")
Back to Journals » International Journal of General Medicine » Volume 14
Treatment of May–Thurner’s Syndrome and Associated Complications: A Multicenter Experience
Authors Sigua-Arce P, Mando R , Spencer L, Halalau A
Received 20 June 2021
Accepted for publication 2 August 2021
Published 20 August 2021 Volume 2021:14 Pages 4705—4710
DOI https://doi.org/10.2147/IJGM.S325231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Priscilla Sigua-Arce,1 Ramy Mando,1 Lisa Spencer,2 Alexandra Halalau1,2
1Department of Internal Medicine, Beaumont Health System, Royal Oak, MI, USA; 2Oakland University William Beaumont School of Medicine, Rochester Hills, MI, USA
Correspondence: Alexandra Halalau Email [email protected]
Objective: To assess the treatment options and associated complications in patients with May–Thurner’s syndrome (MTS).
Methods: We retrospectively reviewed the charts of patients diagnosed with MTS. Thorough review was completed and data relevant to methods of diagnosis, treatment, complications, hospital readmission, and mortality were extracted from patient charts. The patients were followed for two years after diagnosis.
Results: Of the 47 patients identified as having “MTS”, 32 (70%) were diagnosed formally with either magnetic resonance venography, computed tomography venography, or ultrasound. Two patients were excluded for insufficient availability of follow-up records. Mean age of the population included (N = 30) was 50.24 ± 15.33 years and 83% (N = 25) had female gender. The majority (40%) of patients were treated with anticoagulation, thrombolysis, and stent placement, and 13.3% received a combination of anticoagulation, antiplatelet agent, thrombolysis, and stent placement. Overall, we found 28 patients (93%) who underwent endovascular stenting. However, 39.3% (11/28) had stent-related complications that included stent thrombosis, stenosis, and migration. One patient underwent open heart surgery for stent retrieval. Duration of anticoagulation therapy ranged from 6 months to lifelong. Two patients (6.7%) suffered major bleeds requiring transfusion. Fourteen patients (46.6%) developed post-thrombotic syndrome. Seven (23.3%) patients required MTS-related readmission within 30 days. No mortality was noted at two-year follow-up.
Conclusion: Although our study only included 30 patients, it was evident to us that there is no consensus in the management of MTS. Furthermore, endovascular stenting, which has a major role in the management of MTS, has complication rates that hover close to 40%. Further research is needed to help develop a standardized evidence-based approach in the management of MTS that ensures a decreased risk of immediate and long-term complications.
Keywords: May–Thurner syndrome, treatment, complications, diagnosis, anticoagulation
Introduction
May–Thurner syndrome (MTS) was first described in 1908; however, it was not completely understood until mid-1900s.1 It is defined as a compression of the left iliac vein by the right common iliac artery against the lumbar spine resulting in an iliac vein or iliofemoral venous thrombosis.2 Deep venous thrombosis (DVT) secondary to MTS constitutes 2% to 3% of all lower extremity DVT.3 It is currently believed that the low occurrence rate is likely underestimated due to missed diagnoses4 as there are more recognized risk factors for DVT such as oral contraceptives, recent pregnancy or prolonged travel5 that are taken as culprits for the presence of DVT. It typically occurs in women ranging from 20 years old to 40 years old.6
Patients with MTS usually present with left lower extremity DVT, and/or symptoms of swelling, pain, claudication, ulcerations, varicose veins, and pelvic congestion syndrome.6,7 Three different clinical stages based on the presence of asymptomatic compression, spur formation within the vessel and presence of thrombosis have been described by Kim et al.
