")
Back to Journals » International Journal of General Medicine » Volume 15
Treatment for Triple-Negative Breast Cancer: An Umbrella Review of Meta-Analyses
Authors Yin J, Zhu C, Wang G, Gu J
Received 11 April 2022
Accepted for publication 27 June 2022
Published 30 June 2022 Volume 2022:15 Pages 5901—5914
DOI https://doi.org/10.2147/IJGM.S370351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jianyun Yin,1 Changtai Zhu,2 Gaofeng Wang,3 Jianwei Gu1
1Thyroid Breast Surgery, Kunshan Hospital Affiliated to Nanjing University of Traditional Chinese Medicine, Kunshan, People’s Republic of China; 2Department of Transfusion Medicine, Shanghai Sixth Peoples’ Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Department of Gastroenterology, Kunshan Hospital Affiliated to Nanjing University of Traditional Chinese Medicine, Kunshan, People’s Republic of China
Correspondence: Jianyun Yin, Thyroid Breast Surgery, Kunshan Hospital Affiliated to Nanjing University of Traditional Chinese Medicine, Kunshan, People’s Republic of China, Tel +86-0512-57310000, Email [email protected]
Purpose: In recent years, many meta-analyses of triple-negative breast cancer (TNBC) treatment have been published; however, these studies still lack systematic summary. Therefore, the aim of this study is to summarize and evaluate the evidence level and efficacy of treatment for TNBC.
Materials and Methods: Retrospective and prospective studies on treatment of TNBC were searched in the PubMed, Embase, and Cochrane Library databases. The literature search deadline was June 30, 2021. Two investigators independently screened the literature and extracted the data. In addition, the joint World Health Organization–United Nations Food and Agriculture Organization expert consultation was used to evaluate the validity of the evidence.
Results: A total of 28 meta-analyses were included in this study. The treatment interventions for TNBC mainly included surgery, chemotherapy (CT), radiotherapy, molecular targeted therapy, immunotherapy, zoledronic acid, and gonadotropin-releasing hormone (GnRH) analog. Platinum improves the pathological complete response (PCR) rate of patients treated with neoadjuvant chemotherapy (NACT), the objective remission rate (ORR) and overall survival (OS) in patients with metastatic triple-negative breast cancer. Capecitabine improves disease-free survival (DFS) and OS in patients treated with adjuvant CT. Bevacizumab was added to NACT to improve the PCR rate in patients. Immunotherapy improves the PCR rate in patients treated with NACT. The improvement in PCR rate in patients with high Ki67 expression treated with neoadjuvant therapy is highly suggestive. Other interventions had suggestive or weak evidence.
Conclusion: Among the strategies for treating TNBC, platinum, bevacizumab, and immunotherapy can lead to better PCR rates as part of a NACT regimen. Capecitabine as adjuvant CT and platinum in the treatment of metastatic TNBC can benefit patients’ survival. However, the effectiveness of other interventions for TNBC is not yet clear. Further research is needed in the future to obtain more reliable clinical evidence.
Keywords: triple-negative breast cancer, treatment, meta-analysis, umbrella review
Introduction
Breast cancer is the most common malignant tumor among female individuals. The incidence of breast cancer has increased year by year in recent years. According to the latest statistics, new cases of breast cancer account for nearly 30% of all new tumors in female individuals.1 Triple-negative breast cancer (TNBC) is a subtype of breast cancer that is negative on immunohistochemical examination for the estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2.2 TNBC accounts for 15–20% of all breast cancers3 and more than 50% of metastatic breast cancers. The main clinicopathological manifestations of TNBC are high-grade invasive ductal carcinoma and regional necrosis,4 as well as myeloid carcinoma. Compared patients with other subtypes of breast cancer, patients with TNBC are younger, have a larger tumor size, and have more frequent lymph node involvement.5 Moreover, the disease stage in TNBC is typically later,6 the risk of postoperative recurrence is higher, and metastasis is more likely.
Because TNBC has special pathological and biological characteristics, its clinical treatment is difficult. In recent years, the treatment of TNBC has become a focus of tumor research. Many meta-analyses of TNBC treatment have also been published; however, these studies still lack systematic evidence summary and evaluation. Therefore, this study aims to further analyze and evaluate meta-analyses of TNBC treatment to provide more reliable evidence for clinical applications and facilitate the formulation of more effective treatment schemes.
Materials and Methods
Retrieval Strategy
We searched for relevant literature in the PubMed, EMBASE, and Cochrane Library databases as of June 30, 2021. The search terms included “TNBC” or “triple negative breast cancer” or “triple negative breast tumors”, combined with “systematic review or meta-analysis.”
Inclusion Criteria
We included studies that examined patients of any age with TNBC of any disease course; studies that used surgery, chemotherapy (CT), radiotherapy, targeted therapy, immunotherapy, zoledronic acid, GnRH analogs, or their combination as interventions; studies that included overall survival (OS), relapse-free survival (RFS), disease-free survival (DFS), progression-free survival (PFS), event-free survival (EFS), local relapse-free survival (LFS), pathological complete response (PCR), objective response rate (ORR), disease recurrence rate, local recurrence rate, and distant metastasis rate; and studies that were meta-analyses.
Exclusion Criteria
If any of the following conditions were met, the study was excluded from this review: incomplete data, no outcome index literature, only summary text can be obtained, and duplicate publications or those with the same intervention measures.
Literature Screening
Two people independently screened the literature. First, they excluded the studies that obviously did not meet the inclusion criteria after reading the titles and abstracts of all the initially identified studies. The full text of studies passing the initial screening was examined and strictly compared with inclusion and exclusion criteria. Any disagreement about study inclusion was settled by a third evaluator.
Data Extraction
Two people independently extracted data and compared their findings. Extracted data included: title, publication date, author’s name, published journal, disease stage, intervention plan, comparison, number of patients, number of studies, OS, RFS, DFS, PFS, LFS, EFS, ORR, PCR, local recurrence rate, distant metastasis rate, etc.
Evidence Evaluation
Evidence evaluation was based on the joint World Health Organization–United Nations Food and Agriculture Organization expert consultation7 (Table 1). The reliability of evidence was mainly assessed according to the study design (meta-analysis of prospective studies or respective studies), sample number, heterogeneity (I2), and effect size. The evidence was classified as (a) convincing, (b) highly suggestive, (c) suggestive, or (d) weak.
