepsy; 15 experienced hydrocephalus, and eight of these cases underwent surgery for a VP shunt. The time from negative CSF culture to VP shunt surgery was 33.6±20.2 days (range: 10–60 days). The remaining seven patients did not undergo operation for the shunt (Table 4).
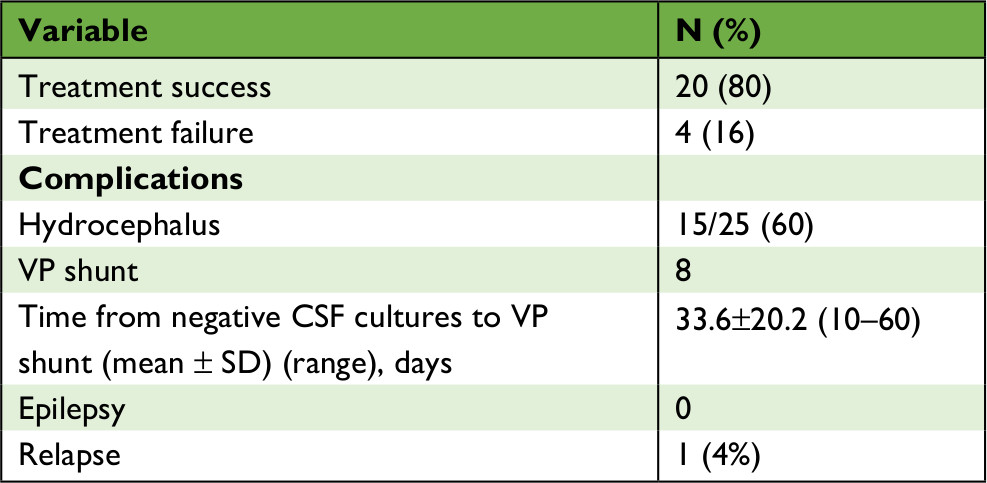 | Table 4 Outcomes and complications Abbreviations: CSF, cerebrospinal fluid; VP, ventriculoperitoneal. |
Discussion
The emergence of XDR A. baumannii over the last several decades has led to a steady increase in the incidence of post-neurosurgical SV, which has been very difficult to manage due to fewer available treatment options.7–10 Colistin is the only drug that is effective against many XDR A. baumannii.11,12,15 Given its poor penetration into CSF, IVT administration has been the major mode of colistin delivery.17,18
Polymyxin was previously administered IV because of its poor ability to cross the blood–brain barrier. IVT is the preferred IV route for colistin, with the dosing scheme ranging from 20,000 IU to 250,000 IU in adults and from 5,000 IU (in infants) to 120,000 IU (divided into two doses) in children.21,23 The duration of IVT/ITH colistin treatment varies significantly from 1 to 9 weeks; the median time required for CSF sterilization is 4 days.24,25 Special equipment connected to the ventricle is required for IVT colistin administration; EVD and Ommaya and lumbar drainage represent important therapeutic advances that are currently used in neurosurgery, although these methods are not sufficient to drain the infected CSF in patients with SV, especially when it contains pus. IL can increase the effectiveness of IVT antibiotics by reducing the infection load and eliminating the nidus of infection, with a success rate of >80%.21,24–28 Our current results are similar to those reported in recent studies.24,25
The efficacy of combining systemic antibiotics with IVT colistin has not been well studied. Given the emergence of antimicrobial resistance, some experimental and clinical studies have examined the role of combination therapy involving polymyxins. The bactericidal activity of polymyxins has been reported to synergize with that of glycopeptides, cefoperazone/sulbactam, amikacin, fosfomycin, trimethoprim-sulfamethoxazole, ciprofloxacin, and tigecycline.29–31 Another commonly used therapeutic strategy is the combination of systemic and IVT polymyxins, which has produced favorable clinical outcomes.24,25
In our study, all patients received systemic antimicrobial agents targeting Gram-negative bacteria in combination with colistin, cefoperazone/sulbactam, amikacin, tigecycline, vancomycin, linezolid, cefepime, fosfomycin, and meropenem, despite reported resistance to these agents. The mean duration of systemic antibiotic treatment was 19.2±9.2 (range: 9–40) days. The effect of the combination treatment was unclear, although the possibility of a beneficial effect cannot be excluded.32
SV has typical neurological manifestations such as neck stiffness and fever. In our study, 100% of patients had fever and showed deterioration of Glasgow Coma Scale score, 64% had neck stiffness, 88% had abnormal CSF white cell counts, 76% had abnormal CSF glucose concentration, 68% had abnormal CSF/blood glucose concentration ratio, and 88% had abnormal CSF protein levels before treatment. After treatment, 84% of patients had no fever, 88% showed no neck stiffness, and 84% showed an improved level of consciousness, which was considered as a clinical response. Regarding laboratory findings, 92% of patients had normal CSF white cell counts, 96% had normal CSF glucose concentration and CSF/blood glucose concentration ratio, 84% had normal CSF protein level, and the treatment success rate was 84%. A review of 81 cases of multidrug-resistant and XDR A. baumannii SV treated with IVT colistin revealed that 89% (72/81) of patients showed improved clinical and bacteriological results.25 Another study of 34 patients found that four had ventriculitis and the others had only meningitis without ventriculitis, with an overall cure rate of 83% (28/34).33 Our findings are in agreement with these reports.
