")
Back to Journals » International Journal of General Medicine » Volume 15
Traditional Chinese Medicine in Treatment of COVID-19 and Viral Disease: Efficacies and Clinical Evidence
Authors Ding X, Fan LL, Zhang SX, Ma XX, Meng PF, Li LP, Huang MY, Guo JL, Zhong PZ, Xu LR
Received 16 August 2022
Accepted for publication 15 November 2022
Published 28 November 2022 Volume 2022:15 Pages 8353—8363
DOI https://doi.org/10.2147/IJGM.S386375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Xue Ding,1 Lei-Lei Fan,2 Shi-Xi Zhang,3 Xiu-Xia Ma,4 Peng-Fei Meng,4 Liang-Ping Li,5 Ming-Yan Huang,5 Jia-Le Guo,5 Peng-Zhan Zhong,5 Li-Ran Xu5
1Department of Medical, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China; 2Department of Cardiovascular, Yellow River Central Hospital, Zhengzhou, People’s Republic of China; 3Department of Infectious Disease, Shangqiu Municipal Hospital, Shangqiu, People’s Republic of China; 4Department of AIDS Clinical Research Center, Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China; 5Department of the First Clinical Medical College, Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China
Correspondence: Li-Ran Xu, Department of the First Clinical Medical College, The First Affiliated Hospital of Henan University of Chinese Medicine, 19 Renmin Road, Zhengzhou, People’s Republic of China, Email [email protected]
Abstract: Coronavirus disease 2019 (COVID-19) remains an uncontained, worldwide pandemic. While battling the disease in China, the Chinese government has actively promoted the use of traditional Chinese medicine, and many studies have been conducted to determine the efficacy of traditional Chinese medicine for treating COVID-19. The present review discusses the effectiveness and safety of traditional Chinese medicine in curing COVID-19 and provides clinical evidence from all confirmed cases in China. Applications of traditional Chinese medicine and specific recipes for treating other viral infections, such as those caused by severe acute respiratory syndrome coronavirus and influenza A viruses (including H1N1), are also discussed. Studies have reported that traditional Chinese medicine treatment plays a significant role in improving clinical symptoms. Therefore, further investigation may be of high translational value in revealing novel targeted therapies for COVID-19.
Keywords: traditional Chinese medicine, coronavirus disease-2019, influenza A viruses, acute respiratory syndrome coronavirus, clinical evidence
Introduction
Coronavirus disease 2019 (COVID-19), an acute respiratory infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first reported in December 2019.1 Since the beginning of the 21st century, three major emerging respiratory viral infections have spread across national borders and have been classified by the World Health Organization as travel advisories or public health emergencies of international concern: severe acute respiratory syndrome (SARS, 2002–2003), influenza virus H1N1 (2009–2010), and COVID-19.2 At present, there are no specific drugs to treat COVID-19.3
Over the past 3000 years in China, Traditional Chinese Medicine (TCM) has been used as the routine treatment regimen for pandemic and endemic diseases, and a complete theoretical system of prevention and treatment has been developed to manage these diseases. Huangdi Neijing, the first practitioner of TCM, wrote about pandemic and endemic diseases, calling them “pestilence” or “Wen Yi”, which refers to a fatal epidemic disease. TCM has a long history of treating infectious diseases and has good application and efficacy in treating viral infections, including SARS-CoV, MERS-CoV, hepatitis B, hepatitis C, influenza A, influenza B, Dengue, Ebola viruses and many more.4
While fighting COVID-19 in China, the National Health Commission of China announced that 92% of COVID-19 cases have been treated with TCM combined with Western medicine (WM), and that >90% of patients have responded to treatment and recovered or significantly improved.5 Three TCM decoctions and 3 formulated Chinese medicines (referred to as the “six most effective recipes” for the rest of the review) have been shown to be most effective in TCM treatments of COVID-19 patients in China.6 In these six highly effective TCM recipes, Jinhua Qinggan granule (JHQG), Lianhua Qingwen capsule (LHQW), Xuanfeibaidu granules (XFBD), Huashibaidu granules (HSBD), Xuebijing (XBJ) and Detoxifying Decoction (LCDD) have been shown to be most effective in treating patients with COVID-19. Mechanisms of the 6 most effective TCM recipes used in treating COVID-19 in 92% of all the confirmed cases in China. TCM can inhibit the replication and transcription of SARS-CoV-2, prevent the combination of SARS-CoV-2 and the host, and attenuate the cytokine storm and immune deficiency caused by the virus infecting the human body.3 TCM can help stabilize and prolong the treatment window for patients with severe cases. Increasing evidence suggests that early intervention with TCM in patients with COVID-19 is important for improving the cure rate, shortening the disease course, delaying disease progression, reducing mortality and safety.7,8 The past few decades have witnessed tremendous efforts in revealing the antiviral action mechanisms of TCM on the viral life cycle, such as viral entry, replication, assembly, and release, as well as virus-host-specific interactions. We describe the TCM therapeutic advantages in the treatment of COVID-19 and other viral disease based on clinical research evidence and the possible mechanism. Therefore, this review aims to provide a reference for the rational use of TCM in the clinical treatment of COVID-19 and other viral disease.
