")
Back to Journals » International Medical Case Reports Journal » Volume 16
Treatment of Facial Lentigines in an Adult Female Patient Suspected with Leopard Overlap Noonan Syndrome
Authors Ruchiatan K , Alifiar NO, Puspitosari D , Hindritiani R
Received 18 February 2023
Accepted for publication 4 May 2023
Published 9 May 2023 Volume 2023:16 Pages 269—274
DOI https://doi.org/10.2147/IMCRJ.S407416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Kartika Ruchiatan, Noer Olivy Alifiar, Diah Puspitosari, Reti Hindritiani
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Kartika Ruchiatan, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +62 811247932, Email [email protected]
Abstract: Lentigines are defined as multiple small pigmented macules measuring up to one centimeter and surrounded by normal-appearing skin, commonly caused by genetic factors. LEOPARD syndrome (LS) is an autosomal dominant distinguished by the presence of several lentigines, with specific phenotypic characteristics that resembles Noonan syndrome (NS). LS is likely to be underdiagnosed or misdiagnosed because many of its symptoms are minor and the accurate diagnosis may be overlooked. Therapy for lentigines are generally aimed at tackling aesthetic disfigurement and its subsequent psychological impacts. This case report aims to highlight the efficacy of 532-nanometer (nm) Q-switched (QS) Nd:YAG laser in treating lentigines in a 21-year-old woman with LS overlap NS. The patient initially came to seek treatment of her facial lentigines. However, some mild abnormalities such as ocular hypertelorism, left eye ptosis, and webbed neck were observed. Hormonal, cardiac, and pulmonary functions were within normal limit. Histopathological results supported the diagnosis of lentigo. The patient was given sunscreen and depigmenting agents and was instructed to apply the medications routinely. The patient then underwent two sessions of 532-nm QS Nd:YAG laser with a 3 mm spot size, 1 J/cm2 fluence, and a 1 Hz frequency. Objective clinical improvements were observed using spectrophotometer examination, there were no side effects found, and she was satisfied with the results. Dermatologists should play an integral role in establishing the diagnosis and management of systemic syndrome, manifesting specifically as dermatological symptoms. Lentigines in LS last throughout the patient’s lifespan. Nd:YAG laser therapy can be effective in treating lentigines with long-lasting results. It plays a role in improving the patient’s life quality, especially where the genetic disorder itself is a debilitating condition. The limitation of this case report was the lack of a genetic test, as the suspected diagnosis was made based on clinical symptoms.
Keywords: lentigo, LEOPARD, Nd:YAG laser, Noonan, syndrome
Introduction
Small, sharply-circumscribed, macular, pigmented, and mucocutaneous lesions, including lentigo, have been described using a variety of terminology. When referring to these lesions, the terms lentigo (singular) and lentigines (plural) are sometimes used interchangeably.1 Generalized lentigines may be an isolated phenomenon without an underlying disease. They can either be present at birth or manifesting themselves during childhood or adolescence. In addition, it may also be a sign of a genetic disorder, such as LS and NS.2 LEOPARD is the abbreviation for multiple lentigines, electrocardiographic (ECG) conduction problems, ocular hypertelorism, pulmonary valve stenosis, abnormalities of genitalia, retardation of growth, and sensorineural deafness.3 LS is thought to be a rare condition.4 About 200 cases have been documented worldwide, although the true incidence of LS has not been determined. LS is probably underdiagnosed or misdiagnosed due to the fact that many of its symptoms are minor and the accurate diagnosis might be missed in the absence of lentigines.5
The manifestation of NS shares common features with LS, such as hypertelorism, eyelid ptosis, delayed development of secondary sex characteristics, and lentigines. The exact relation between LS and NS is unclear. It is possible that they are both the result of same pleiotropic gene. It appears very clear that there are cases that could be placed in either syndrome.6 Due to their visibility, facial lentigines either in LS or NS are the most cosmetically important.7 Treatment other than for cosmetic purposes is generally not indicated.8 Lentigines are effectively treated using 532-nm QS Nd:YAG laser.9 This case report aims to present the use of 532-nm QS Nd-YAG laser in the treatment of facial lentigines in a 21-year-old woman suspected with LS overlapping NS.
