")
Back to Journals » Patient Preference and Adherence » Volume 13
Treatment Adherence And Persistence Among HIV-1 Patients Newly Starting Treatment
Authors Hines DM, Ding Y, Wade RL , Beaubrun A, Cohen JP
Received 9 March 2019
Accepted for publication 1 August 2019
Published 7 November 2019 Volume 2019:13 Pages 1927—1939
DOI https://doi.org/10.2147/PPA.S207908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Dionne M Hines,1 Yao Ding,1 Rolin L Wade,1 Anne Beaubrun,2 Joshua P Cohen3
1Health Economics and Outcomes Research, IQVIA Inc, Plymouth Meeting, PA, USA; 2Health Economics and Outcomes Research, Gilead Sciences Inc, Foster City, CA, USA; 3Institute for Clinical Research and Health Policy Studies, Tufts University, Boston, MA, USA
Correspondence: Rolin L Wade
IQVIA Inc., One IMS Drive, Plymouth Meeting, PA 19462, USA
Tel +1 215 434 812 2958
Email [email protected]
Objective: To assess adherence and persistence with first-line single-tablet regimen (STR) and multi-tablet regimen (MTR) antiretroviral therapy (ART) in newly treated HIV-1 patients.
Methods: Retrospective analysis of longitudinal pharmacy claims among US patients initiating ART between 1/1/2016 and 5/31/2016 (index date was defined by first ART claim for STRs, and fill date for the last therapy in the regimen for MTRs). Adherence was assessed over a 12-month period and reported as the proportion of adherent or non-adherent (defined as ≤5-day and > a 5-day gap between successive fills, respectively) patients. Sensitivity analysis using ≤7-day and ≤14-day gap thresholds to define adherence was performed. Persistence was assessed as the number of days on therapy from index until treatment discontinuation (>90 day gap in therapy). Kaplan–Meier curves and Cox Proportional Hazard models were generated to evaluate discontinuation rates. Assessments were performed on STRs vs MTRs overall and by regimen.
Results: Patients initiating ART (STR: n=10,623; MTR: n=2504) had a mean age of 42.8 years; 76.0% were male. STR patients were >2 times more likely to be adherent over 12 months than MTR patients (24.9% vs 11.7%, respectively). Patients using EVG/COBI/FTC/TAF had greater adherence than those using other STRs. Among MTRs, patients were more adherent with FTC/TDF+DTG (15.1%) than other MTRs. Persistence was also greater with STRs, with MTR patients being 61% more likely to discontinue therapy. Persistence was best for FTC/TAF-based regimens. Predictors of treatment discontinuation included younger age, female gender, and Medicare or Medicaid insurance type.
Conclusion: Patients receiving STRs were significantly less likely to discontinue therapy and were more adherent with their regimens, providing further evidence of greater adherence and persistence with STRs versus MTRs. However, there was a large proportion of patients who interrupted or discontinued treatment. Further research examining treatment patterns beyond first line is warranted.
Keywords: antiretroviral, HIV, adherence, persistence
Introduction
In 2015, approximately 40,000 individuals were newly diagnosed with HIV, bringing the prevalence to over 1.2 million in the United States (US).1 While the incidence of HIV has steadily declined over the past 10 years,2 it remains a serious public health concern given the burden it imposes on patients and the health care system.
The introduction of antiretroviral therapy (ART) agents revolutionized HIV treatment and substantially lowered mortality and morbidity in HIV patients.3–5 ART is recommended for all HIV patients with the primary goal of reducing HIV-associated mortality and morbidity. Early initiation of ART has demonstrated an increased survival benefit and delayed disease progression in randomized clinical trials.6,7 As a result, the Department of Health and Human Services (DHHS) guidelines for HIV treatment recommend early initiation of ART regardless of the disease stage in order to delay disease progression, prolong survival, decrease drug resistance, and prevent HIV transmission.8 These guidelines recommend initiating ART in treatment naïve patients with a regimen consisting of two nucleoside reverse transcriptase inhibitors (NRTIs) along with a third drug: either an integrase strand transfer inhibitor (INSTI), or a non-nucleoside reverse transcriptase inhibitor (NNRTI) or protease inhibitor (PI) as alternatives to INSTIs. The choice of therapy is based on factors such as virologic efficacy, co-morbid conditions, toxicity, and pill burden.8
After initiation, ART must be continued indefinitely. Adherence is considered to be one of the key factors in maintaining viral suppression and reducing the risk of drug resistance.8 Adherence is defined as the extent to which a patient conforms to the prescribed treatment in terms of timing, dose, and frequency of administration, and is a challenge for many patients.9 It has been observed that many patients experience interruptions in their ART regimen.10 As ART is composed of combination therapy with multiple agents, patients are frequently required to take 2 or more pills a day.11 These multi-tablet regimens (MTRs) have been found to be a barrier to adherence and a predictor of treatment discontinuation.12,13 However, drugs with longer half-life and fixed-dose combinations combining multiple antiretroviral drugs in a single pill (single-tablet regimens [STRs]) allow for simple, once-daily regimens. Results from randomized clinical trials and observational studies have shown that STRs are associated with higher adherence and persistence when compared with MTRs.11,14–18 In a recent meta-analysis, Altice et al found that STR use was associated with a 1.7 times higher likelihood of achieving ≥95% adherence compared to use of an MTR, even across different regions (US and EU) and using different measures of adherence. In turn, higher adherence was related to increased viral suppression in most of the studies evaluated.19 Adherence has also been found to be associated with tolerability and the ART class of therapy a patient is prescribed. Patients who experience an adverse event are more likely to discontinue their regimen or switch to a different regimen.20 Additionally, patients treated with INSTI-based regimens have been found to have better persistence, while discontinuations have been observed more frequently amongst patients treated with NRTI regimens.20,21
Adherence to ART is a critical determinant of survival, and the consequences of poor adherence include reduced viral suppression, hospitalization, higher risk of progression to AIDS, and reduced quality of life and survival.8,22–29 Persistence is defined as the duration of time from initiation to discontinuation of therapy which may be influenced by providers’ decisions to switch therapies, newly-available treatment options, patient behavior, or adverse events. A lack of persistence was found to be associated with the development of reduced viral suppression, disease progression, and mortality.30,31
While evidence shows that adherence and persistence are better with STRs than with MTRs, contemporary treatment options with greater potency and tolerability have become available since those data have been published. With the availability of newer antiretroviral regimens, there is a need to update the existing evidence in a large representative sample. Hence, the objectives of the current study were to (1) assess adherence with first-line STR and MTR regimens overall as well as with the individual regimens among treatment naïve patients, (2) evaluate persistence of first-line ART, and (3) determine the adjusted risk of discontinuation of ART across regimens.