Diagnosis requires a high index of suspicion; tests include duplex ultrasound (DUS), computed tomography venography (CTV), magnetic resonance venography (MRV), catheter-based venography, and intravascular ultrasound (IVUS).8 For definitive diagnosis of MTS, stenosis of left common iliac vein should be proved. In case of acute DVT, the lesion is obscured by overlying thrombus, in which case the thrombus should first be removed. In the absence of thrombus, noninvasive vascular imaging such as CTV/MRV or DUS can be used; among invasive diagnostic methods, IVUS is probably the method of choice.7 There are several modalities of treatment for MTS, including catheter directed thrombolysis with or without stent placement, balloon angioplasty with or without stent placement, pharmacomechanical catheter directed thrombolysis with stent placement and anticoagulation. These are treatment options that have been pursued and studied in several randomized clinical trials as well as retrospective studies advocating for catheter directed thrombolysis and pharmacomechanical interventions with stent placement3,9–12 while other studies have shown no difference in terms of post-thrombotic syndrome (PTS) when compared to anticoagulation.13 The cause of MTS is the stenotic lesion, which cannot be treated with anticoagulation nor thrombolysis; these treatment options are reserved for patients with MTS who suffered acute DVT.
At this point, there is no consensus or guidelines for the management of MTS.14 Given the multiple approaches that exist for MTS treatment and the lack of clear recommendations, we evaluated the treatment modalities that patients with this pathology received in our health system as well as the outcomes related to the interventions to determine if there were variations in treatment and outcomes.
Methods
Permission was granted by the Institutional Review Board. A retrospective chart review of patients with a diagnosis of MTS across all eight hospitals within Beaumont Health (BH) from 11/2009 to 11/2017 was done. BH is considered the largest health system in Southeast Michigan. Patients were identified by using the International Statistical Classification of Disease and Related Health Problems (ICD 9) code for MTS. For patients to be included, they had to have MTS confirmed by any imaging modality, intervention reported and at least two-year follow-up; if these were not present, patients were excluded. Once identified, each chart was reviewed to find imaging tests that would support the diagnosis of MTS, which included venography, computed tomography angiography, magnetic resonance venography, or venous duplex ultrasound. Demographic characteristics such as age and sex were collected. Risk factors such as obesity, smoking, oral contraceptive use, prior history of DVT, and pulmonary embolism (PE) were identified. Signs and symptoms that led to the eventual diagnosis of MTS were determined by chart review and included shortness of breath, pain, and edema of the left and/or right lower extremity. Outcomes of interest were choice of management, treatment duration, treatment-related complications, frequency of PTS, major bleed (intracranial, retroperitoneal bleeding or need for transfusion), 30-day readmission and mortality.
Results
Forty-seven patients with MTS diagnosis by ICD 9 code were identified. Thirty-two (68%) patients were formally diagnosed with computed tomography venography, magnetic resonance venography, or venous duplex ultrasound. Two patients were excluded as there was insufficient availability of follow-up records. Mean age of the population included (N = 30) was 50.24 ±15.33 years, and 83% (N = 25) had female gender; obesity was reported in 40% of patients, smoking was present in one-third of patients, a prior history of DVT or PE was present in 37% of patients. All the patients included had an initial presentation of pain or edema of the left lower extremity that led to the diagnosis of MTS (Table 1Table 2).