Case
A 21-year-old woman presented to the Dermatology and Venereology Department with chief complaint of hyperpigmented macules across nearly the entire face and neck without pain or itch. The lesions first noticed by her mother when she was 4 years old, appeared on her cheeks and gradually increased in number, and spread to almost her entire face and neck. However, during physical examination, we discovered some abnormalities, such as ocular hypertelorism and left eye ptosis (Figure 1A), webbed neck (Figure 1B), vertebrae scoliosis (Figure 1C), and a lack of pubic hair. Regarding Leopard overlap Noonan syndrome, we referred the patient to Internal Medicine Department for further evaluation. Echocardiographic revealed no ventricular hypertrophy related to LS. No abnormalities were found from electrocardiograms with sinus rhythm interpretation. Patient also underwent thoracal radiologic examination that visualized a projected internal fixation at the level of corpus vertebrae Th4-L2 related to her scoliosis history. Laboratory results consist of routine blood examination, thyroid, liver, and renal function were within normal range. Electrolytes and hormonal laboratory values, such as estradiol and follicle stimulating hormone, were within normal limit. Dermatological examination revealed generalized hyperpigmented macules on almost the entire face and body. The histopathological analysis of hyperpigmented macules from the right arm revealed a greater number of melanocytes in the epidermis’ basal layer, elongated epidermal rete ridges, mild inflammatory cells infiltrate on the upper dermis, dilation of blood vessels, and no tumor cells (Figure 2). These histopathological findings were consistent with lentigines. The patient was treated with a combination of kojic acid and 4% hydroquinone cream twice per day, as well as two sessions of 532-nm QS Nd:YAG laser (3 mm spot, 1 J/cm2, 1 Hz) administered at a monthly interval. The patient was also advised to re-apply sunscreen with minimum SPF of 30 every 2 hours during the day. Improvement was observed in terms of skin tone brightness as assessed using spectrophotometry (Figure 3A and B). No issues were observed and the patient was pleased with the outcome.
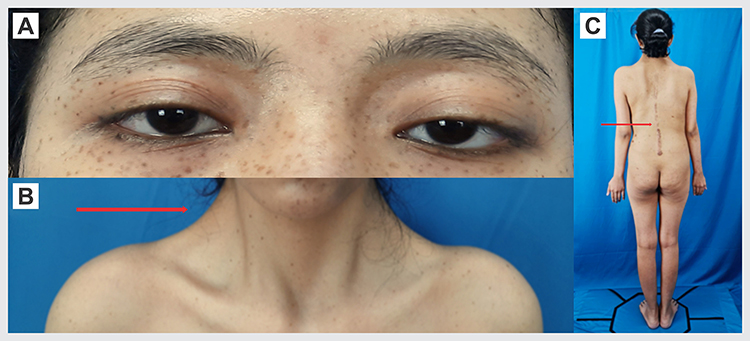 |
Figure 1 Clinical image of physical finding. (A) Ocular hypertelorism and left eye ptosis. (B) Webbed neck. (C) Scoliosis. |
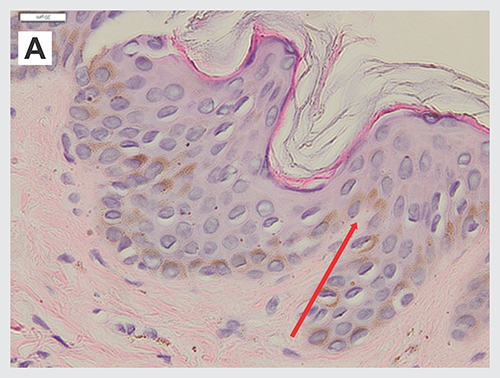 |
Figure 2 Histopathological examination from hyperpigmented macules on right arm showed melanocytes deposition on basal layer of epidermis. |
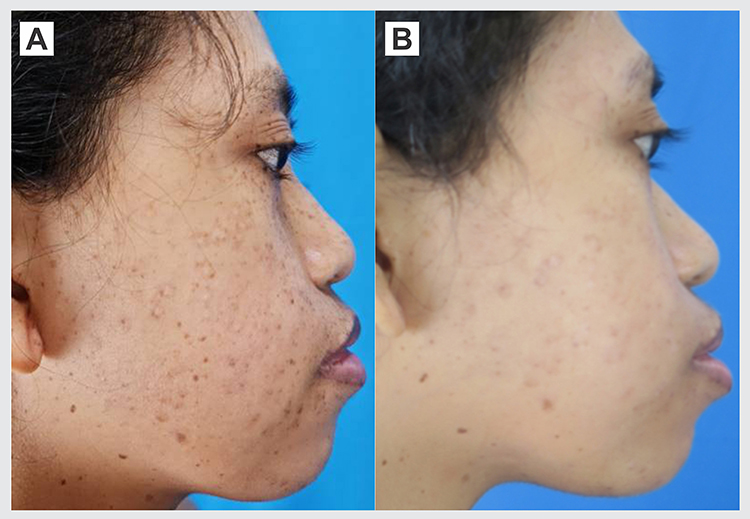 |
Figure 3 Comparison between skin manifestation before and after two sessions of treatment. (A) Hyperpigmented macules on right cheek. (B) Improvement on right cheek skin lesions after two sessions of treatment. |
Discussion
Lentigo derives from the Latin word “lens”, which means lentil. Lentigines are commonly found across all ethnicities.9 Their pigmentation varies from light-brown or brown-black, and their shapes are quite regular, typically circular or oval with a diameter of 3–5 mm.10 They may develop gradually over a number of years, or they may be eruptive, emerging suddenly. Depending on the types of lentigo, they may be solitary or multiple and can develop anywhere on the body surface.9 Lentigo is classified according to its etiology, such as lentigo associated with excessive UV exposure, lentigo not associated with excessive UV exposure, and lentigo associated with syndrome.10 Histopathological findings include epidermal hyperplasia with increased basal layer pigmentation, elongated epidermal rete ridges, and mild inflammatory cells infiltrate on the upper dermis.9,11–13
