")
Back to Journals » International Journal of General Medicine » Volume 15
Translation and Cross-Cultural Adaptation of the Japanese Version of the INTERMED Self-Assessment Questionnaire (IMSA) for Patient-Case Complexity Assessment
Authors Yokokawa D , Shikino K , Kishi Y, Ikusaka M
Received 8 April 2022
Accepted for publication 19 July 2022
Published 28 July 2022 Volume 2022:15 Pages 6309—6313
DOI https://doi.org/10.2147/IJGM.S369056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Daiki Yokokawa,1 Kiyoshi Shikino,1 Yasuhiro Kishi,2 Masatomi Ikusaka1
1Department of General Medicine, Chiba University Hospital, Chiba, Japan; 2Department of Psychiatry, Nippon Medical School Musashikosugi Hospital, Kanagawa, Japan
Correspondence: Daiki Yokokawa, Department of General Medicine, Chiba University Hospital, 1-8-1 Inohana, Chuo-ku, Chiba City, Chiba, 260-8677, Japan, Tel/Fax +81-43-224-4758, Email [email protected]
Purpose: This study aims to translate and ensure cross-cultural adaptation of a Japanese version of the INTERMED Self-Assessment Questionnaire (IMSA).
Methods: A family medicine physician, a medical education specialist, a psychiatrist who prepared the Japanese version of the INTERMED, and two members of the INTERMED consortium were selected as committee members. We used the standard forward and backward translation method to translate the IMSA into Japanese. After translating the original IMSA into Japanese, all committee members discussed and reached a consensus on the proposed translation. The back-translation was performed by an English native professional translator who did not know the original text. We contacted the INTERMED consortium and asked them to review the conceptual equivalence of the back-translated Japanese version with the original version; after two reviews, the members approved the Japanese version. Thereafter, we conducted cognitive debriefings with four patients and nine healthcare professionals to ensure cross-cultural adaptation.
Results: The members of the INTERMED consortium approved the use of the Japanese version. We modified some expressions and words, while retaining the original meaning, to make it easier for Japanese patients to understand.
Conclusion: We developed a Japanese version of the IMSA. A future study will investigate the construct criterion-related validity and the reliability of the scale.
Keywords: IMSA, Japanese version, translation, patient-case complexity
Introduction
The INTERMED is a multidimensional rating scale developed by Huyse et al to reflect the physical, psychological, and social approaches that are required to plan the treatment of hospitalized patients.1,2 It can quantitatively assess and describe the patient-case complexity based on four domains: biological, psychological, social, and health care. Every domain is divided into three-time segments: history, current state, and prognosis. It assesses biopsychosocial complexity,3 identifies patients at risk for adverse outcomes4 and those who have health care needs,1,2,4 predicts prolonged hospital stay,2,5,6 and improves complex patient outcomes.7 The INTERMED was developed to assess the complexity of patients’ diseases, and its validity and reliability has been demonstrated.1,8 The INTERMED has shown good psychometric validity in the primary health care population.9 The reliability of the Japanese version of the INTERMED has been confirmed.10
We have presented an instance of high patient-case complexity as follows.
An 85-year-old man had multiple bone metastases from prostate cancer, a history of old myocardial infarction, diabetes mellitus, and alcohol use disorder. He was hospitalized for recurrent lower leg cellulitis and treated with antimicrobial agents. During his hospitalization, he developed delirium. He had always walked with a cane, but his walking function deteriorated during this hospitalization. He lived alone and had difficulty living at home after discharge from the hospital. He had biological, psychological, and social problems.
In Japan, the number of such patients is increasing owing to the rising age of the population. Higher patient-case complexity is associated with longer hospital stays.11
Despite its usefulness in clinical practice, the INTERMED has not been widely adopted in clinical settings. The INTERMED Self-Assessment Questionnaire (IMSA) was developed for use in various clinical settings to foster a patient’s perspective on health care needs.12,13 The main difference between the IMSA and the INTEMED is that the IMSA is a self-assessed questionnaire. The IMSA has a similar structure to the INTERMED. The maximum score for the IMSA is 60 points, with 19 points as the cutoff; scores above 19 points denote high complexity. This instrument assesses biopsychosocial complexity, healthcare needs, and barriers to receiving standard care. Moreover, the IMSA score indicates an individual’s level of healthcare need complexity. To determine the complexity of patients per time segment and per domain, the scores of the single questions were added as shown in Figure 1.