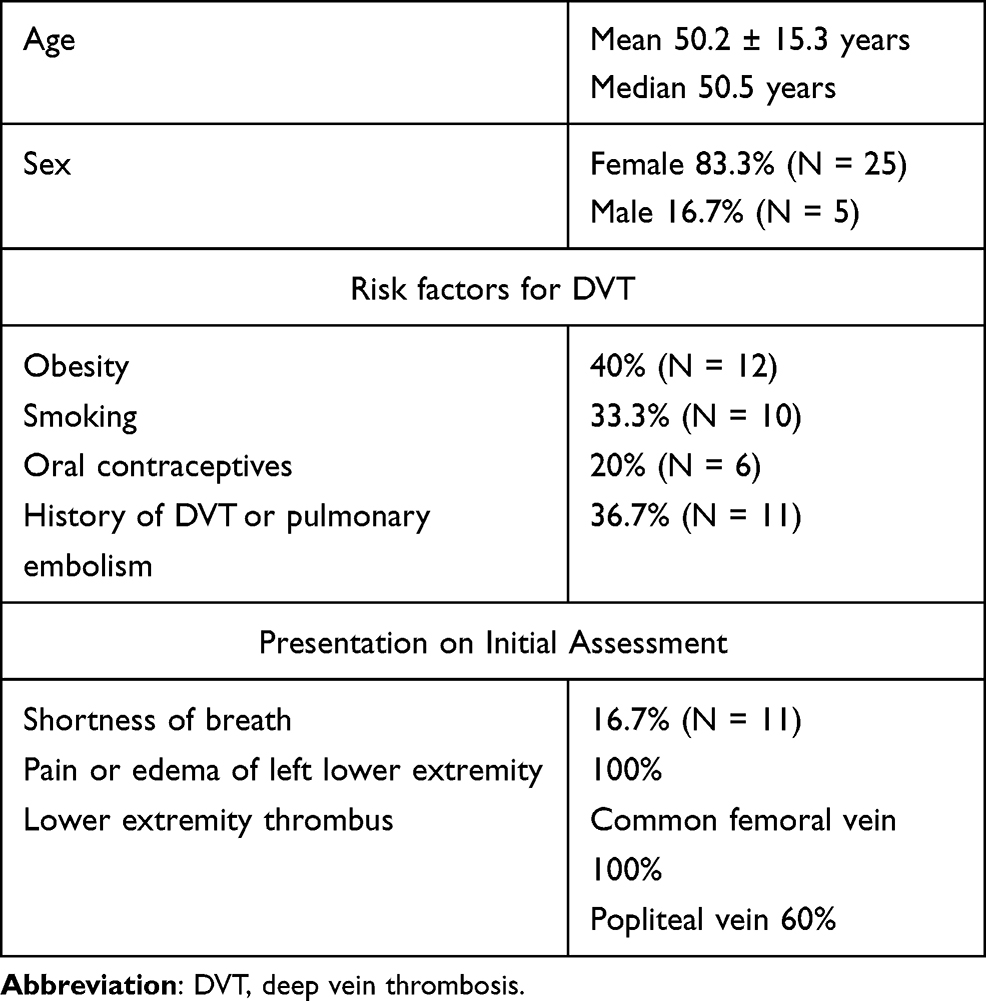 |
Table 1 Demographics of Patients Included in the Study |
There were ten different treatment combinations that were pursued which included anticoagulation, antiplatelet therapy, thrombolysis, and stent placement. The majority (40%) of patients’ treatment consisted of anticoagulation (either with warfarin or non-vitamin K oral).
Twenty-eight (93%) patients underwent endovascular stenting with 39.2% (11/28) having stent-related complications that included stent thrombosis, stenosis, and migration (Table 3). One patient underwent open heart surgery for stent retrieval. Of the 28 patients that received a stent as part of their treatment, 75% (21/28) had surveillance studies, 9 had complications that were detected on follow-up. Duration of anticoagulation therapy ranged from 6 months to lifelong; 7 patients remained on anticoagulation indefinitely while 6 were placed on anticoagulation and aspirin indefinitely. Two patients suffered major bleeds requiring transfusion. Fourteen patients (46.6%) developed PTS, with the group that combined anticoagulation, thrombolysis, and stent placement having 4 cases while the groups that combined triple therapy with stent placement and anticoagulation with stent placement had 2 cases each; the rest of the treatment groups had one case each. Seven (23.3%) patients required MTS-related readmission within 30 days. No mortality was noted at two-year follow-up. Twenty out of 30 patients underwent hypercoagulable work-up with 10 patients (50%) having a hypercoagulable state; 5 patients had factor V Leiden, 3 of them were heterozygous while the remaining 2 were not specified.
