")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Translation and Cultural Adaptation of the Polish Version of the Communication Assessment Tool (CAT)
Authors Świątoniowska-Lonc N , Białoszewski A , Makoul G, Jankowska-Polańska B
Received 11 May 2020
Accepted for publication 22 July 2020
Published 14 September 2020 Volume 2020:13 Pages 1533—1542
DOI https://doi.org/10.2147/RMHP.S261710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Natalia Świątoniowska-Lonc,1 Artur Białoszewski,2 Gregory Makoul,3,4 Beata Jankowska-Polańska1
1Department of Clinical Nursing, Faculty of Health Science, Wroclaw Medical University, Wroclaw, Poland; 2Department of Prevention of Environmental Hazards and Allergology, Warsaw Medical University, Warsaw, Poland; 3PatientWisdom, Inc., New Haven, CT, USA; 4Department of Medicine, Yale School of Medicine, New Haven, CT, USA
Correspondence: Natalia Świątoniowska-Lonc
Department of Clinical Nursing, Faculty of Health Science, Wroclaw Medical University, K. Bartla 5, Wroclaw 51-616, Poland
Tel +48 71 784 18 24
Fax +48 71 345 93 24
Email [email protected]
Background and Objective: Adequate communication skills are the core competency of healthcare providers for optimal patient interaction and relationships based on mutual trust. Unfortunately, there are still few publications assessing the type and effectiveness of therapeutic communication, and there are no tools to facilitate the standard, regular evaluation of the process. The objective of this study was the translation and cultural adaptation of a Polish version of the 14-item Communication Assessment Tool (CAT) to assess the interpersonal and communication skills of physicians and to identify determinants influencing the quality of communication.
Design: It is an exploratory and cross-sectional survey design. The patients completed a survey consisted of the CAT. Socio-demographic data were obtained from the hospital register.
Setting: Hypertension clinic at the clinical hospital in Wrocław.
Participants: A total of 300 patients with diagnosed hypertension were selected. Of these, 50 patients were excluded (mental illness, cognitive impairment, resignation). A total of 250 people (61.23± 14.34 years) participated in the study. Qualification for the study was carried out by a trained doctor, who is an internal medicine specialist.
Main Measure Outcome: Translation and cultural adaptation of Polish CAT.
Results: Cronbach’s alpha for the CAT is 0.96 and does not require the exclusion of any items to increase its value. The loadings of the individual items ranged from 0.725 to 0.894. At the item level, results ranged from 28.4% to 50.4% “excellent”, the highest scores were given to “let me talk without interruptions” (50.4%) and “talked in terms I could understand” (47.6%). The correlation analysis showed a modestly positive statistical effect of the duration of a medical visit (r=0.225) and the time spent on talking about patient’s problems (r=0.23) with the general result of the CAT questionnaire (p< 0.001).
Conclusion: The CAT is a very good tool for assessing the quality of communication in Polish-speaking settings and can be recommended for use in everyday practice.
Keywords: assessment tool, communication skills, psychometric, physician–patient communication
Introduction
Interpersonal and communication skills are essential for high-quality care. The Accreditation Council for Graduate Medical Education (ACGME) has identified communication skills as one of the six core competencies of physicians and provides a framework for measuring the development of these skills in different competencies.1 In recent decades, a patient-oriented approach and effective communication have been recognised as the basis for high-quality care.2
Research has shown the importance of communication between a patient and a healthcare provider by determining how it correlates with an improvement in patient’s satisfaction and medical results, including emotional health, less suffering, treatment efficacy, symptoms treatment, increased health control, functional abilities, vitality, and physiological measures such as blood pressure and blood sugar levels control.3,4 Proper communication is a set of non-technical skills that enable a physician to optimise interaction with a patient. In order to achieve success and effective communication, attention should be paid to active and effective listening, and effective verbal and non-verbal listening.5
Communication and interpersonal skills overlap and relate to the ability of providers to communicate ideas, knowledge, explanations or instructions to patients, and the ability to receive, understand and use information received from patients and to interact effectively in the scope of decision-making. Interpersonal skills focus more specifically on the ability of providers to interact with and understand patients, including building relationships of mutual trust.6 In this study, we use the term “communication skills” as an umbrella term that includes interpersonal skills.
A doctor’s relationship with a patient is aimed at addressing needs that are significant for health and life. Both parties interact with each other based on their own perspectives and values, as well as on common values such as positive treatment outcomes. Communication between healthcare providers and patients has an important impact on patients’ attitude towards their conditions. The level of patient satisfaction, including that in the therapy relationship, is considered one of the elements of the quality of health care provided in treatment facilities. Measuring the level of satisfaction can also constitute a source of clues as to the directions in which the patient will develop, organisational changes or patient expectations. It is worth emphasising that the patient’s satisfaction has a significant impact on their choice of doctor and on the choice of the treatment facility itself.
Few published reviews prove the relationship between effective communication and satisfaction of communication with better quality of life and better patient compliance with therapeutic recommendations.7 So far there has been no gold standard that would indicate how to evaluate satisfaction in the doctor–patient relationship, nor is it clear which questionnaire is best to use in such research.