Methods
Study Design And Data Source
This was a retrospective database analysis that involved the use of IQVIA’s US-based open-source point-of-service longitudinal pharmacy claims database (LRx). LRx captures information on adjudicated dispensed prescriptions sourced from retail (86% coverage), mail (55% coverage), long-term care, and specialty pharmacies (40–70% coverage). The data suppliers have direct, long-standing relationships with IQVIA, with many providing data on a daily basis. Information is available for over 150 million unique patients. Data are updated monthly with a reporting lag time of 30 days. All data are de-identified and Health Insurance Portability and Accountability Act (HIPAA) compliant to protect patient privacy. As this study was based on secondary analysis of de-identified data, Institutional Review Board approval was not required.
Patient Selection
This study included patients with at least two claims for one of the ARTs of interest (Table 1) between January 1, 2016 and May 31, 2016 (index window). For patients prescribed an STR, the index date was defined as the date of the first ART claim within the index window. For patients prescribed an MTR, the index date was defined as the claim date for the last-filled drug in the regimen. A window of ±5 days between fills for the agents in an MTR was allowed. The pharmacy dispensing the index prescription was required to have consistently submitted claims to the LRx database from 12 months prior to the index date until the end of the study (May 31, 2017). Patients were required to be 18 years of age or older on the index date, have no prescription claim for an ART during the 12-month period prior to the index date (thus capturing those newly starting treatment), and have no ART use other than the index drugs on the index date. Patients with missing information on age, gender, or prescription were not included (Figure 1).
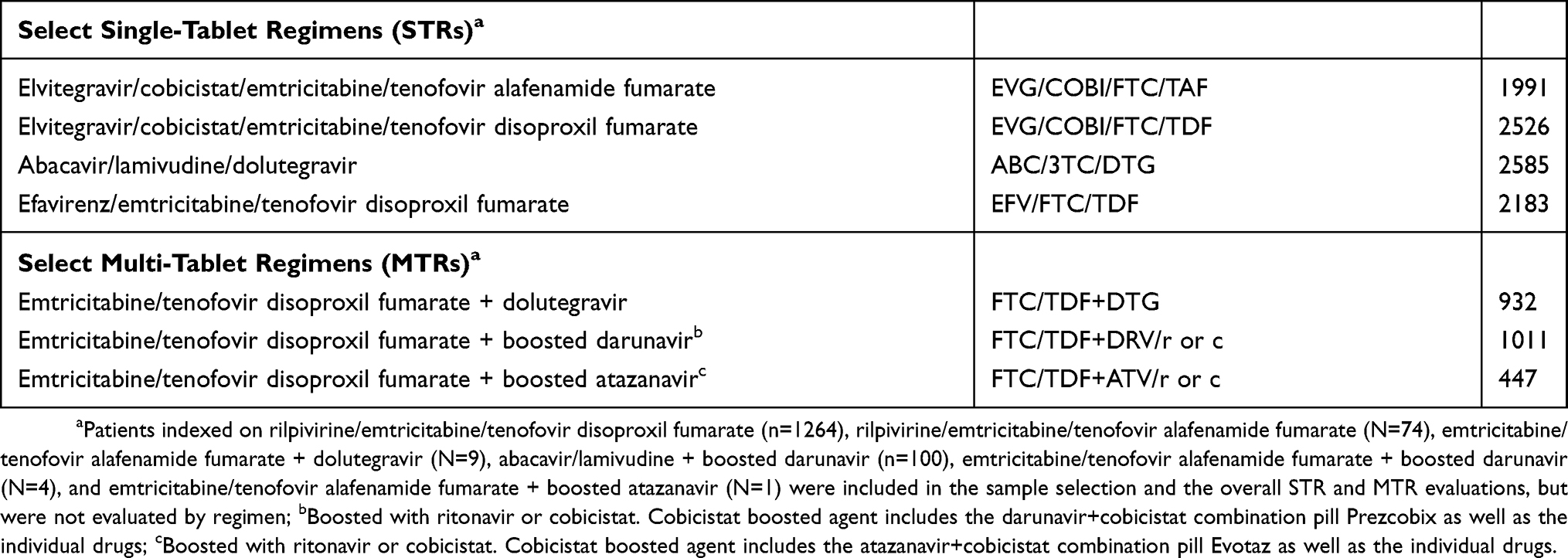 |
Table 1 Antiretroviral Regimens Of Interest |
Demographics And Outcome Measures
Baseline Patient Characteristics
Demographics, including age, gender, geographic region (Northeast, Midwest, South, West), and insurance type (commercial, Medicaid, Medicare Risk), were measured on the index date. Number of unique non-ART drugs filled on index date and proportion of patients with non-ART medication use (including antibiotics, anti-hypertensives, antidiabetics, lipid-lowering therapy, anticoagulant, and respiratory agents) during the 12-month pre-index period were also reported.
Adherence With ART
Adherence with ART was measured for STRs, MTRs, and the individual regimens on a monthly basis (30-day intervals) during a 12-month assessment period. Assessments were made for first-line therapy only. For MTRs, adherence was measured based on the number of days in which the patient had all drugs in the regimen on hand and was assessed separately for each drug in the regimen.
For each 30-day period within the 12-month assessment period, patients were classified as being adherent, non-adherent, or as having discontinued therapy. Adherence was defined as a ≤5-day gap between successive claims for STR (measured from the end of days’ supply of one claim and the date of the following claim) or ≤5 days in which one or more of the drugs in the regimen was not on hand for MTRs. The definition for adherence was based on previous studies of HIV patients that utilized a similar 4–5 days gap,32,33 as well as empirically from the distribution of the data. An examination of the distribution of days between fills showed that 75% of the patients filled within 5 days of the end of days’ supply of the prior fill.
Non-adherence was defined by a >5-day gap between claims. For patients with non-adherence, we estimated a refill gap as the number of days between claims. In cases where a patient had multiple claims within a 30-day period, the refill gap was reported as the sum of gap days in the 30-day period. A cumulative refill gap was calculated as the sum of the days in the gap over the 12-month assessment period. Once a patient met the requirement for non-adherence, they remained classified as non-adherent throughout the remainder of the assessment period. Thus, the final adherence assessment (made in month 12) represents patients who remained adherent throughout the 12-month assessment period, and patients with a >5-day gap between refills (non-adherent) at any time during the 12-month period. Patients were considered to have discontinued first-line therapy if a ≥90-day gap between fills was observed, which included patients who switched to a different ART regimen. This 90-day period was informed by the empirical distribution of refill gaps observed in the data. As restarts were not captured in this analysis, patients who restarted therapy after a ≥90-day gap remained classified as discontinued. As there is no clinically defined threshold for adherence, sensitivity analyses were performed by using different gap thresholds (≤7 and ≤14 days) to evaluate the impact of expanding the gap window on adherence to STR.
