")
Back to Journals » Infection and Drug Resistance » Volume 12
Treatment of late bacterial infections resulting from soft-tissue filler injections
Authors Marusza W, Olszanski R, Sierdzinski J , Ostrowski T, Szyller K, Mlynarczyk G , Netsvyetayeva I
Received 10 September 2018
Accepted for publication 27 December 2018
Published 20 February 2019 Volume 2019:12 Pages 469—480
DOI https://doi.org/10.2147/IDR.S186996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Wojciech Marusza,1 Romuald Olszanski,2 Janusz Sierdzinski,3 Tomasz Ostrowski,4 Kamila Szyller,1 Grazyna Mlynarczyk,5 Irina Netsvyetayeva5
1Academy of Face Sculpting, Warsaw, Poland; 2Military Institute of Health Services, Warsaw, Poland; 3Department of Medical Informatics and Telemedicine, Medical University of Warsaw, Warsaw, Poland; 4Department of General and Endocrine Surgery, Medical University of Warsaw, Warsaw, Poland; 5Department of Microbiology, Medical University of Warsaw, Warsaw, Poland
Purpose: Late bacterial infections (LBIs) after esthetic facial augmentation using hyaluronic acid (HA) fillers are relatively rare yet severe complications that are difficult to treat. No adequate treatment standards have hitherto been formulated. We have bridged this gap by formulating a treatment scheme based on the principles of treating foreign-body implantation-related infections and treating bacterial growth in the form of biofilm. The objective of this study was to evaluate the efficacy of a comprehensive scheme for treating LBI complications after facial augmentation using cross-linked HA fillers.
Methods: A total of 22 patients with LBI symptoms at a site of cross-linked HA injection underwent treatment and observation. The comprehensive treatment scheme formulated by Marusza and Netsvyetayeva (M&N scheme) comprised draining the lesion, dissolution of cross-linked HA with hyaluronidase, broad-spectrum antibiotic combination therapy, and use of probiotics. While 17 patients underwent the M&N scheme, the remaining five were treated with other schemes. Statistical analysis of the data was performed using Mann–Whitney U and χ2 nonparametric tests with SAS 9.4 software.
Results: All 17 patients who underwent the M&N scheme experienced resolution of symptoms, with no recurrence of infection at the HA-injection sites.
Conclusion: To treat LBI at a site of cross-linked HA administration, the principles applicable to infections resulting from implantation of a foreign body must be followed. The treatment period should be sufficiently long for complete resolution of symptoms. The efficacy of treatment is considered proven if 2 months have elapsed without recurrence since the symptoms resolved. The M&N scheme is recommended for use as the first therapeutic option for treating LBI related to soft-tissue fillers.
Keywords: bacterial biofilm, hyaluronic acid, soft-tissue filler complications, biofilm treatment
Introduction
Aesthetic medical procedures involving facial augmentation using hyaluronic acid (HA) fillers are commonplace and their number is steadily increasing. In the US, the use of fillers soared from 1.8 million procedures in 2010 to 2.6 million in 2016, according to data from the American Society of Plastic Surgeons.1 One in every hundred of these patients experiences an infection at a site where a soft-tissue filler has been administered. Inflammatory swelling or nodules usually emerge several weeks to several years after the procedure. Treating infections of this kind poses a serious challenge. If appropriate treatment is not provided at the initial stage of infection (induration, inflammation, and pain), fistulae can form, through which pus and degraded filler pour out.
In cases of culture-negative pus, some medical practitioners consider the aforementioned symptoms to represent an allergic reaction.2 The chief arguments against this diagnosis of an allergic reaction are the long time span (often extending from several weeks to several years after the procedure) and the inefficacy of steroidal therapy.3 Over the last few years, many studies have been published that elucidate the infectious etiology of complications of this kind.4–8 These studies indicate that the inflammatory swelling or nodules at sites of HA injection are related to bacterial biofilm growth on the surface of the filler, which constitutes a foreign body in the subcutaneous tissue.4–8 It has also been proven that various fillers, HA included, constitute a foundation upon which bacterial biofilm can form, generating symptoms of late bacterial infection (LBI) complications.6–8
In 2014, the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) published guidelines on the diagnosis and treatment of biofilm-related infections. Infections complicating procedures involving tissue fillers were included in the scope of the guidelines.9 The following typical yet low-intensity inflammatory reactions were considered clinical symptoms of biofilm-related infections: induration, swelling, erythema, pain, and loss of function. Additionally, the following factors were linked to biofilm-related infections: history of a condition predisposing the patient to biofilm growth (ie, a condition involving implantation of a foreign body), infection lasting >7 days, inefficacy of antibiotic treatment, and objective and subjective symptoms of infection that resolve during antibiotic treatment, but recur after its termination.9
A biofilm is an aggregation of bacterial cells attached to an artificial surface, embedded in a matrix of extracellular bacterial macromolecules. A biofilm, or sedentary microbial amalgam, may consist of one or many strains. Bacterial cells in a biofilm differ physiologically from planktonic cells (free-floating single cells),3 including having a significantly lower metabolic rate.
The eradication of a biofilm from a solid surface is difficult. The matrix protects the microbes from many externally applied factors, such as bactericides. Its branched system of tubules ensures nutrient transport and communication among microbes via chemical and physical signaling (quorum sensing). Bacterial cells in a developed biofilm have a shared set of defensive mechanisms that allow the microbial amalgams to function in conditions in which separate cells would likely die.
Cultivation and identification of bacterial cultures in so altered a state are very difficult.10 In addition, the thickness of a biofilm layer on an artificial surface can be 5–1,200 µm, thereby significantly hindering the extraction of representative samples for examination. Whenever typical microbiological culture methods are used, the results are generally false negative. However, the following methods are deemed valid: biopsy with subsequent utilization of peptide nucleic acid fluorescence in situ hybridization or with subsequent three-dimensional confocal laser-scanning microscopy and direct observation using confocal laser-scanning microscopy.9 Therefore, in recent years, medical biofilm research has progressed from in vitro bacterial cultivation and detection methods to direct in vivo visualization and the utilization of animal models.10
Bacteria in a biofilm possess immunity to antibiotics and other antibacterial medications.11 This immunity is related to their exceedingly slow growth, their resistance to antibiotic penetration, the emergence of resistant phenotypes, and the unfavorable microenvironment within the biofilm.12 Standard methods for determining resistance to medication that were formulated based on planktonic bacteria do not provide valid results in the case of biofilm. Biofilm-related infections resemble chronic and recurrent diseases, are resistant to conventional antibiotic treatment, and do not yield culture-positive results.13 The 2014 ESCMID guidelines on the treatment of infections related to foreign-body implantation recommend the use of antibiotics and debridement, in addition to defining the criteria for either removal or retention of the implant. The guidelines recommend that empirical antibiotic therapy should be extensive, involving at least two antibiotics affecting both Gram-positive and Gram-negative bacteria for at least 3 weeks. In most cases, the infected implant should be removed. It should be retained only if its integrity is preserved, there are no fistulae, and the etiological agent of the infection has been identified and is susceptible to antibiotics effective against biofilm-related infections.9 The objective of this study was to evaluate the efficacy of a comprehensive scheme for treating LBI complications after facial augmentation using cross-linked HA fillers.