Zill et al’s meta-analysis describes 20 tools that are currently available to evaluate medical communication.8 None of the questionnaires described meet the criterion of an ideal tool. This is why we decided to use the CAT questionnaire, which is often used by other researchers, has cultural adaptations in several countries, and has been recognized as a simple but effective way of evaluating doctor-patient communication.8–15 Moreover, in Zill et al’s meta-analysis, the questionnaire obtained a good score for inter-rater-reliability.8 Because there is no Polish version of the CAT and, in our opinion, satisfaction with communication impacts the effectiveness of treatment, adherence and quality of life, we decided to use this scale in our study. Therefore, the aim of this study is to assess the psychometric properties of the Polish version of the CAT scale. Additionally, we assessed the quality of communication between doctors and patients and explored the determinants influencing perceptions of quality.
Methods
During the study period, August–November 2019, a total of 300 patients with diagnosed hypertension were selected. Of these, 36 patients did not meet the criteria to be included in the study or refused to participate. In the first stage of qualification, 264 persons who met the criteria were included, but 14 resigned despite a prior consent for participation. In sum, 250 people participated in the study. Qualification for the study was carried out by a trained medical doctor specialist in internal medicine. On the day of the study, following a visit to the clinic, all qualified patients evaluated their satisfaction with the doctor-patient communication. In addition to satisfaction, the study questions dealt with the frequency of visits to the clinic and further appointments arranged on the day of the visit.
Socio-demographic data were obtained from the hospital register. The time of the visit was assessed by the patient on the basis of their time at the doctor’s office, but the patients were also asked about the time devoted to the discussion of their problems.
Inclusion and Exclusion Criteria
The criteria for patients to be included in the study were age ≥18, cognitive status allowing to understand the purpose and methods of the study and to fill in the questionnaire (Mini Mental State Examination ≥18), diagnosis of at least one chronic disease that requires taking at least 1 drug for several months (the need to apply for a prescription and make appointments for control visits was one of the variables defined in the study), informed consent to participate in the study and use of Polish in order to understand the questions included in the questionnaire.
Patients without one or more chronic diseases treated pharmacologically, with coexisting cancer, mental illness, exacerbation of heart failure (NYHA IV), ischaemic heart disease (CCS IV) and acute respiratory diseases due to the complexity of the clinical condition and the risk of disturbing the assessment of the degree of compliance with therapeutic recommendations and not consenting for the study or patients who have withdrawn from the study at any stage were excluded from the study.
Ethical Considerations
The study was approved by the Bioethics Committee of the Wrocław Medical University (No. KB 42/2019). Participation was voluntary and anonymous, and all patients were informed about the study’s purpose and their right to decline or discontinue their participation. Written informed consent was obtained from each participant prior to their inclusion before the interview. Data confidentiality was assured by using assigned code numbers in lieu of participants’ names. The study was performed in accordance with the Helsinki Declaration and the principles of good clinical practice, with respect to the rights and dignity of participants.
Questionnaire
The Communication Assessment Tool developed by Makoul et al (2007)9 is a 14-item instrument aimed at assessing patients’ perception of the effectiveness of communication with individual doctors. Patients are asked to give answers on the basis of their last visit to the doctor. The survey can be conducted individually or by an interviewer and can be filled in on paper, by an automated telephone system or via the Internet. In this study, patients responded independently to questions. While completing the items, the patients were supported, where necessary, by a researcher throughout the testing period (each 30-minute session).
Each item is scored on a 5-point scale from poor to excellent. The overall score is reported as the percentage of items rated as excellent, because previous research demonstrated that “excellent” maps onto “yes” and all other responses map onto “no”, in addition to the fact that in reporting results as a percentage, “excellent” has more impact than using mean values.9
Translation Procedures
In the framework of the project, the original version of the questionnaire was translated into Polish and the psychometric properties of the CAT were assessed. The consistency of the scale results was calculated using the Cronbach α method. Additionally, multidimensional regression analysis was used to find predictive factors that significantly influenced adhesion. A 14-point CAT was translated from English into Polish and then backward translated to check the accuracy of the translation.9
Permission to do such a translation was obtained in 2018 from the author of the original English version of the CAT. The translation was carried out as follows: 1) Translation sent – two bilingual people (a nurse and a public health specialist) translated the instrument themselves from English into Polish without mutual consultation; 2) Translation returned – a bilingual nurse blind to the original English version of the instrument translated the instrument from Polish into English; and 3) Decency – both the English version and the translated Polish version of the instrument were considered equally important to verify that the scale elements in different language versions are very similar.16
The translations received were verified by the research team, and all the differences were discussed and agreed upon. The design of the instrument was then developed. The version prepared through a feedback translation was sent to the author of the original CAT questionnaire for approval.16 After the translation was approved by the author, a pilot study was conducted to verify patients’ understanding of the Polish version of the questionnaire. The pilot study included 30 patients of a cardiology clinic with hypertension. All patients filled in the questionnaire on their own and did not report any difficulties in understanding or responding to any of the items. The pretested version of CAT-14 was used as the final version for psychometric tests in the population of patients with hypertension in Poland.
Statistical Analysis
Internal consistency was assessed with the use of Cronbach’s alpha and Confirmatory Factor Analysis (CFA). In the latter, the Hu and Bentler double indicator method was used to assess the model fit. Comparison of the CAT results in two groups was performed with the use of Student’s t-test (when the variable had normal distribution in these groups) or Mann–Whitney’s test (otherwise). Comparison of the CAT results in three or more groups was performed using the Kruskal–Wallis test. After the discovery of statistically significant differences, post hoc analysis with Fisher’s LSD test (in the case of normal distribution) or Dunn’s test (in the case of a lack of normality) was performed in order to identify statistically significantly different groups. Correlations between the CAT results and quantitative variables were analysed with the use of the Pearson correlation coefficient (when both had normal distribution) or Spearman correlation coefficient (otherwise). The strength of the relationship was interpreted as follows:
- |r| ≥ 0.9 – very strong
- 0.7 ≤ |r| < 0.9 – strong
- 0.5 ≤ |r| < 0.7 – moderate
- 0.3 ≤ |r| < 0.5 – weak
- |r| < 0.3 – very weak (negligible).
