")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 12
Transient Eosinophilic Granulomatosis with Polyangiitis-Like Vasculitis During Omalizumab Therapy: A Case Report
Authors Elhadari S , Hamad M
Received 1 May 2020
Accepted for publication 30 June 2020
Published 14 July 2020 Volume 2020:12 Pages 127—131
DOI https://doi.org/10.2147/OARRR.S259746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Sara Elhadari, Mahir Hamad
Acute Medicine Department, The James Cook University Hospital, Middlesbrough, TS4 3BW, UK
Correspondence: Sara Elhadari Email [email protected]
Abstract: A 67-year-old Caucasian female presented in August 2019 to our rheumatology service, with 3 days history of severe neck pain and right-sided headache with aches in both shoulders and arms and mild stiffness. Other symptoms included mild jaw claudication. She had recently returned from Majorca after an uneventful two-week trip. She had a background of severe allergic asthma and allergic rhinitis, well controlled with omalizumab which was started in 2016, based on persistently high IgE. Her sister suffers from a type of vasculitis and is currently on steroids. The patient is an ex-smoker and drinks two bottles of wine a week. She had high inflammatory markers with raised eosinophilic count and was admitted for further work up to rule out infection and to commence steroid after for a likely diagnosis of eosinophilic granulomatosis with polyangiitis. Shortly after admission to the acute assessment unit, she became confused and febrile. An extensive work up ruled out infection, and she was started on steroids and treated for acute hyponatremia. Omalizumab was stopped. She improved and was discharged on a tapering dose of steroids and was weaned off completely within 4 months. Her inflammatory markers returned to normal as well as her eosinophilic count, with complete resolution of her presenting symptoms.
Keywords: EGPA, ANCA, vasculitis, Churg-Strauss syndrome, eosinophilia, anti-IgE antibodies
Introduction
Omalizumab is a recombinant humanized antibody of IgG1k subclass targeted against IgE for the treatment of moderate to severe asthma. It is unclear whether omalizumab can cause eosinophilic granulomatosis with polyangiitis (EGPA), however different reports described the occurrence of EGPA while on omalizumab in patients with asthma or vasculitic urticaria. Interestingly, omalizumab is used to treat asthma in EGPA with success. We report a case of a lady, who was on omalizumab for more than 3 years presenting with EGPA like vasculitis which resolved completely after treatment with steroids and discontinuation of omalizumab.
Case Presentation
We present a case of a 67-year-old, right-handed, retired administrator female, referred urgently by her GP to the rheumatology service, with 3-days history of severe neck pain radiating to both shoulders and shoulder blades with aches in both arms. She also had a severe persistent headache in the right temporal and orbital areas. Both her headache and neck pain were severe and only marginally helped with analgesia including paracetamol, ibuprofen and codeine. She also had jaw pain on chewing as well as exquisite pain over her temple and occipital region. She had some neck stiffness but no restriction to movement of the neck or shoulders. She had no muscle stiffness or symptoms around her pelvic girdle or lower limbs. There was some blurring of vision but no visual loss or diplopia and there was no limb claudication. She also complained of episodic sore throat with odynophagia. She denied fever, sweats or weight loss; however, her appetite was reduced. There were no respiratory, gastrointestinal, urinary or neurological symptoms. There were no other extra-articular features and no history of altered sensorium. She had been on a holiday to Majorca 2 weeks prior to the presentation and had a background of severe allergic asthma and allergic rhinitis diagnosed in 1996 with multiple environmental allergies. Because of persistently raised IgE and recurrent asthma exacerbation, she was commenced on omalizumab injections in 2016. Azithromycin 250 mg three times a week was also added over the months October to April for better control. Short courses of steroids for asthma exacerbations were given once or twice a year during omalizumab therapy. She also had previous septoplasty and chronic plaque psoriasis of the extensor surfaces of the upper limb since her teenage years, tolerated and treated with calcipotriol (as monohydrate) and betamethasone (as dipropionate) ointment with the last flare up in 2009 treated with narrow-band phototherapy (UVB) and emollient creams.