Efficacies and Clinical Evidence
Improvement of Clinical Signs and Symptoms
The main clinical manifestations of COVID-19, SARS, and H1N1 include fever and respiratory symptoms. SARS and COVID-19 have similar clinical manifestations.9 COVID-19 has the additional clinical symptoms of dry coughing and fatigue, and severe cases experience dyspnea approximately 1 week after disease onset.10 H1N1 symptoms include coughing, obvious upper respiratory symptoms, sore throat, catarrh, and gastrointestinal symptoms.11
Liu et al12 reported a single-center, open-label, randomized controlled trial. Here, 204 patients with laboratory-confirmed COVID-19 were randomized into the treatment group (Hua Shi Bai Du granules plus standard care (SC)) or control group (SC alone), with 102 patients per group. The treatment group recovered from fever faster and experienced a significantly greater attenuation of symptoms such as coughing, fatigue, and chest discomfort than did the control group. Shen et al13 studied 248 patients who met the moderate-type COVID-19 diagnostic criteria. Patients were divided into the SC group (n=158) and LHQW treatment group (n=90). After treatment, the LHQW group experienced a significantly higher recovery rate from symptoms (ie, fever, fatigue, and coughing) than did the control group (91.5% vs 82.4%). This suggests that LHQW exhibits safety and efficacy in improving clinical symptoms of COVID-19. A meta-analysis showed that compared with SC alone, Chinese herbal medicine plus SC had a superior effect on alleviating symptoms and reducing sign scores.14
Duan et al15 reported a randomized controlled trial in which 244 patients with confirmed influenza A (H1N1) viral infection were randomized to one of two treatment groups of 122 patients each. Each group received either LHQW or oseltamivir for 5 days and were observed for 7 days. LHQW significantly reduced the illness severity and duration of symptoms including fever, cough, sore throat, and fatigue. A meta-analysis showed that participants treated with LHQW had a shorter duration of fever, cough, sore throat, and body ache than did those treated with oseltamivir for influenza A viral infection.16
Xie et al17 reported a retrospective multicenter study involving 524 hospitalized patients with SARS. Compared with the WM treatment group, the fatigue time of patients in the integrated Chinese and western medicine e(CWM) treatment group was shortened by an average of 1.5 days, and tachypnea, shortness of breath, and muscle soreness were shortened by averages of 2, 1, and 2 days, respectively. These authors argued that CWM helps improve the clinical symptoms of patients with SARS. A study identified 12 randomized controlled trials and one quasi-randomized controlled trial involving 654 SARS patient. Clinical evidence shows that Chinese herbs combined with Western medicines may improve symptoms, quality of life, and lung infiltrate absorption and decrease the corticosteroid dosage for SARS patients.18
Prevention of Disease Progression
The proportion of severe cases (including critical cases) of SARS and COVID-19 is approximately 20%.19 The proportion of severe cases of H1N1 is 1.0%–4.6%.11 Severe patients with all three conditions are at a very high risk for worsening adverse outcomes such as acute respiratory distress or septic shock. Clinically, new therapeutic methods are urgently needed to replace or supplement current methods to reduce the incidence of severe disease.
Xiong et al20 reported a retrospective study that enrolled 116 patients with laboratory-confirmed COVID-19. The clinical cure rate of the CWM group was significantly higher than that of the WM group, and the incidence of the common-type to severe-type disease was lower in the CWM group than in the WM group, indicating that early application of TCM intervention therapy may block disease progression.21 A meta-analysis showed that CWM treatment showed superior overall clinical effectiveness for reducing the percentage of COVID-19 cases that became severe/critical.22
The First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine treated 37 SARS patients with early intervention of CWM and TCM, and no death or disease aggravation occurred. All patients were discharged within 10–15 days.23
Wang et al24 conducted a retrospective study of 326 cases of mild influenza A and showed that early intervention with TCM in severe treatment of H1N1 improved the symptoms of coughing, sputum coughing, shortness of breath, and bloody sputum and reduced the incidence of severe illness.
Reduced Mortality
COVID-19-related mortality in China is 0.4%,19 and as of 24 June 2022, global COVID-19-related mortality is 1.17%.25 SARS-related mortality is 11% globally and 6.6% in China.9 H1N1-related mortality has been reported at 0.4%11 and at 1.1%.26 Compared with the H1N1 pandemic, COVID-19 has shown higher rates of severe illness and death, especially among elderly patients.
Zhou et al27 reported an open-label, multicenter, randomized, controlled clinical trial that assigned 54 patients to the control group (SC alone) and 57 to the Shenhuang granule (SHG) plus SC group. The overall mortality was 75.9% (41/54) in the control group and 38.6% (22/57) in the SHG group. Post hoc analysis showed that in the severe category, the mortality rates of the control group vs the SHG group were 58.8% (10/17) vs 5.3% (1/19), and in the critical category, these rates were 83.8% (31/37) vs 55.3% (21/38). These authors concluded that SHGs are a promising integrative therapy for severe and critical COVID-19. A meta-analysis showed that a combination therapy of honeysuckle and SC therapy was more effective than SC therapy alone in clinical cure rates and in reducing rates of conversion to severe cases of COVID-19.7
Zhou et al28 reported a single-center, randomized, controlled clinical trial in which 2015 H1N1 patients were divided into the TCM group (n=379) and the CWM group (n=1636). In these cases, the severe disease conversion rate (0.05%) was lower than that in the US (0.24%), and the complication rate (1.09%) was lower than that in the US (1.44%), indicating that the treatment results were closely related to patients receiving TCM at the early disease stage.
Li et al29 divided 112 patients with SARS into two groups. In the CWM group (n=73), two patients died, whereas in the WM group (n=39), nine patients died, and the statistical difference was significant. These authors concluded that CWM significantly improved the prognosis and reduced the mortality of patients with SARS.
Shorter Hospital Stays
SARS and COVID-19 have a similar courses of illness, lasting approximately 2 weeks for mild cases and 4 weeks for severe and critical cases.9,10 The course of influenza A H1N1 is short; symptoms generally disappear within 2–7 days, but complications of the course may last a long time. Patients with COVID-19 with a longer hospitalization duration use more medical resources, resulting in higher medical costs. Therefore, shortening hospital stays will significantly reduce the costs associated with COVID-19.7
Shi et al30 conducted a retrospective study in which 782 patients with confirmed COVID-19 were divided into four groups according to treatment initiation time from the first date of symptom onset to the date they started treatment with QFPD. Receiving treatment within a week was correlated with a 14-day decrease in the median hospital stay length compared with those who started treatment later (P<0.0001). Early treatment with QFPD was associated with a shorter hospital stay length.