Methods
The study was conducted at the Academy of Face Sculpting (Akademia Rzeźbienia Twarzy), Warsaw, Poland in 2012–2017.
Participants
Individuals participating in the study were 22 women aged 30–68 (mean 47.32, median 47.0, SD 10.82) years who had been referred by various cosmetic doctors in Poland. All had symptoms of LBI at sites of cross-linked HA injection. The symptoms had occurred at 1–18 months (mean 3.59, median 2.0, SD 3.86) after the procedure. The patients had been treated with cross-linked HA gel supplied by various manufacturers. The HA was produced by bacterial fermentation, which is legally permitted for use in aesthetic medicine in Poland. The volume of cross-linked HA administered was 1–6 (mean 2.09, median 2.0, SD 1.19) mL. Table 1 shows the relevant data on the participants.
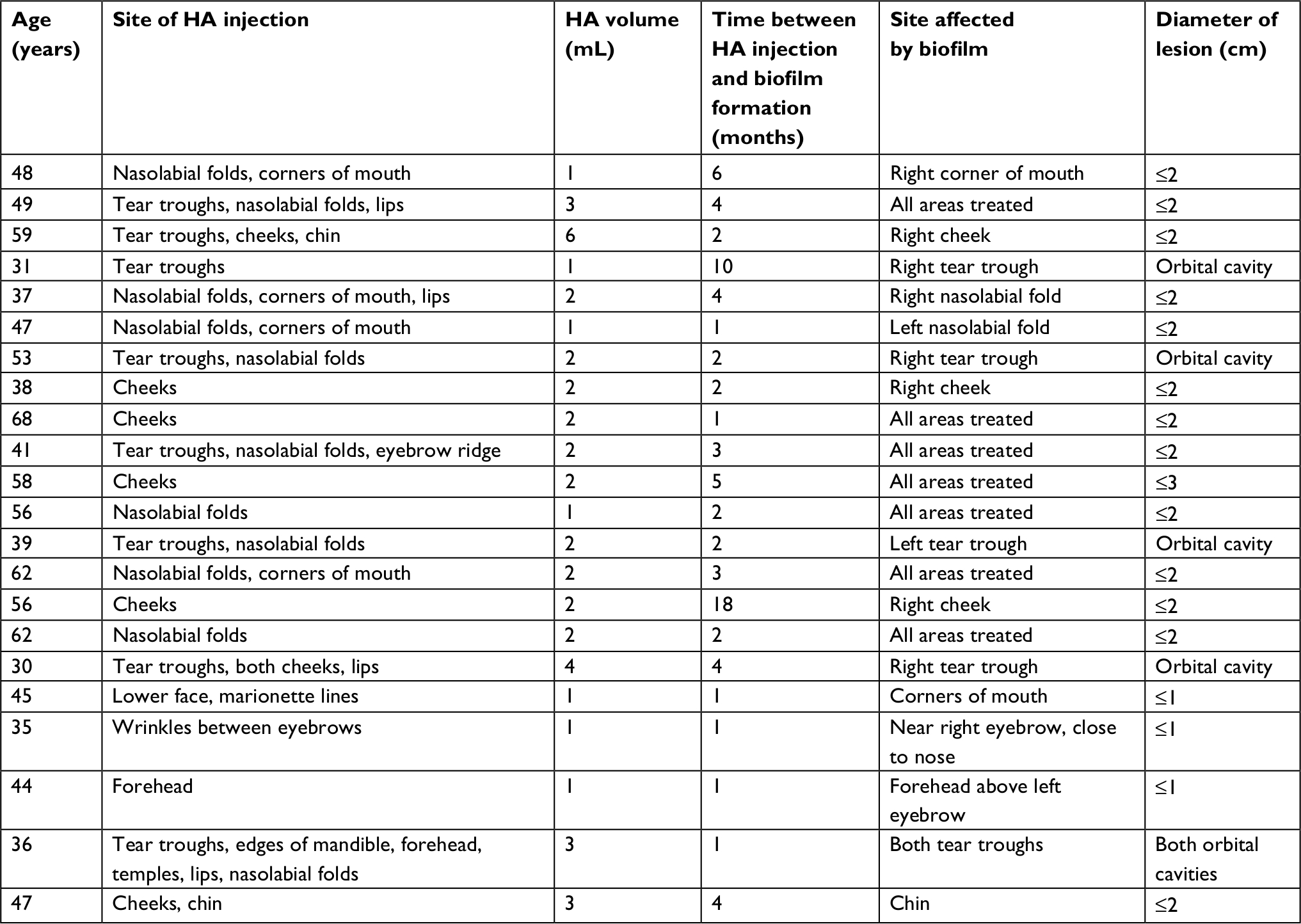 | Table 1 Description of study participants Abbreviation: HA, hyaluronic acid. |
Inclusion criteria for participation in the study were: 1) having undergone an aesthetic procedure with the use of ≥1 mL cross-linked HA gel containing ≥20 mg/mL of stabilized cross-linked HA, which was injected into facial tissue; 2) LBI symptoms of inflammatory swelling or nodules as a complication at one or more sites of injection of cross-linked HA, involving redness, swelling, induration, tenderness, and pus discharge; 3) duration from initial HA administration to LBI occurrence >1 month; and 4) a signed consent form.
Marusza and Netsvyetayeva (M&N) scheme of comprehensive treatment
The M&N scheme involves the following procedures.