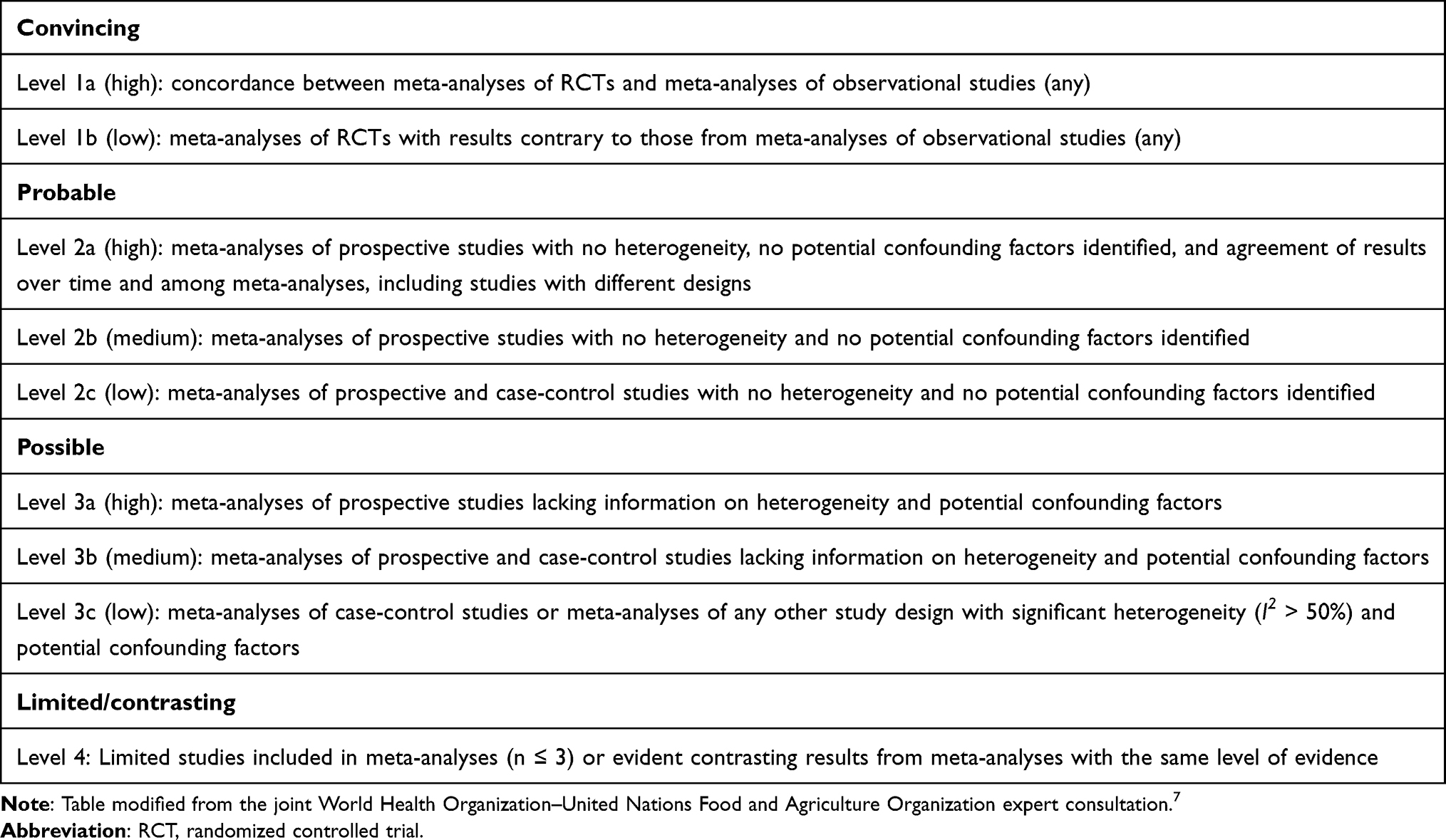 |
Table 1 Criteria Used to Rate the Level of Evidence for the Treatment of Triple-Negative Breast Cancer |
Results
Search Results and General Characteristics of Included Literature
According to the search strategy, a total of 784 studies were screened out. After reading the full text according to the protocol, 28 studies (10 meta-analyses of observational studies and 20 meta-analyses of interventional studies) including seven treatment methods (surgical treatment, 2 studies; CT, 16 studies; radiotherapy, 1 study; targeted therapy, 6 studies; immunotherapy, 1 study; zoledronic acid, 1 study; and GnRH analog, 1 study) were included in this study. The literature screening process is shown in Figure 1. The basic characteristics and results of the included studies are shown in Table 2.
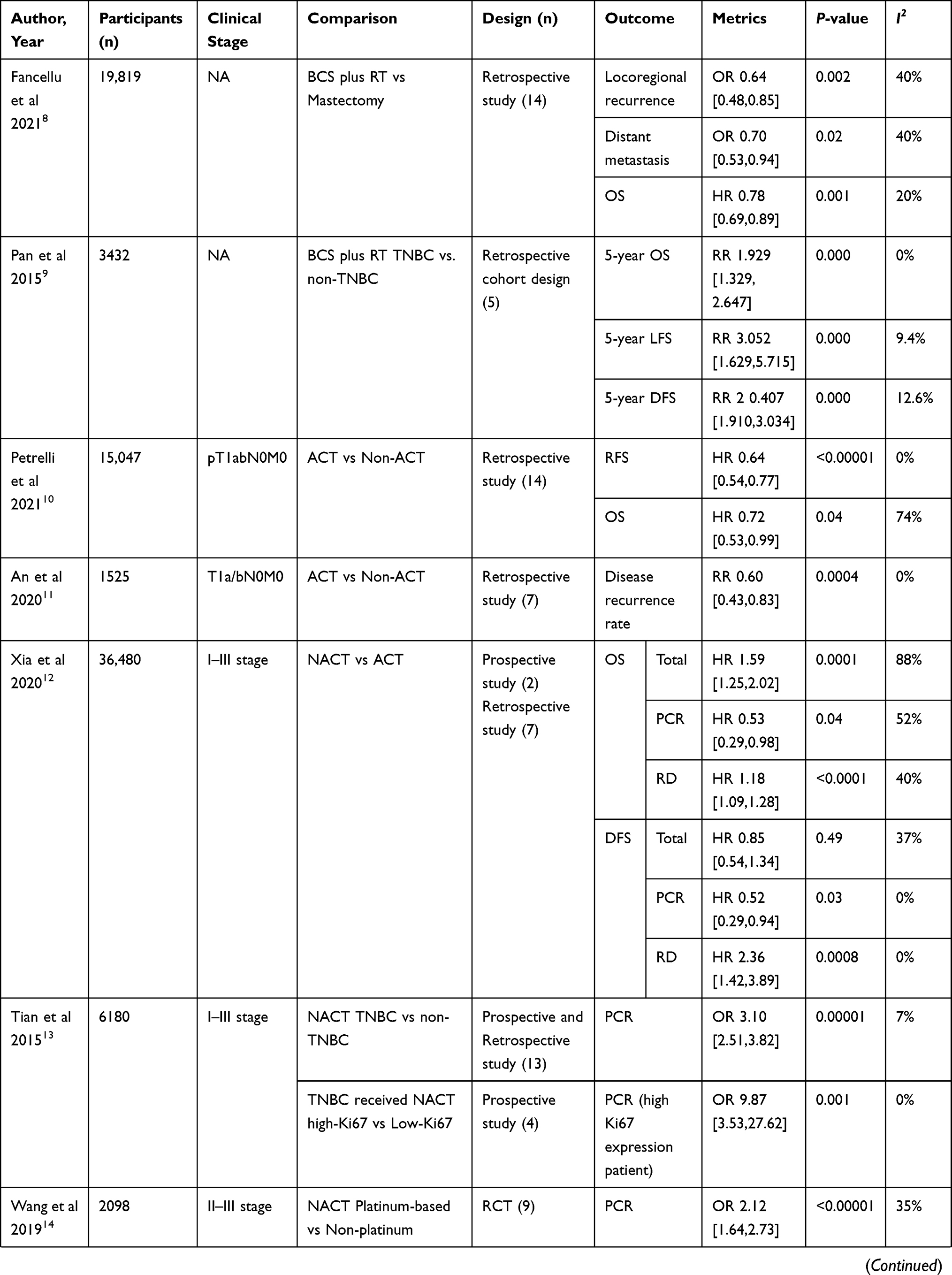 |  | 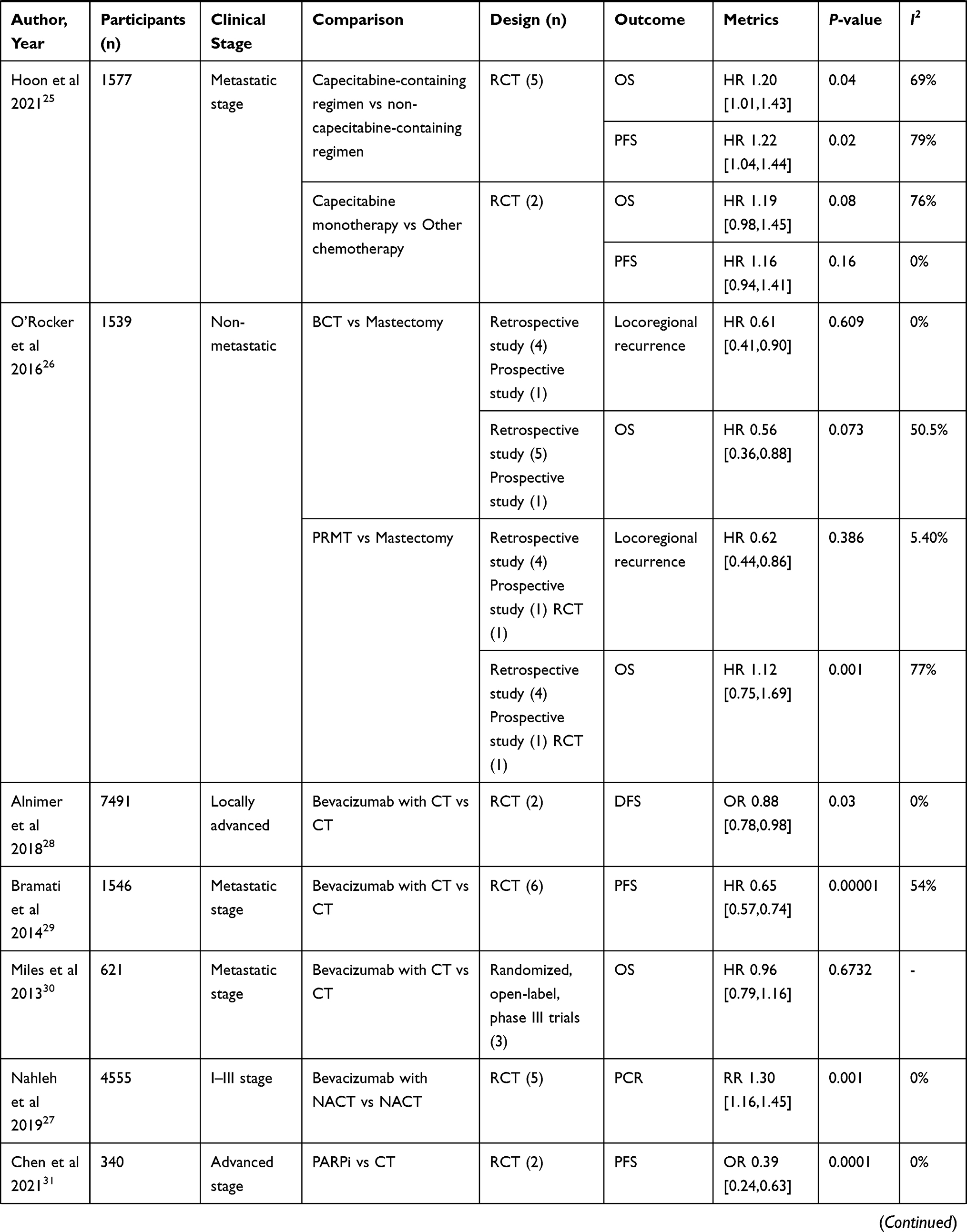 | 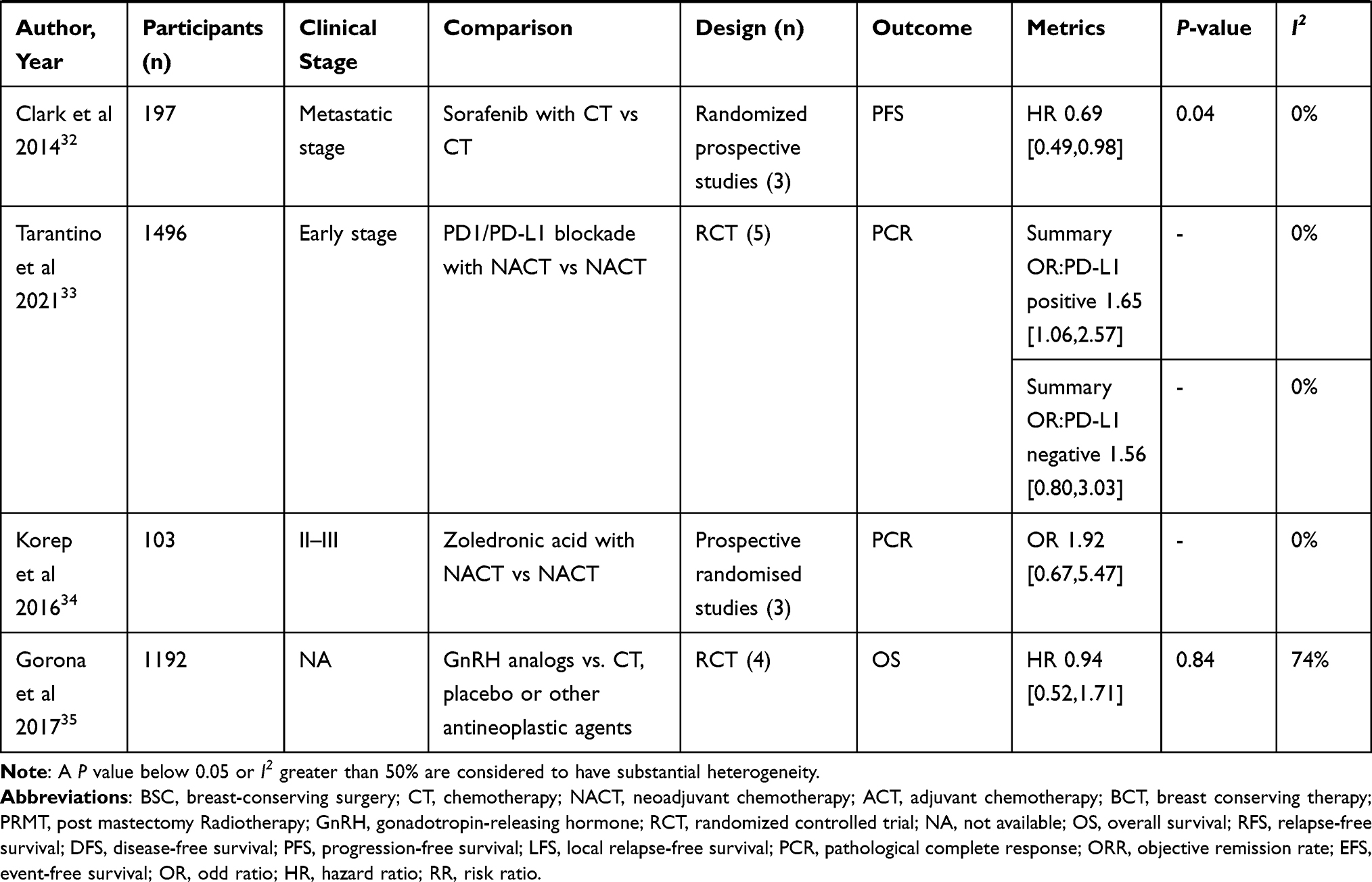 |
Table 2 Main Characteristics and Results of the Eligible Studies |
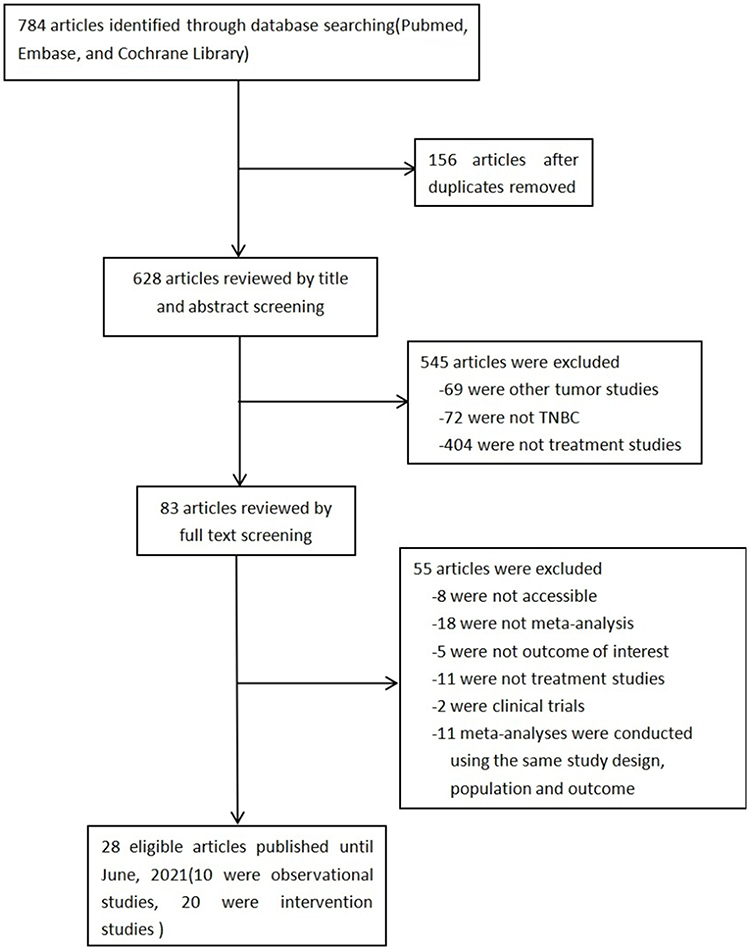 |
Figure 1 Flow chart of literature screening included in this study. |
Breast-Conserving Surgery Plus Radiotherapy versus Simple Mastectomy
Patients with TNBC with small tumor volume are more likely to choose breast-conserving surgery than simple mastectomy. After breast conserving surgery plus radiotherapy, the local recurrence rate, distant metastasis rate, and all-cause mortality of patients were significantly reduced.8 The local control rate in patients with TNBC after breast conserving surgery plus radiotherapy was similar to that of patients with non TNBC.9
CT versus Non-CT
Adjuvant CT combined with surgery reduced the risk of recurrence in patients (pT1abN0M0),10,11 and the OS was improved (HR = 0.72, 95% CI: 0.53–0.99);10 however, further analysis suggested that only T1b patients (rather than T1a) truly benefited from adjuvant CT.10,11
Neoadjuvant CT versus Adjuvant CT