Persistence With ART
Persistence with STRs and MTRs was assessed overall and by treatment for the index therapy (i.e., the ART therapy initiated during the index period) only. Persistence was measured as the number of days on index therapy and the proportion of patients remaining on index therapy at 12 months post-index. Days on therapy were calculated from the index date until the first of treatment discontinuation (the end of days’ supply of the last claim for all therapies in the regimen) or the end of the data stream. A treatment gap of <90 days between refills was allowed. For MTRs, a ≥90-day gap for any drug in the regimen was considered a discontinuation of the regimen, and persistence required that patients must have remained on all drugs in the regimen. Observation of a claim for any agent not included in the index regimen or removal of an agent indicated a change to the index regimen and the end of the persistence period.
Statistical Analyses
All statistical analyses were performed using SAS® version 9.2 (Copyright © 2002–2008, SAS Institute Inc., Cary, NC). Chi-square tests were used to compare the proportion of patients adherent at 12 months of follow-up. Kaplan–Meier curves were used to estimate the time to discontinuation of index therapy, censoring patients who remained on therapy at the end of follow-up. Statistically significant differences in discontinuation of STRs vs MTRs and among the individual regimens were evaluated using the Log-rank test. Adjusted risk of discontinuation was assessed with Cox Proportional Hazard models. Separate models were constructed to generate hazard ratios (HRs) comparing STRs to MTRs, and also to compare individual STR regimens, as well as STR regimens to MTRs. Covariates included in the models were age group, gender, US geographic region, insurance type, baseline medications, and number of unique prescriptions on index date. All tests of statistical significance were evaluated using a significance level of 0.05.
Results
Patient Demographic And Clinical Characteristics
After applying inclusion and exclusion criteria, 13,127 patients were identified (STR = 10,623, MTR = 2504) (Figure 1). Patient baseline characteristics are shown in Table 2. The mean (SD) age of the study population was 42.8 (12.9) years (STR: 42.6 [13.0], MTR: 43.8 [12.4] years). There were more males than females for STRs (77.6%) and MTRs (69.1%); however, more females used MTRs (30.9%) than STRs (22.4%). The majority of patients were insured by a commercial payer (STR: 74.9%, MTR: 67.9%).
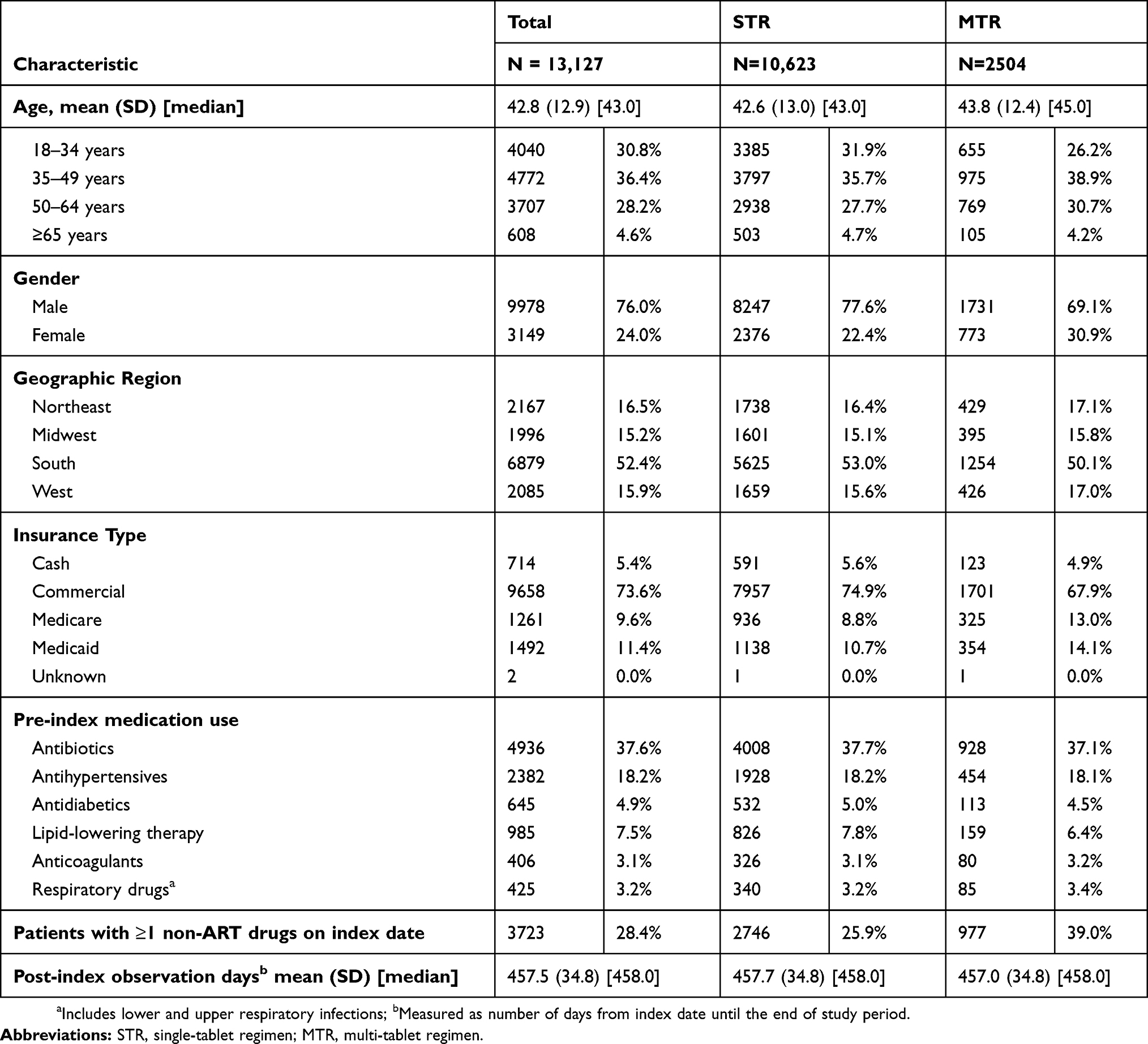 |
Table 2 Baseline Demographic And Clinical Characteristics |
In the 12 months prior to initiating ART, antibiotics were used by 37.6% of the patients and cardiovascular and metabolic drugs (antihypertensives, antidiabetics, lipid-lowering therapy, anticoagulants, and antiarrhythmic drugs) were used by 33.8% of the patients. Approximately 28.4% of the patients (STR: 25.9%, MTR: 39.0%) used ≥1 drug other than an ART on the index date. Patients initiating STR and MTR had similar post-index follow-up days (457.7 and 457.0 days) (Table 2).