In 1969, Dr. Michael Blaw published a review about “The multiple Lentigines Syndrome”, currently known as LS. Multiple lentigines, ECG conduction abnormalities, ocular hypertelorism, pulmonary valve stenosis, abnormalities of genitalia, retardation of growth, and sensorineural deafness were the major characteristics of LS.14 Multiple lentigines plus two additional known features or a first-degree relative with multiple lentigines plus three other features are diagnostic criteria for LS.15
The presence of lentigines in LS is an aesthetic problem since malignant transformation of the lentigines has not been reported. However, other associated features need to be considered in the clinical presentation as they may be associated with multisystem anomaly.16 Hypertelorism is almost always present, as are a flat nasal bridge and dysmorphic ears in around 87% of patients. Furthermore, palpebral ptosis, thick lips, and low-set ears with overfolded helix were discovered in 50% of patients. Meanwhile, redundant neck skin or webbed neck were found in 37% of patients.17
In 1963, Noonan described several children manifest many feature in common with LS. The label “Noonan syndrome” has been applied. Both syndromes are predicted to be the result of the same pleiotropic gene.6 Short stature, congenital heart defect, pectus deformities, developmental delay of varying degrees, cryptorchidism, which contributes to lower fertility, and distinctive facies such as ptosis, downslanting palpebral fissures, and webbed neck, are all features of NS in which could be found in LS. Many of the phenotypic abnormalities in NS and LS are extremely similar, both have proportionate short stature, facial dysmorphism, and skeletal anomalies. However, their cardiac phenotypes are substantially diverse. The majority of LS patients with ECG anomalies have left ventricular hypertrophy.17 Making the diagnosis of LS is more challenging. Besides, LS patients’ do not usually present with all its typical clinical features, increasing the possibility of underdiagnosis or misdiagnosis.5 Despite frequent cardiac involvement, most individuals with LS are asymptomatic. Long-term prognosis is relatively good in patients with LS with only mild abnormalities.17
In this case report, hyperpigmented macules without pain or itch on almost the entire face and body were part of the clinical symptoms. Cutaneous lesion manifested initially as a solitary lentigo on the face which later increased in number and size, forming lentigines. The presence of lentigines is an aesthetic problem as the patient presented to the clinic asking for aesthetic treatment of multiple lentigines covering her face. The initial physical examination revealed hypertelorism of the eyes, a webbed neck, and vertebral scoliosis. Therefore, further examination is required to determine the possibility of any syndrome related internal disorders. Examinations of hormonal, cardiac, and pulmonary functions were within normal limit. Histopathological findings showed greater number of melanocytes within the epidermis’ basal layer, elongated epidermal rete ridges, mild inflammatory cells infiltrate on the upper dermis, dilation of blood vessels, and no tumor cells. These findings supported lentigines as the skin manifestation. The patient was suspected of having LS overlapping with NS based on physical examination findings, which included multiple lentigines, left eye ptosis, webbed neck, vertebrae scoliosis, and secondary sexual growth disorder as shown in the lack of pubic hair. Despite this, the patient was never bothered by the abnormality and felt that genetic testing was not necessary to be done.