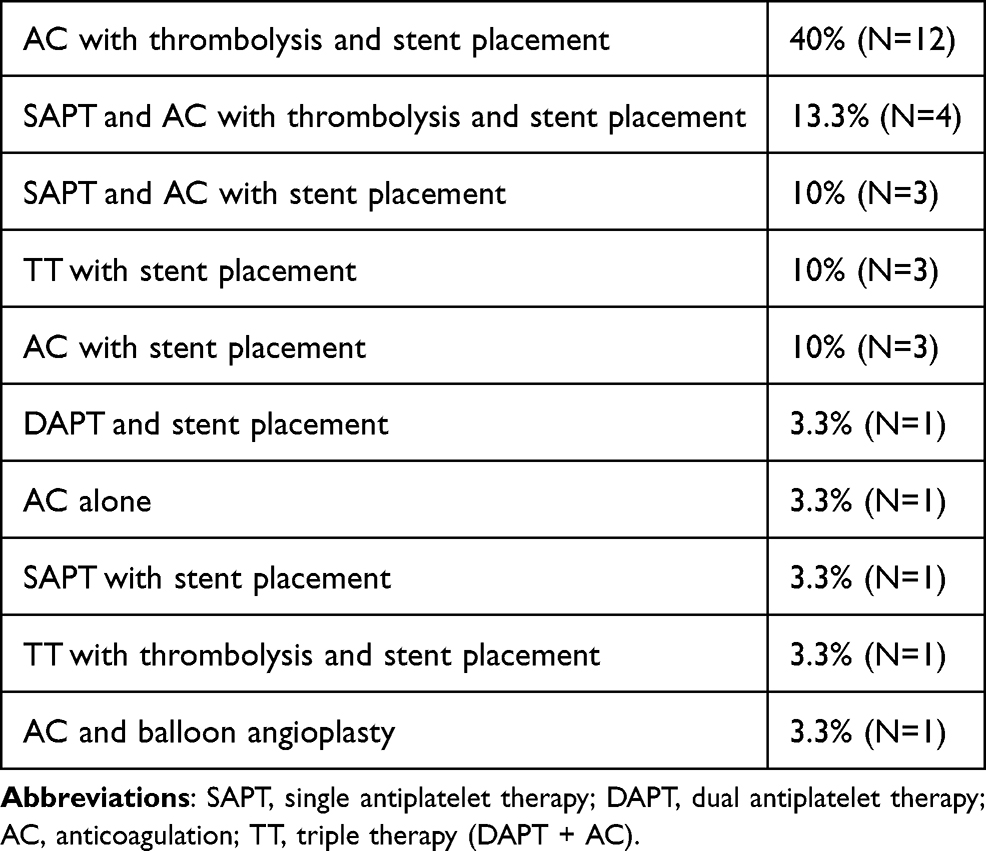 |
Table 2 Summary of Regimens in the Management of MTS |
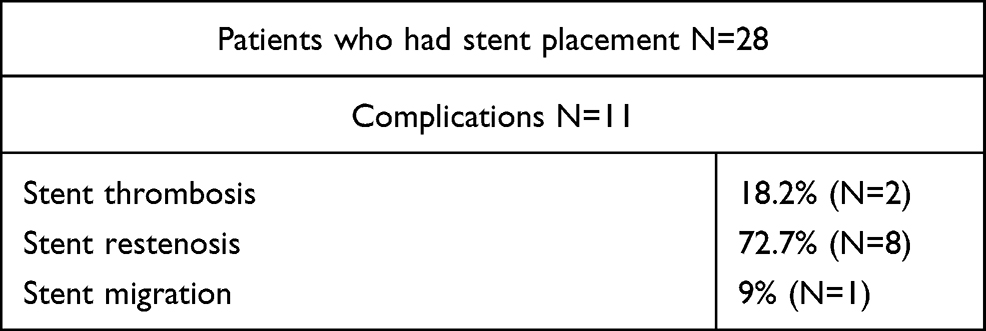 |
Table 3 Stent-Related Complications |
Discussion
Our study shows the wide array of treatments for MTS used in our institution. The most common management included anticoagulation (with warfarin or NOACs), thrombolysis, and stent placement. Several other combinations were noted as well. There was a high rate of stent complications as 40% of patients had stent thrombosis, stenosis, and migration with one patient requiring open heart surgery for stent retrieval; this last complication has been rare however previously reported.15 Major bleeding, which included intracranial, retroperitoneal, and/or need for transfusion, was also reported in two cases. This data highlights the need for consensus in the management of MTS as well as the importance of assessing the risks associated with each intervention. Management of MTS should be undertaken only after consideration of factors such as the clinical context in which the lesion was discovered, the likelihood that it explains the patient’s symptoms, the level of clinical severity of venous disease and the patient’s life expectancy, comorbidities and personal preferences.16
Symptoms associated with MTS include acute lower extremity DVT, lower extremity edema, venous claudication, chronic venous insufficiency, and PE; in our study, all the patients presented with pain and/or edema of the left lower extremity. Risk factors for MTS include female gender, use of oral contraceptive medication, history of multiparity, and hypercoagulable disorders.17–20 In our study, 83% of patients were female with 37% having a prior history of DVT or PE, with one-third of patients reporting tobacco use, which highlights how prevalent common risk factors for thrombosis are. Hypercoagulable states should always be assessed to identify risk factors for DVT,21 as 67% of patients with chronic iliac vein occlusion or MTS have some form of thrombophilia.22 In our study, two-thirds of patients underwent hypercoagulable work-up, with 50% having a positive result of which 5 patients had factor V Leiden, 3 of them were heterozygous.
Currently, there is no expert consensus or guidelines available to help direct the management of MTS. To exemplify this, the venous thromboembolism disease guidelines recommend against the routinely use of thrombolytic therapy for acute DVT management,23,24 however, MTS is not separately considered. Therapeutic options previously described in the literature include endovenous treatment with balloon angioplasty, endovascular stenting, catheter-directed thrombolysis, pharmacomechanical thrombolysis and surgical exploration of the lesion with thrombectomy and decompression of the vein.25 Several retrospective reviews have supported the use of minimally invasive techniques as they provide symptomatic improvement with a good safety profile.26,27 PTS is factored when it comes to treatment options as its incidence in patients with iliofemoral venous thrombosis is around 50% to 70%28 and it can cause chronic limb pain and swelling and can progress to cause major disability, leg ulcers and impaired quality of life.28–30 Angioplasty without subsequent stent placement has been demonstrated to have low patency rates.31 A 73% recurrence rate was noted in patients with acute left-sided ilio-femoral DVT when the underlying obstruction was not treated with a stent.32