Adherence
Adherence Over 12-Month Period
A greater proportion of patients receiving STR were consistently more adherent over 12 months than patients receiving MTR, with higher proportion of STR patients adherent at each 30-day interval (Figure 2A). The proportion of patients adherent to STR was consistently 10–15% higher than patients adherent to MTR at each 30-day interval. Over the 12 months, more than double the number of STR recipients remained adherent compared with MTR recipients (24.9% [95% CI: 24.08%, 25.72%] vs 11.7% [95% CI: 10.48%, 13.0%]; p<0.0001). Among those who discontinued or switched therapy, 40.3% were on STRs vs 57.7% of the MTR recipients.
By regimen type, EVG/COBI/FTC/TAF regimen had consistently more adherent patients over 12 months than other regimens (Figure 2B). This trend of higher adherence held throughout each 30-day interval, with a higher proportion of EVG/COBI/FTC/TAF recipients adherent compared to every other regimen. Differences in the proportion of adherent patients by regimen became evident by month 3 (61–90-day interval) and persisted through 12 months. The proportions of STR patients who remained adherent at 12 months were EVG/COBI/FTC/TAF: 32.04% (95% CI: 29.99%, 34.09%), EVG/COBI/FTC/TDF: 18.92% (95% CI: 17.40%, 20.45%), ABC/3TC/DTG: 30.02% (95% CI: 28.25%, 31.79%), and EFV/FTC/TDF: 23.18% (95% CI: 21.41%, 24.95%); p<0.0001. Among MTRs, the proportions remaining adherent at 12 months were FTC/TDF+DTG: 15.13% (12.83%, 17.43%), FTC/TDF+DRV combo: 12.18% (8.91%, 15.44%), FTC/TDF+DRV/r,c: 9.28% (7.01%, 11.55%); FTC/TDF/ATV combo: 10.87% (1.87%, 19.86%), and FTC/TDF+ATV/r,c: 8.73% (5.97%, 11.49%); p=0.002.
Sensitivity Analyses On STR Adherence Definition
Sensitivity analyses using an adherence definition of ≤7 gap days between successive fills yielded similar adherence rates as the base case definition (≤5 days), with 27.7% (n=2937) of patients maintaining adherence throughout the 12-month period and 32.1% (n=3407) classified as non-adherent. Higher adherence rates were noted when a ≤14-day gap was allowed: 34.5% (n=3664) patients maintained adherence and 25.2% (n=2,680) were non-adherent by month 12. Consistent with the base case, EVG/COBI/FTC/TAF had the highest proportion of adherent patients among the STRs when the ≤7 and ≤14-day gaps were applied.
Persistence
Persistence With STR Vs MTR Overall
Patients who initiated ART with an STR experienced longer persistent days (unadjusted mean [SD]) than patients initiating therapy with an MTR (316.3 [156.9] vs 259.1 [156.5] days, respectively). Congruently, Kaplan–Meier estimates revealed a significantly longer time to treatment discontinuation for STR patients than for MTR patients (p<0.0001) (Figure 3A). In adjusted analyses controlling for age group, gender, geographic region, insurance type, baseline medications, and number of unique prescriptions on index date, patients on MTRs were 61% more likely to discontinue treatment than patients with STRs (HR: 1.61 [95% CI: 1.53, 1.71]) (Figure 4). Significant predictors of discontinuation in the adjusted models included age (with patients age 18–34 having a higher risk of discontinuation than patients ≥65 years; HR: 1.19 [95% CI: 1.05, 1.35]), gender (with females having a higher risk of discontinuation than males; HR: 1.20 [95% CI: 1.14, 1.27]), insurance type (with patients with Medicare or Medicaid coverage having a higher risk of discontinuation than patients covered by a commercial payer; HR: 1.08 [95% CI: 1.02, 1.14]), and baseline medication use (with patients using antibiotics [HR: 0.89 (95% CI: 0.85, 0.93)] and lipid-lowering therapies [HR: 0.88 (95% CI: 0.79, 0.98)] being less likely to discontinue therapy).
Comparison Of Persistence By Regimen
Kaplan–Meier estimates of discontinuation of the individual regimens yielded a statistically significant difference in time to discontinuation between the therapies (p<0.0001), with EVG/COBI/FTC/TAF having the longest time to discontinuation (Figure 3B).
Among the individual STRs, adjusted analysis indicated that compared to EVG/COBI/FTC/TAF, EVG/COBI/FTC/TDF patients were nearly twice as likely to discontinue therapy (HR: 1.92 [95% CI: 1.76–2.09]), and that the risk of treatment discontinuation was approximately 13% higher with ABC/3TC/DTG (HR: 1.13 [95% CI: 1.03–1.24]), and approximately 65% higher with EFV/FTC/TDF (HR: 1.65 [95% CI: 1.50–1.81]). Compared to ABC/3TC/DTC, discontinuation of an STR was 71% greater with EVG/COBI/FTC/TDF (HR: 1.71 [95% CI: 1.58–1.85]) and 47% greater with EFV/FTC/TDF (HR: 1.47 [95% CI: 1.35–1.60]) (Figure 4).
Comparing STRs with MTRs, the risk of discontinuing FTC/TDF+DTG was approximately twice as common as the risk of discontinuing ABC/3TC/DTG (HR: 1.96 [95% CI: 1.77–2.17]), and EVG/COBI/FTC/TAF (HR: 2.21 [95% CI: 1.98–2.47]). Additionally, the risk of discontinuation was 16% to 30% more common for FTC/TDF+DTG (HR: 1.16 [95% CI: 1.05–1.27]), FTC/TDF+DRV/r or c (HR: 1.22 [95% CI: 1.11–1.33]), and FTC/TDF+ATV/r or c (HR: 1.30 [95% CI: 1.15–1.47]) than for EVG/COBI/FTC/TDF.
With respect to NRTI backbones, there was a 17% greater risk of discontinuing ABC/3TC-based regimens (HR: 1.17 [95% CI: 1.07–1.28]), and about 2 times greater risk of discontinuing FTC/TDF regimens (HR: 1.94 [95% CI: 1.79–2.09]) compared to FTC/TAF regimens. In addition, there was a 63% greater risk of discontinuing FTC/TDF (HR: 1.63 [95% CI: 1.53–1.74]) compared to ABC/3TC regimens.
Discussion
This retrospective analysis of pharmacy claims evaluated adherence and persistence among over 13,000 newly treated HIV patients and included current ART regimens not previously reported. While there is a preponderance of data evaluating adherence with ART, our study offers a novel approach. Whereas most published studies present adherence as medication possession ratio (MPR),18,22,34 we evaluated adherence over 30-day intervals within a 12-month period and determined the proportion of patients who were adherent or non-adherent at each interval. This allowed for adherence to be evaluated in the context of time from initiation of therapy and an assessment of the number of days a patient may be without therapy within a month’s time.