Her regular medication included omalizumab 375 mg fortnightly subcutaneous injections, Symbicort 200/6 Turbo haler (120-dose) one puff twice daily and Dymista 137 µg/dose/50 µg/dose nasal spray one puff twice daily.
Family history revealed a sister with a type of vasculitis and currently on steroids. Her father suffered from osteoarthritis. She is a widow and has three children who are fit and well. She gave up smoking 40 years ago and drinks two bottles of wine a week and lives independently on her own.
On examination, she looked well, and general peripheral examination was unremarkable. Peripheral pulses were well palpable. There was no lymphadenopathy or bruit. Her blood pressure was high at 198/106 in the right arm and 198/107 in the left arm. She weighed 54 Kg. She did not have any temporal artery tenderness and both temporal arteries were well palpable, however she had some tenderness over frontal and ethmoidal sinuses. There were no peripheral stigmata of vasculitis or connective tissue diseases. The rest of the clinical examination was unremarkable including the musculoskeletal system.
A temporal artery ultrasound scan did not reveal any ultrasound evidence of temporal arteritis. Initial investigations are summarized (Table 1).
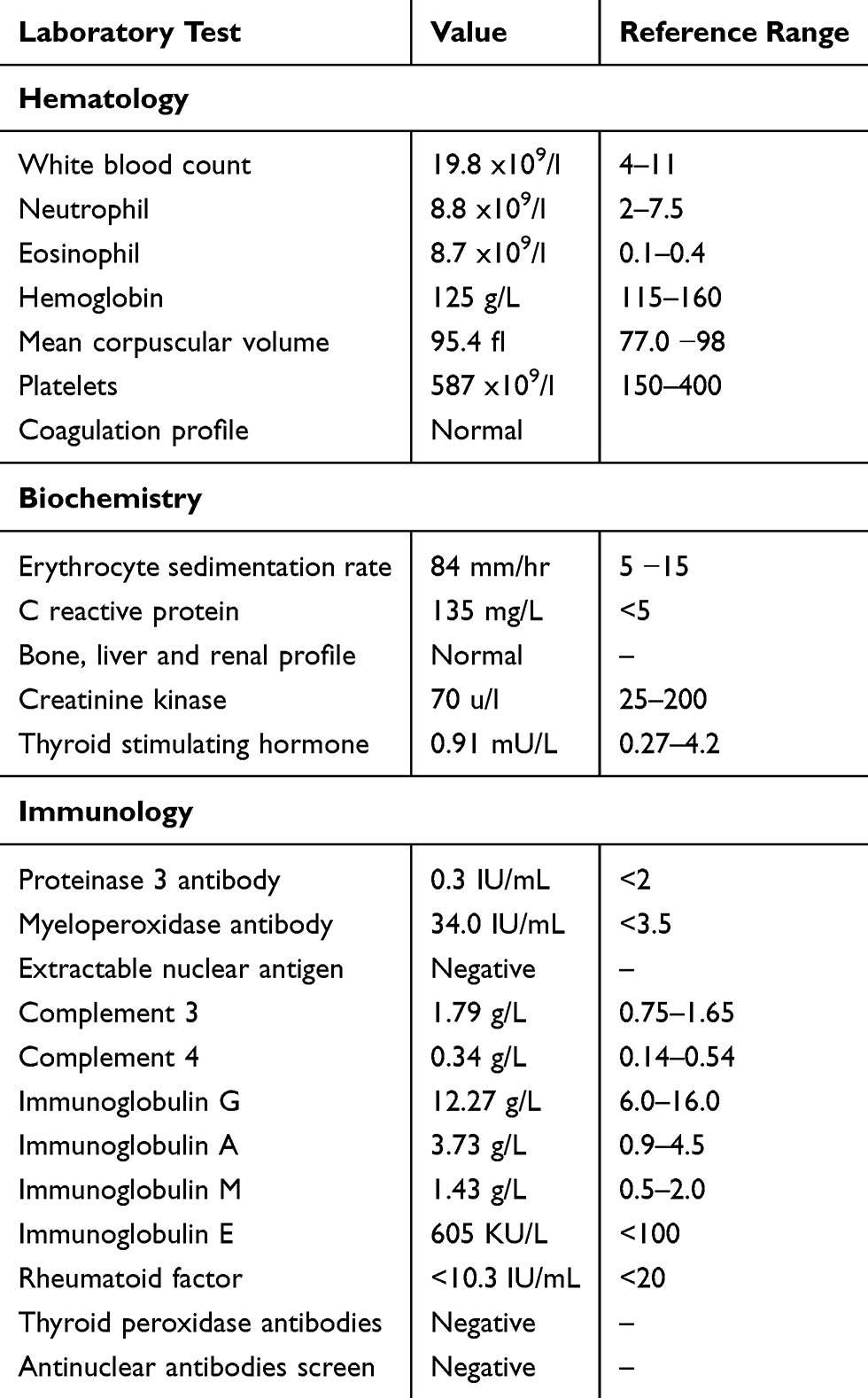 |
Table 1 Initial Investigation |
She was admitted to the acute assessment unit for further investigations and to rule out infection before commencing her on steroids for a likely diagnosis of EGPA.