Zuo et al31 reported on 60 SARS patients who were admitted to the hospital and treated with CWM. All patients were cured and discharged. The patients’ average body temperatures returned to normal after 3.15 days; the average time for complete absorption of the lung shadow on radiographic imaging was 6.64 days, and the average hospital stay was 10 days, which is lower than the average hospital stay in mainland China.32
Tian et al33 reported a multicenter, randomized, controlled clinical trial in which 100 patients with H1N1 were randomly divided into two groups of 50 patients each. The treatment group was treated with CWM; the control group received oseltamivir phosphate capsules, and the patients were observed for 7 days. The CWM group exhibited adjusted immune states, improved antiviral abilities, enhanced tissue stability, and a shorter disease course. Li et al34 conducted a randomized controlled trial of H1N1 and confirmed that on the basis of antiviral therapy plus TCM treatment, the CWM group experienced a significantly shorter hospitalization time than did the WM group.
Enhanced Quality of Life
Quality of life (QOL) is a person’s perception of their life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. In the context of increasing medical attention to overall patient health, more attention is being paid to patients achieving physical, psychological, and social integrity. Improving patients’ QOL is as important as treatment.
A systematic review showed that different CAM interventions significantly improved various psychological symptoms (depression, anxiety, stress, sleep quality, negative emotions, and QOL) and physical symptoms (inflammatory factors, physical activity, chest pain, and respiratory function) in patients with COVID-19.35
Yao et al36 randomly divided 75 patients with H1N1 into the CWM and WM groups. The CWM group exhibited improved clinical symptoms and an improved QOL (P<0.01).
Jiang et al37 reported a multicenter, prospective, open, randomized control trial of 85 patients to evaluate the convalescent efficacy of TCM in treating patients with SARS. The TCM group exhibited better QOL scores than did the WM group, mainly in total score and psychological and emotional factors, thus indicating a significantly improved QOL of these patients.
Enhanced Immunity
Cellular immunity plays a critical role in the human immune system. CD4+ T-cell counts are frequently used in TCM clinical trials. Studies have shown that lymphocyte counts decrease continuously in nonviable patients, and decreases in CD4+, CD8+, and natural killer cells are related to COVID-19 severity. Lymphocyte counts and the absolute values of CD3+, CD4+, and CD8+ cells are decreased in the peripheral blood of SARS patients. One study found that patients with severe SARS had significantly fewer CD4+ cells than did healthy participants.38 H1N1 has a complex pathogenesis, and immune function instability plays a key role in its occurrence and development. The immune systems of these patients must be improved to control the disease and improve patient outcomes.39 TCM improves patients’ immunity, prevents disease progression, and promotes recovery.
Zhang et al40 reported a retrospective cohort study of patients with laboratory-confirmed mild and moderate COVID-19. The treatment group received Tanreqing capsules orally in addition to conventional WM treatments, which were also administered to the control group. The results showed increased CD3+ T-cell levels in the treatment group compared with those of the control group. The underlying mechanism of Tanreqing capsules may be related to improved levels of the immune indicator CD3+ T cells.
Wang et al41 divided 155 patients with H1N1 into the CWM (n=78) and CM (n=77) groups. After WM treatment, serum IFN-γ and IL-4 levels and the IFN-γ/IL-4 ratio were significantly improved in both groups (P<0.05), with a better degree of improvement in the CWM group than in the CM group (P<0.01). After treatment, the CD4+, CD8+, IgA, and IgM levels were improved in both groups compared with those before treatment (P<0.01), with a more significant improvement in the CWM group than in the WM group (P<0.01). The authors believe that combining TCM and WM treatments for H1N1 can effectively regulate the immune state of patients and improve the clinical efficacy.
Li et al38 randomly divided 51 SARS patients into the CWM (n=29) and WM (n=22) groups. The CWM group exhibited significantly increased numbers of CD4+ T cells, and the immune function was restored.
Promotion of Negative Conversion
The three diseases described herein are all caused by RNA viruses, which can be detected by RT-PCR. Accelerating the virus’s negative conversion will shorten hospital stays and reduce medical costs.
Ni et al42 conducted a multicenter, randomized, open-label, parallel-controlled, trial using Shuanghuanglian to treat patients with COVID-19. Here, 176 patients received Shuanghuanglian in addition to SC, while 59 control patients received standard therapy alone. Patients receiving Shuanghuanglian treatment for 14 days had significantly higher negative conversion rates of SARS-CoV-2 on nucleic acid swab tests than did the control patients.
Wang et al43 conducted a retrospective study of the duration of H1N1 viral shedding in patients who were hospitalized and treated in China. Clinical data were collected from 963 patients with H1N1 infection. In patients with body temperatures ≥38.1°C, TCM therapy reduced the viral shedding duration (P<0.05 vs oseltamivir therapy).
Ease of Rehabilitation
The three diseases discussed herein manifest different degrees of grid-like shadow densities on chest high-resolution computed tomography (CT) during recovery. Fibrotic changes will decrease patients’ lung function as well as their corresponding work ability and exercise tolerance, thus severely affecting their QOL, with a stronger impact on severe and critically ill patients.44–46 Improving lung function and attenuating pulmonary fibrosis are crucial to rehabilitating these patients. TCM treatment is recommended in the rehabilitation period of COVID-19.
One study randomly divided 131 patients in the rehabilitation period of COVID-19 into the Bufei Huoxue (BFHX; n = 66) or placebo (n = 65) group. After 3 months of treatment, the BFHX group exhibited greater attenuation of pneumonia lesions on chest CT than did the placebo group (P<0.05). The BFHX group exhibited a significantly improved 6-min walk distance relative to baseline compared with that of the placebo group (P<0.01). Thus, BFHX may exert strong rehabilitative effects on physiological activity in patients recovering from COVID-19.