Compared with adjuvant CT, neoadjuvant CT (NACT) led to no significant improvement in OS or DFS in patients with TNBC. However, when PCR was achieved after NACT, the OS and DFS were significantly improved. The OS was lower when there were residual lesions after neoadjuvant therapy (HR = 1.18, 95% CI: 1.09–1.28).12
Compared with patients with non TNBC, patients with TNBC had higher PCR rates after NACT (OR = 3.10, 95% CI: 2.51–3.82), and DFS and OS were significantly improved in patients with PCR. The PCR rate in patients with TNBC with high Ki-67 expression was higher than that in patients with low Ki-67 expression (OR = 9.87, 95% CI: 3.53–27.62).13
Platinum Chemotherapy
Platinum-based NACT significantly improved the PCR rate in patients with TNBC patients (OR = 2.12, 95% CI: 1.64–2.73) compared with non-platinum-based NACT14. There was no significant difference in ORR between platinum-containing and platinum-free NACT (RR = 1.11, 95% CI: 0.96, 1.29),15 and there was no significant improvement in long-term survival.16 Compared with non platinum containing chemotherapy, Platinum-based CT significantly increased ORR (OR = 2.34, 95% CI: 1.66–3.28) in patients with metastatic TNBC17 and slightly improved OS and PFS in patients with metastatic TNBC.18 Compared with patients with non TNBC, the PCR rate of patients with TNBC was significantly better after NACT (OR = 2.89, 95% CI: 1.28–6.53). There was no significant difference in PFS between patients with advanced or metastatic TNBC and non TNBC after platinum therapy.19 For patients with TNBC with BRCA mutation, platinum-containing neoadjuvant therapy did not significantly improve the PCR rate.20,21
Capecitabine Chemotherapy
Adding capecitabine to the CT regimen can significantly improve DFS and OS in patients with early TNBC.22–24 However, in the subgroup analysis of DFS, patients treated with adjuvant CT containing capecitabine benefited significantly, while patients with NACT did not improve.22 In patients with metastatic TNBC, there was no significant benefit in OS and PFS in patients treated with capecitabine CT. There was no significant improvement in OS in patients treated with capecitabine alone (HR = 1.19, 95% CI: 0.98–1.45).25