Two days later, she developed a fever and became confused. She was noted to have an ejection systolic murmur on cardiac examination. Repeat blood tests showed profound hyponatremia (Table 2). A CT scan of the head and neck followed by a brain MRI showed enhancing soft tissue mass at the right submandibular area of indeterminate nature, but was otherwise normal. Arterial spine labelling MRI, MR Venography of the cerebral veins and MR angiograph of the circle of Willis showed no acute large hemispheric subdural collection, The FLAIR suggests multiple white matter, basal ganglia, and pons as well as general subcortical changes due to underlying small vessel cerebrovascular disease. No mass effect or midline shift was seen. The paranasal sinuses demonstrate right circular mucosal thickness.
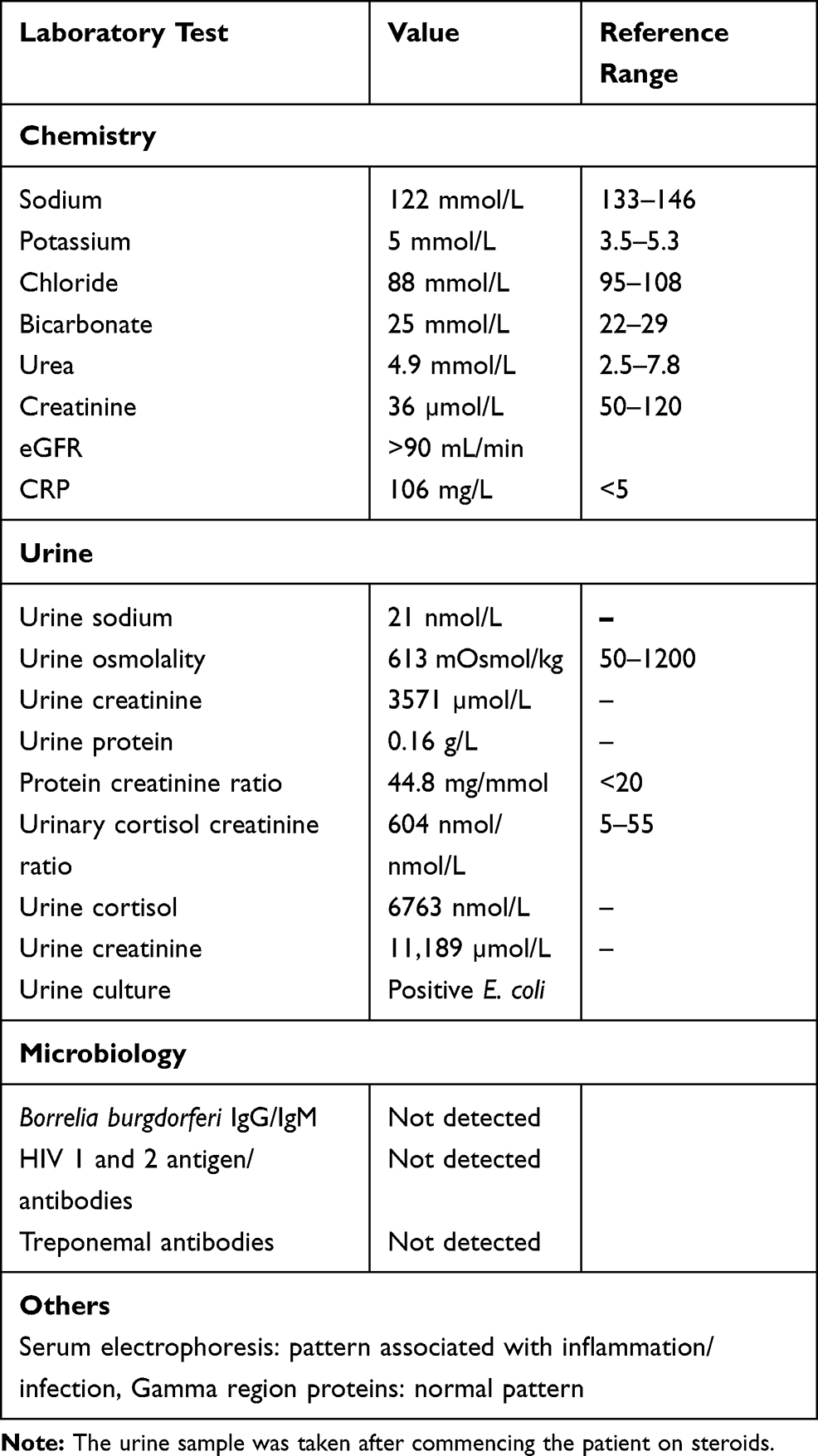 |
Table 2 Further Investigations |
An EEG was requested based on a neurologist’s advice to rule out encephalitis. It showed bi-frontal abnormalities with emphasis on the left and possible minor temporal involvement. There was no evidence to point strongly to diffuse encephalitis, however focal encephalitis was possible but the distribution of abnormalities was not typical of herpes simplex and there were no periodic complexes to point to this condition. She was started on acyclovir which was discontinued after 3 days as lumbar puncture was normal with no growth after 48 hrs and cerebrospinal fluid (CSF) polymerase chain reaction (PCR) for Herpes simplex type 1 and 2, varicella zoster, parvovirus and enterovirus was negative.
To investigate the murmur, an Echocardiogram showed mild Aortic Regurgitation (AR), small pericardial effusion, no haemodynamic compromise, normal size and function of both ventricles. A neck ultrasound showed dilated ducts in the submandibular salivary gland (SMG) and both parotid glands, and multinodular thyroid. As EGPA has pulmonary involvement a Chest x-ray was requested followed by high-resolution computed tomography (HRCT) scan which showed central bronchial dilatation, abnormal inflammatory/atelectasis in the left apex, no focal mass lesion in this area.
Treatment and Referrals
The below table lists the treatments recommended by each department on referral (Table 3).