The normality of the distribution of variables was tested with the use of the Shapiro–Wilk test. The analysis assumed a significance level of 0.05. Thus, all p-values below 0.05 were interpreted as indicating significant dependencies. The analysis was performed in R program, version 3.6.0.17
Patient and Public Involvement Statement
Patients were not involved in planning or conducting this specific research project.
Results
Study Participants
Two hundred and fifty patients were qualified for the study (56% of women); the average age of the study group was 61.23±14.34. For the most part, the respondents were in a relationship (70.4%) and rural residents (77.2%) who had secondary education (52.8%) or higher education (38%). In the group surveyed, more than half of the respondents were no longer professionally active (46.8% retired and 14.8% on a pension). The majority of the patients assessed their financial situation as good (38.8% could afford most expenses and could even save, while 44% could afford everyday expenses). The health problems most commonly associated with hypertension were cardiovascular diseases (55.2%) and type 2 diabetes (39.6%). (Table 1)
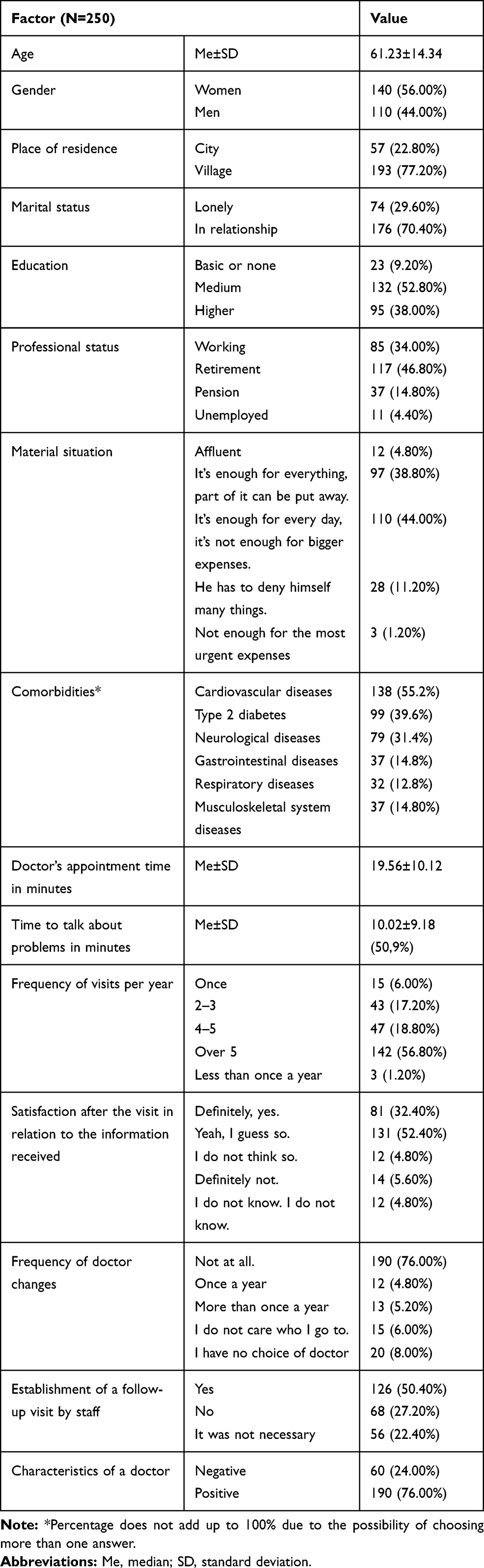 |
Table 1 Socio-Demographic Characteristics of the Surveyed Group and Characteristics of the Last Visit to the Doctor |
The study defined the profile of a meeting with a physician. In the opinion of the patients surveyed, the average visit time was 19.56±10.12 minutes, and more than half of this time was devoted to discussing the patient’s problems (10.02±9.18) (Table 1). Over half of the patients received more than 5 medical consultations in the last year (56.8%), 54.4% of the respondents were rather or definitely satisfied (32.4%) with the information received during the visit to the doctor. Seventy-six percent of the patients did not change their doctor in the last year and the vast majority of patients (76%) assessed their doctor’s characteristics positively (Table 1).
CAT
Performance
Following the instructions of the author of the original version of the questionnaire, the results were given as a percentage of “excellent” answers in each of the CAT questions. The results ranged from 28.4% to 50.4%. As shown in Table 2, the highest scores were given to: “let me talk without interruptions” (50.4%), “talked in terms I could understand” (47.6%), “paid attention to me (looked at me, listened)” (47.2%), and “treated me with respect” (46.0%). The lowest scores were given to: “encouraged me to ask questions” (28.4%), “involved me in decisions as much as I wanted” (29.2%), “discussed next steps” (35.2%), and “greeted me in a way that made me feel comfortable” (38.4%).