Our findings are congruent with the reports of others and provide further evidence of differences in adherence rates between patients using STRs vs MTRs. Across existing adherence studies, the biggest predictor of adherence is pill burden, with patients on STR having better adherence than patients using MTRs.34–36 In our analysis, we found adherence rates at the end of the 12-month period to be more than two times higher with STRs than with MTRs. Additionally, a greater proportion of STR than MTR patients was adherent at each 30-day interval. While we found that more STR than MTR patients became non-adherent after month 7, we observed discontinuation rates of first-line therapy to be higher for MTR patients. Thus, the pattern of fewer MTR patients being classified as non-adherent towards the end of the observation period may have resulted from more MTR patients moving into the discontinuation category.
Consistent with the adherence findings, we observed that persistence was greater with STRs than MTRs. Our results suggest that patients treated with an MTR are approximately 60% more likely to discontinue therapy within 12 months than those treated with an STR. These observations underscore the important role of convenient treatment regimens with minimal toxicities in treatment continuity and may reflect important provider-driven clinical decisions to switch patients. The results further suggest that persistence with ART is influenced by age, gender, insurance payer type, and medication history. For example, we observed better persistence among patients covered by commercial payers than Medicare or Medicaid. This may be due to socio-economic factors that go beyond the scope of the current analysis. Further research is warranted to better understand the age, gender, and socioeconomic influences, as other researchers have noted similar correlations. In their evaluation of a US commercially insured population, Juday et al identified female gender as a significant predictor of ART discontinuation.37 Likewise, Asad et al found female gender and younger age to be predictors of ART discontinuation among Medicaid recipients and uninsured individuals,38 and Hughes et al found that female gender, younger age, and insurance coverage significantly predicted treatment discontinuation in a nationally representative sample of HIV patients.39
Although not evaluated in the current study, other reasons for treatment discontinuation might include virological failure or treatment tolerability.30,31 Our assessment of adherence and persistence by regimen revealed that patients using EVG/COBI/FTC/TAF were more adherent and persistence was greater than for other therapies. EVG/COBI/FTC/TAF has been shown in prior research to be well-tolerated with reduced side effects,40 which may account for these results. Along with this, we noted greater persistence with FTC/TAF-based regimens versus FTC/TDF-based regimens. This may be due to the association between TDF-based regimens and increased risk of bone mineral density decline and reduced renal function.41,42 Many physicians and their patients are switching from an FTC/TDF to F/TAF-based regimens, which may explain the 2-fold greater discontinuation of FTC/TDF backbones found in the current analysis. The decision to switch from one regimen to another can be driven by a multitude of reasons including, but not limited to, the novelty of the new regimen, adverse events, to avoid long-term toxicity, regimen simplification, and patient request.