- Puncturing the lesion with an 18 G needle, followed by drainage of pus and fermented cross-linked HA twice a week, until complete resolution.
- An allergy test is performed before the first administration of hyaluronidase. It entails subcutaneous injection of 20 units of hyaluronidase into the forearm skin, followed by a 30-minute observation period. At least 72 hours must pass before assessing the result to ensure that any negative results are valid, as intolerance may be either the early or late type.14
- Local administration of hyaluronidase directly onto the lesion twice a week for 14–21 days or until complete resolution of swelling and nodules (whichever is longer). The recommended hyaluronidase doses, according to the size of the swelling and nodules, are presented in Table 2.
- Oral administration of combination antibiotic therapy: 2×400 mg moxifloxacin per os +2×500 mg clarithromycin per os for 14–21 days or until the complete resolution of swelling and nodules (whichever is longer).
- Probiotic formulation consisting of 1.6 billion CFU of lyophilized strains of Lactobacillus acidophilus, L. delbrueckii subsp. bulgaricus, and Bifidobacterium lactis, three capsules per day, during the antibiotic therapy and for 1 month after its completion.
 | Table 2 Variation in hyaluronidase dose with size of inflammatory facial swelling or nodule Notes: aAssessed based on the diameter measured between the opposite rims that were furthest apart. bThere are routinely six units per injection. |
Criteria for recovery
These were the absence of symptoms of bacterial infection, such as redness, swelling, hardness, tenderness, and pus discharge, at the site of cross-linked HA administration and an asymptomatic state for 2 years.
Criteria for unsuccessful treatment
These were lack of substantial improvement within the first 14 days after beginning LBI therapy, and relapse, ie, recurrence of LBI symptoms (redness, swelling, hardness, tenderness, or pus discharge) at the site of cross-linked HA administration in the 2-year period after treatment of the original lesions was finished.
Statistical analysis
The SAS 9.4. software suite (SAS Institute Inc., Cary, NC, USA) was utilized for statistical evaluation of the data. A descriptive analysis of the data was performed. This was followed by an analysis using the Shapiro–Wilk test of normality to compare the distribution of the data with the Gaussian distribution. To assess differences between subgroups, the nonparametric Mann–Whitney U test (for continuous variables) and the nonparametric χ2 test (for discrete variables) were applied. P<0.05 was considered to represent statistical significance.
Results
Of the 22 patients, 17 (77.27%) were cured using the M&N scheme, while five (22.73%) were cured using other treatment schemes. Of the 17 patients cured with the M&N scheme, five were cured after application of the scheme as the first therapeutic option, whereas for 12 it was applied only after unsuccessful treatment with other schemes.
Based on the treatment schemes and results, the 22 patients were divided into three subgroups: 1) five patients who were treated with the M&N scheme as the first therapeutic option; 2) 12 patients who were treated with the M&N scheme as the second therapeutic option after unsuccessful treatment with other schemes; and 3) five patients who were cured using treatment schemes other than the M&N scheme. Table 3 shows the descriptions of the groups: the group of 17 patients cured using the M&N scheme and subgroups 1–3.
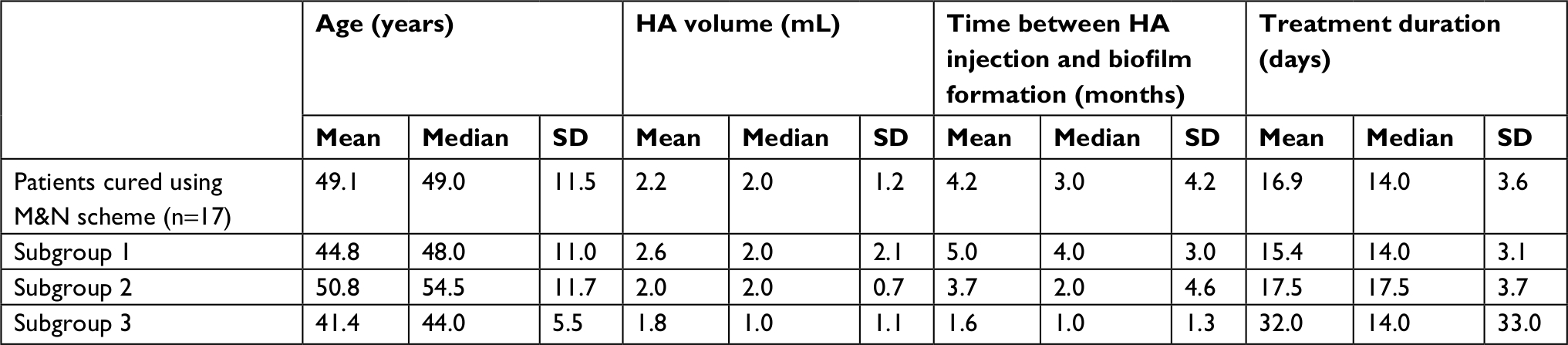 | Table 3 Description of the groups Abbreviations: HA, hyaluronic acid; M&N, Marusza and Netsvyetayeva. |
Subgroup 1
As shown in Table 4, in subgroup 1 there were five patients for whom the M&N scheme was applied as the first therapeutic option after LBI was noticed at a site where cross-linked HA had been administered. For all subgroup 1 patients, resolution of local symptoms was achieved after treatment lasting 14–21 days, with no relapse during the subsequent 2 months. After the 2-month period, all patients underwent remedial therapy with cross-linked HA, with no infectious complications at the site of administration within the subsequent 2 years.