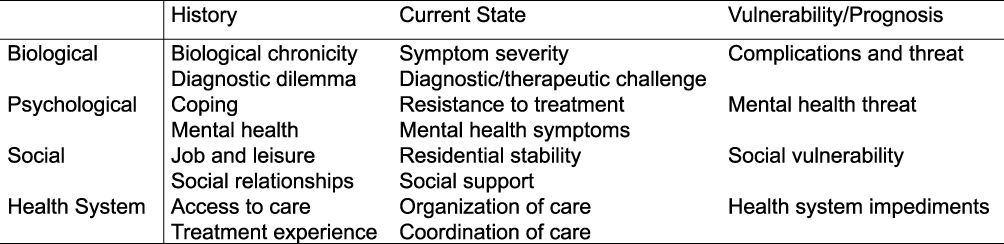 |
Figure 1 The Self-Assessment Questionnaire of INTERMED questions per domain (from Manual IM-SA following revision by the authors) Data from reference 13.13 |
The IMSA is one of the few self-assessment screening tools available to identify patients with high biopsychosocial complexity. It is a versatile and time-efficient method for assessing the biopsychosocial complexity of adult patients and has good reliability and validity across different cultures.10 A recent scoping review, which aimed to find a quick (<15 minutes) and valuable screening tool to identify all adults with complex health needs who are at risk for high utilization of health services, revealed that most tools are targeted at older adults.14 The IMSA was the only questionnaire targeted at adults in general. However, although the IMSA has been translated into many languages, it currently has no Japanese translated version. Thus, this study aims to develop a Japanese version of the IMSA.
Materials and Methods
The English version of the IMSA is freely accessible through its web page.13 We used the standard forward and backward translation method to translate the IMSA into Japanese.15 The authors of the study, which included a family medicine physician (DY), a medical education specialist (KS) who is not familiar with the IMSA, a psychiatrist who created the Japanese version of the INTERMED (YK), and members of the INTERMED consortium (AB and SF) were selected as committee members. The committee held meetings as needed at each stage of the back-translation process.
First, DY and KS independently translated the original IMSA into Japanese. They synthesized the translations and resolved any discrepancies. Subsequently, DY, KS, and YK discussed and reached a consensus on the proposed translation and later prepared a back-translation into English. The back-translation was performed by a professional translator, who was a native English speaker and unaware of the original text. We contacted members of the INTERMED consortium (AB and SF) and asked them to review the conceptual equivalence of the back-translated Japanese version with the original version. After two serial reviews, all committee members approved the Japanese version.
Thereafter, we conducted cognitive debriefings with 13 participants (two physicians, seven nurses, and four patients). Participants were selected from physician colleagues, nurses, and consenting patients. The exclusion criterion was failure to obtain consent. The participants read the Japanese version and completed the questionnaire by checking the fluency of the sentences, the clarity of the words used, and the clarity of the text. Then, DY and participants discussed the points that were checked through the personal interview. DY, KS, and YK reviewed all issues and made minor modifications to the wording to improve the clarity and understandability based on the results. This study is a pre-test of a study approved by the Ethics Board of Chiba University Hospital (No. 2731). Participants in the cognitive debriefing received an explanation of the purpose of the study from the author (DY), and consent for the study was obtained by answering the questionnaire.
Results
Only two items required minor modification in the review of the back-translated Japanese version of the IMSA. The phrase “I have contacts with others, though now and then it might become tense” in item 10 in the original version was translated to “I interact with other people, but it sometimes makes me nervous.” In the original version, the text reads “it might become tense”, meaning that things may become difficult, tense, and conflicting, and not, as it seems in our translation, “I get nervous when I interact with people.” Thus, we translated it as “tense relationships” to avoid conveying nervous intention.
We also revised the text for item 15 (Table 1) and its answer. The original version for option (b) indicates a condition when patients only need basic assistance. Private practice is generally used to refer to consultants; thus, it indicates second-level care. The difference between options (b) and (c) (which also includes a general practitioner [GP]) is that option (b) indicates the need for a GP without a medical condition, that is, patients need medical assistance that only requires a GP’s attention. However, they choose option (c) if they have at least one medical condition. Thus, we added the phrase (not seen continuously) at the end of the sentence in option (b). However, since GPs are not recognized as specialists in Japan, the original version in option (c) “general practitioner” was translated as a general internist in the revised version.