Angioplasty and stent placement have gained popularity in recent decades with 79% to 100% primary patency rates 1 to 2 years after treatment.33 Compared with anticoagulation therapy, catheter-directed thrombolysis can more effectively remove the thrombus and improve symptoms.34 A prospective randomized controlled trial, CAVENT, showed that patients with ileo-femoral DVT treated with catheter-directed therapy and anticoagulation had less incidence of PTS when compared with anticoagulation alone with an absolute risk reduction of 14.4%.35 Among endovascular physicians, the consensus seems to be that failure to treat a known iliac vein obstructive lesion in a patient that will undergo catheter-directed thrombolysis for DVT would place the patient at a high risk for re-thrombosis.16 Catheter-directed thrombolysis with stent placement has become a preferred therapy in the setting of acute iliofemoral venous thrombosis. Three randomized controlled trials that evaluated the use of catheter-directed thrombolysis in conjunction with stent placement and anticoagulation for the treatment of extensive DVT showed that the combined use of these strategies was associated with better outcomes for prevention of PTS and valvular reflux when compared to anticoagulation alone.11,36–39 A large multicenter trial, ATTRACT trial, that assessed the use of anticoagulation alone versus anticoagulation and pharmacomechanical catheter-directed thrombolysis for the treatment of ilio-femoral and femoral popliteal DVT supported the use of anticoagulation alone as catheter-directed thrombolysis did not reduce the incidence of PTS and was associated with increased risk of bleeding; however, it did acknowledge that the severity of PTS was significantly lower in the group that received catheter-directed thrombolysis.14 An exploratory analysis of the ilio-femoral subpopulation from the ATTRACT trial showed no difference in the development of PTS and bleeding risk, however, pharmacomechanical catheter-directed thrombolysis showed reduced occurrence of moderate or severe PTS and quality of life when compared with anticoagulation alone.40 In our study, 46% (14/30) developed PTS; the group with the lowest percentage of PTS (33%) was the one that combined thrombolysis with stent placement and anticoagulation; 66% was reported in those who had triple therapy with stent placement as well as in those who had stent placement with anticoagulation; the rest of treatment combinations had one case each; however, for most of these groups this would be a 100% incidence; the group that included triple therapy with thrombolysis with stent placement and anticoagulation did not report PTS. It is important to acknowledge that the Villalta scale, which stratifies the severity of PTS based on clinical signs and patient symptoms (mild 5 to 9 points, moderate 10 to 14 points and severe >15 points),41 was not reported for most of the patients; this would make it difficult to assess how significant this finding was in each group. Stents were used in eight out of ten treatment combinations with almost 40% of patients having complications. Stents have shown to reduce PTS; studies such as CAVENT and ATTRACT, in which stents play a limited role, might indicate that they can be used but with discretion and careful case by case analysis. This exemplifies why guidelines and expert consensus are needed.