Ma et al46 conducted follow-up visits of 12 patients with H1N1, in which ten patients were treated with CWM. Nine patients were tested for lung function during follow-up, and 67% had varying degrees of lung function abnormalities, mainly with mildly restrictive ventilatory dysfunction. All patients, including three critically ill patients, underwent a 6-minute walking test at follow-up in which one patient scored grade I, one patient scored grade III, and the remaining patients scored grade IV. Active TCM intervention should improve patients’ long-term prognosis.
Chen et al45 conducted follow-up visits of 85 patients with SARS during the convalescent period and randomly divided them into the TCM and control groups. All patients underwent pulmonary function tests. The TCM group presented significantly higher changes in restrictive ventilatory disorder and diffusion dysfunction than did the control group (P<0.05). These authors suggest that the TLC% and DLCO% of the lung function impairment in these patients improved significantly with prolonged discharge time, and TCM treatment enhanced these improvements.
Infection Prevention
Most people are generally susceptible to the three diseases discussed herein. However, SARS and COVID-19 affect primarily younger and older patients, respectively, and COVID-19 affects patients more severely, with a higher death rate than that of H1N1. Active prevention is an important means of treatment.
Yan et al47 recruited 22,065 participants from 11 communities during a 1-month period. Participants were randomly assigned to receive either a 5-day herbal medicine therapy plus a reference manual or a reference manual only (control group). Use of herbal medicine reduced the risk of the common cold by 89.6% in all community-dwelling residents and by 94.0% in residents aged 16–59 years. These authors suggested that herbal medicine may be a useful public health intervention method to minimize preventable morbidity during COVID-19 outbreaks.
Liu et al48 reported a 14-day multicenter, non-blinded, control trial during the SARS outbreak, in which medical workers in Hong Kong were randomly divided into the Qingfei Paidu (QFPD) decoction group (2601 patients) and the control group (15,374 patients). No patients in the QFPD group became infected with SARS, whereas 64 (0.4%) in the control group became infected with SARS. Cold-like symptoms and QOL were significantly improved in the QFPD group. Thirty-seven patients in the QFPD group underwent serum immunology examinations, which showed that TCM improved the body’s immune functions. These authors suggested that TCM may improve QOL and prevent SARS by alleviating clinical symptoms and enhancing immune functions. Liu et al49 randomly divided 53 medical workers into the prevention group (n=28) who took TCM preventive prescriptions and the control group (n=25) who took no medication. After 10 days of observation and treatment, the TCM group had only two confirmed cases of influenza A (7.14%), which was significantly lower than that of the control group (eight cases, 32%). The authors concluded that taking TCM significantly reduced the incidence of H1N1.
Underlying Mechanisms
Mounting evidence supports the therapeutic efficacy of TCM in alleviating the clinical symptoms of COVID-19 and other viral disease, the underlying mechanisms of TCM mainly involve antiviral, anti-inflammatory, and immunomodulatory actions and organ protection (Table 1).
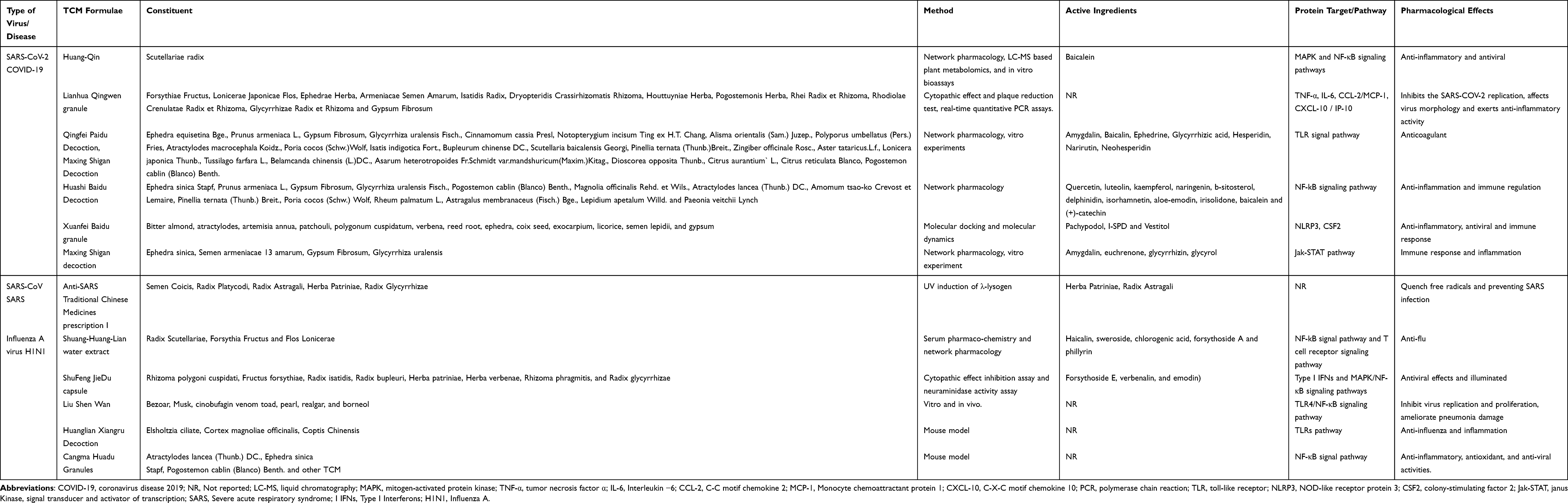 |
Table 1 Mechanism of TCM Treatment of COVID-19 and Other Viral Disease |
Glycyrrhizin, licorice and Ephedra62,63 can disrupting viral uptake into the host cells and disrupting the interaction between receptor- binding domain (RBD) of SARS-COV2 and ACE2. Qingwenjiere Mixture64 can inhibited the expression of RdRp/Hel and s genes of SARS-CoV-2 and reduced virus-induced mRNA expression of a panel of pro-inflammatory cytokines. Honeysuckle and Huangqi65 can inhibited SARS-CoV-2 Mpro activity alleviating viral entry as well as replication. MXSG66 might directly inhibit the adsorption and replication of SARS-CoV-2 at the viral entry step. Anemarrhenae Rhizoma67 can inhibit the activity of the main protease of SARS-CoV-2 and inhibit replication and transcription. After the virus infects the human body, immune abnormalities, cytokine storm, lung and cardiovascular injury would affect each other. Keguan-168 can reduce inflammation and pulmonary vascular endothelial injury. HSBDF and MXSG66,69 can regulate inflammatory cytokines production and relieve lung injury through toll-like receptors signaling pathway. Rhei Radix et Rhizome-Schisandrae Sphenantherae Fructus70 can regulate immune function, cardiovascular protection, anti-inflammation. LHQW71 can modulates the inflammatory process, repairs lung injury, relieve the cytokine storm, improves ACE2-expression-disorder-caused symptoms. Moreover, Fufang Yinhua Jiedu granules72 can suppressing the expression of inflammatory cytokines via regulating the TLR7/MyD88/NF-κB signaling pathway to affect the normal biological function of influenza virus. Ge Gen Decoction73 can modulate immune system and relieve lung inflammation of H1N1 via regulating the toll-like receptor 7 signaling pathway. Yinhuapinggan granule1 is used in TCM to treat influenza, cough, and viral pneumonia. Yinhuapinggan granule had antiviral effects, which might be associated with regulation of the inflammatory cytokines production, evaluation of the levels of IFN-stimulated genes, and modulation of the protein expressions of key effectors in the Type I IFN and PRRs signaling pathway.