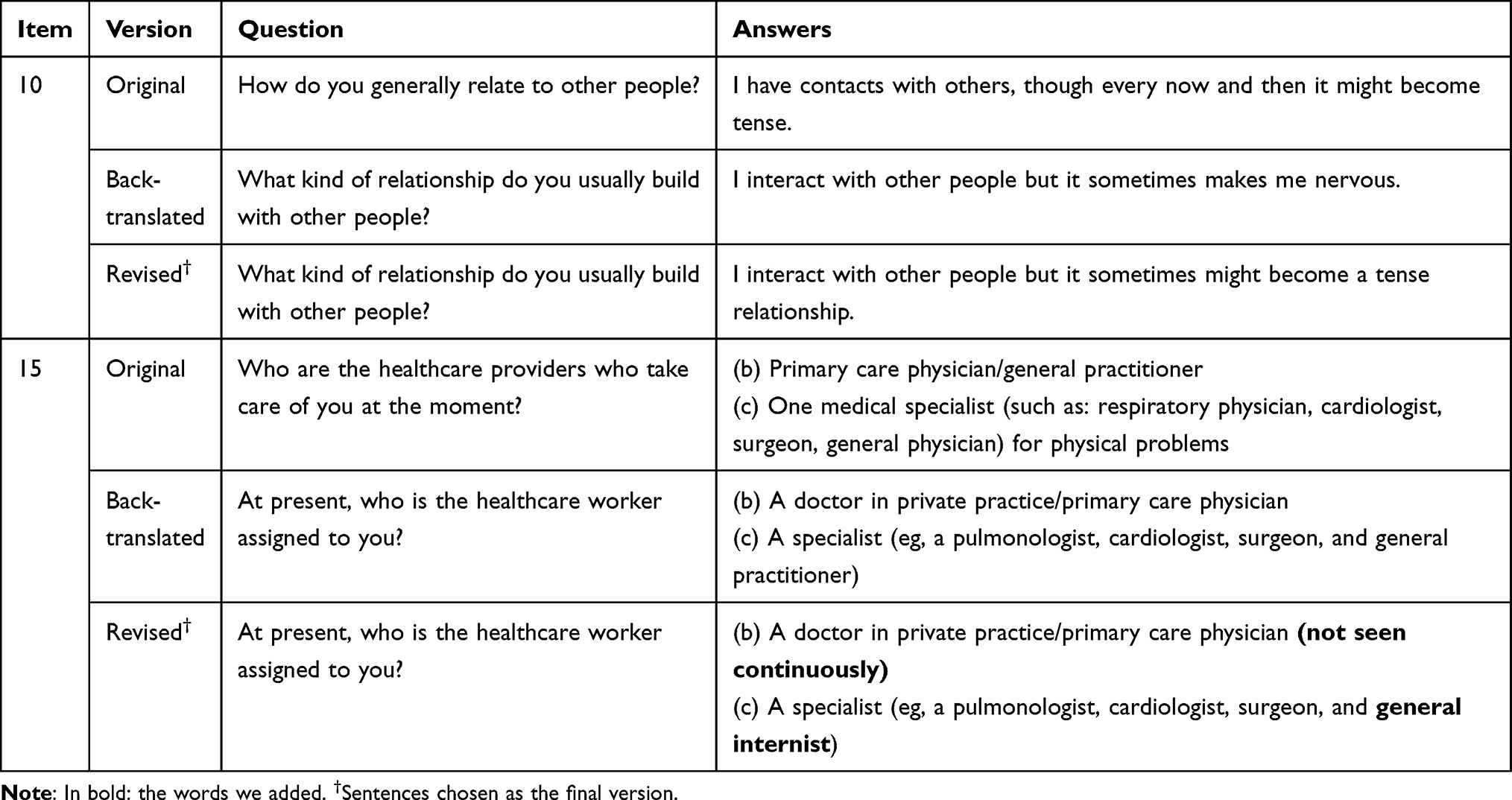 |
Table 1 Original, Back-Translated, and Revised Versions of Items 10 and 15. |
In the cognitive briefing, responses were obtained from all 13 participants. We corrected the following: 1. We attached a sample check on how to respond. 2. We revised “Dear Patients”, which was translated from “Dear Sir/Madam” on the front cover to “Dear Patient.” 3. In item 4a, we added “I think” to the beginning of the answers (b) “My doctors do understand the origin of my current physical problem/s” and (c) “My doctors understand the origin of my current physical problem/s but they have some doubts.” 4. We revised “your carer”, which was translated from “health caregivers” in item 7, to “health care professionals.” 5. In item 13, stating “Yes, some of these are big problems for me”, we revised “these are big problems” to “there are big problems.” 6. We added “Q” to each item to improve clarity. We were more interested in whether the participants understood the questionnaire and completed it.