In terms of stent complications, stent restenosis was reported in 72.7% of patients with MTS that had stent placed. The restenosis rate is quite high when compared with Neglén et al that reported a cumulative rate of severe in-stent restenosis (ISR) (<50%) in 5% of limbs at 72 months.42 We can hypothesize that given the fact that MTS diagnosis is quite rare, the vascular surgeons’ skills and knowledge in stent placement in patients with MTS can be quite variable.
Duration of anticoagulation in patients with MTS and acute DVT is not clearly established. Current guidelines for the management of DVT favor at least 3 months of anticoagulation therapy, however, the studies included in this recommendation do not factor MTS.23,24 Furthermore, there are no comparative studies to establish the optimal type, target range, or duration of anticoagulation therapy following endovascular therapy for DVT.16 The consensus among endovascular physicians is to use anticoagulation for at least 6 months after stent placement.43 In our study, 13 out of 30 patients were on anticoagulation indefinitely; 7 out of those 13 where on anticoagulation alone while 6 were on anticoagulation and aspirin. It was not taken into account if the patients required these medications for other indications.
Limitations
This study has several limitations including the fact that this was a retrospective chart review of patients in a single health system with a low sample size. Villalta scale was not reported for most of the patients which makes assessing the severity of PTS challenging. For patients on anticoagulation alone or in combination with aspirin that might have had concomitant indications, there was no further evaluation of such indications.
Conclusions
Further research is needed to establish the best treatment approach for MTS as multiple studies have shown conflicting recommendations. Guidelines to help direct therapy for these patients are needed, as our study showed, ten different approaches were used when dealing with this pathology.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval
The study was approved by the Beaumont Health Institutional Review Board. The study was approved under expedited review and the patient consent was waived as the study design was retrospective. The data confidentiality and compliance with the Declaration of Helsinki was maintained.
Acknowledgments
The abstract from this manuscript was presented at the 2019 Michigan Chapter American College of Physicians.
Funding
This research did not receive any specific funding.
Disclosure
The authors have no conflicts of interest regarding this work or the publication of this paper.
References
1. May R, Thurner J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology. 1957;8:419–427.
2. Virchow R. Uber die Erweinterung kleiner Gafassee. Arch Path Anat. 1851;3:427.
3. O’Sullivan GJ, Semba CP, Bittner CA, et al. Endovascular management of iliac vein compression (May-Thurner) syndrome. J Vasc Interv Radiol. 2000;11:823–836.