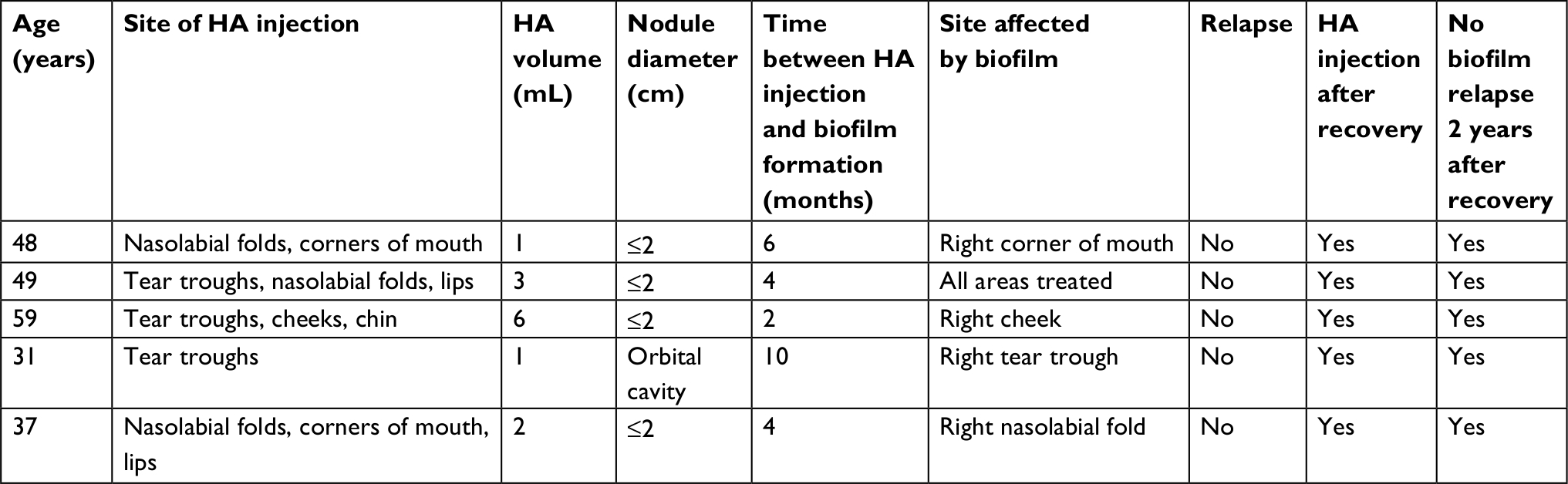 | Table 4 Description of participants treated with M&N scheme as first therapeutic option Notes: Comprehensive treatment in accordance with the M&N scheme: puncture of the lesion and drainage of pus and fermented HA. Orally administered combination antibiotic and probiotic therapy: 2×400 mg moxifloxacin + 2×500 mg clarithromycin + probiotic formulation consisting of 1.6 billion CFU lyophilized strains of Lactobacillus acidophilus, L. delbrueckii subsp. bulgaricus, and Bifidobacterium lactis, three capsules a day. Duration of antibiotic therapy: 14–21 days or until the complete resolution of swelling and nodules (whichever is longer). Duration of probiotic treatment: during the antibiotic therapy and 1 month after its termination. Duration of locally administered hyaluronidase treatment: 14–21 days or until the complete resolution of swelling and nodules (whichever was longer). Hyaluronidase dosage: according to Table 2. Abbreviations: M&N, Marusza and Netsvyetayeva; HA, hyaluronic acid; CFU, colony-forming unit. |
Subgroup 2
As shown in Table 5, in subgroup 2 there were 12 patients for whom the M&N scheme was applied as the second therapeutic option after unsuccessful treatment with other treatment schemes. The original unsuccessful biofilm treatments were as follows. Four patients were treated with the M&N scheme, but with ciprofloxacin instead of moxifloxacin. Resolution of symptoms was achieved, followed by remission during the 2-month observation period. After remedial administration of cross-linked HA, three patients experienced relapse of symptoms at previously affected sites, while the fourth experienced a relapse at another site. Another three patients were treated with the M&N scheme, but with clarithromycin monotherapy in two cases and a combination of clarithromycin with amoxicillin and clavulanic acid in the other case. Spontaneous relapse (without remedial HA administration) occurred in all three patients after the original symptoms had resolved. Four other patients were treated with a variety of antibiotics, but without hyaluronidase, and there was a lack of initial symptom resolution at the site of the original biofilm. The final patient of the 12 had four symptom relapses after each remedial HA administration, despite having been comprehensively treated with the M&N scheme three times. The scheme was successful only after the patient had a tooth with a periodontal cyst extracted and was treated for chronic odontogenic sinusitis.
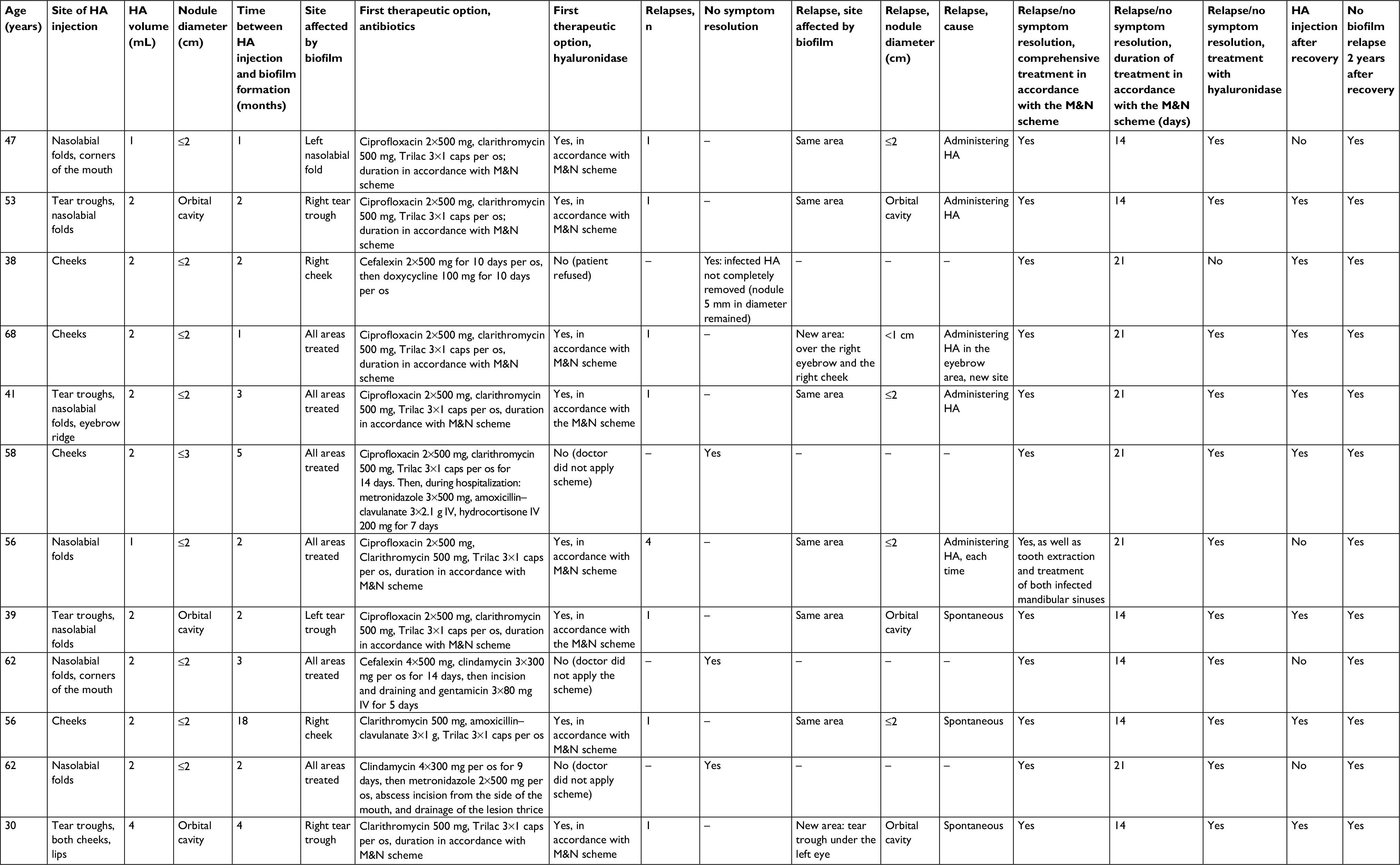 | Table 5 Description of participants successfully treated in accordance with the M&N scheme after unsuccessful treatment with other schemes Notes: Comprehensive treatment in accordance with the M&N scheme: puncture of the lesion and drainage of pus and fermented HA. Orally administered combination antibiotic and probiotic therapy: 2×400 mg moxifloxacin + 2×500 mg clarithromycin + probiotic formulation consisting of 1.6 billion CFU lyophilized strains of Lactobacillus acidophilus, L. delbrueckii subsp. bulgaricus, and Bifidobacterium lactis, three capsules a day. Duration of antibiotic therapy: 14–21 days or until complete resolution of swelling and nodules (whichever is longer). Duration of probiotic treatment: during antibiotic therapy and 1 month after its termination. Duration of locally administered hyaluronidase treatment: 14–21 days or until complete resolution of swelling and nodules (whichever was longer). Hyaluronidase dosage: according to Table 2. Abbreviation: M&N, Marusza and Netsvyetayeva; HA, hyaluronic acid; IV, intravenous. |
