")
Back to Journals » Infection and Drug Resistance » Volume 16
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Authors Wu C, Lu J, Ruan L, Yao J
Received 24 August 2022
Accepted for publication 4 February 2023
Published 15 March 2023 Volume 2023:16 Pages 1499—1509
DOI https://doi.org/10.2147/IDR.S386311
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Cuiyun Wu,1 Jiehong Lu,1 Lijin Ruan,2 Jie Yao1
1Department of Clinical Laboratory, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde), Foshan, Guangdong, People’s Republic of China; 2Department of Radiology, Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, People’s Republic of China
Correspondence: Jie Yao, Department of Clinical Laboratory, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde) Foshan, Guangdong, People’s Republic of China, No. 1, Jiazi Road, Lunjiao, Shunde District, Foshan City, Guangdong Province, 528308, People’s Republic of China, Tel +86 0757 22318169, Email [email protected]
Objectives: Multi-drug resistance (MDR) emerged as a serious threat in intensive care unit (ICU) settings. Our study aimed to investigate the major pathogens in ICU and identify the risk factors for MDR infection.
Methods: We performed a retrospective analysis of patients admitted to the ICU. Multivariate logistic regression was applied to identify the independent predictors, and then a nomogram to predict the probability of MDR infection.
Results: A total of 278 patients with 483 positive cultures were included. 249 (51.55%) had at least one MDR pathogen, including extensively drug-resistant (XDR) 77 (30.92%) and pan drug-resistant (PDR) 39 (15.66%), respectively. Klebsiella pneumonia was the most frequently isolated pathogen. We identified the number of bacteria (OR 2.91, 95% CI 1.97– 4.29, P < 0.001), multiple invasive procedures (OR 2.23, 95% CI 1.37– 3.63, P = 0.001), length of stay (LOS) (OR 1.01, 95% CI 1.00– 1.02, P = 0.007), Hemoglobin (Hb) (OR 0.99, 95% CI 0.98– 1.00, P = 0.01) were independent risk factors for MDR infection. Our nomogram displayed good discrimination with curve AUC was 0.75 (95% CI: 0.70– 0.81). The decision curves also indicate the clinical utility of our nomogram. Additionally, the in-hospital mortality with MDR pathogens was independently associated with XDR (HR, 2.60; 95% CI: 1.08– 6.25; P = 0.03) and total protein (TP) (HR, 0.95; 95% CI: 0.91– 0.99; P = 0.03).
Conclusion: The number of bacteria, multiple invasive procedures, LOS, and Hb were the independent predictors associated with MDR pathogens. Our nomogram is potentially useful for predicting the occurrence of MDR infection. Besides, we also identify XDR and TP as the independent risk factors for in-hospital mortality with MDR infection. The current prevalence of MDR strains was also described. The results will contribute to the identification and preventive management of patients at increased risk of infection.
Keywords: multi-drug resistance, intensive care unit, risk factors, nomogram
Introduction
Nosocomial infections are a leading global health issue encountered today.1 This global health problem has been exacerbated in recent years due to the increase in multidrug-resistant (MDR) pathogens, with more than 2.8 million antibiotic-resistant infections estimated to occur annually in the United States, resulting in 35,000 deaths.2 WHO and many other organizations and researchers agree that the spread of MDR is an urgent problem that requires a coordinated global action plan to address.3–5
Due to the high frequency, high dose and long duration of antibiotic use in ICU patients, compared with patients in other departments, the probability of infection with MDR bacteria is increased.6 According to the data of the Chinese Antimicrobial Resistance Surveillance System (CARSS) and Chinese Antimicrobial Surveillance Network (CHINET), carbapenem-resistant Klebsiella pneumoniae (CRKP) increased from 3.0% in 2005 to 20.9% in 2017.7 Similarly, an increasing trend in MDR has been seen in most bacteria studied in some European intensive care units (ICUs).8 For instance, a study from Luna reported that in developed countries, 3% to 12% of hospitalized patients develop healthcare-associated infections, of which about a quarter occur in ICU Settings, with high rates of antimicrobial resistance and mortality.9 While Shi et al assessed that nosocomial infections caused by MDR and extensively drug-resistant (XDR) Acinetobacter baumannii are associated with high mortality in the ICU.10 Indeed, antimicrobial resistance is a particular challenge in the ICU.11 One major challenge in tackling MDR is understanding its prevalence, risk factors, mortality, etc., especially in areas with little surveillance and sparse data. However, the pattern of MDR pathogens responsible for nosocomial infections appears to be changed geographically and temporally. While a particular MDR may be endemic in one region, the same pathogen may be rare in other areas.12 Therefore, local epidemiological characteristics are key in determining the preferred strategy for combating MDR.