4. Thijs W, Rabe KF, Rosendaal FR, Middeldorp S. Predominance of left-sided deep vein thrombosis and body weight. J Thromb Haemost. 2010;8:2083–2084.
5. Peters M, Syed RK, Katz M, et al. May-Thurner syndrome: a not so uncommon cause of a common condition. Proc (Bayl Univ Med Cent). 2012;25:231–233.
6. Kim DOD, Porter DH. Venography anatomy, technique and interpretation. In: Kim DOD, editor. Peripheral Vascular Imaging and Intervention. Saint Louis, MO: Mosby-Year Book; 1992:269–349.
7. Knuttinen MG, Naidu S, Oklu R, et al. May-Thurner: diagnosis and endovascular management. Cardiovasc Diagn Ther. 2017;7:S159–S164.
8. Suwanabol PA, Tefera G, Schwarze ML. Syndromes associated with the deep veins: phlegmasia cerulean dolens, May-Thurner syndrome, and nutcracker syndrome. Perspect Vasc Surg Endovasc Ther. 2010;22:223–230.
9. Watson L, Broderick C, Armon MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev. 2016;11(11):CD002783.
10. Sharifi M, Medhipour M, Bay C, Smith G, Sharifi J. Endovenous therapy for deep venous thrombosis: the TORPEDO trial. Catheter Cardiovasc Interv. 2010;76:316–325.
11. Sharifi M, Bay C, Medhipour M, et al. Thrombus obliteration by rapid percutaneous endovenous intervention in deep venous occlusion (TORPEDO) trial: midterm results. J Endovasc Ther. 2012;19:273–280.
12. Titus JM, Moise MA, Bena J, Lyden SP, Clair DG. Iliofemoral stenting for venous occlusive disease. J Vasc Surg. 2011;53:1138–1144.
13. Vedantham S, Goldhaber SZ, Julian JA, et al. Pharmacomechanical catheter-directed thrombolysis for deep-vein thrombosis. N Engl J Med. 2017;377:2240–2252.
14. Mando R, Sigua-Arce P, Spencer L, Halalau A. Slippery stents: a case report and review of literature describing patients with May-Thurner syndrome that experienced stent migration. Case Rep Vasc Med. 2019;2019:7606727.
15. Elmahdy S, Shults CC, Moustafa MA. An unusual case of acute heart failure: a case report of iliocaval venous stent migration. J Investig Med High Impact Case Rep. 2018;6:1–3.
16. Birn J, Vedantham S. May-Thurner syndrome and other obstructive iliac vein lesions: meaning, myth, and mystery. Vasc Med. 2015;20:74–83.
17. Marston W, Fish D, Unger J, Keagy B. Incidence of and risk factors for iliocaval venous obstruction in patients with active or healed venous leg ulcers. J Vasc Surg. 2011;53:1303–1308.
18. Kibbe MR, Ujiki M, Goodwin AL, Eskandari M, Yao J, Matsumura J. Iliac vein compression in an asymptomatic patient population. J Vasc Surg. 2004;39:937–943.
19. Murphy EH, Davis CM, Journeycake JM, DeMuth RP, Arko FR. Symptomatic ileofemoral DVT after onset of oral contraceptive use in women with previously undiagnosed May-Thurner Syndrome. J Vasc Surg. 2009;49:697–703.
20. Oteros Fernandez R, Bravo Rodriguez F, Delgado Acosta F, Gonzalez Barrios I. [May-Thurner syndrome and surgery for scoliosis]. Radiologia. 2008;50:245–247. Portuguese
21. Kalu S, Shah P, Natarajan A, Nwankwo N, Mustafa U, Hussain N. May-Thurner syndrome: a case report and review of the literature. Case Re Vasc Med. 2013;2013:740182.