Most of pigmentary lesions are cosmetic concern and may not need treatment, although other organ systems may be involved as part of a syndrome.17 Facial hyperpigmentation can cause substantial cosmetic deformity with subsequent emotional impact. Hydroquinone and kojic acid are depigmenting agents impede the conversion of L-3,4- dihydroxyphenylalanine (L-DOPA) into melanin.18,19 A combination therapy with two depigmenting agents show better result compared to monotherapy and sunscreens are essential as complementary treatment to prevent repigmentation.20
Multiple types of laser have been used in the treatment of lentigines,21 among them is QS Nd:YAG laser due to the fact that the absorption spectrum of melanin ranges from 351 to 1064 nm.21,22 It has been reported that the QS Nd:YAG laser achieves superior outcomes compared to other types of laser.22 Its therapeutic endpoint is immediate whitening of the pigmented lesion that indicate melanosomes rupture resulting in the release of gas bubbles into the tissue. The laser’s brief burst of high energy destroys melanosomes and melanin-containing cells by selective photothermal and photomechanical effects.23 However, postinflammatory hyperpigmentation (PIH) commonly occurred in patients with Fitzpatrick skin type III–IV as the laser’s side effect.22
To assess the efficacy of treatment in pigmentation disorder, it is necessary to evaluate color changes as indicators of treatment response. Objective quantification of skin color can be achieved with spectrophotometer. This tool objectively evaluates three parameters, namely L* (luminance: black and white) to examine the level of skin brightness, a* (green and red) to examine erythema, and b* (blue and yellow) to examine hyperpigmentation problems.24 Based on the spectrophotometric examination, the patient’s skin got brighter with an increased L* value and less pigmentation with a decreased b* value. The L* value on the forehead was increased from 80.58 to 82.51, on the right cheek from 101.41 to 103.16 and on the left cheek from 59.26 to 99.73. The b* value on the forehead was decreased from 3.32 to 2.63 and on the left cheek from 15.74 to 0.45. Improvement was reported after two sessions with no adverse effects. The use of lasers as adjuvant and maintenance therapy is relatively safe and can be continued for long-term use.
Conclusion
In conclusion, dermatologists provide a crucial role in the diagnosis and management of systemic syndrome that manifests as dermatological symptoms. This case demonstrates that the 532-nm QS Nd:YAG laser is effective for treating facial lentigines in patients with either LS or Noonan syndrome, contributing to enhance the patient’s quality of life, as the genetic disorder itself is a debilitating condition. A limitation to this case was the lack of genetic examination, thus the diagnosis was established based solely on clinical manifestations.
Ethic Statement
The publications of images were included in the patient’s consent for publication of the case. Institutional approval has been obtained to publish the case details.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of the case details and images.
Acknowledgments
The authors would like to thank the staff of Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rahman SB, Bhawan J. Lentigo. Int J Dermatol. 1996;35(4):229–239. doi:10.1111/j.1365-4362.1996.tb02994.x
2. Balin SJ, Barnhill RL. Benign melanocytic neoplasms. In: Bolognia JL, Schaffer JV, Cerroni L, editors. Dermatology.
3. Moatamedi M, Derakhshan M. LEOPARD syndrome: a case report and literature review. Clin Med. 2019;19(Suppl 3):s23. doi:10.7861/clinmedicine.19-3s-s23
4. U.S National Library of Medicine. Noonan syndrome with multiple lentigines; 2016. Available from: https://medlineplus.gov/genetics/condition/noonan-syndrome-with-multiple-lentigines/#.