The results presented here should be interpreted in the context of several limitations. First, this analysis was based on point-of-service, open-source pharmacy claims and is therefore subject to the inherent limitations of administrative claims data. Additionally, only pharmacies that continuously submitted claims to the database were included in the analysis, creating the potential for information bias. Next, as this study only relied on pharmacy claims, no diagnostic or other clinical information was available to confirm an HIV diagnosis. However, as ARTs are only used in HIV, it is reasonable to conclude that patients identified by use of ART are HIV-infected. In the absence of clinical information, the presence of comorbid conditions that may have influenced treatment patterns could not be confirmed. The definition of adherence or non-adherent used for this study did not allow patients to move back and forth between these categories. Thus, once patients were classified as non-adherent, they remained in that category for the duration of follow-up. Hence, patients with non-routine lapses in refills were not distinguished from those with consistent non-adherent behavior. In the current contemporary era, the threshold of adherence that is needed to sustain viral suppression is unknown. While there is some evidence suggesting that viral rebound occurs as early as two weeks after discontinuing ART,43 more research is needed to better understand the point at which adherence to the newer, more potent treatment options impacts viral suppression. As a claims database, reasons for non-adherence and discontinuation of ART could not be discerned. It is therefore unknown whether discontinuation was due to switching to new regimens, virologic failure, adverse drug reactions, or drug–drug interactions. Lastly, while we were able to delineate some risk factors associated with treatment discontinuation through multivariable analyses, unobserved confounders may remain.
Conclusion
This study found that among over 13,000 US health plan enrollees with HIV, patients using STRs were significantly less likely to discontinue ART and were more adherent with their regimens than patients taking MTRs. These observations support the findings of previously published results that suggested better adherence and persistence with STRs than MTRs. However, across all regimens, there was a large proportion of patients who interrupted therapy, discontinued therapy, or switched to a new regimen. As this research only evaluated adherence and persistence with first-line ART, further studies examining patients’ treatment trajectory beyond first-line are warranted.
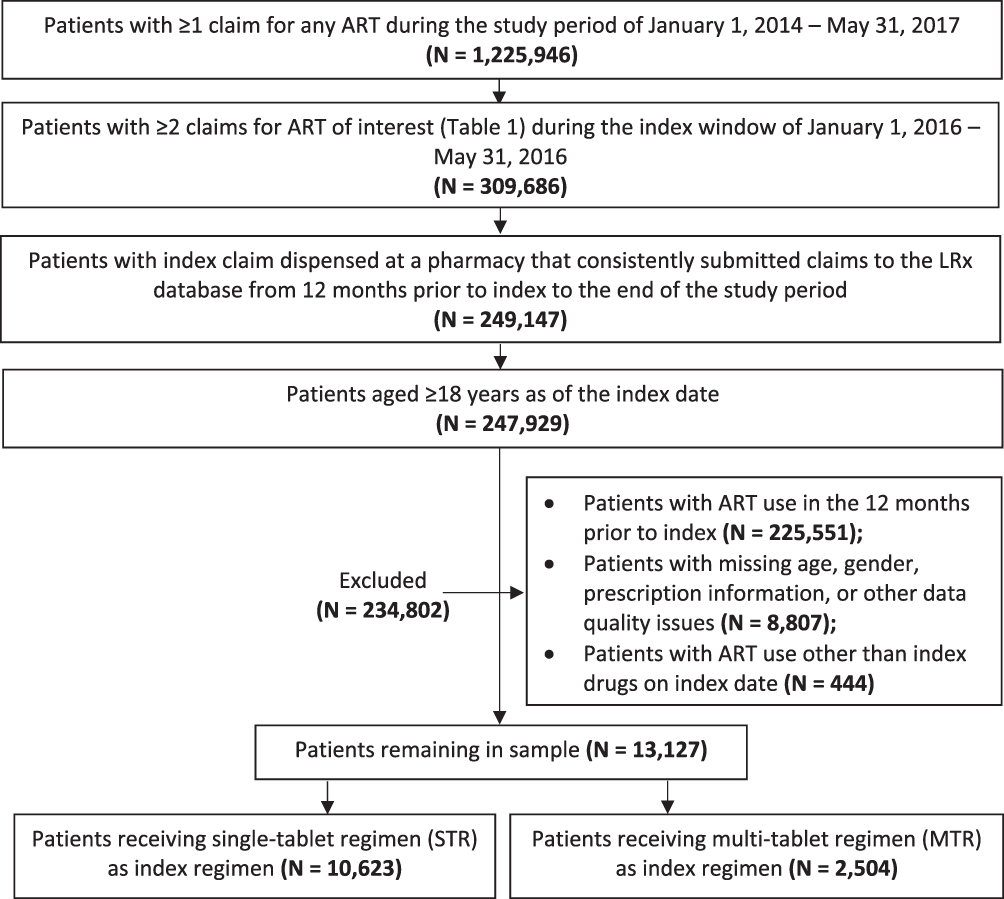 |
Figure 1 Sample selection. |
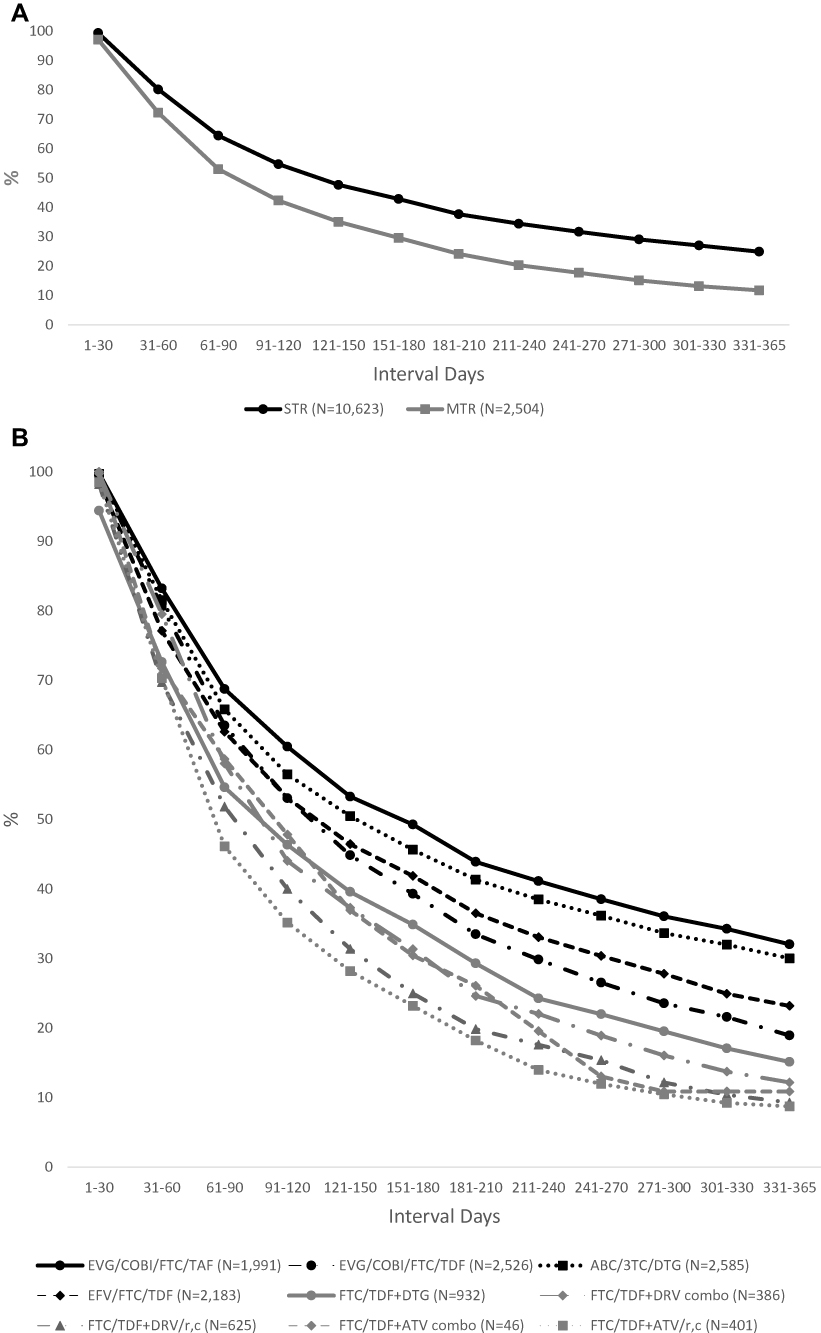 |
Figure 2 Proportion of adherent patients by 30-day Intervals: STR vs MTR ART regimens (A) and ART Regimen (B). |
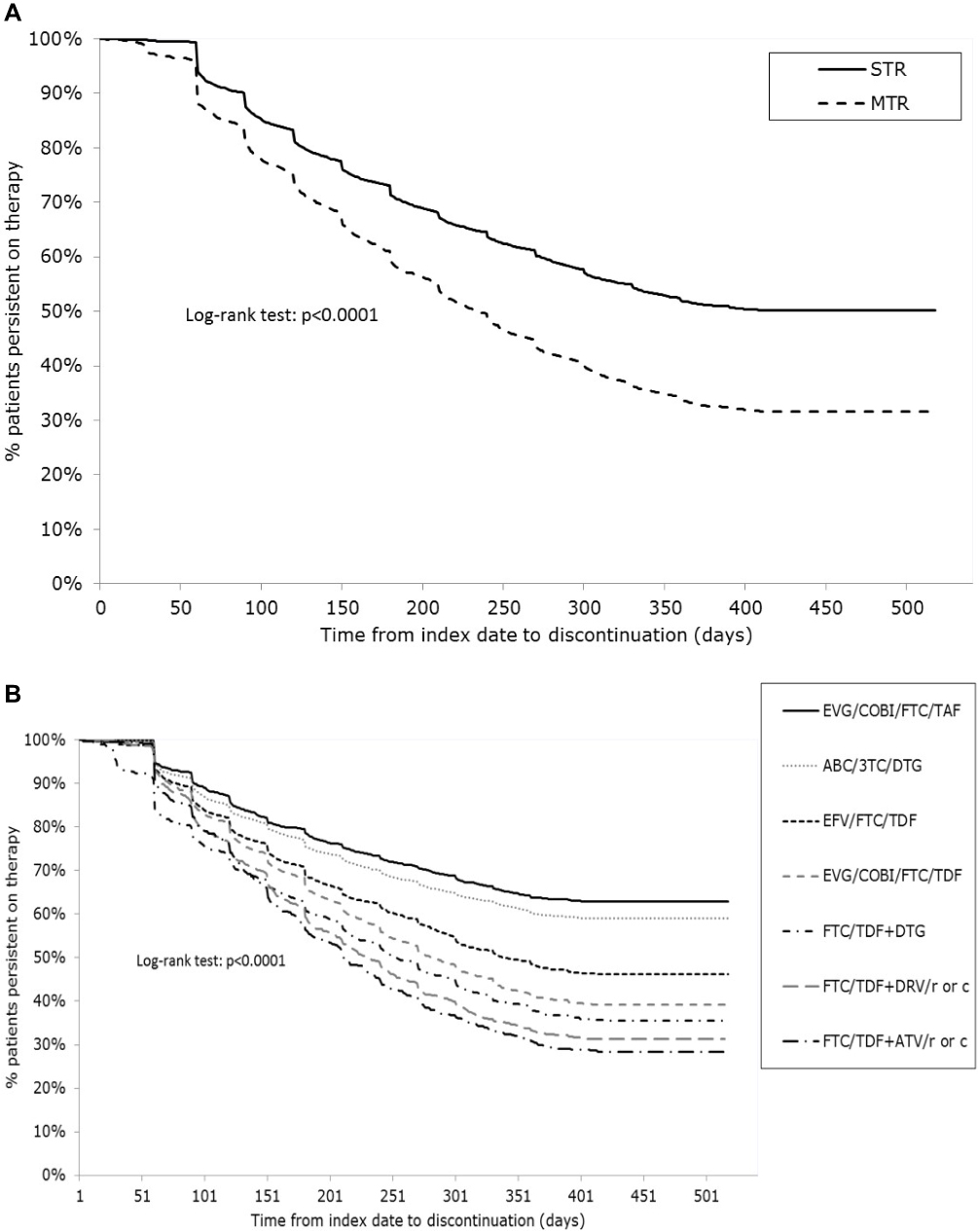 |
Figure 3 Time to discontinuation for STR vs MTR ART regimens (A) and among select ART regimens (B). |
 |
Figure 4 Adjusted* hazard ratios for select treatment discontinuation. *Each model was adjusted for age group, gender, geographic region, insurance type, baseline medications, and number of unique prescriptions on index date. |
Acknowledgment
The authors would like to thank Yi-Chien Lee, Master of Science, for statistical support throughout this study.
Disclosure
DMH and RLW are employees of IQVIA Inc. YD was an employee of IQVIA Inc. during the conduct of this study. IQVIA was contracted by Gilead Sciences to conduct this study. AB is an employee of Gilead Sciences. JPC is supported by a research grant from the Drug Information Association of Europe, a non-profit association, and has served as a consultant for Gilead Sciences. The authors report no other conflicts of interest in this work.