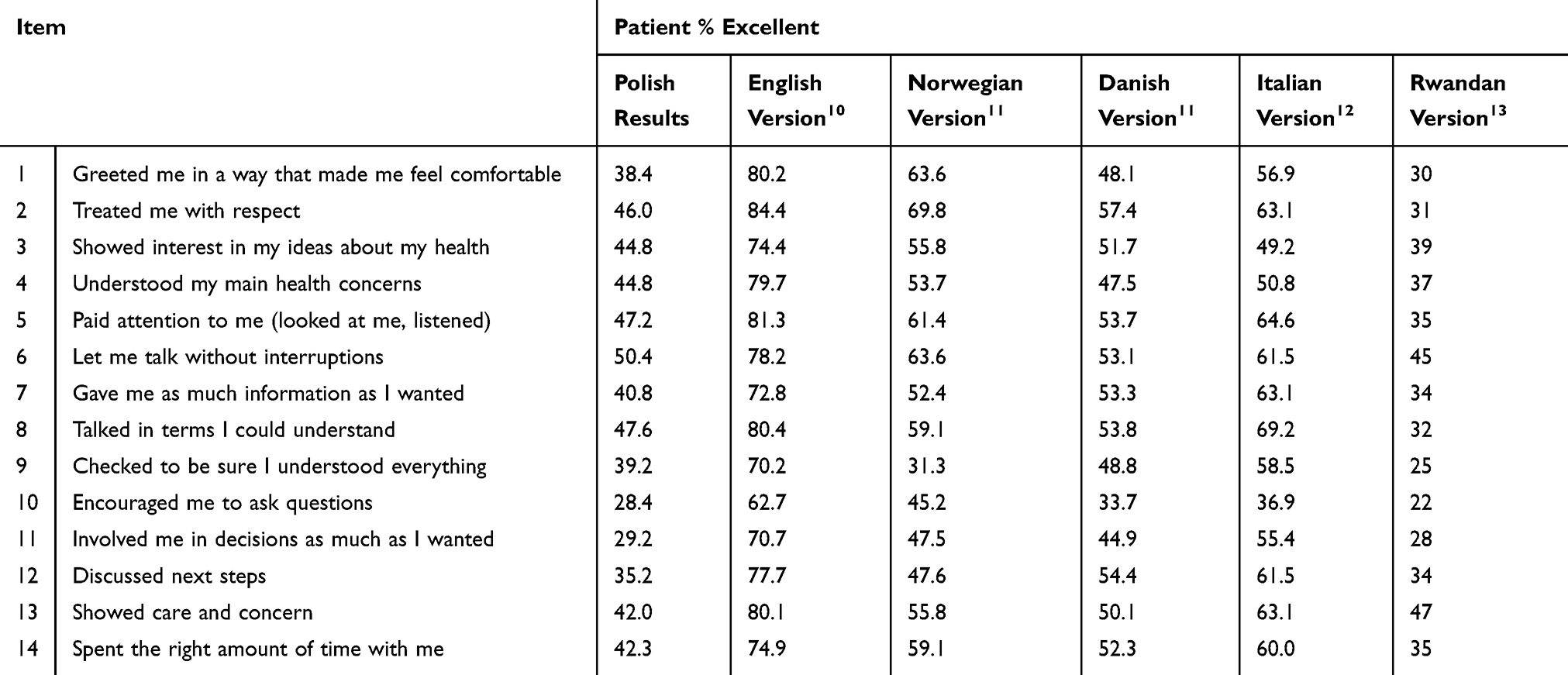 |
Table 2 Results of CAT Questionnaire and Comparison of Results from Different Language Versions of the CAT Questionnaire |
External Validity
Table 2 presents the results of the CAT conducted in different countries using relevant translations. While the overall proportion of excellent responses varies widely from country to country, it is notable that “encouraged me to ask questions” and “involved me in decisions as much as I wanted” are the lowest scores in each of these studies.
Reliability – Confirmatory Factor Analysis
For a univariate structure of the CAT questionnaire, unsatisfactory values of fit indices RMSEA, CFI and TLI were obtained. Only the SRMR value indicated a good fit between the model and the data (the exact values are described as Model I in Table 3).
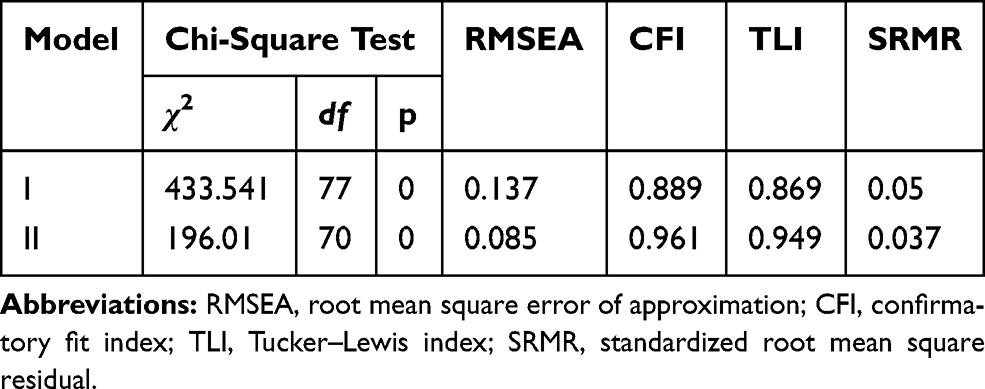 |
Table 3 Reliability – Confirmatory Factor Analysis |
Since no direct confirmation of a univariate CAT structure was obtained, the modifications indicated by the so-called modification indices were applied. In this case, they suggest introducing correlation between the following pairs of items into the model: 1 and 2, 10 and 11, 13 and 14, 5 and 6, 6 and 8, 4 and 12, 8 and 9. This allows the desired parameter values to be obtained (RMSEA<0.06, CFI>0.96, model II). The loadings of individual items ranged from 0.725 to 0.894 and were statistically significant (p<0.05) (Table 4).