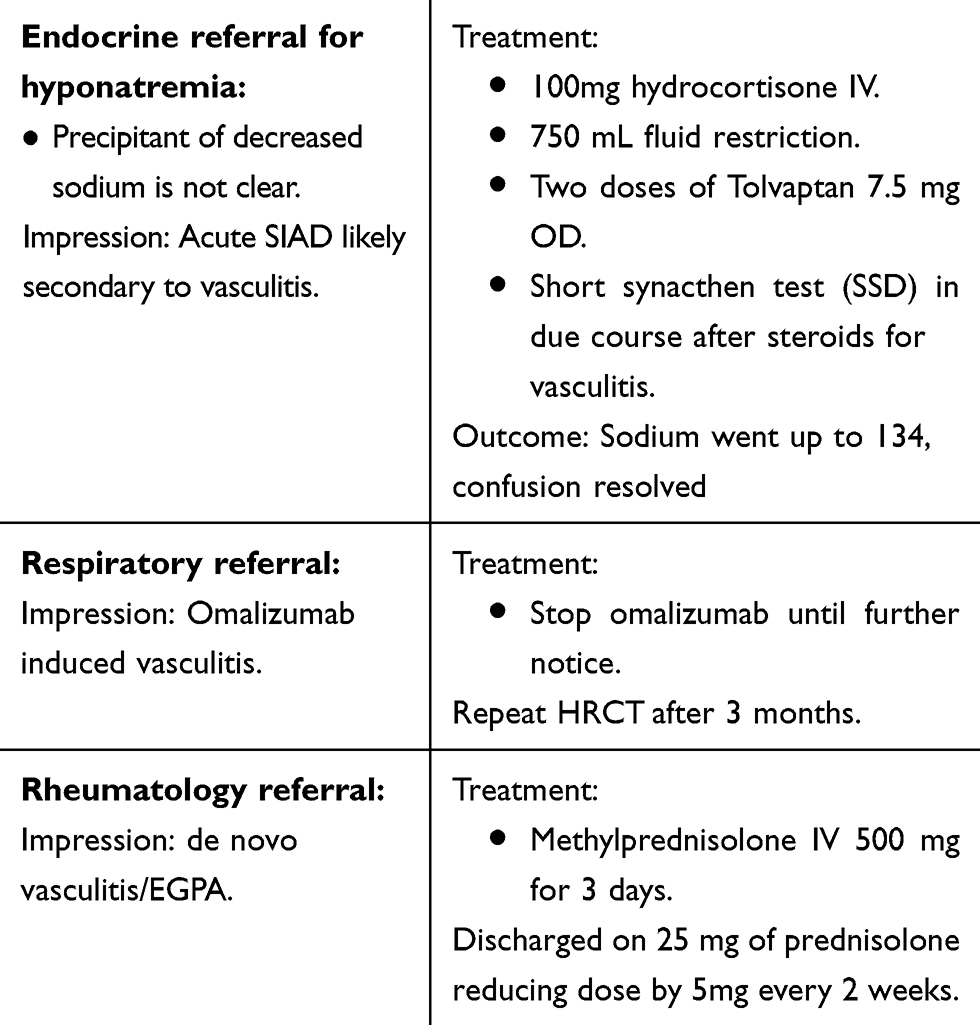 |
Table 3 Referrals and Treatments |
Outcome and Follow-Up
During the 8-months follow-up period, she continued to improve gradually and was weaned off steroids which were given for a total of 4 months after her admission. However, she was concomitantly experiencing increasing cough and mucous production but coping relatively well. Repeat blood tests, including inflammatory markers as well as eosinophilic count and Myeloperoxidase antibodies (MPO) were taken and were all back to normal range remaining so when repeated 2 months after steroid discontinuation. Her sodium levels remained within normal range. She was seen in the respiratory outpatient clinic and was started on prophylactic azithromycin during wintertime along with her usual inhaler and nasal spray. Moreover, she was advised not to restart omalizumab at this time.
Discussion
EGPA is a systemic necrotizing granulomatous inflammation often involving the respiratory tract, and necrotizing vasculitis predominantly affecting small to medium vessels and associated with asthma and eosinophilia.1
There are no clinical diagnostic criteria for EGPA, however, for research purposes, the American College of Rheumatology 1990 criteria suggests the presence of EGPA if four or more of six clinical criteria in the setting of vasculitis were met: Asthma, Peak peripheral eosinophilia of >10% of the total WBC count, Peripheral neuropathy attributable to a systemic vasculitis, transient pulmonary infiltrates on chest radiographic imaging, paranasal sinus abnormality, blood vessel biopsy demonstrating extravascular eosinophils.2 Our case does not fully fulfil the criteria for EGPA; however, the atypical presentation of PMR like symptoms, raised inflammatory markers, high MPO antibodies titre, eosinophilia, pulmonary infiltrates and the resolution of symptoms and abnormal biochemical markers with steroids and omalizumab discontinuation, point to the diagnosis. Vasculitis induced syndrome of inappropriate antidiuresis (SIAD) is another aspect of this atypical presentation. Histological diagnosis in this case was not applicable and the rapid response to steroids did not prompt more invasive tests.