Conclusion
TCM has a well-documented history of treating infectious diseases in China. The gradual development of TCM in the treatment of infectious diseases is based on the constant accumulation and summarization of experience in clinical practice. TCM has been shown to be highly effective in treating patients with infectious diseases such as SARS, H1N1, and COVID-19. Much evidence-based clinical studies have confirmed the efficacy and safety of TCM methods in managing infectious disease alone or in combination with WM. In China, the Chinese medicines and Chinese recipes were used to treat viral infections, significantly alleviating disease symptoms, delaying mild disease progression to a severe stage, improving cure rates, decreasing mortality rates, enhancing immune functions and quality of life. The role of TCM is related to affecting the transcription, replication, and binding of viral to the host. TCM74 can inhibit the enzyme activity of SARS-CoV-2 3CLpro, which is vital for the replication and activity of virus, and thus may be a promising therapeutic target for SARS-CoV-2.75 TCM76–78 can reduce the binding of SARS-CoV2 to ACE2 and reduce the attachment of the virus to the host cell. In-depth exploration of the active components of TCM on SARS-CoV-2 3CLpro and ACE2 may be helpful to screen anti-COVID-19 drugs. Influenza is caused by influenza virus and the neuraminidase encoded by virus has vital role in the life cycle of the virus for its recognition, entry and release from the cells they infect. TCM79 exerted strong inhibitory activities towards neuraminidase and exhibited antiviral effect against influenza A virus by reducing viral reproduction and reduced cytopathic effect of the viral infected cells.
In conclusion, this study summarized the comprehensive and updated evidence of Chinese medicine for infectious diseases treatment. However, there are some limitations, such as difficult to maintain the stability of the various formulations and lack of perfect evaluation index system and evaluation methodology. It is expected to further high-level evidence is needed to support TCM for treating infectious diseases to help better manage the devastating effects of COVID-19 and other diseases and provide a complete chain of evidence for the prevention, treatment, and recovery using TCM.
Funding
This work was supported by Nation Natural Science Foundation of China (U1904153), Special subject of scientific research on Traditional Chinese Medicine in Henan Province (2019AZB006, 2019JDZX2096) and Special subject of scientific research of Traditional Chinese Medicine on COVID-19 in Henan Province (2022ZYFY02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Du HX, Zhou HF, Wan HF, et al. Antiviral effects and mechanisms of Yinhuapinggan granule against H1N1 influenza virus infection in RAW264.7 Cells. Inflammopharmacology. 2018;26:1455–1467. doi:10.1007/s10787-018-0457-1
2. World Healthe Organization. WHO Director-General as Guest Lecture at Robert S. McNamara Lecture on War and Peace, Harvard Kennedy School - 25 February 2022. World Healthe Organization; 2022.
3. Huang Y, Yang C, Xu XF, Xu W, Liu SW. Structural and functional properties of SARS-CoV-2 spike protein: potential antivirus drug development for COVID-19. Acta Pharmacol Sin. 2020;41:1141–1149. doi:10.1038/s41401-020-0485-4
4. Huang K, Zhang P, Zhang Z, et al. Traditional Chinese Medicine (TCM) in the treatment of COVID-19 and other viral infections: efficacies and mechanisms. Pharmacol Ther. 2021;225:107843. doi:10.1016/j.pharmthera.2021.107843
5. China NHCotPsRo. Transcript of Press Conference on March 17, 2020; Vol. 2022, 2022.
6. Luo H, Gao Y, Zou J, et al. Reflections on treatment of COVID-19 with traditional Chinese medicine. Chin Med. 2020;15(1):94. doi:10.1186/s13020-020-00375-1
7. Du XQ, Shi LP, Cao WF, Chen ZW, Zuo B, Hu JY. Add-on effect of honeysuckle in the treatment of coronavirus disease 2019: a systematic review and meta-analysis. Front Pharmacol. 2021;12:708636. doi:10.3389/fphar.2021.708636
8. Xing D, Liu Z. Effectiveness and safety of traditional Chinese medicine in treating COVID-19: clinical evidence from China. Aging Dis. 2021;12(8):1850–1856. doi:10.14336/AD.2021.0906
9. Nan-shan Z. Diagnosis and treatment of SARS. Natl Med J China. 2003;2003;95–116.
10. Medicine NHCNAoTC. COVID-19 diagnosis and treatment protocol (trial version 9). China Med. 2022;17:481–487.
11. Yuan-sheng C, Qi-ru S, Iao TW-X, et al. Epidemiological analysis on the global pandemic (H1N1)2009. Med Philos. 2009;30:9–11+61.