Radiotherapy
For patients with TNBC, whether they underwent breast conserving surgery or mastectomy, adjuvant radiotherapy significantly reduced the risk of local recurrence. However, it was not relevant in terms of overall survival. Nevertheless, patients with early-stage disease and young patients may benefit from it.26
Targeted Therapy
NACT with bevacizumab improved the PCR rate in patients with TNBC (RR = 1.30, 95% CI: 1.16–1.45).27 In patients with locally progressive TNBC, DFS was also significantly improved after bevacizumab treatment (HR = 0.88, 95% CI: 0.78–0.98).28 CT containing bevacizumab can significantly improve PFS.29 OS was improved in patients with metastatic TNBC, but the result was not statistically significant (HR = 0.96, 95% CI: 0.79–1.16).30
Poly (ADP-ribose) polymerase inhibitors (PARPis) can improve PFS in patients with advanced TNBC (OR = 0.39, 95% CI: 0.24–0.63).31 Moreover, patients with BRCA1/2 mutations and patients who have not received platinum therapy can benefit more from PARPis therapy.31 Sorafenib plus CT can improve PFS in patients with metastatic TNBC (HR = 0.69, 95% CI: 0.49–0.98).32
Immunotherapy
Adding a programmed death ligand 1 (PD-L1) inhibitor to NACT can improve the PCR rate in patients with early PD-L1-positive TNBC (summary OR = 1.65, 95% CI: 1.06–2.57).33
Other Therapies
For patients with premenopausal TNBC, treatment with NACT plus zoledronic acid non-significantly increased the PCR rate (OR = 1.92, 95% CI: 0.67–5.47).34
Compared with other anti-tumor drugs and placebo, GnRH analog based treatment non-significantly improved OS in patients with TNBC (HR = 0.94, 95% CI: 0.52–1.71). PFS was also not improved.35
Evidence Rating