Of the 12 patients in subgroup 2, eight received remedial cross-linked HA after resolution of symptoms with the M&N scheme, and remission was observed during the following 2 months. No relapses occurred in the following 2 years. The other four patients did not wish for another application of cross-linked HA as part of remedial therapy.
Subgroup 3
As shown in Tables 6 and 7, in subgroup 3 there were five patients who were cured after using schemes other than the M&N. The biofilm treatments and results were as follows. For the first patient, resolution of symptoms of the original biofilm was achieved after a single administration of 40 units of hyaluronidase alone (not in accordance with the hyaluronidase dosage in the M&N scheme). Following a 1-month remission period, a relapse caused by remedial cross-linked HA administration was observed. Treatment of the relapse involved administration of hyaluronidase alone at the dosage of 135 units recommended in the M&N scheme (first time for this patient according to the M&N scheme, and no other aspects of the M&N scheme were involved). For the second patient, resolution of symptoms of the original biofilm was observed after the sole use of a hyaluronidase dose according to the M&N scheme for 28 days (no other aspects of the M&N scheme were involved). For the third patient, resolution of symptoms of the original biofilm was achieved after laser surgery (the initial lesion was removed with laser, leaving scar tissue). For the final two patients, resolution of symptoms of the original biofilm was observed after the application of a modified M&N scheme, with clarithromycin monotherapy as the only deviation.
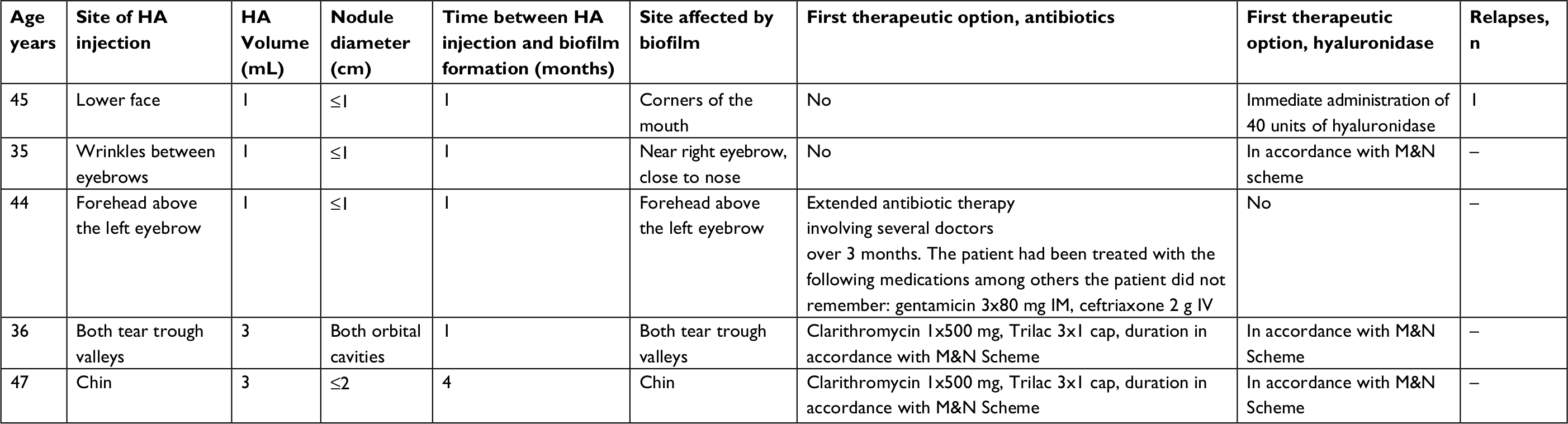 | Table 6 Participants (subgroup 3) successfully treated by application of schemes other than M&N, description of initial treatment Notes: Comprehensive treatment in accordance with M&N scheme: puncture of the lesion and drainage of pus and fermented HA. Orally administered combination antibiotic and probiotic therapy: 2x400 mg moxifloxacin + 2x500 mg clarithromycin + probiotic formulation consisting of 1.6 billion CFU lyophilized strains of Lactobacillus acidophilus, L. delbrueckii subsp. bulgaricus, and Bifidobacterium lactis, three capsules a day. Duration of antibiotic therapy: 14–21 days or until complete resolution of swelling and nodules (whichever was longer). Duration of probiotic treatment: during antibiotic therapy and 1 month after its termination. Duration of locally administered hyaluronidase treatment: 14–21 days or until complete resolution of swelling and nodules (whichever was longer). Hyaluronidase dosage according to Table 2. Abbreviations: HA, hyaluronic acid; IM, intramuscular; IV, intravenous; M&N, Marusza and Netsvyetayeva. |
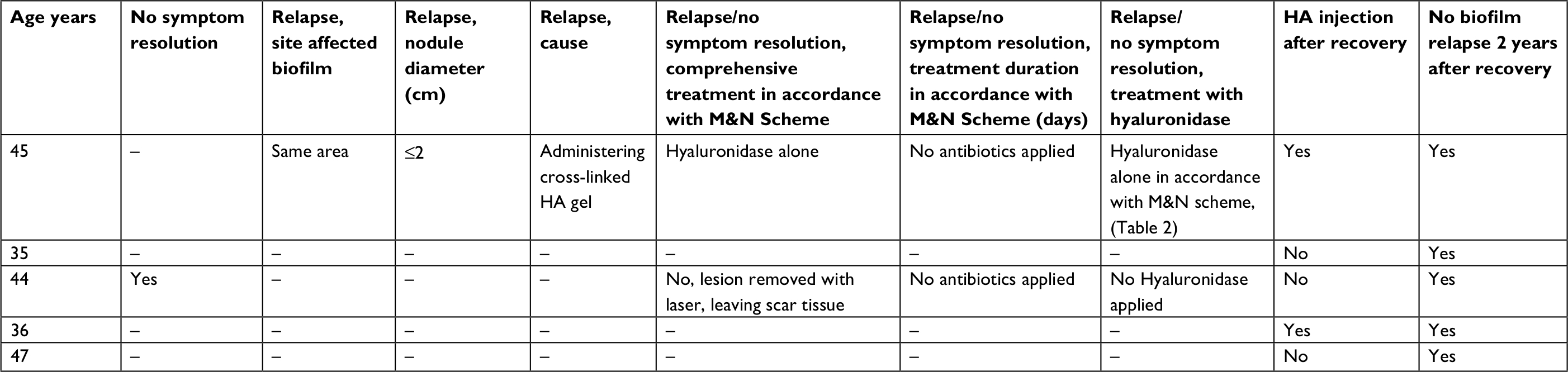 | Table 7 Participants (subgroup 3) successfully treated by application of schemes other than M&N, description of relapses and recovery Notes: Comprehensive treatment in accordance with M&N scheme: puncture of the lesion and drainage of pus and fermented HA. Orally administered combination antibiotic and probiotic therapy: 2x400 mg moxifloxacin + 2x500 mg clarithromycin + probiotic formulation consisting of 1.6 billion CFU lyophilized strains of Lactobacillus acidophilus, L. delbrueckii subsp. bulgaricus, and Bifidobacterium lactis, three capsules a day. Duration of antibiotic therapy: 14–21 days or until complete resolution of swelling and nodules (whichever was longer). Duration of probiotic treatment: during antibiotic therapy and 1 month after its termination. Duration of locally administered hyaluronidase treatment: 14–21 days or until complete resolution of swelling and nodules (whichever was longer). Hyaluronidase dosage according to Table 2. Abbreviations: HA, hyaluronic acid; M&N, Marusza and Netsvyetayeva. |