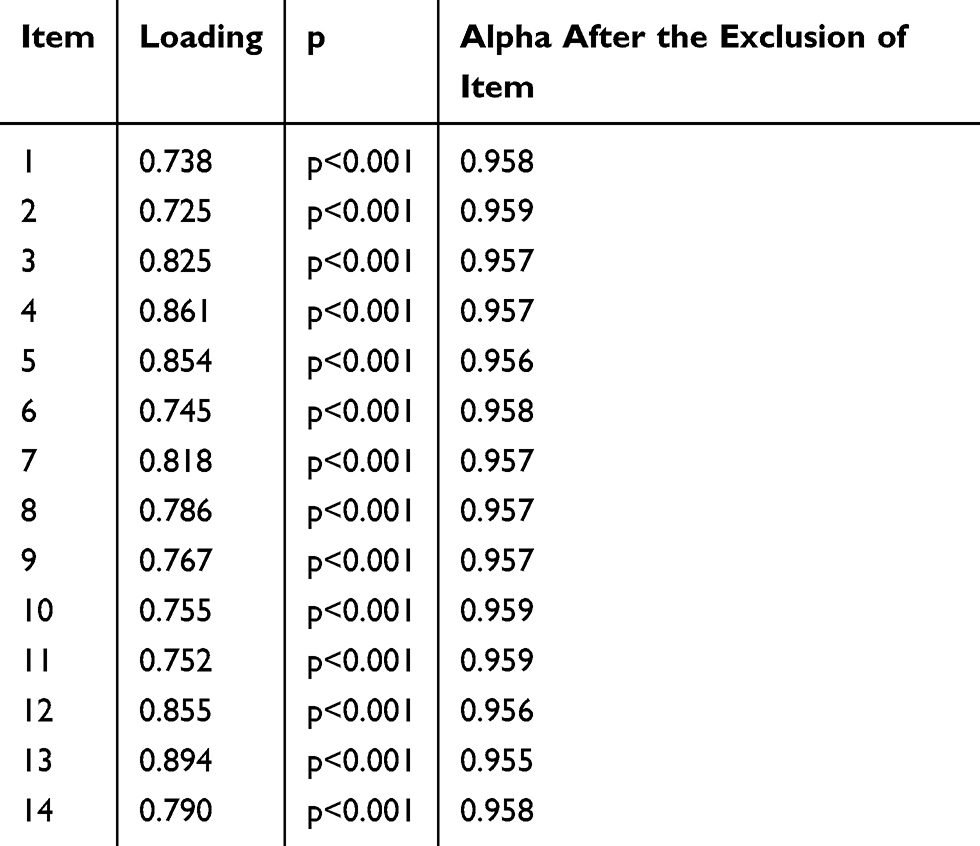 |
Table 4 The Loadings of Individual Items and Cronbach’s Alpha Value for Individual Items |
Cronbach’s Alpha
In the Polish version of the CAT questionnaire, the value of the Cronbach’s alpha coefficient was 0.96, which indicates very good psychometric properties and high internal consistency of the tool.18 In the procedure for evaluating the psychometric properties of the scale, it is not necessary to exclude any of the items due to the lack of influence on the Cronbach’s alpha values (Table 4).
Relevance of the Questionnaire
In terms of content validity, the Polish version of the CAT, in the opinion of the experts participating in the survey, seems to be a very good tool, which does not differ from the original version. In the Polish version, no cultural or linguistic differences were found in relation to the original version of the questionnaire.
CAT Results and Patient Characteristics
The comparative analysis showed significant differences in the values of the CAT questionnaire between the selected variables (Table 5). Table 5 presents the average result for the entire CAT questionnaire in comparative analysis depending on selected variables. Women reported higher scores than men (56.97±12.56 vs 53.93±11.82; p=0.018). Similar differences were observed in the values of the CAT questionnaire between those satisfied and dissatisfied with the information obtained from the doctor (61.78±8.74 vs 45±13.6; p<0.001), patients who had a scheduled follow-up visit in comparison to those who did not have such a visit or who did not need to have a scheduled follow-up visit (57.03±12.27 vs 50.57±12.26 vs 58.62±10.76; p<0.001), persons describing physicians with positive traits in comparison to persons negatively talking about physicians (58.99±9.72 vs 45±13.63; p<0.001). People with a permanent primary care physician reported better communication than those who often changed their doctors (57.51±10.28 vs 49.31±16.32; p=0.006).