12. Liu J, Yang W, Liu Y, et al. Combination of Hua Shi Bai Du granule (Q-14) and standard care in the treatment of patients with coronavirus disease 2019 (COVID-19): a single-center, open-label, randomized controlled trial. Phytomedicine. 2021;91:153671. doi:10.1016/j.phymed.2021.153671
13. Shen P, Li J, Tu S, et al. Positive effects of Lianhuaqingwen granules in COVID-19 patients: a retrospective study of 248 cases. J Ethnopharmacol. 2021;278:114220. doi:10.1016/j.jep.2021.114220
14. Fan AY, Gu S, Alemi SF. Chinese herbal medicine for COVID-19: current evidence with systematic review and meta-analysis. J Integr Med. 2020;18(5):385–394. doi:10.1016/j.joim.2020.07.008
15. Duan ZP, Jia ZH, Zhang J, et al. Natural herbal medicine Lianhuaqingwen capsule anti-influenza A (H1N1) trial: a randomized, double blind, positive controlled clinical trial. Chin Med J. 2011;124:2925–2933.
16. Zhao P, Yang HZ, Lv HY, Wei ZM. Efficacy of Lianhuaqingwen capsule compared with oseltamivir for influenza A virus infection: a meta-analysis of randomized, controlled trials. Altern Ther Health Med. 2014;20:25–30.
17. YM, X, JQ, H, WL, W, RB, W, YP, Z, XH, L Effects of integrated traditional Chinese and western medicine on clinical symptoms of 318 patients with SARS. JTCM. 2004;671–674+644.
18. Liu X, Zhang M, He L, Li Y. Chinese herbs combined with western medicine for severe acute respiratory syndrome (SARS). Cochrane Database Syst Rev. 2012;10:Cd004882. doi:10.1002/14651858.CD004882.pub3
19. COVID-19 Emergency Response Mechanism Epidemiology Group C. Analysis of epidemiological characteristics of COVID-19. Chin J Epidemiol. 2020;41:145–151. doi:10.3760/cma.j.issn.0254-6450.2020.02.003
20. Xiong S, Liu L, Lin F, et al. Clinical characteristics of 116 hospitalized patients with COVID-19 in Wuhan, China: a single-centered, retrospective, observational study. BMC Infect Dis. 2020;20(1):787. doi:10.1186/s12879-020-05452-2
21. WG, X, CQ, A, CJ, Z, JX, Z, M, H, Y, W Clinical study of integrated Chinese and Western medicine in the treatment of 1934 cases of COVID-19. JTCM. 2020;61:375–382.
22. Luo X, Ni X, Lin J, et al. The add-on effect of Chinese herbal medicine on COVID-19: a systematic review and meta-analysis. Phytomedicine. 2021;85:153282. doi:10.1016/j.phymed.2020.153282
23. ZY, S Combination of traditional Chinese and western medicine to overcome SARS. Chin J Integr Med. 2003;2003:566–567.
24. Clinical characteristics of 326 cases with mild influenza A (H1N1). Global Tradit Chin Med. 2011;4:31–34.
25. World Health Oraganization. Coronavirus Disease (COVID-19) Pandemic. Vol. 2022. World Health Oraganization; 2022.
26. LH, L, ZM, Z, JF, H, HJ, Z, WQ, L, F, Y Epidemiological analysis of severe and fatal cases of influenza A (H1N1) in Guangdong Province. J South China Prev Med. 2010;36:17–20.
27. Zhou S, Feng J, Xie Q, et al. Traditional Chinese medicine shenhuang granule in patients with severe/critical COVID-19: a randomized controlled multicenter trial. Phytomedicine. 2021;89:153612. doi:10.1016/j.phymed.2021.153612
28. H, Z, HQ, H, ZD, Z, LT, T Clinical observation of 2015 cases of influenza A H1N1 treated by TCM syndrome differentiation. J New Chin Med. 2011;43:24–26.
29. Xiuhui L, Ke Z, Jian H, Yu Y, Lianchun L. Clinical effect of integrated Traditional Chinese and western medicine on severe acute respiratory syndrome (SARS). J Chin Med. 2003;2003:326–328+383.
30. Shi N, Liu B, Liang N, et al. Association between early treatment with Qingfei Paidu decoction and favorable clinical outcomes in patients with COVID-19: a retrospective multicenter cohort study. Pharmacol Res. 2020;161:105290. doi:10.1016/j.phrs.2020.105290
31. JL, Z, M, Z, ZZ, Y Clinical experience of treating 60 SARS patients with Yinqiao Qing Decoction. J Henan Tradit Chin Med. 2005;2005:41–42.
32. Feng D, Jia N, Fang LQ, et al. Duration of symptom onset to hospital admission and admission to discharge or death in SARS in mainland China: a descriptive study. Trop Med Int Health. 2009;14(Suppl 1):28–35. doi:10.1111/j.1365-3156.2008.02188.x
33. YZ, T, DY, D, HS, W, YS, A, JD, C et al Treatment of 50 cases of influenza A H1N1 virus pneumonia by ergen Qingfei Decoction combined with Tanreqing injection. J Chin Med Res. 2019;32:12–16.
34. Treatment of 43 cases of influenza A H1N1 with Yinqiao powder. J Henan Tradit Chin Med. 2014;34:1938–1940.
35. Badakhsh M, Dastras M, Sarchahi Z, Doostkami M, Mir A, Bouya S. Complementary and alternative medicine therapies and COVID-19: a systematic review. Rev Environ Health. 2021;36(3):443–450. doi:10.1515/reveh-2021-0012
36. JH, Y Clinical study on early intervention of Chaima Qingwen decoction and western medicine on influenza A (H1N1). Chin Arch Tradit Chin Med. 2012;30:2742–2744.