References
1. Department of Health and Human Services. What is HIV/aids? Available from: https://www.aids.gov/hiv-aids-basics/hiv-aids-101/what-is-hiv-aids/.
2. Centers for Disease Control and Prevention. HIV in the United States: at a glance. Available from: https://www.cdc.gov/hiv/statistics/overview/ataglance.html.
3. HIV-CAUSAL Collaboration. The effect of combined antiretroviral therapy on the overall mortality of HIV-infected individuals. AIDS. 2010;24(1):123–137. doi:10.1097/QAD.0b013e3283324283
4. Lesko C, Cole S, Hall H, et al. The effect of antiretroviral therapy on all-cause mortality, generalized to persons diagnosed with HIV in the USA, 2009–11. Int J Epidemiol. 2016;45(1):140–150. doi:10.1093/ije/dyv352
5. Murphy E, Collier A, Kalish L, et al. Highly active antiretroviral therapy decreases mortality and morbidity in patients with advanced HIV disease. Ann Intern Med. 2001;135(1):17. doi:10.7326/0003-4819-135-11-200112040-00011
6. Gallant J, Brunetta J, Crofoot G et al. Efficacy and safety of switching to simpler single-tablet regimen of elvitegravir/cobicistat/emtricitabine/tenofovirAlafenamide (E/C/F/TAF) in HIV-1/hepatitis B coinfected adults in North America and Japan (NCT02071082): week 48 results [Poster WELBPA13]. Vancouver:
7. Lee F, Amin J, Carr A. Efficacy of initial antiretroviral therapy for HIV-1 infection in adults: a systematic review and meta-analysis of 114 studies with up to 144 weeks’ follow-up. PLoS One. 2014;9(5):e97482. doi:10.1371/journal.pone.0097482
8. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. Department of Health and Human Services. Available from: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed October 1, 2017.
9. Cramer J, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
10. Bansi-Matharu L, Rodriguez LG, Cole SR, et al. Risk factors for Antiretroviral Therapy (ART) discontinuation in a large multinational trial of early ART initiators. AIDS. 2019;33(8):1385–1390. doi:10.1097/QAD.0000000000002210
11. Scott Sutton S, Magagnoli J, Hardin J. Impact of pill burden on adherence, risk of hospitalization, and viral suppression in patients with HIV infection and AIDS receiving antiretroviral therapy. Pharmacotherapy. 2016;36(4):385–401. doi:10.1002/phar.1728
12. Portsmouth S, Osorio J, McCormick K, Gazzard B, Moyle G. Better maintained adherence on switching from twice-daily to once-daily therapy for HIV: a 24-week randomized trial of treatment simplification using stavudine prolonged-release capsules. HIV Med. 2005;6(3):185–190. doi:10.1111/j.1468-1293.2005.00287.x
13. Gardner E, Burman W, Maravi M, Davidson A. Selective drug taking during combination antiretroviral therapy in an unselected clinic population. JAIDS. 2005;40(3):294–300. doi:10.1097/01.qai.0000182229.84182.06
14. Hanna DB, Hessol NA, Golub ET, et al. Increase in single-tablet regimen use and associated improvements in adherence-related outcomes in HIV-infected women. J Acquired Immune Deficiency Syndrome. 2014;65(5):587–596. doi:10.1097/QAI.0000000000000082
15. Airoldi M, Zaccarelli M, Bisi L, et al. One-pill once-a-day HAART: a simplification strategy that improves adherence and quality of life of HIV-infected subjects. Patient Prefer Adherence. 2010:115–125.
16. Bangsberg D, Ragland K, Monk A, Deeks S. A single tablet regimen is associated with higher adherence and viral suppression than multiple tablet regimens in HIV+ homeless and marginally housed people. AIDS. 2010;24(18):2835–2840. doi:10.1097/QAD.0b013e328340a209
17. Armstrong B, Chan D, Stewart M, Fagan D, Smith D. Single tablet regimen usage and efficacy in the treatment of HIV infection in Australia. AIDS Res Treat. 2015;2015:1–5.