Discussion
In this study, we translated the IMSA into Japanese. In general, when developing a self-administered questionnaire, it is necessary to choose easy-to-understand expressions and words that facilitate the understanding and response of the target audience.16 It was also necessary to select terms in line with the Japanese culture and the healthcare delivery system.15 Patients living in Japan can visit any medical institution they prefer.17 Therefore, some patients do not have GPs as gatekeepers who first see the patient and are responsible for referring the patient to a specialist, as is the case in some European countries.18 They may not be familiar with the terms “primary care physician”, “general practitioner”, or “private practice”. This may be due to the small number of trained primary care physicians in Japan.19 We revised the wording and added supplementary information, without compromising the original meaning, based on feedback from patients and healthcare professionals.
A previous study that used the IMSA revealed that it was effective in predicting healthcare and social costs for orthopedic trauma patients with persistent disabilities.20 Unfortunately, only a few studies have utilized the IMSA thus far. It is hoped that the development of the Japanese form of the IMSA will increase its use in Japan, where the increase in medical costs has become a social problem.
In this study, we developed a Japanese version of the IMSA. To identify all adults with complex health needs, reliability and validity assessments of the Japanese version of the IMSA are needed for use in various settings. In the future, we would like to examine the convergent validity (comparison of the IMSA with the Japanese version of the INTERMED and quality-of-life scale [SF-36v2]), divergent validity (comparison of the IMSA with Hospital Anxiety and Depression Scale), criterion-related validity, and reliability of the scale. There are several potential limitations to this report: first, during the back-translation process, it was not possible to hire two individual translators due to budget constraints. The recommendations advise that for effective back-translation, a minimum of two back-translators, who are native speakers of the original language and blinded to the original version, should be used.15 The translation was outsourced to Honyaku Center Inc. and was handled by a translator and a native checker with extensive experience in the pharmaceutical field. Second, the number of people involved in the cognitive debriefing process conducted to verify that all items were appropriate and understood by patients was small (13 people). Based on this report, we plan to expand the target group in the future.
Conclusion
The IMSA is one of the few self-administered screening tools designed to address patient-case complexity, which has been translated into many languages; however, currently, there is no Japanese translated version. Therefore, we successfully developed a Japanese version of the IMSA in this study.
Abbreviations
IMSA, INTERMED Self-Assessment Questionnaire; GP, general practitioner.
Data Sharing Statement
The Japanese version of the IMSA and data are available upon request to the corresponding author.