22. Kolber T, Lindh M, Akesson M, Wasselius J, Gottsater A, Ivancev K. Chronic iliac vein occlusion: midterm results of endovascular recanalization. J Endovasc Ther. 2009;16:483–491.
23. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease CHEST guideline and expert panel report. Chest. 2016;149:315–352.
24. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease. Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;14:e419S–e494S.
25. White JM, Comerota AJ. Venous compression syndromes. Vasc Endovasc Surg. 2017;5:155–168.
26. Mousa AY, Broce M, Yacoub M, AbuRahma AF. Iliac vein interrogation augments venous ulcer healing in patients who have failed standard compression therapy along with pathological venous closure. Ann Vas Surg. 2016;34:144–151.
27. Raju S, Davis M. Relative importance of iliac vein obstruction in patients with post-thrombotic femoral vein occlusion. J Vasc Surg Venous Lymphat Disord. 2014;2:107.
28. Delis KT, Bountouroglou D, Mansfield AO. Venous claudication in iliofemoral thrombosis: long-term effects on venous hemodynamics, clinical status, and quality of life. Ann Surg. 2004;239:118–126.
29. Kahn SR, Shbaklo H, Lamping DL, et al. Determinants of health-related quality of life during 2 years following dee vein thrombosis. J Thromb Haemost. 2008;6:1105–1112.
30. Watson L, Broderick C, Armon MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev. 2016;11:CD002783.
31. Roy M, Sasson M, Rosales-Velderrain A, Moon S, Grove M, King T. Pharmacomechanical thrombolysis for deep vein thrombosis in may-thurner syndrome. Innovations. 2017;12:466–471.
32. Mickley V, Schwagierek R, Rillinger N, et al. Left iliac venous thrombosis caused by venous spur: treatment with thrombectomy and stent implantation. J Vasc Surg. 1998;28:492–497.
33. Oguzkurt L, Tercan F, Ozkan U, Gulcan O. Iliac vein compression syndrome: outcome of endovascular treatment with long-term follow-up. Eur J Radiol. 2008;68:487–492.
34. Zhang X, Shi X, Gao P, et al. Endovascular management of May-Thurner syndrome. Medicine. 2016;95:4.
35. Enden T, Haig Y, Kløw NE, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. 2012;379:31–38.
36. Sharifi M, Bay C, Medhipour M, et al. Thrombus obliteration by rapid percutaneous endovenous intervention in deep venous occlusion (TORPEDO) trial: midterm results. J Endovasc Ther. 2012;19:273–280.
37. Enden T, Haig Y, Klow N, et al. Long-term outcome after additional catheter directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. 2012;379:31–38.
38. Haig Y, Enden T, Slagsvold CE, et al. Determinants of early and long-term efficacy of catheter-directed thrombolysis in proximal deep vein thrombosis. J Vasc Interv Radiol. 2012;24:17–24.
39. Elsharawy M, Elzayat E. Early results of thrombolysis vs anticoagulation in iliofemoral venous thrombosis. Eur J Vasc Surg. 2002;24:209–214.
40. Comerota AJ, Kearon C, Gu CS, et al. Endovascular thrombus removal for acute iliofemoral deep vein thrombosis: analysis from a stratified multicenter randomized trial. Circulation. 2019;139:1162–1173.
41. Kahn SR, Partsch H, Vedantham S, Prandoni KC. Subcommittee on control of anticoagulation of the scientific and standardization committee of the international society on thrombosis and heamostasis. J Thromb Haemost. 2009;7(5):879.
42. Neglén P, Hollis KC, Olivier J, Raju S. Stenting of the venous outflow in chronic venous disease: long-term stent-related outcome, clinical, and hemodynamic result. J Vasc Surg. 2007;46(5):979–990. doi:10.1016/j.jvs.2007.06.046
43. Moudgill N, Hager E, Gonsalves C, Larson R, Lombardi J, DiMuzio P. May-Thurner syndrome: case report and review of the literature involving modern endovascular therapy. Vascular. 2009;17:330–335.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.