The results of evidence evaluation showed that platinum-containing NACT improved PCR rate, platinum-containing CT improved ORR and OS for patients with metastatic disease, capecitabine-containing adjuvant CT improved DFS and OS; bevacizumab-containing NACT improved PCR rate, and programmed death 1 (PD-1)/PD-L1 blockade-containing NACT improved PCR rate. Probable evidence showed that NACT improved PCR rate for patients with high Ki67 expression. There was suggestive evidence that breast-conserving therapy reduced local recurrence and distant metastasis and improved OS; CT reduced the disease recurrence rate and improved OS for patients with pT1abN0M0 TNBC; NACT improved DFS and OS; platinum-containing CT improved PFS for metastatic disease, platinum-containing NACT improved PCR rate for patients with BRCA mutation; capecitabine-containing regimens improved OS and PFS for patients with metastatic disease; radiotherapy reduced local recurrence and improved OS; bevacizumab-containing CT improved PFS for patients with metastatic disease; and GnRH analogs improved OS. However, other evidence is limited (Table 3).
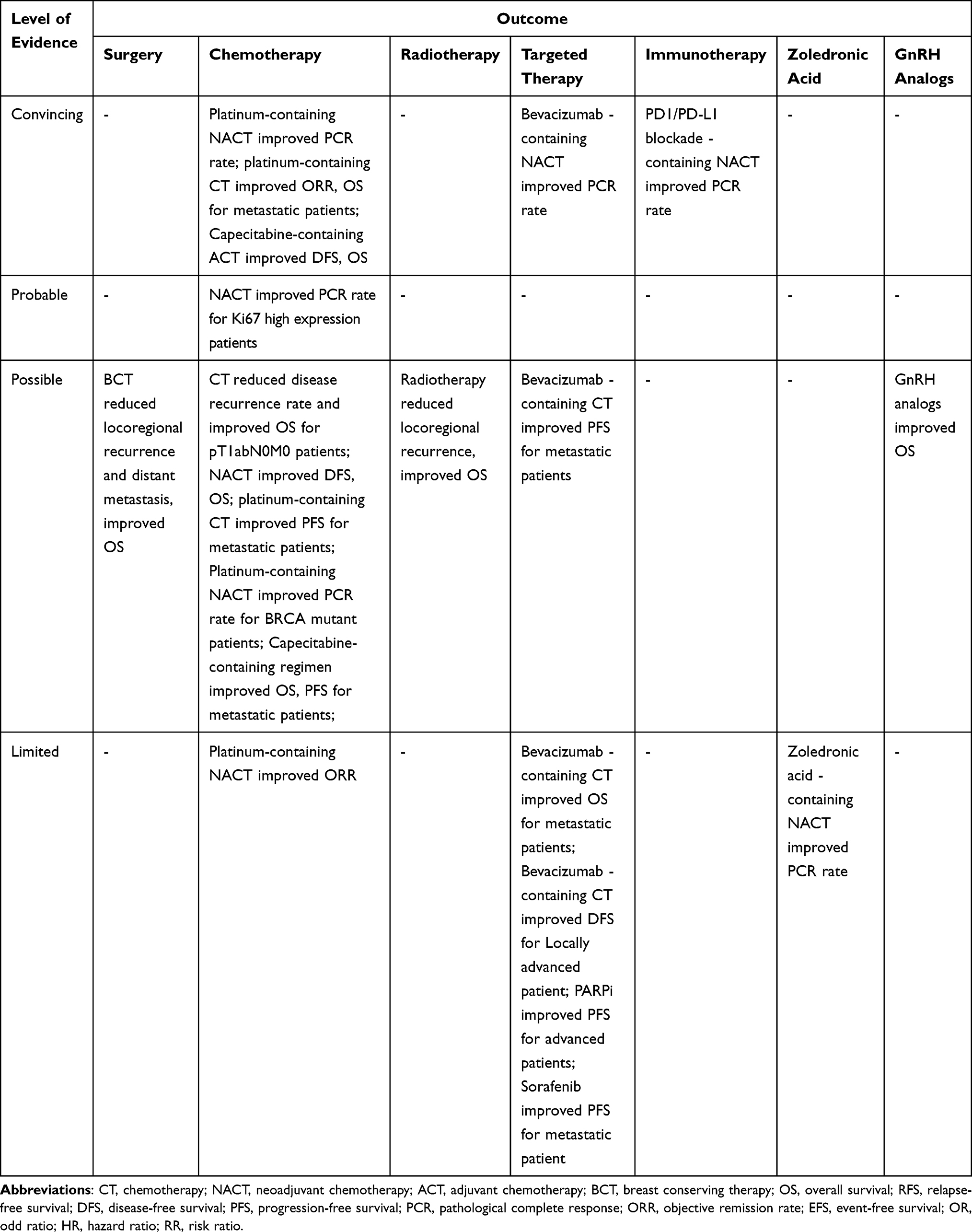 |
Table 3 Evidence from Studies of Treatment for TNBC |
Discussion
TNBC has special pathological and biological characteristics. It is a disease with poor prognosis. At present, surgery combined with conventional CT cannot meet the survival needs of patients. Patients with TNBC have clinical characteristics such as young onset age and large tumor volume. NACT improves the opportunities for surgical resection and breast conserving surgery36 and reduces the scope of surgery. It is also a frequently selected scheme clinically. The main end point of treatment is to achieve PCR. At present, anthracycline combined with taxane is commonly used clinically; however, long-term use can lead to drug resistance. Studies have shown that adding platinum37 or capecitabine,38 to the above CT regimen can benefit patients with TNBC. Other studies have suggested that targeted therapeutic drugs, such as PARPis,39 bevacizumab,40 sorafenib41 and PD-L1 inhibitors42 also have certain curative effects on patients with TNBC. However, the clinical stages most benefitting from these treatments and the specific benefits of patients need to be further studied.