IVT administration of colistin was previously considered to be toxic. The main forms of toxicity observed during this therapy included increased signs of meningeal irritation and seizure, which were associated with inappropriate dosing and were reversible.24,25,34 Relapse of existing infection, re-infection with a new microbe as a result of numerous operations, and a chemical reaction are possible factors that can lead to a differential diagnosis.25 In one of the largest reviews of the use of IVT colistin in neurosurgical patients, successful clinical and bacteriological outcomes were achieved in 89% (72/81) of A. baumannii SV cases treated with IVT or ITH colistin, and the two recorded relapses were ultimately cured with colistin.25 In our study, one (4%) patient experienced a relapse at 40 days after the discontinuation of IVT colistin and no patients presented with epilepsy.
Few experimental or clinical studies are found in the literature on managing hydrocephalus after cured SV. Based on our clinical experience, when hydrocephalus appeared in cured patients, we tested the patients’ CSF at an interval of 2–3 days and at least for three times. If CSF laboratory data were normal for more than three times and during this period if the patients had no other abnormal clinical manifestations (eg, fever >38°C), patients underwent a VP shunt according to the indication of hydrocephalus. In our study, 60% (15/25) of the patients had hydrocephalus, eight underwent surgery for a VP shunt, and the time from a negative CSF culture to the shunt was 33.6±20.2 days, with a minimum time interval of 10 days. The remaining seven patients did not undergo the shunt operation as they did not have clear surgical indications; they instead went directly to the rehabilitation hospital for therapy. Follow-up cranial CT was performed to monitor hydrocephalus progression.
Conclusion
We determined that IVT lavage and external CSF drainage combined with IVT colistin is an effective treatment strategy for patients with SV due to XDR A. baumannii. The clinical results showed a success rate of up to 80%. We also observed that there were few complications associated with this treatment; in particular, there was no toxicity related to IVT colistin. Thus, IL and external CSF drainage combined with IVT colistin is a relatively safe and effective therapeutic strategy in cases of SV due to XDR A. baumannii, although these findings require confirmation in a large-scale study.
Acknowledgment
We acknowledge the support received from Health and Family Planning Commission of Shanghai (No. 03.02.16.001).
Disclosure
The authors report no conflicts of interest in this work.
References
Martin C, Thomachot L, Albanèse J. Iatrogenic and traumatic cerebro-meningeal infections. Rev Prat. 1994;44(16):2207–2212. | ||
Eljamel MS. Antibiotic prophylaxis in unrepaired CSF fistulae. Br J Neurosurg. 1993;7(5):501–505. | ||
Durand ML, Calderwood SB, Weber DJ, et al. Acute bacterial meningitis in adults. A review of 493 episodes. N Engl J Med. 1993;328(1):21–28. | ||
Buckwold FJ, Hand R, Hansebout RR. Hospital-acquired bacterial meningitis in neurosurgical patients. J Neurosurg. 1977;46(4):494–500. | ||
Lai WA, Lu CH, Chang WN. Mixed infection in adult post-neurosurgical bacterial meningitis: a hospital-based study. Biomed J. 2013;36(6):295–303. | ||
Munoz-Price LS, Weinstein RA. Acinetobacter infection. N Engl J Med. 2008;358(12):1271–1281. | ||
Gordon NC, Wareham DW. Multidrug-resistant Acinetobacter baumannii: mechanisms of virulence and resistance. Int J Antimicrob Agents. 2010;35(3):219–226. | ||
Maragakis LL, Perl TM. Acinetobacter baumannii: epidemiology, antimicrobial resistance, and treatment options. Clin Infect Dis. 2008;46(8):1254–1263. | ||
Fournier PE, Richet H. The epidemiology and control of Acinetobacter baumannii in health care facilities. Clin Infect Dis. 2006;42(5):692–699. | ||
Jawad A, Heritage J, Snelling AM, Gascoyne-Binzi DM, Hawkey PM. Influence of relative humidity and suspending menstrua on survival of Acinetobacter spp. on dry surfaces. J Clin Microbiol. 1996;34(12):2881–2887. | ||