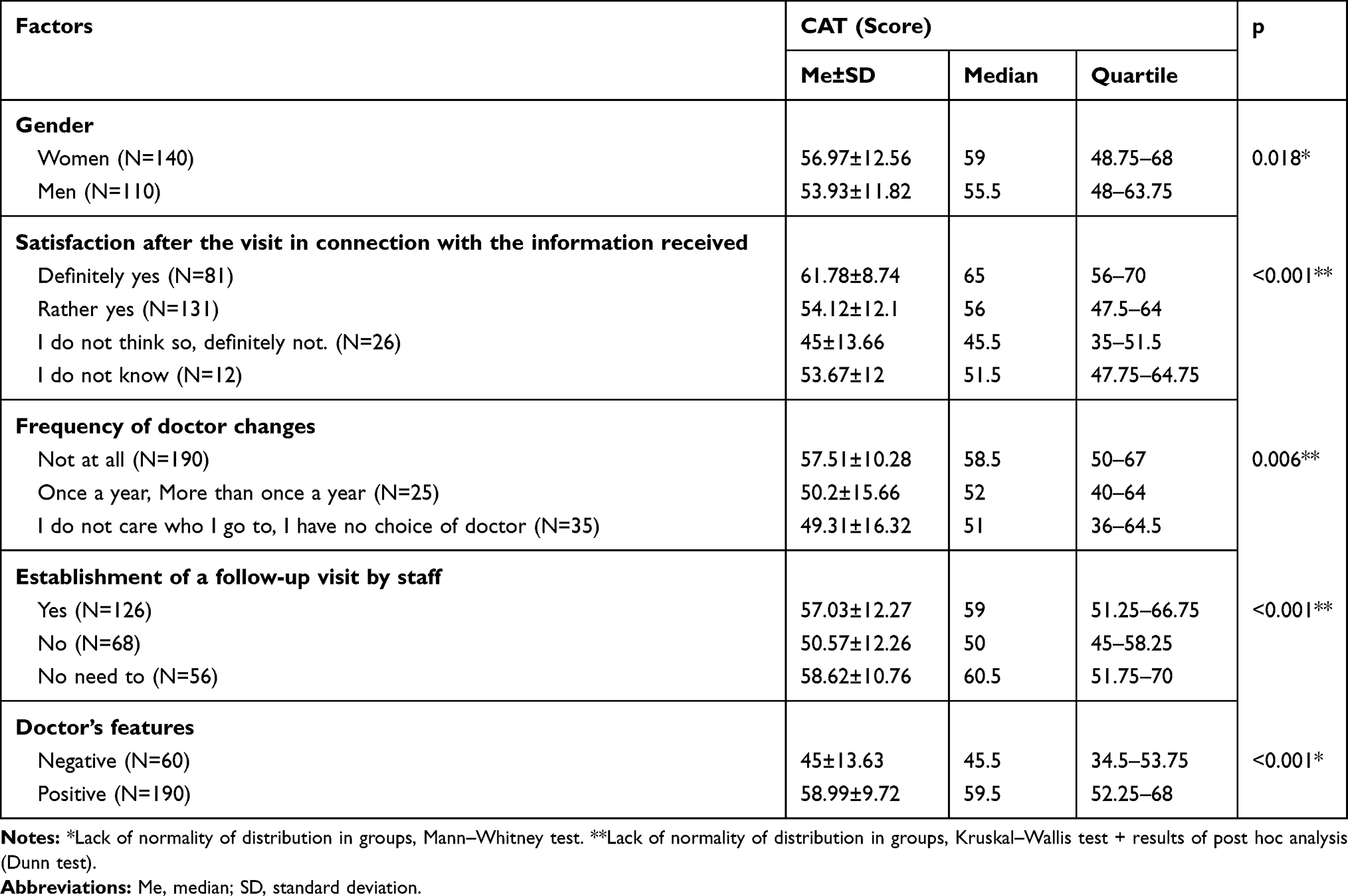 |
Table 5 Results of a Comparative Analysis of CAT Values Depending on Selected Variables |
Pearson Correlation Analysis
The comparative analysis revealed significant differences in the levels of satisfaction between gender, satisfaction after the visit in connection with the information received, frequency of doctor changes, establishment of a follow-up visit by staff, and doctor’s features. However, in this analysis, only correlations of visit time and time devoted to discussing problems had a statistically significant relation to satisfaction with communication. The correlation analysis showed a significant positive statistical effect of the duration of a medical visit (correlation coefficient 0.225) and the time spent on talking about patient’s problems (correlation coefficient 0.23) with the general result of the CAT questionnaire (p<0.001) (Table 6).
 |
Table 6 Results of an Analysis of Correlations Between Selected Variables and CAT Questionnaire Results |
Discussion
This study is the first to translate and validate the CAT into the Polish language, with the questionnaire being translated from the original English version. The CAT questionnaire is a reliable and valid instrument to measure satisfaction with doctor-patient communication and to assess the doctor’s interpersonal skills. A 14-item version was analysed in the survey, which strictly evaluates the doctor’s attitude towards the patient.
The Polish version of the CAT questionnaire showed very good psychometric properties and no cultural/linguistic differences were observed between the Polish version and the original version of the questionnaire in terms of what the doctor-patient communication should look like.