Ethics Approval and Informed Consent
This study is a pre-test of a study approved by the Ethics Board of Chiba University Hospital (No. 2731). Participants in the cognitive debriefing received an explanation of the purpose of the study from the author (DY), and consent for the study was obtained by answering the questionnaire.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huyse FJ, Lyons JS, Stiefel FC, et al. “INTERMED”: a method to assess health service needs. I. Development and reliability. Gen Hosp Psychiatry. 1999;21(1):39–48. doi:10.1016/S0163-8343(98)00057-7
2. De Jonge P, Huyse FJ, Stiefel FC, Slaets JPJ, Gans ROB. INTERMED—a clinical instrument for biopsychosocial assessment. Psychosomatics. 2001;42(2):106–109. doi:10.1176/appi.psy.42.2.106
3. Duong HP, Konzelmann M, Vuistiner P, et al. Psychiatric comorbidity and complex regional pain syndrome through the lens of the biopsychosocial model: a comparative study. J Pain Res. 2020;13:3235–3245. doi:10.2147/JPR.S278614
4. Mazzocato C, Stiefel F, De Jonge P, Levorato A, Ducret S, Huyse FJ. Comprehensive assessment of patients in palliative care: a descriptive study utilizing the INTERMED. J Pain Symptom Manage. 2000;19(2):83–90. doi:10.1016/S0885-3924(99)00156-6
5. De Jonge P, Bauer I, Huyse FJ, Latour CHM. Medical inpatients at risk of extended hospital stay and poor discharge health status: detection with COMPRI and INTERMED. Psychosom Med. 2003;65(4):534–541. doi:10.1097/01.PSY.0000077504.01963.1B
6. Lobo E, De Jonge P, Huyse FJ, Slaets JPJ, Rabanaque MJ, Lobo A. Early detection of pneumology inpatients at risk of extended hospital stay and need for psychosocial treatment. Psychosom Med. 2007;69(1):99–105. doi:10.1097/PSY.0b013e31802e46da
7. Stiefel F, Zdrojewski C, Bel Hadj F, et al. Effects of a multifaceted psychiatric intervention targeted for the complex medically ill: a randomized controlled trial. Psychother Psychosom. 2008;77(4):247–256. doi:10.1159/000129658
8. Stiefel FC, De Jonge P, Huyse FJ, et al. “INTERMED”: a method to assess health service needs. II. Results on its validity and clinical use. Gen Hosp Psychiatry. 1999;21(1):49–56. doi:10.1016/S0163-8343(98)00061-9
9. Oliveira CA, Weber B, Dos Santos JLF, et al. Health complexity assessment in primary care: a validity and feasibility study of the INTERMED tool. PLoS One. 2022;17(2):e0263702. doi:10.1371/journal.pone.0263702
10. Kishi Y, Matsuki M, Mizushima H, Matsuki H, Ohmura Y, Horikawa N. The INTERMED Japanese version: inter-rater reliability and internal consistency. J Psychosom Res. 2010;69(6):583–586. doi:10.1016/J.JPSYCHORES.2010.02.006
11. Yokokawa D, Shikino K, Kishi Y, et al. Does scoring patient complexity using COMPRI predict the length of hospital stay? A multicentre case–control study in Japan. BMJ Open. 2022;12(4):e051891. doi:10.1136/BMJOPEN-2021-051891
12. Boehlen FH, Joos A, Bergmann F, et al. Evaluation of the German version of the “INTERMED-self-assessment”-questionnaire (IM-SA) to assess case complexity. Psychother Psychosom Med Psychol. 2016;66(5):180–186. In German. doi:10.1055/s-0042-104281
13. Instrument. Intermed Consortium. Available from: http://www.intermedconsortium.com/instrument/.
14. Marcoux V, Chouinard MC, Diadiou F, Dufour I, Hudon C. Screening tools to identify patients with complex health needs at risk of high use of health care services: a scoping review. PLoS One. 2017;12(11):e0188663. doi:10.1371/JOURNAL.PONE.0188663
15. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
16. Davis TC, Mayeaux EJ, Fredrickson D, Bocchini JA, Jackson RH, Murphy PW. Reading ability of parents compared with reading level of pediatric patient education materials. Pediatrics. 1994;93(3):460–468. doi:10.1542/PEDS.93.3.460
17. Nomura H, Nakayama T. The Japanese healthcare system. BMJ. 2005;331(7518):648–649. doi:10.1136/bmj.331.7518.648
18. Gérvas J, Pérez Fernández M, Starfield BH. Primary care, financing and gatekeeping in Western Europe. Fam Pract. 1994;11(3):307–317. doi:10.1093/fampra/11.3.307
19. Yoshida S, Matsumoto M, Kashima S, Koike S, Tazuma S, Maeda T. Geographical distribution of family physicians in Japan: a nationwide cross-sectional study. BMC Fam Pract. 2019;20(1). doi:10.1186/S12875-019-1040-6
20. Burrus C, Vuistiner P, Léger B, Stiefel F, Rivier G, Luthi F. The self-assessment INTERMED predicts healthcare and social costs of orthopaedic trauma patients with persistent impairments. Clin Rehabil. 2021;35(1):135–144. doi:10.1177/0269215520949170
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.