18. Cooke C, Lee H, Xing S. Adherence to antiretroviral therapy in managed care members in the United States: a retrospective claims analysis. J Managed Care Pharm. 2014;20(1):86–92. doi:10.18553/jmcp.2014.20.1.86
19. Altice F, Evuarherhe O, Shina S, Carter G, Beaubrun AC. Adherence to HIV Treatment regimens: systematic literature review and meta-analysis. Patient Prefer Adherence. 2019;13:475–490. doi:10.2147/PPA.S192735
20. Kim MJ, Kim SW, Chang HH. Comparison of antiretroviral regimens: adverse effects and tolerability failure that cause regimen switching. Infect Chemother. 2015;47(4):231–238. doi:10.3947/ic.2015.47.4.231
21. Davy-Mendez T, Erron JJ, Zakharova O, Wohl DA, Napravnik S. Increased persistence of initial treatment for HIV infection with modern antiretroviral therapy. J Acquir Immune Defic Syndr. 2017;76(2):111–115. doi:10.1097/QAI.0000000000001481
22. Cohen C, Meyers J, Davis K. Association between daily antiretroviral pill burden and treatment adherence, hospitalisation risk, and other healthcare utilisation and costs in a US medicaid population with HIV. BMJ Open. 2013;3(8):e003028. doi:10.1136/bmjopen-2013-003028
23. Wood E, Hogg R, Yip B, Harrigan P, O’Shaughnessy M, Montaner J. Effect of medication adherence on survival of HIV-infected adults who start highly active antiretroviral therapy when the CD4+ cell count is 0.200 to 0.350 × 109 cells/L. Ann Intern Med. 2003;139(10):810. doi:10.7326/0003-4819-139-10-200311180-00008
24. Fielden S, Rusch M, Yip B, et al. Nonadherence increases the risk of hospitalization among HIV-infected antiretroviral Naïve patients started on HAART. J Int Assoc Physicians AIDS Care. 2008;7(5):238–244. doi:10.1177/1545109708323132
25. Kitahata M, Reed S, Dillingham P, et al. Pharmacy-based assessment of adherence to HAART predicts virologic and immunologic treatment response and clinical progression to AIDS and death. Int J STD AIDS. 2004;15(12):803–810. doi:10.1258/0956462042563666
26. Bangsberg D, Perry S, Charlebois E, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–1183. doi:10.1097/00002030-200106150-00015
27. Meyers J, Mugavero M, Davis K. Adherence to antiretroviral treatment and correlation with risk of hospitalization among commercially insured HIV patients in the United States. PLoS One. 2012;7(2):e31591. doi:10.1371/journal.pone.0031591
28. Lam W, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
29. Schaecher K. The importance of treatment adherence in HIV. Am J Manag Care. 2013;19(12 Suppl):s231–7.
30. Raffi F, Yazdanpanah Y, Fagnani F, Laurendeau C, Lafuma A, Gourmelen J. Persistence and adherence to single-tablet regimens in HIV treatment: a cohort study from the French National Healthcare Insurance Database. J Antimicrob Chemother. 2015;70(7):2121–2128. doi:10.1093/jac/dkv083
31. Bae J, Guyer W, Grimm K, Altice F. Medication persistence in the treatment of HIV infection: a review of the literature and implications for future clinical care and research. AIDS. 2011;25(3):279–290. doi:10.1097/QAD.0b013e328340feb0
32. Robbins GK, Cohn SE, Harrison LJ, et al. Characteristics associated with virologic failure in high-risk HIV-positive participants with prior failure: a post hoc analysis of ACTG 5251. HIV Clin Trials. 2016;17(4):165–172. doi:10.1080/15284336.2016.1189754
33. Bardeguez AD, Lindsey JC, Shannon M, et al. Adherence to antiretrovirals among US women during and after pregnancy. J Acquir Immune Defic Syndr. 2008;48(4):408–417. doi:10.1097/QAI.0b013e31817bbe80
34. Tennant SJ, Hester EK, Caulder CR, Lu K, Bookstaver PB. Adherence among rural HIV-infected patients in the deep-south: a comparison between single-tablet and multi-tablet once-daily regimens. J Int Assoc Provid AIDS Care. 2015;4(1):64–71. doi:10.1177/2325957414555228
35. Clay PG, Nag S, Graham CM, Narayanan S. Meta-analysis of studies comparing single and multi-tablet fixed dose combination HIV treatment regimens. Medicine. 2015;94(42):e1677. doi:10.1097/MD.0000000000000874
36. Stone VE, Jordan J, Tolson J, Miller R, Pilon T. Perspectives on adherence and simplicity for HIV-infected patients on antiretroviral therapy: self-report of the relative importance of multiple attributes of highly active antiretroviral therapy (HAART) regimens in predicting adherence. J Acquir Immune Defic Syndr. 2004;36(3):808–816. doi:10.1097/00126334-200407010-00007
37. Juday T, Grimm K, Zoe-Powers A, Willig J, Kim E. A retrospective study of HIV antiretroviral treatment persistence in a commercially insured population in the United States. AIDS Care. 2011;23(9):1154–1162. doi:10.1080/09540121.2010.543884
38. Asad S, Hulgan T, Raffanti SP, Daugherty J, Ray W, Sterling TR. Sociodemographic factors predict early discontinuation of HIV non-nucleoside reverse transcriptase inhibitors and protease inhibitors. J Natl Med Assoc. 2008;100(12):1417–1424. doi:10.1016/s0027-9684(15)31541-8
39. Hughes AJ, Mattson CL, Scheer S, Beer L, Skarbinski J. Discontinuation of antiretroviral therapy among adults receiving HIV care in the United States. J Acquir Immune Defic Syndr. 2014;66(1):80–89. doi:10.1097/QAI.0000000000000084
40. Angione SA, Cherian SM, Ozdener AE. A review of the efficacy and safety of Genvoya® (elvitegravir, cobicistat, emtricitabine, and tenofoviralafenamide) in the management of HIV-1 infection. J Pharm Pract. 2018;31(2):216–221. doi:10.1177/0897190017710519
41. DeJesus E, Haas B, Segal-Maurer S, et al. Superior efficacy and improved renal and bone safety after switching from a tenovofir disoproxil fumarate- to a tenofovir aladenamide-based regimen through 96 weeks of treatment. AIDS Res Hum Retroviruses. 2018;34(4):337–342. doi:10.1089/AID.2017.0203
42. Hagins D, Orkin C, Daar ES, et al. Switching to coformulated rilpivirine (RPV), emtricitabine (FTC) and tenofovir alafenamide from either RPV, FTC and tenofovir disoproxil fumarate (TDF) or efavirenz, FTC and TDF: 96-week results from two randomized clinical trials. HIV Med. 2018;19(10):724–733. doi:10.1111/hiv.12664
43. Calin R, Hamimi C, Lambert-Niclot S, et al. Treatment interruption in chronically HIV-infected patients with an ultralow HIV reservoir. AIDS. 2016;30(5):761–769. doi:10.1097/QAD.0000000000000987
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.