A high Cronbach’s alpha score (0.96) obtained in the present study indicates very good psychometric properties of the Polish version of the CAT questionnaire. According to the literature, the optimum value of Cronbach’s alpha should be ≥0.90. The CAT questionnaire seems to be a very well-prepared tool for assessing satisfaction of communication: English - 0.96, Norwegian and Dutch - 0.97, Italian - 0.95, Rwandan >0.9, Portuguese - 0.97 and German - 0.86.9–14
While translation and cultural adaptation in Italy and Rwanda required slight clarifications of certain CAT items, the team working on the Polish CAT did not encounter any problems related to the adaptation of individual questions of the questionnaire.11,12 The authors of the Rwandan version had problems translating questions 12 and 13, and these stemmed from the specific nature of the country and its accepted norms. For item 12, it was not possible to identify an equivalent Kinyarwanda concept for “follow-up plans”. The final agreed version was back-translated as “a time to come back”. Item 13 was initially back-translated as “He/she cared for me and had pity for me” reflecting a difficulty in finding a Kinyarwanda equivalent of “showed care and concern”. As “cared for me” in Kinyarwanda includes the concept of “concern”, the final version back-translation became “He seemed like one who cared for me”.12 In an Italian validating study, the group included in the study had difficulty understanding the translated items. Patients had problems with questions 1, 3, 4, 8 and 9, which resulted in the authors replacing problematic phrases with more standard terms that were more understandable for the patients.11
The CAT has also been adapted in other countries, including Norway, Portugal, Germany, South Korea, but intercultural adaptation and validation are not detailed in these studies.10,13–15
Overall satisfaction regarding the medical services provided by the doctor was moderate. The original version of the CAT questionnaire did not evaluate communication as a whole, but rather its individual components in the form of a percentage of excellent answers. In our own study, the worst scores were given for encouraging patients to ask questions (28.4% of excellent answers), enabling patients to participate in decision-making (29.2% of excellent answers) and discussing further treatment with patients (35.2% of excellent answers). The results of this study are consistent with those of other authors, who observed an equally low percentage of excellent answers to the statement concerning encouragement to ask questions presented in other available studies.9,18,19 In our study, the best score was given to the following: “let me talk without interruptions” (50.4%) and “talked in terms I could understand” (47.6%), “Paid attention to me (looked at me, listened)” (47.2%). Moreover, in this respect, the Polish results do not differ from those of other countries. Similar results were found by the authors of the original Danish and Italian versions, where comprehensibility of speech was the most frequently positively evaluated feature of the doctor (47.6% of excellent answers).10,11
In our own study, an attempt was made to compare the overall result obtained from the satisfaction with the doctor-patient communication depending on the selected variables. In the analysis, women had a significantly higher level of satisfaction with communication with their doctor than men (56.97±12.56 vs 53.93±11.82; p=0.018). The results of our study are in accordance with other publications.10,18 The low assessment given by men may be explained by the fact that men are reluctant to both ask for help when they experience health problems and talk about these.19 If they finally see the doctor, their communication style will be influenced by their male gender identity. However, the gender issue also applies to the doctor themself. The review shows that patients talked to female doctors more than male doctors, revealed more biomedical and psychosocial information and made more positive statements to female doctors. Patients were more assertive towards doctors and interrupted more often. Partner statements were much more frequently addressed to women than to male physicians. This concerned visits to the general practitioner, but not the obstetrician and gynaecologist.20
Satisfaction with the doctor-patient communication depends on the time devoted and doctor’s attention. It is important for patients to discuss their health problems and concerns and to be listened to when they talk about them. In our own study, the average time spent on a visit exceeded the standards set by the National Health Fund and the vast majority of this time was focused on talking about the patient’s problems. The results of the correlation showed that the duration of a medical visit has a significant impact on the level of satisfaction and the longer it is, the higher the level of patient satisfaction. Available Polish studies confirm that patients respect the time spent at the doctor’s and appreciate the opportunity to talk during the visit. In another Polish study, as many as 91% of patients considered the time devoted by a doctor as sufficiently long and the activities performed as accurate and satisfactory.21
Nowadays, patients are not passive participants of the treatment. In our study, the lowest scores were obtained for “encouraged me to ask questions” and “involved me in decisions as much as I wanted”. Patients highly appreciated the comprehensibility of the message. In several surveys on communication, the importance of explaining the causes and symptoms of the disease by a physician or symptoms troubling patients has been confirmed. However, as the results show, the percentage of satisfied patients is still low.22
In our study, patients who have a permanent doctor are more satisfied with the visit than those who change their specialist a few times a year. This may be caused by the fact that the doctor knows the patient’s medical history, has worked out a way of communicating with the patient, and the conditions and possibilities of the visit are suitable for the patient. It is known that the possibility of a free choice of a PCP is a factor increasing their satisfaction with medical services.23
The group surveyed was characterised by being over 60 years of age and having a high percentage of people with primary and secondary education. Older patients with low educational attainment have a higher rate of insufficient health literacy, which is a significant communication barrier for healthcare providers to ensure adequate healthcare. Lack of adequate literacy skills and the concealment of this fact from doctors through shame creates a vicious circle that can be broken by establishing a good doctor–patient relationship. If doctors can help such patients to become involved in healthcare, it will directly improve the physician–patient relationship and also partly mediate the influence of the health surveillance site on that relationship.18
Strength and Limitation
This study is the first to translate and validate the CAT into the Polish language. The survey was forward- and back-translated from English to Polish. There was no comparison of perceptions of doctor-patient communication depending on the gender of the doctor. This study addresses communication between patients and physicians dealing with only hypertension in outpatient conditions.
Conclusion
The CAT is a very good tool for assessing the quality of communication in Polish-speaking settings and can be recommended for use in everyday practice. Women, persons receiving regular medical care, and those arranging regular check-up visits tended to rate doctor communication more highly. A factor influencing satisfaction is the duration of a medical visit and the time focused on conversation about the patient’s problems (the longer the visit, the greater the satisfaction).
Implications
- Pre- and post-diploma communication training for physicians must be standard and physicians should be able to impart communication skills to everyday practice.
- The introduction of a standard evaluation with feedback on the results will lead to an improvement in the quality of services provided and will increase the involvement of both patients and physicians.
Study Limitations
While there are many strengths to this study, it is not without limitations. One such limitation is the lack of retest analysis, which would certainly emphasise the merits of our study. A further limitation is the patient sample, which firstly was drawn from only one centre and secondly, was analysed by different doctors. Another limitation is the diversity in the number of visits made by patients over the course of the last year.