37. Evaluation of convalescent efficacy evaluation of convalescent efficacy of traditional Chinese medicine in treating patients with SARS in treating patients with SARS. J Tradit Chin Med. 2003;2003:666–668.
38. Xiuhui L, Jianhua H, Ke Z, et al. Clinical observation of 51 cases of severe SARS treated by integrated traditional Chinese and western medicine. Chin J Integr Tradit West Med Intensive Care Med. 2003:2003;259–261.
39. Bing Y, Runfeng L, Chunguang Y, et al. Pharmacokinetic and pharmacodynamic application of oseltamivir in tree shrews. Chin J Comp Med. 2019;29:7–13.
40. Zhang X, Xue Y, Chen X, et al. Effects of Tanreqing capsule on the negative conversion time of nucleic acid in patients with COVID-19: a retrospective cohort study. J Integr Med. 2021;19:36–41. doi:10.1016/j.joim.2020.10.002
41. Zhenhua W, Xiaoli Y. Effect of Lianhua Qingwen capsule combined with Oseltamivir on immune level of patients with influenza A. J Med Theory Pract. 2021;34:2058–2060.
42. Ni L, Wen Z, Hu X, et al. Effects of Shuanghuanglian oral liquids on patients with COVID-19: a randomized, open-label, parallel-controlled, multicenter clinical trial. Front Med. 2021;15:704–717. doi:10.1007/s11684-021-0853-6
43. Wang YG, Jiang M, Wang RB, et al. Duration of viral shedding of influenza A (H1N1) virus infection treated with oseltamivir and/or traditional Chinese medicine in China: a retrospective analysis. J Tradit Chin Med. 2012;32:148–155. doi:10.1016/S0254-6272(13)60004-7
44. Ojha V, Mani A, Pandey NN, Sharma S, Kumar S. CT in coronavirus disease 2019 (COVID-19): a systematic review of chest CT findings in 4410 adult patients. Eur Radiol. 2020;30(11):6129–6138. doi:10.1007/s00330-020-06975-7
45. C, X, L, JT, Y, HX, L, Y, Z, XM, S, Nan et al Effect of Chinese medicine treatment on lung function and quality of life of SARS convalescent patients. Chin J Rehabil Med. 2006;2006:124–126.
46. Yanfang M, Chengjie M, Xin L, et al. Long-term follow-up study of 12 patients with influenza A (H1N1) (2009). Acta Chin Med. 2016;31:957–961.
47. Yan B, Jiang Z, Yuan J, et al. Effects and safety of herbal medicines among community-dwelling residents during COVID-19 pandemic: a large prospective, randomized controlled trial (RCT). Phytomedicine. 2021;85:153403. doi:10.1016/j.phymed.2020.153403
48. Dehui L, Bingzhong L, Liyi H, et al. Clinical Observation on Prevention of SARS by Kangdu Bufei Decoction. Chin J Integr Med. 2004;2004:685–688.
49. Lin L, Guoli X, Xiangdong X, et al. Preliminary observation on the prevention of influenza A by “a flu prevention method”. J Beijing Tradit Chin Med. 2013;32:91–92.
50. Liu J, Meng J, Li R, et al. Integrated network pharmacology analysis, molecular docking, LC-MS analysis and bioassays revealed the potential active ingredients and underlying mechanism of Scutellariae radix for COVID-19. Front Plant Sci. 2022;13:988655. doi:10.3389/fpls.2022.988655
51. Runfeng L, Yunlong H, Jicheng H, et al. Lianhuaqingwen exerts anti-viral and anti-inflammatory activity against novel coronavirus (SARS-CoV-2). Pharmacol Res. 2020;156:104761. doi:10.1016/j.phrs.2020.104761
52. Yang R, Liu H, Bai C, et al. Chemical composition and pharmacological mechanism of Qingfei Paidu decoction and Ma Xing Shi Gan decoction against coronavirus disease 2019 (COVID-19): in silico and experimental study. Pharmacol Res. 2020;157:104820. doi:10.1016/j.phrs.2020.104820
53. Zhu YW, Yan XF, Ye TJ, et al. Analyzing the potential therapeutic mechanism of Huashi Baidu decoction on severe COVID-19 through integrating network pharmacological methods. J Tradit Complement Med. 2021;11:180–187. doi:10.1016/j.jtcme.2021.01.004
54. Xiong L, Cao J, Yang X, et al. Exploring the mechanism of action of Xuanfei Baidu granule (XFBD) in the treatment of COVID-19 based on molecular docking and molecular dynamics. Front Cell Infect Microbiol. 2022;12:965273. doi:10.3389/fcimb.2022.965273
55. Li Y, Chu F, Li P, et al. Potential effect of Maxing Shigan decoction against coronavirus disease 2019 (COVID-19) revealed by network pharmacology and experimental verification. J Ethnopharmacol. 2021;271:113854. doi:10.1016/j.jep.2021.113854
56. Li Y, Li J, Fang C. Inhibitory effects of anti-SARS traditional Chinese medicines on the UV irradiation of lambda-lysogen. Am J Chin Med. 2006;34:147–155. doi:10.1142/S0192415X06003710
57. Zhang FX, Li ZT, Yang X, et al. Discovery of anti-flu substances and mechanism of Shuang-Huang-Lian water extract based on serum pharmaco-chemistry and network pharmacology. J Ethnopharmacol. 2021;268:113660. doi:10.1016/j.jep.2020.113660
58. Tao Z, Chen J, Su J, et al. Quantitative proteomics analysis of systemic responses and biological mechanisms of ShuFengJieDu capsule using H1N1-infected RAW264.7 Cells. ACS Omega. 2020;5:15417–15423. doi:10.1021/acsomega.0c01545