A comparative analysis of interventional methods for TNBC was summarized in this umbrella evaluation. It was found that platinum, bevacizumab, and immunotherapy improved PCR rate in neoadjuvant therapy; platinum improved ORR and OS in metastatic TNBC; and capecitabine improved DFS and OS as part of adjuvant therapy.
Platinum compounds, as a DNA crosslinking agent, cross connect with DNA after entering tumor cells, interfere with tumor cell DNA replication, lead to tumor cell DNA double strand break, and play an anti-tumor role. Studies have shown that platinum-containing CT can be used as an option for anthracycline and taxus resistant patients.37 Its advantages in improving the PCR rate of patients with TNBC as part of neoadjuvant therapy and improving long-term survival in patients with metastatic disease have also been confirmed in some other relevant studies.15–17,43–45
Capecitabine, as an oral drug for fluorouracil, has often been used in metastatic breast cancer or after anthracycline or taxane treatment.46 Some studies suggest that capecitabine can benefit patients with TNBC treated with anthracycline combined with taxane.38 This review showed that it has certain benefits in improving the long-term survival of early-stage patients, especially as an adjuvant treatment. Jiang et al also drew a similar conclusion in their studies.47
Bevacizumab is a monoclonal antibody against vascular endothelial growth factor receptor (VEGF). It can bind to VEGF-A, block VEGF, and lose its biological activity. In the studies of Ma et al, it was also found that adding bevacizumab to NACT regimens can improve the PCR rate of patients.48
Immunotherapy may play an anticancer role by activating T cell autoimmunity in human body. PD-1 and PD-L1 are co-inhibitory molecules expressed on the surface of a variety of tumor cells. PD-1, as a key cell surface receptor, triggers the activation of inhibitory pathways by binding with its ligand, PD-L1, thereby inhibiting the T-cell response.49 PD-(L)1 blockade can block the immune escape of tumor cells mediated by PD-1 and PD-L1. Monoclonal antibodies against PD-1/PD-L1 immune checkpoints have become a new tumor treatment strategy. The current analysis results suggest that such an approach has certain advantages in the neoadjuvant treatment of PD-L1-positive TNBC.
Other interventions, such as breast-conserving surgery, radiotherapy, zoledronic acid, GnRH inhibitors, targeted drugs such as sorafenib and PARPis, have also achieved some favorable results. However, due to the retrospective design or small sample size of some studies, the results of some studies have obvious heterogeneity and other problems, the level of evidence in this analysis is low. Therefore, further research is needed.
In recent years, we have a deeper understanding of the typing and molecular biological characteristics of different subtypes of TNBC. Lehmann et al50 divided TNBC into six subtypes including 2 basal-like (BL1 and BL2), an immunomodulatory (IM), a mesenchymal (M), a mesenchymal stem-like (MSL), and a luminal androgen receptor (LAR) subtype. However, Jiang et al51 divided TNBC into four transcriptome-based subtypes: luminal androgen receptor (LAR), immunomodulatory (IM), basal-like immune-suppressed (BLIS), and mesenchymal-like (MES). Putative therapeutic targets or biomarkers were identified among each subtype; the comprehensive profile of TNBCs provided here will serve as a reference to further advance the understanding and precision treatment of TNBC. Compared with the European and American patients, premenopausal African American women with breast cancer have higher morbidity and mortality of TNBC.52 On the one hand, the reason is that their proportion of receiving surgery and chemotherapy is relatively low; on the other hand, factors such as tumor microenvironment or tumor biological characteristics also play an important role.53 The study found that,54,55 African American TNBC women are more likely to resist chemotherapy after neoadjuvant chemotherapy than white women, resulting in a lower pathological complete remission rate. Studies have shown that different molecular subtypes, genomic structure and cellular microenvironment may lead to different response and prognosis of TNBC to chemotherapy.56,57 However, there were not the relevant meta-analysis literatures regarding treatment comparison for different molecular subtypes and races of TNBC.
At present, precision therapy is formulated based on TNBC molecular typing, and better outcomes have been achieved in some studies.58,59 In the future, more efforts should be devoted to the in-depth exploration of precise treatment based on molecular typing, and more reliable meta-analysis articles are also expected, which is conducive to the individualized treatment of TNBC patients.
Conclusion
TNBC is a heterogeneous disease with poor prognosis. In this study, we comprehensively reviewed the meta-analysis literature of various treatment methods of TNBC and defined the evidence level of each comparison to determine the reliability of the analyses. The results showed that only some analyses of platinum, capecitabine, bevacizumab, and immune checkpoint inhibitors were supported by convincing evidence. Many studies are low-level evidence, because there are various adverse factors in these studies, including retrospective, small sample size, short follow-up time, and other biases. However, we did not find out the relevant meta-analysis literatures regarding different molecular subtypes and races of TNBC treatment. Therefore, more rigorous and detailed researches on the treatment of TNBC are needed in the future to obtain more reliable clinical evidence.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethical Statement
Ethics statement was not required since the research is an umbrella review of previously published studies.