In Poland, there is also a lack of standardised tools for evaluating satisfaction with communication, which resulted in our comparing the results of the CAT questionnaire results with those of the PRF questionnaire, and this might also be a limitation of our study.
Data Sharing Statement
Data are available on reasonable request. The data are available by request from the corresponding author after appropriate ethics approval.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Written informed consent was obtained from all individual participants included in the study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Horowitz SD. Evaluation of clinical competencies: basic certification, subspecialty certification, and recertification. Am J Phys Med Rehabil. 2000;79:478–480. doi:10.1097/00002060-200009000-00016
2. Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm. A New Health System for the 21st Century; 2001. Available from: https://www.ncbi.nlm.nih.gov/books/NBK222274/pdf/Bookshelf_NBK222274.pdf.
3. Street RL, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. 2009;74:295–296. doi:10.1016/j.pec.2008.11.015
4. Zolnierek KBH, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47:826–828. doi:10.1097/MLR.0b013e31819a5acc
5. Travaline JM, Ruchinskas R, D’Alonzo GE. Patient-physician communication: why and how. J Am Osteopath Assoc. 2005;105:13–15.
6. Duffy FD, Gordon GH, Whelan G, et al. Assessing competence in communication and interpersonal skills: the Kalamazoo II report. Acad Med. 2004;79:495–512. doi:10.1097/00001888-200406000-00002
7. Surmacka J, Motyka M. Problems in clinical communication problems involving hospitalised patients. Nurs Topics. 2015;23(3):386–391.
8. Zill JM, Christalle E, Müller E, Härter M, Dirmaier J, Scholl I. Measurement of physician-patient communication-a systematic review. PLoS One. 2014;9(12):e112637. doi:10.1371/journal.pone.0112637
9. Makoul G, Krupat E, Chang CH. Measuring patient views of physician communication skills: development and testing of the Communication Assessment Tool. Patient Educ Couns. 2007;67(3):333–342. doi:10.1016/j.pec.2007.05.005
10. Iversen ED, Steinsbekk A, FalbeVind B, et al. Translation and cultural adaptation of the Communication Assessment Tool (CAT), developing a Danish and Norwegian version. [published online ahead of print March 28, 2019]. Int J Qual Health Care. 2019;31:748–751. doi:10.1093/intqhc/mzz020
11. Scala D, Menditto E, Armellino MF, et al. Italian translation and cultural adaptation of the communication assessment tool in an outpatient surgical clinic. BMC Health Serv Res. 2016;16:163. doi:10.1186/s12913-016-1411-9
12. Cubaka VK, Schriver M, Vedsted P, et al. Measuring patient-provider communication skills in Rwanda: selection, adaptation and assessment of psychometric properties of the Communication Assessment Tool. Patient Educ Couns. 2018;101(9):1601–1610. doi:10.1016/j.pec.2018.04.010
13. Paquete VC CAT - Aplicação do Communication Assessment Tool a profissionais de saúde: validação do instrumento no contextoportuguês. [Validation of the self-assessment of communication skills and professionalism for nurses]. Available from: https://www.repositorio.ul.pt/handle/10451/27058.
14. Altin SV, Lorrek K, Stock S. Development and validation of a brief screener to measure the Health Literacy Responsiveness of Primary Care Practices (HLPC). BMC Fam Pract. 2015;16:122. doi:10.1186/s12875-015-0336-4
15. Yoo MN, Chae SM. Effects of peer review on communication skills and learning motivation among nursing students. J Nurs Educ. 2011;50:230–233. doi:10.3928/01484834-20110131-03
16. Kripalani S, Risser J, Gatti ME, Jacobson TA. Development and evaluation of the Adherence to Refills and Medications Scale (ARMS) among low-literacy patients with chronic disease. Value Health. 2009;12(1):118–123. doi:10.1111/j.1524-4733.2008.00400.x
17. R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing; 2019. Available from: https://www.R-project.org/.
18. Liang CY, Wang KY, Hwang SJ, et al. Factors affecting the physician–patient relationship of older veterans with inadequate health literacy: an observational study. Br J Gen Pract. 2013;63(610):e354–e360. doi:10.3399/bjgp13X667222
19. Addis ME, Mahalik JR. Men, masculinity, and the contexts of help seeking. Am Psychol. 2003;58(1):5–14. doi:10.1037/0003-066X.58.1.5
20. Hall JA, Roter DL. Do patients talk differently to male and female physicians? A meta-analytic review. Patient Educ Couns. 2002;48(3):217–224. doi:10.1016/S0738-3991(02)00174-X
21. Łukomska A, Rość D, Jachimowicz-Wołoszynek D. Wpływ wieku na poziom satysfakcji pacjentów korzystających z usług lekarza rodzinnego. [Influence of age on patient satisfaction in primary health care]. Fam Med Primary Care Rev. 2006;8(1):88–94. Polish.
22. Rudzka D, Stecka B. Dobra praktyka lekarza rodzinnego. [Good practice of a family doctor]. Lek Rodz. 2008;13(1):94. Polish.
23. Kurpas D, Steciwko A. Satysfakcja pacjenta jako główny wskaźnik poziomu jakości podstawowej opieki zdrowotnej. [Patient satisfaction measure of the quality of primary health care]. Przegl Lek. 2005;62(12):1546–1551. Polish.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.