Statistical analysis
For subgroups 1 and 2, there were no significant differences in the median age (χ2=–0.90, P=0.37), median volume of HA administered (χ2=0.10, P=0.92), or median duration between cross-linked HA administration and LBI symptoms (χ2=1.58, P=0.11). For subgroups 1 and 3, there were no significant differences in median age (χ2=0.83, P=0.40) or median volume of HA administered (χ2=0.42, P=0.68). However, there was a significant difference in median duration between cross-linked HA administration and LBI symptoms (χ2=2.09, P=0.04), with subgroup 1 having a longer median duration than subgroup 3.
When comparing the group of 17 patients cured using the M&N scheme with the group of five patients cured with other schemes (subgroup 3), there were no significant differences in median age (χ2=1.52, P=0.12) or median volume of HA administered (χ2=0.54, P=0.58). However, there was a significant difference in median duration between cross-linked HA administration and LBI symptoms (χ2=2.07, P=0.03), with the group of 17 patients having a longer median than subgroup 3.
Discussion
When developing the scheme for treating LBI complications at sites where cross-linked HA fillers were administered, we assumed that the complications were related to bacterial growth in the form of biofilm on the surface of the filler.3 We also adopted the view that cross-linked HA introduced into facial soft tissue constituted a foreign body. As such, we used a comprehensive compound approach for the development of the treatment scheme. We modeled this approach on principles used in other medical disciplines regarding foreign-body implantation-related infections and bacterial growth in the form of biofilm. These principles are: first, draining and removal of necrobiotic tissues; second, complete removal of the foreign body on which the biofilm has formed; and third, empirical antibiotic therapy in the form of combination therapy for an extended period. As a result of this approach, development of antibiotic resistance can be avoided and the entire spectrum of bacteria that could be etiological agents can be accounted for. Unless the entire infection is eradicated, biofilm microbes may survive and cause a relapse once antibiotic treatment is terminated.9 This occurred in some of the patients in our study: ineffective treatment and spontaneous relapses occurred in each subgroup when any lesions had been left in soft facial tissue.
In compliance with the first rule, drainage of pus along with the bacteria-contaminated and fermented HA filler should be performed. We suggest draining the lesions as the first procedural stage, twice a week until complete resolution. The second rule is to remove the foreign body completely, ie, the basis upon which the biofilm has formed. The intended effect can be accomplished by application of hyaluronidase directly onto the lesion. This is the method utilized by the majority of practitioners of aesthetic medicine. According to other study authors, the recommended dosage ranges between 1.5 and 75 units and is dependent on the specific complication site.15–17 Successful treatment relies on the complete dissolution of nodules. Based on our practical experience, the volume associated with each hyaluronidase administration, which is conducted twice a week, should be proportional to the size of the lesion (assessed based on its diameter, measured between the opposite rims that are farthest apart) and ranges from 6 to 195 units per administration. The estimated duration of therapy should be adequate for the intended effect, and no shorter than 14 days.