Acknowledgments
We thank all authors whose publications could be included in our review.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This manuscript did not receive any funding.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33. doi:10.3322/caac.21654
2. Rakha EA, El-Sayed ME, Green AR, et al. Prognostic markers in triple-negative breast cancer. Cancer. 2007;109:25–32. doi:10.1002/cncr.22381
3. Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathologic features, patterns of recurrence, and survival among women with triple-negative breast cancer in the national comprehensive cancer network. Cancer. 2012;118:5463–5472. doi:10.1002/cncr.27581
4. Hudis CA, Gianni L. Triple-negative breast cancer: an unmet medical need. Oncologist. 2011;1:1–11. doi:10.1634/theoncologist.2011-S1-01
5. Sharma P. Biology and management of patients with triple-negative breast cancer. Oncologist. 2016;21:1050–1062. doi:10.1634/theoncologist.2016-0067
6. Kumar P, Aggarwal R. An overview of triple-negative breast cancer. Arch Gynecol Obstet. 2015;293:247–269. doi:10.1007/s00404-015-3859-y
7. World Health Organization. Population nutrient intake goals for preventing diet-related chronic diseases. Geneva: World Health Organization. Availablr from: http://www.who.int/nutrition/topics/5_population_nutrient/en/.
8. Fancellu A, Houssami N, Sanna V, et al. Outcomes after breast-conserving surgery or mastectomy in patients with triple-negative breast cancer: meta-analysis. Br J Surg. 2021;108:760–768. doi:10.1093/bjs/znab145
9. Pan XB, Qu S, Jiang YM, et al. Triple negative breast cancer versus non-triple negative breast cancer treated with breast conservation surgery followed by radiotherapy: a systematic review and meta-analysis. Breast Care. 2015;10:413–416. doi:10.1159/000441436
10. Petrelli F, Parati MC, Borgonovo K, et al. Adjuvant chemotherapy for pT1abN0M0 triple-negative breast cancer: a systematic review and meta-analysis of published studies. Eur J Cancer. 2021;147:151–153. doi:10.1016/j.ejca.2021.01.030
11. An X, Lei X, Huang R, et al. Adjuvant chemotherapy for small, lymph node-negative, triple-negative breast cancer: a single-center study and a meta-analysis of the published literature. Cancer. 2020;126:3837–3846. doi:10.1002/cncr.32878
12. Xia LY, Hu QL, Zhang J, et al. Survival outcomes of neoadjuvant versus adjuvant chemotherapy in triple-negative breast cancer: a meta-analysis of 36,480 cases. World J Surg Oncol. 2020;18:129. doi:10.1186/s12957-020-01907-7
13. Tian M, Zhong Y, Zhou F, et al. Effect of neoadjuvant chemotherapy in patients with triple-negative breast cancer: a meta-analysis. Oncol Lett. 2015;9:2825–2832. doi:10.3892/ol.2015.3072
14. Wang D, Feng J, Xu B. A meta-analysis of platinum-based neoadjuvant chemotherapy versus standard neoadjuvant chemotherapy for triple-negative breast cancer. Future Oncol. 2019;15:2779–2790. doi:10.2217/fon-2019-0165
15. Wang LY, Xie H, Zhou H, et al. Efficacy of carboplatin-based preoperative chemotherapy for triple-negative breast cancer. A meta-analysis of randomized controlled trials. Saudi Med J. 2017;38:18–23. doi:10.15537/smj.2017.1.14969
16. Poggio F, Bruzzone M, Ceppi M, et al. Platinum-based neoadjuvant chemotherapy in triple-negative breast cancer: a systematic review and meta-analysis. Ann Oncol. 2018;29:1497–1508. doi:10.1093/annonc/mdy127
17. Lu F, Hou Y, Chen Z, et al. Efficacy and safety of platinum-based chemotherapy as first-line therapy for metastatic triple-negative breast cancer: a meta-analysis of randomized controlled trials. Technol Cancer Res Treat. 2021;20:1–10. doi:10.1177/15330338211016369
18. Egger SJ, Chan MMK, Luo Q, et al. Platinum-containing regimens for triple-negative metastatic breast cancer. Cochrane Database Syst Rev. 2020;10:D13750. doi:10.1002/14651858.CD013750
19. Liu M, Mo QG, Wei CY, et al. Platinum-based chemotherapy in triple-negative breast cancer: a meta-analysis. Oncol Lett. 2013;5:983–991. doi:10.3892/ol.2012.1093
20. Caramelo O, Silva C, Caramelo F, et al. The effect of neoadjuvant platinum-based chemotherapy in mutated triple negative breast cancers -systematic review and meta-analysis. Hered Cancer Clin Pract. 2019;17:11. doi:10.1186/s13053-019-0111-y
21. Wang CJ, Xu Y, Lin Y, et al. Platinum-based neoadjuvant chemotherapy for breast cancer with BRCA mutations: a meta-analysis. Front Oncol. 2020;10:592998. doi:10.3389/fonc.2020.592998
22. Huo X, Li J, Zhao F, et al. The role of capecitabine-based neoadjuvant and adjuvant chemotherapy in early-stage triple-negative breast cancer: a systematic review and meta-analysis. BMC Cancer. 2021;21:78. doi:10.1186/s12885-021-07791-y
23. Li Y, Zhou Y, Mao F, et al. Adjuvant addition of capecitabine to early-stage triple-negative breast cancer patients receiving standard chemotherapy: a meta-analysis. Breast Cancer Res Treat. 2020;179:533–542. doi:10.1007/s10549-019-05513-4
24. Xu D, Chen X, Li X, et al. Addition of capecitabine in breast cancer first-line chemotherapy improves survival of breast cancer patients. J Cancer. 2019;10:418–429. doi:10.7150/jca.29739
25. Hoon SN, Lau PK, White AM, et al. Capecitabine for hormone receptor-positive versus hormone receptor-negative breast cancer. Cochrane Database Syst Rev. 2021;5:D11220. doi:10.1002/14651858.CD011220.pub2
26. O’Rorke MA, Murray LJ, Brand JS, et al. The value of adjuvant radiotherapy on survival and recurrence in triple-negative breast cancer: a systematic review and meta-analysis of 5507 patients. Cancer Treat Rev. 2016;47:12–21. doi:10.1016/j.ctrv.2016.05.001
27. Nahleh Z, Botrus G, Dwivedi A, et al. Bevacizumab in the neoadjuvant treatment of human epidermal growth factor receptor 2-negative breast cancer: a meta-analysis of randomized controlled trials. Mol Clin Oncol. 2019;10:357–365. doi:10.3892/mco.2019.1796
28. Alnimer Y, Hindi Z, Katato K. The effect of perioperative bevacizumab on disease-free and overall survival in locally advanced HER-2 negative breast cancer: a meta-analysis. Breast Cancer. 2018;12:1–11. doi:10.1177/1178223418792250
29. Bramati A, Girelli S, Torri V, et al. Efficacy of biological agents in metastatic triple-negative breast cancer. Cancer Treat Rev. 2014;40:605–613. doi:10.1016/j.ctrv.2014.01.003