5. Sarkozy A, Digilio MC, Dallapiccola B. Leopard syndrome. Orphanet J Rare Dis. 2008;3(1):1–8. doi:10.1186/1750-1172-3-13
6. Gorlin RJ, Anderson RC, Moller JH. The Leopard (multiple lentigines) syndrome revisited. Birth Defects Orig Artic Ser. 1971;7(4):110–115.
7. Carcavilla A, Santomé JL, Pinto I, et al. LEOPARD syndrome: a variant of Noonan syndrome strongly associated with hypertrophic cardiomyopathy. Rev Esp Cardiol. 2013;66(5):350–356. doi:10.1016/j.recesp.2012.09.017
8. Paller AS, Mancini AJ. Disorders of pigmentation. In: Paller AS, Mancini AJ, editors. Hurwitz Clinical Pediatric Dermatology.
9. Okulicz JF, Schwartz RA, Jozwiak S. Lentigo. Cutis. 2001;67(5):367–370.
10. Carli P, Salvini C. Lentigines including lentigo simplex, reticulated lentigo and actinic lentigo. In: Color Atlas Melanocytic Lesions Ski. Springer; 2007:290–294.
11. Stefanaki I, Antoniou C, Stratigos A. Benign melanocytic proliferations and melanocytic naevi. In: Griffiths CEM, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook’s Textbook of Dermatology.
12. Rodrigues M, Pandya AG. Hypermelanoses. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, editors. Fitzpatrick’s Dermatology in General Medicine.
13. James WD, Berger TG, Elston DM. Melanocytic nevi and neoplasms. In: James WD, Berger TG, Elston DM, editors. Andrews’diseases of the Skin: Clinical Dermatology.
14. Sarkozy A. Clinical and molecular analysis of 30 patients with multiple lentigines LEOPARD syndrome. J Med Genet. 2004;41(5):e68. doi:10.1136/jmg.2003.013466
15. Digilio MC, Conti E, Sarkozy A, et al. Grouping of multiple-lentigines/LEOPARD and Noonan syndromes on the PTPN11 gene. Am J Hum Genet. 2002;71(2):389–394. doi:10.1086/341528
16. Kontoes PP, Vlachos SP, Marayiannis KV. Intense pulsed light for the treatment of lentigines in LEOPARD syndrome. Br J Plast. 2003;56(6):607–610. doi:10.1016/S0007-1226(03)00218-2
17. Martínez-Quintana E, Rodríguez-González F. LEOPARD syndrome: clinical features and gene mutations. Mol Syndromol. 2012;3(4):145–157. doi:10.1159/000342251
18. Vashi NA, Kundu RV. Facial hyperpigmentation: causes and treatment. Br J Dermatol. 2013;169:41–56. doi:10.1111/bjd.12536
19. Schwartz C, Jan A, Zito PM. Hydroquinone. StatPearls; 2021.
20. Deo KS, Dash KN, Sharma YK, Virmani NC, Oberai C. Kojic acid vis-a-vis its combinations with hydroquinone and betamethasone valerate in melasma: a randomized, single blind, comparative study of efficacy and safety. Indian J Dermatol. 2013;58(4):281. doi:10.4103/0019-5154.113940
21. Dawood N, Tahir K, Shahid M, Aman S, Jawaid K, Ali U. Comparison of efficacy of cryotherapy vs Q-switch Nd: YAG Laser in the treatment of solar lentigines. J Pak Assoc Dermatol. 2020;30(2):277–281.
22. Vachiramon V, Panmanee W, Techapichetvanich T, Chanprapaph K. Comparison of Q‐switched Nd: YAG laser and fractional carbon dioxide laser for the treatment of solar lentigines in Asians. Laser Surg Med. 2016;48(4):354–359. doi:10.1002/lsm.22472
23. Kang HJ, Na JI, Lee JH, Roh MR, Ko JY, Chang SE. Postinflammatory hyperpigmentation associated with treatment of solar lentigines using a Q-Switched 532-nm Nd: YAG laser: a multicenter survey. J Dermatol Treat. 2017;28(5):447–451. doi:10.1080/09546634.2016.1254330
24. Ly BC, Dyer EB, Feig JL, Chien AL, Del Bino S. Research techniques made simple: cutaneous colorimetry: a reliable technique for objective skin color measurement. J Invest Dermatol. 2020;140(1):3–12. doi:10.1016/j.jid.2019.11.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.