The third rule relates to the use of combination antibiotic therapy of proven efficacy against the type of bacteria forming the biofilm. Given this, we sought efficacious empirical therapeutic options with the broadest possible bactericidal spectra, as the etiological agents of infection could not be determined for any of the participants. The antimicrobial medication regimen needed to be efficacious against both Gram-positive and Gram-negative aerobic bacteria, as well as against anaerobes. In addition, medications had to be orally administrable and certified for the treatment of skin and subcutaneous tissue infections.
According to the relevant sources, these criteria are met by moxifloxacin and clarithromycin.18–27 Moxifloxacin is a chemotherapeutic agent belonging to the fluoroquinolone group. It differs from ciprofloxacin in terms of its in vitro effectiveness against Gram-positive aerobic bacteria, strong bactericidal properties against Gram-negative aerobic bacteria, and simultaneous effectiveness against anaerobes. It also affects atypical mycobacteria related to dermatological infections. In addition, it penetrates the biofilm environment well and exhibits its bactericidal properties within the biofilm. The effectiveness of moxifloxacin monotherapy has also been proven against biofilm formed by staphylococci.18–21 Moxifloxacin can also enter infected vesicles, muscles, and subcutaneous fatty tissue. Therefore, it is a reasonable option for treating skin and skin-structure infections.22
Clarithromycin is a semisynthetic macrolide antibiotic with bactericidal properties against Gram-positive and atypical bacteria. In addition, it has the unique property of destroying biofilm structures irrespective of the type of bacteria comprising them.23–27 Many authors have recommended eradicating biofilm using combination therapy in which clarithromycin is the second antibiotic, as it can increase the effectiveness of the first antibiotic.23–27 In cases of biofilm formed by methicillin-resistant Staphylococcus aureus, clarithromycin acts synergistically with daptomycin to remove the biofilm from titanium implants, which cannot be achieved with daptomycin monotherapy.23 Fujimura et al also described the destruction of S. aureus biofilm on titanium implants using combination therapy involving clarithromycin with cefazolin or vancomycin.24 Gander et al indicated that a combination of clarithromycin with moxifloxacin considerably increased the destructive impact on staphylococci biofilm in an in vitro model.25 Lastly, the combination of ciprofloxacin and clarithromycin displays considerable synergy in the destruction of Pseudomonas aeruginosa biofilm in rat mucosal tissue.26,27
The duration of the antibiotic therapy should be related to the clinical response and last at least 7 days after the complete resolution of symptoms and disappearance of palpable lesions in the soft tissue. Subsequent remedial administration of cross-linked HA after the resolution of symptoms should occur no earlier than 2 months after successful treatment.
The introduction of probiotics into the scheme was justified by the results of our previous study, which showed that treatment with physiological skin flora decreased the risk of LBI after cross-linked HA administration.28 We are aware that our choice of probiotics was not perfect for ensuring an appropriate composition of the physiological skin flora during and after empirical broad-spectrum antibiotic usage. However, the formulation that we used is the only probiotic registered in Poland as a medication, rather than as a mere supplement. We have only recently begun a search for specific probiotic formulations adjusted for the location and type of infection, as well as the antibiotic therapy used.
By adhering to this therapeutic approach, we achieved satisfactory efficacy in treating LBI after cross-linked HA administration. One exception occurred in a case of one patient of 17, who had four relapses following each attempt at remedial administration of cross-linked HA, despite rigorous application of the M&N scheme. This was related to a concurrent uncured periodontium infection and to odontogenic sinusitis. As such, we wish to stress the importance of appropriate establishment of eligibility before treatment.29 It is essential always to diagnose and eradicate any other infections before administering cross-linked HA, in line with the presurgery rules used before cardiology and orthopedic surgeries involving foreign-body implantation. This minimizes the risk of complications from aesthetic medical procedures, including biofilm-related LBIs at sites where cross-linked HA has been administered.
An interesting observation was made during our study regarding the significant difference in the median duration from cross-linked HA administration to LBI-symptom development between the 17-patient group cured using the M&N scheme and the five-patient group cured using other schemes (subgroup 3). For the former group, the mean duration was 4.2 (median 3.0, SD 4.2) months, while for the latter group it was 1.6 months (median 1.0, SD 1.3). This suggests that quickly growing bacteria (which generate symptoms in a shorter time frame) are easier to eradicate. Nevertheless, due to the insufficient size of the five-patient subgroup 3 and our lack of knowledge about the microbial species that caused the infections, we are unable to make a more informed comment regarding this phenomenon, and it requires further study.
In conclusion, it is worth underscoring that the recommended scheme is designed for empirical treatment of LBI complications related to bacteria in a biofilm. These complications manifest >4 weeks after the procedure, the etiological microbes are unidentifiable using standard microbiological methods, and their original source is rarely identified. The etiology of LBI complications is the subject of our future research. It is suggested, but with the caveat of a lack of rigorous evidence, that etiological microbes have low virulence, unlike those causing early bacterial complications. Early bacterial complications, which are usually caused by S. aureus or Streptococcus pyogenes, are severe and thus require other treatment schemes. Their occurrence is directly related to inappropriately performed skin disinfection at the HA-administration site or to infringements of other rules related to aseptic and antiseptic methods. It is essential to follow these rules carefully with respect to all procedures that involve compromising skin integrity.
Conclusion
In LBI therapy for a site of cross-linked HA administration, the principles used in other medical disciplines regarding foreign-body implantation-related infections must be observed. The therapy ought to be of sufficient duration for symptoms to resolve without relapse in the following 2-month period. This ensures that cross-linked HA can be administered safely as part of remedial therapy after treatment of LBI. The M&N scheme is recommended as the first therapeutic option for treating LBI complications related to soft-tissue fillers.
Ethics approval and consent to participate
All participants provided written informed consent. The research was approved by the Ethics Committee at the Department of Microbiology of Warsaw Medical University. This study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
The authors hereby certify that all work contained in this article is original. All authors contributed to this research, claim full responsibility for the contents of this article, and have read and approved the final manuscript.
Availability of data and material
All available data are presented in the tables.