30. Miles DW, Diéras V, Cortés J, et al. First-line bevacizumab in combination with chemotherapy for HER2-negative metastatic breast cancer: pooled and subgroup analyses of data from 2447 patients. Ann Oncol. 2013;24:2773–2780. doi:10.1093/annonc/mdt276
31. Chen Z, Wang X, Li X, et al. Deep exploration of PARP inhibitors in breast cancer: monotherapy and combination therapy. J Int Med Res. 2021;49:1221790571. doi:10.1177/0300060521991019
32. Clark O, Botrel TE, Paladini L, et al. Targeted therapy in triple-negative metastatic breast cancer: a systematic review and meta-analysis. Core Evid. 2014;9:1–11. doi:10.2147/CE.S52197
33. Tarantino P, Gandini S, Trapani D, et al. Immunotherapy addition to neoadjuvant chemotherapy for early triple negative breast cancer: a systematic review and meta-analysis of randomized clinical trials. Crit Rev Oncol Hematol. 2021;159:103223. doi:10.1016/j.critrevonc.2021.103223
34. Kroep JR, Charehbili A, Coleman RE, et al. Effects of neoadjuvant chemotherapy with or without zoledronic acid on pathological response: a meta-analysis of randomised trials. Eur J Cancer. 2016;54:57–63. doi:10.1016/j.ejca.2015.10.011
35. Corona SP, Roviello G, Strina C, et al. Could gonadotropin-releasing hormone analogs be helpful in the treatment of triple-negative breast cancer? Future Oncol. 2017;13:2473–2477. doi:10.2217/fon-2017-0272
36. King TA, Morrow M. Surgical issues in patients with breast cancer receiving neoadjuvant chemotherapy. Nat Rev Clin Oncol. 2015;12:335–343. doi:10.1038/nrclinonc.2015.63
37. Minckwitz GV, Schneeweiss A, Loibl S, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised Phase 2 trial. Lancet Oncol. 2014;15:747–756. doi:10.1016/S1470-2045(14)70160-3
38. Jassem J. Highlights from the San Antonio breast cancer symposium 2015. ESMO Open. 2016;1:e43. doi:10.1136/esmoopen-2016-000043
39. Geenen JJJ, Linn SC, Beijnen JH, et al. PARP inhibitors in the treatment of triple-negative breast cancer. Clin Pharmacokinet. 2018;57:427–437. doi:10.1007/s40262-017-0587-4
40. Sikov WM, Berry DA, Perou CM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (alliance). J Clin Oncol. 2015;33:13–21. doi:10.1200/JCO.2014.57.0572
41. Gradishar WJ, Kaklamani V, Sahoo TP, et al. A double-blind, randomised, placebo-controlled, phase 2b study evaluating sorafenib in combination with paclitaxel as a first-line therapy in patients with HER2-negative advanced breast cancer. Eur J Cancer. 2013;49:312–322. doi:10.1016/j.ejca.2012.08.005
42. Schmid P, Adams S, Rugo HS, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379:2108–2121. doi:10.1056/NEJMoa1809615
43. Pandy JGP, Balolong-Garcia JC, Cruz-Ordinario MVB, et al. Triple negative breast cancer and platinum-based systemic treatment: a meta-analysis and systematic review. BMC Cancer. 2019;19:1065. doi:10.1186/s12885-019-6253-5
44. Li ZY, Zhang Z, Cao XZ, et al. Platinum-based neoadjuvant chemotherapy for triple-negative breast cancer: a systematic review and meta-analysis. J Int Med. 2020;48:1220763892. doi:10.1177/0300060520964340
45. Kaya V, Yildirim M, Yazici G, et al. of platinum-based treatment for triple negative metastatic breast cancer: a meta-analysis. Asian Pac J Cancer Prev. 2018;19:1169–1173. doi:10.22034/APJCP.2018.19.5.1169
46. O’Shaughnessy J, Miles D, Vukelja S, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: Phase III trial results. J Clin Oncol. 2002;20:2812–2823. doi:10.1200/JCO.2002.09.002
47. Jiang Y, Yin W, Zhou L, et al. First efficacy results of capecitabine with anthracycline- and taxane-based adjuvant therapy in high-risk early breast cancer: a meta-analysis. PLoS One. 2012;7:e32474. doi:10.1371/journal.pone.0032474
48. Ma X, Wang X, Huang J, et al. Bevacizumab addition in neoadjuvant treatment increases the pathological complete response rates in patients with her-2 negative breast cancer especially triple negative breast cancer: a meta-analysis. PLoS One. 2016;11:e160148. doi:10.1371/journal.pone.0160148
49. Marmé F, Schneeweiss A. Targeted therapies in triple-negative breast cancer. Breast Care. 2015;10:159–166. doi:10.1159/000433622
50. Lehmann BD, Bauer JA, Chen X, et al. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest. 2011;121:2750–2767. doi:10.1172/JCI45014
51. Jiang YZ, Ma D, Suo C, et al. Genomic and transcriptomic landscape of triple-negative breast cancers: subtypes and treatment strategies. Cancer Cell. 2019;35:428–440. doi:10.1016/j.ccell.2019.02.001
52. Carey LA, Perou CM, Livasy CA, et al. Race, breast cancer subtypes, and survival in the Carolina breast cancer study. JAMA. 2006;295:2492–2502. doi:10.1001/jama.295.21.2492
53. Cho B, Han Y, Lian M, et al. Evaluation of racial/ethnic differences in treatment and mortality among women with triple-negative breast cancer. JAMA Oncol. 2021;7:1016–1023. doi:10.1001/jamaoncol.2021.1254
54. Killelea BK, Yang VQ, Wang SY, et al. Racial differences in the use and outcome of neoadjuvant chemotherapy for breast cancer: results from the national cancer data base. J Clin Oncol. 2015;33:4267–4276. doi:10.1200/JCO.2015.63.7801
55. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384:164–172. doi:10.1016/S0140-6736(13)62422-8
56. Nedeljkovic M, Damjanovic A. Mechanisms of chemotherapy resistance in triple-negative breast cancer-how we can rise to the challenge. Cells. 2019;8:957. doi:10.3390/cells8090957
57. Filho OM, Stover DG, Asad S, et al. Association of immunophenotype with pathologic complete response to neoadjuvant chemotherapy for triple-negative breast cancer: a secondary analysis of the brightness phase 3 randomized clinical trial. JAMA Oncol. 2021;7:603–608. doi:10.1001/jamaoncol.2020.7310
58. Jiang YZ, Liu Y, Xiao Y, et al. Molecular subtyping and genomic profiling expand precision medicine in refractory metastatic triple-negative breast cancer: the FUTURE trial. Cell Res. 2021;31:178–186. doi:10.1038/s41422-020-0375-9
59. Vagia E, Mahalingam D, Cristofanilli M. The landscape of targeted therapies in TNBC. Cancers. 2020;12:916. doi:10.3390/cancers12040916
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.