Differential diagnosis includes infections such as toxocariasis, strongyloides stercoralis, HIV and aspergillus species, drug-induced eosinophilia, hypereosinophilic syndromes (HES), and paraneoplastic eosinophilia. In our case, serology for Lyme disease, HIV, syphilis, and spinal fluid PCR were tested initially, but because the patient improved shortly after commencing steroids, there was no need to test for parasitic infections despite her recent travel history. Hyper eosinophilic syndrome is a disease of exclusion characterized by persistently raised eosinophilic count for at least 6 months with multisystem involvement, in our case, the eosinophilic count return to normal in less than 4 months.
Omalizumab has been implicated as a trigger for EGPA mainly during steroids withdrawal for asthmatic patients.3–9 However, as an exceptional option for patients with severe asthma and urticarial vasculitis, it can also be used in patients with EGPA in this context 0.10−12 Rechallenging with omalizumab can still be an option for patients with severe allergic asthma and raised IgE who do not respond to other treatment modalities.
Patient Informed Consent
Written informed consent was obtained from the patient described in this report to have the case details published. Institutional approval was not required to publish the case details.
Acknowledgments
The authors would like to thank Dr Azmi Mohammad, consultant endocrinologist for his constructive criticism of the manuscript. Sincere thanks to Mr David Watson, Assistant Librarian at South Tees NHS Foundation Trust for his diligent proofreading of this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1–11. doi:10.1002/art.37715
2. Masi AT, Hunder GG, Lie JT, et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990;33:1094–1100. doi:10.1002/art.1780330806
3. Nazir S, Tachamo N, Fareedy SB, Khan MS, Lohani S. Omalizumab-associated eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome). Ann Allergy Asthma Immunol. 2017;118:372–374. doi:10.1016/j.anai.2016.12.003
4. Bekçibaşı M, Baruttu S, Jelen MK, Dayan S, Hoşoglu S. Churg-Strauss syndrome occurring during omalizumab treatment. Eur J Rheumatol. 2015;2(3):129–130. doi:10.5152/eurjrheum.2015.0086
5. Szwarc D, Veillon F, Moser T, Averous G, De Blay F, Riehm S. Churg-Strauss syndrome under omalizumab treatment: a rare visceral manifestation [in French]. J Radiol. 2009;90:1737–1739. doi:10.1016/S0221-0363(09)73273-1
6. Wechsler ME, Wong DA, Miller MK, Lawrence-Miyasaki L. Churg-Strauss syndrome in patients treated with omalizumab. Chest. 2009;136:507–518. doi:10.1378/chest.08-2990
7. Winchester DE, Jacob A, Murphy T. Omalizumab for asthma. N Engl J Med. 2006;355(12):1281.
8. Ruppert AM, Averous G, Stanciu D, et al. Development of Churg-Strauss syndrome with controlled asthma during omalizumab treatment. J Allergy Clin Immunol. 2008;121(1):253. doi:10.1016/j.jaci.2007.10.040
9. Bargagli E, Rottoli P. Omalizumab treatment associated with Churg-Strauss vasculitis. Int Arch Allergy Immunol. 2008;145(3):268. doi:10.1159/000109296
10. Giavina-Bianchi P, Giavina-Bianchi M, Agondi R, Kalil J. Administration of anti-IgE to a Churg-Strauss syndrome patient. Int Arch Allergy Immunol. 2007;144(2):155–158. doi:10.1159/000103228
11. Varricchi G, Detoraki A, Liccardo B, Spadaro G, Marone G, Triggiani M. 275 efficacy of omalizumab in the treatment of urticaria-vasculitis associated to churg-strauss syndrome: a case report. World Allergy Organ J. 2012;5(Suppl 2):S106–7. doi:10.1097/01.WOX.0000412032.39383.49
12. Sozener ZC, Gorgulu B, Mungan D, et al. Omalizumab in the treatment of eosinophilic granulomatosis with polyangiitis (EGPA): single-center experience in 18 cases. World Allergy Organ J. 2018;11(1):39. doi:10.1186/s40413-018-0217-0
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.