Acknowledgments
This article was not supported by any grants. The funding for the research and manuscript preparation was sourced from MW, OR, OT, and SK.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
PlasticSurgery.org [website on the Internet]. American Society of Plastic Surgeons Online Resources, Inc.; 2017 Plastic Surgery Statistics Report. Available from: https://edition.cnn.com/2017/12/21/health/dermal-lip-filler-injections-risks-study/index.html. Accessed December 18, 2018. | ||
Requena L, Requena C, Christensen L, Zimmermann US, Kutzner H, Cerroni L. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):1–34. | ||
Alhede M, Bjarnsholt T. Are biofilms responsible for the adverse effects experienced following soft-tissue fillers? Future Microbiol. 2014;9(8):931–933. | ||
Christensen L, Breiting V, Janssen M, Vuust J, Hogdall E. Adverse reactions to injectable soft tissue permanent fillers. Aesthetic Plast Surg. 2005;29(1):34–48. | ||
Bjarnsholt T, Tolker-Nielsen T, Givskov M, Janssen M, Christensen LH. Detection of bacteria by fluorescence in situ hybridization in culture-negative soft tissue filler lesions. Dermatol Surg. 2009;35(Suppl 2):1620–1624. | ||
Saththianathan M, Johani K, Taylor A, et al. The role of bacterial biofilm in adverse soft-tissue filler reactions: a combined laboratory and clinical study. Plast Reconstr Surg. 2017;139(3):613–621. | ||
Alhede M, Er Ö, Eickhardt S, et al. Bacterial biofilm formation and treatment in soft tissue fillers. Pathog Dis. 2014;70(3):339–346. | ||
Dayan S, Arkins J, Brindise R. Soft tissue fillers and biofilms. Facial plast Surg. 2011;27(1):23–28. | ||
Høiby N, Bjarnsholt T, Moser C, et al. ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin Microbiol Infect. 2015;21(Suppl 1):S1–S25. | ||
Hall-Stoodley L, Stoodley P, Kathju S, et al. Towards diagnostic guidelines for biofilm-associated infections. FEMS Immunol Med Microbiol. 2012;65(2):127–145. | ||
Singh S, Singh SK, Chowdhury I, Singh R. Understanding the mechanism of bacterial biofilms resistance to antimicrobial agents. Open Microbiol J. 2017;11(1):53–62. | ||
Høiby N, Bjarnsholt T, Givskov M, Molin S, Ciofu O. Antibiotic resistance of bacterial biofilms. Int J Antimicrob Agents. 2010;35(4):322–332. | ||
Ciofu O, Rojo-Molinero E, Macià MD, Oliver A. Antibiotic treatment of biofilm infections. APMIS. 2017;125(4):304–319. | ||
Andre P, Fléchet ML. Angioedema after ovine hyaluronidase injection for treating hyaluronic acid overcorrection. J Cosmet Dermatol. 2008;7(2):136–138. | ||
Cavallini M, Gazzola R, Metalla M, Vaienti L. The role of hyaluronidase in the treatment of complications from hyaluronic acid dermal fillers. Aesthet Surg J. 2013;33(8):1167–1174. | ||
Menon H, Thomas M, D’Silva J. Low dose of hyaluronidase to treat over correction by HA filler – a case report. J Plast Reconstr Aesthet Surg. 2010;63(4):e416–e417. | ||
Cohen be, Bashey S, Wysong A. The use of hyaluronidase in cosmetic dermatology: a review of the literature. J Clin Investigat Dermatol. 2015;3(2):7. | ||
Parra-Ruiz J, Vidaillac C, Rose WE, Rybak MJ. Activities of high-dose daptomycin, vancomycin, and moxifloxacin alone or in combination with clarithromycin or rifampin in a novel in vitro model of Staphylococcus aureus biofilm. Antimicrob Agents Chemother. 2010;54(10):4329–4334. | ||
Jacqueline C, Caillon J. Impact of bacterial biofilm on the treatment of prosthetic joint infections. J Antimicrob Chemother. 2014;69(Suppl 1):i37–i40. | ||
San Juan R, Garcia-Reyne A, Caba P, et al. Safety and efficacy of moxifloxacin monotherapy for treatment of orthopedic implant-related staphylococcal infections. Antimicrob Agents Chemother. 2010;54(12):5161–5166. | ||
Swidsinski A, Dörffel Y, Loening-Baucke V, Schilling J, Mendling W. Response of Gardnerella vaginalis biofilm to 5 days of moxifloxacin treatment. FEMS Immunol Med Microbiol. 2011;61(1):41–46. | ||
Guay DR. Moxifloxacin in the treatment of skin and skin structure infections. Ther Clin Risk Manag. 2006;2(4):417–434. | ||
Fujimura S, Sato T, Hayakawa S, Kawamura M, Furukawa E, Watanabe A. Antimicrobial efficacy of combined clarithromycin plus daptomycin against biofilms-formed methicillin-resistant Staphylococcus aureus on titanium medical devices. J Infect Chemother. 2015;21(10):756–759. | ||
Fujimura S, Sato T, Mikami T, Kikuchi T, Gomi K, Watanabe A. Combined efficacy of clarithromycin plus cefazolin or vancomycin against Staphylococcus aureus biofilms formed on titanium medical devices. Int J Antimicrob Agents. 2008;32(6):481–484. | ||
Gander S, Kinnaird A, Finch R. Telavancin: in vitro activity against staphylococci in a biofilm model. J Antimicrob Chemother. 2005;56(2):337–343. | ||
Elkhatib W, Noreddin A. Efficacy of ciprofloxacin-clarithromycin combination against drug-resistant Pseudomonas aeruginosa mature biofilm using in vitro experimental model. Microb Drug Resist. 2014;20(6):575–582. | ||
Hou W, Xiao H. The eliminating effects of clarithromycin combined with ciprofloxacin on Pseudomonas aeruginosa biofilms in the middle ear mucosa of rats. Int J Clin Exp Med. 2016;9(2):2945–2952. | ||
Netsvyetayeva I, Marusza W, Olszanski R, et al. Skin bacterial flora as a potential risk factor predisposing to late bacterial infection after cross-linked hyaluronic acid gel augmentation. Infect Drug Resist. 2018;11:213–222. | ||
Marusza W, Mlynarczyk G, Olszanski R, et al. Probable biofilm formation in the cheek as a complication of soft tissue filler resulting from improper endodontic treatment of tooth 16. Int J Nanomedicine. 2012;7:1441–1447. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.