59. Ma Q, Huang W, Zhao J, Yang Z. Liu Shen Wan inhibits influenza a virus and excessive virus-induced inflammatory response via suppression of TLR4/NF-κB signaling pathway in vitro and in vivo. J Ethnopharmacol. 2020;252:112584. doi:10.1016/j.jep.2020.112584
60. Wu QF, Zhu WR, Yan YL, Zhang XX, Jiang YQ, Zhang FL. Anti-H1N1 influenza effects and its possible mechanism of Huanglian Xiangru decoction. J Ethnopharmacol. 2016;185:282–288. doi:10.1016/j.jep.2016.02.042
61. Cui XR, Guo YH, Liu QQ. Cangma Huadu granules, a new drug with great potential to treat coronavirus and influenza infections, exert its efficacy through anti-inflammatory and immune regulation. J Ethnopharmacol. 2022;287:114965. doi:10.1016/j.jep.2021.114965
62. Gomaa AA, Abdel-Wadood YA. The potential of glycyrrhizin and licorice extract in combating COVID-19 and associated conditions. Phytomed Plus. 2021;1:100043. doi:10.1016/j.phyplu.2021.100043
63. Mei J, Zhou Y, Yang X, Zhang F, Liu X, Yu B. Active components in Ephedra sinica stapf disrupt the interaction between ACE2 and SARS-CoV-2 RBD: potent COVID-19 therapeutic agents. J Ethnopharmacol. 2021;278:114303. doi:10.1016/j.jep.2021.114303
64. Xie P, Fang Y, Shen Z, et al. Broad antiviral and anti-inflammatory activity of Qingwenjiere mixture against SARS-CoV-2 and other human coronavirus infections. Phytomedicine. 2021;93:153808. doi:10.1016/j.phymed.2021.153808
65. Yeh YC, Doan LH, Huang ZY, et al. Honeysuckle (Lonicera japonica) and Huangqi (Astragalus membranaceus) suppress SARS-CoV-2 entry and COVID-19 related cytokine storm in vitro. Front Pharmacol. 2022;12:765553. doi:10.3389/fphar.2021.765553
66. Li Q, Bai C, Yang R, et al. Deciphering the pharmacological mechanisms of Ma Xing Shi Gan decoction against COVID-19 through integrating network pharmacology and experimental exploration. Front Pharmacol. 2020;11:581691. doi:10.3389/fphar.2020.581691
67. Qi X, Li B, Omarini AB, Gand M, Zhang X, Wang J. Discovery of TCMs and derivatives against the main protease of SARS-CoV-2 via high throughput screening, ADMET analysis, and inhibition assay in vitro. J Mol Struct. 2022;1268:133709. doi:10.1016/j.molstruc.2022.133709
68. Bai Z, Li P, Wen J, et al. Inhibitory effects and mechanisms of the anti-covid-19 traditional Chinese prescription, Keguan-1, on acute lung injury. J Ethnopharmacol. 2022;285:114838. doi:10.1016/j.jep.2021.114838
69. Wei WL, Wu SF, Li HJ, et al. Chemical profiling of Huashi Baidu prescription, an effective anti-COVID-19 TCM formula, by UPLC-Q-TOF/MS. Chin J Nat Med. 2021;19:473–480. doi:10.1016/S1875-5364(21)60046-8
70. Qi JH, Dong FX, Wang K, et al. Feasibility analysis and mechanism exploration of Rhei Radix et Rhizome-Schisandrae Sphenantherae Fructus (RS) against COVID-19. J Med Microbiol. 2022;2022:71.
71. Zheng S, Baak JP, Li S, et al. Network pharmacology analysis of the therapeutic mechanisms of the traditional Chinese herbal formula Lian Hua Qing Wen in Corona virus disease 2019 (COVID-19), gives fundamental support to the clinical use of LHQW. Phytomedicine. 2020;79:153336. doi:10.1016/j.phymed.2020.153336
72. Zhang Y, Wang R, Shi W, et al. Antiviral effect of fufang yinhua jiedu (FFYH) granules against influenza A virus through regulating the inflammatory responses by TLR7/MyD88 signaling pathway. J Ethnopharmacol. 2021;275:114063. doi:10.1016/j.jep.2021.114063
73. Geng ZK, Li YQ, Cui QH, Du RK, Tian JZ. Exploration of the mechanisms of Ge Gen decoction against influenza A virus infection. Chin J Nat Med. 2019;17:650–662. doi:10.1016/S1875-5364(19)30079-2
74. Su HX, Yao S, Zhao WF, et al. Anti-SARS-CoV-2 activities in vitro of Shuanghuanglian preparations and bioactive ingredients. Acta Pharmacol Sin. 2020;41:1167–1177. doi:10.1038/s41401-020-0483-6
75. Agrahari R, Mohanty S, Vishwakarma K, Nayak SK, Samantaray D, Mohapatra S. Update vision on COVID-19: structure, immune pathogenesis, treatment and safety assessment. Sens Int. 2021;2:100073. doi:10.1016/j.sintl.2020.100073
76. Das K, Pingali MS, Paital B, et al. A detailed review of the outbreak of COVID-19. Front Biosci. 2021;26:149–170.
77. Tao P, Jiming L. Molecular mechanisms revealed by network pharmacology of Xuebijing on the treatment of acute respiratory distress syndrome caused by novel coronavirus infection. Eur Rev Med Pharmacol Sci. 2022;26:2651–2661. doi:10.26355/eurrev_202204_28594
78. Xing Y, Hua YR, Shang J, Ge WH, Liao J. Traditional Chinese medicine network pharmacology study on exploring the mechanism of Xuebijing injection in the treatment of coronavirus disease 2019. Chin J Nat Med. 2020;18:941–951. doi:10.1016/S1875-5364(20)60038-3
79. Tian L, Wang Z, Wu H, et al. Evaluation of the anti-neuraminidase activity of the traditional Chinese medicines and determination of the anti-influenza A virus effects of the neuraminidase inhibitory TCMs in vitro and in vivo. J Ethnopharmacol. 2011;137:534–542. doi:10.1016/j.jep.2011.06.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.