O’Neill E, Humphreys H, Phillips J, Smyth EG. Third-generation cephalosporin resistance among Gram-negative bacilli causing meningitis in neurosurgical patients: significant challenges in ensuring effective antibiotic therapy. J Antimicrob Chemother. 2006;57(2):356–359. | ||
Karageorgopoulos DE, Falagas ME. Current control and treatment of multidrug-resistant Acinetobacter baumannii infections. Lancet Infect Dis. 2008;8(12):751–762. | ||
Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. | ||
Paterson DL, Doi Y. A step closer to extreme drug resistance (XDR) in gram-negative bacilli. Clin Infect Dis. 2007;45(9):1179–1181. | ||
Giamarellou H, Antoniadou A, Kanellakopoulou K. Acinetobacter baumannii: a universal threat to public health? Int J Antimicrob Agents. 2008;32(2):106–119. | ||
Giamarellou H, Poulakou G. Multidrug-resistant Gram-negative infections: what are the treatment options? Drugs. 2009;69(14):1879–1901. | ||
Markantonis SL, Markou N, Fousteri M, et al. Penetration of colistin into cerebrospinal fluid. Antimicrob Agents Chemother. 2009;53(11):4907–4910. | ||
Antachopoulos C, Karvanen M, Iosifidis E, et al. Serum and cerebrospinal fluid levels of colistin in pediatric patients. Antimicrob Agents Chemother. 2010;54(9):3985–3987. | ||
Spanos A, Harrell FE, Durack DT. Differential diagnosis of acute meningitis. An analysis of the predictive value of initial observations. JAMA. 1989;262(19):2700–2707. | ||
Sigurdardóttir B, Björnsson OM, Jónsdóttir KE, Erlendsdóttir H, Gudmundsson S. Acute bacterial meningitis in adults. A 20-year overview. Arch Intern Med. 1997;157(4):425–430. | ||
Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 Infectious diseases society of America’s clinical practice guidelines for healthcare-associated ventriculitis and meningitis*. Clin Infect Dis. 2017;64(6):701–706. | ||
Humphries RM. Susceptibility testing of the polymyxins: where are we now? Pharmacotherapy. 2015;35(1):22–27. | ||
Swift PN, Bushby SR. Haemophilus influenza meningitis treated with polymyxin. Lancet. 1951;2(6675):183–190. | ||
Falagas ME, Bliziotis IA, Tam VH. Intraventricular or intrathecal use of polymyxins in patients with Gram-negative meningitis: a systematic review of the available evidence. Int J Antimicrob Agents. 2007;29(1):9–25. | ||
Karaiskos I, Galani L, Baziaka F, Giamarellou H. Intraventricular and intrathecal colistin as the last therapeutic resort for the treatment of multidrug-resistant and extensively drug-resistant Acinetobacter baumannii ventriculitis and meningitis: a literature review. Int J Antimicrob Agents. 2013;41(6):499–508. | ||
Beer R, Lackner P, Pfausler B, Schmutzhard E. Nosocomial ventriculitis and meningitis in neurocritical care patients. J Neurol. 2008;255(11):1617–1624. | ||
Laxmi S, Tunkel AR. Healthcare-associated bacterial meningitis. Curr Infect Dis Rep. 2011;13(4):367–373. | ||
Wada T, Kuroda K, Yoshida Y, et al. A case of posttraumatic severe ventriculitis treated by intraventricular lavage. No Shinkei Geka. 2000;28(8):737–743. | ||
Dizbay M, Tozlu DK, Cirak MY, Isik Y, Ozdemir K, Arman D. In vitro synergistic activity of tigecycline and colistin against XDR-Acinetobacter baumannii. J Antibiot. 2010;63(2):51–53. | ||
Berlana D, Llop JM, Fort E, Badia MB, Jódar R. Use of colistin in the treatment of multiple-drug-resistant gram-negative infections. Am J Health Syst Pharm. 2005;62(1):39–47. | ||
Viehman JA, Nguyen MH, Doi Y. Treatment options for carbapenem-resistant and extensively drug-resistant Acinetobacter baumannii infections. Drugs. 2014;74(12):1315–1333. | ||
Rynn C, Wootton M, Bowker KE, Alan Holt H, Reeves DS. In vitro assessment of colistin’s antipseudomonal antimicrobial interactions with other antibiotics. Clin Microbiol Infect. 1999;5(1):32–36. | ||
Remeš F, Tomáš R, Jindrák V, Vaniš V, Setlík M. Intraventricular and lumbar intrathecal administration of antibiotics in postneurosurgical patients with meningitis and/or ventriculitis in a serious clinical state. J Neurosurg. 2013;119(6):1596–1602. | ||
Wise BL, Mathis JL, Jawetz E. Infections of the central nervous system due to pseudomonas aeruginosa. J Neurosurg. 1969;31(4):432–434. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.