In the present study, we have outlined the prevalence and epidemiology of various MDR bacteria in the ICU. We also dissected the risk factors between MDR and no-MDR. Further, we established a risk-predictive nomogram for patients with MDR infection. Besides, the risk factor and in-hospital mortality of patients with MDR also be assessed. We hope that this analysis will serve as a starting point to improve the identification and preventive management of patients at increased risk of infection and to improve clinical outcomes for patients.
Patients and Methods
Study Setting and Data Collection
We performed a retrospective study from January 2021 to March 2022 in the ICU of the Southern Medical University of Shunde Hospital, Foshan City, Guangdong Province, China. All patients (aged ≥18 years) who were admitted to ICU and had at least one positive microbiological culture were included in the study. The drug susceptibility results of the same strain of each patient were analyzed only once, and the repeated culture strains were excluded. We reviewed patients’ medical records and collected the following data: age, gender, co-morbidities, length of stay (LOS), underlying diseases, number of invasive procedures or surgeries during hospitalization, septic shock, antimicrobial susceptibility tests (ASTs) results. The levels of total protein (TP (reference range:60–80g/L)), albumin (ALB), blood urea nitrogen (BUN), creatinine (Cr), leucocyte count (WBC), red blood cell count (RBC), Hemoglobin (Hb), and procalcitonin (PCT). The primary clinical outcome was in-hospital mortality. The study protocol was approved by the Institutional Review Board of Shunde Hospital of Southern Medical University.
Study Groups and Definitions
The patients were divided into two groups according to the results of bacterial drug susceptibility cultured during hospitalization. Patients with at least one MDR bacteria were assigned to the MDR group, and those who grew only non-MDR organisms on all cultures during hospitalization were assigned to the non-MDR group. MDR refers to bacteria that are resistant to 3 or more classes of antibiotics simultaneously.13–15 Besides, all Vancomycin-resistant Enterococcus (VRE), methicillin-resistant Staphylococcus aureus (MRSA), carbapenem-resistant Enterobacterales (CRE), and extended-spectrum β-lactamase (ESBL) Enterobacterales are also considered as MDR.16 An ESBL-producing Enterobacterales refers to those resistant to the first, second, and third-generation cephalosporins or reported to produce ESBL according to the results of the modified Hodge test.17 CRE was defined as Enterobacterales that were resistant to carbapenem antibiotics. Extensively drug-resistance (XDR) was defined as insensitivity to all classes of antibiotics (at least one in each class) except one or two classes.13,14 Pan drug-resistant (PDR) refers to insensitivity to all drugs in all antimicrobial classes.13,14
Diagnostic and Drug Susceptibility Test
Clinical specimens were identified after conventional culture, and related operations were completed by the hospital’s microbiology laboratory. Vitek 2 system (Biomerieux, France) was used for species identification and antibiotic sensitivity test. The minimum inhibitory concentration was established according to the Clinical and Laboratory Standards Institute (2019) guidelines.18 Specimen sources include a respiratory sample (sputum, bronchoalveolar lavage, and nasopharyngeal swabs), blood, secretions, catheters, and sterile body fluids (pleural and abdominal fluid, cerebrospinal fluid, pus, and various puncture fluids).
Statistical Analysis
Continuous variables were performed using the Mann–Whitney U-test, while the categorical variables were analyzed using chi-square tests. Continuous variables were expressed as the median and interquartile range (IQR), whereas the categorical variables were presented as numbers and percentages. Risk factors for MDR were explored using univariate and multivariate logistic regression analyses. A Cox regression analysis was conducted to reveal the independent variables for in-hospital mortality. The results were listed as odds ratio (OR) or hazard ratio (HR) and 95% confidence intervals (CIs). Kaplan–Meier (KM) survival curves were generated with Log-rank test analysis. The nomogram was constructed performing with the “rms” package. P < 0.05 was considered statistically significant, and all tests were two-tailed. All statistics were analyzed using R version 3.6.3 (The R Foundation, Vienna, Austria).
Results
Patient Characteristics
A total of 278 patients were enrolled in the study. The median age was 65 years (IQR 50.25–73 years), and 202 (72.66%) were male. The details of demographic and clinical characteristics are shown in Table 1. The number of bacteria≥3 (25.09% vs 5.63%), multiple invasive procedures (60.84% vs 41.07%), and LOS (27 (14.25–47) day vs 19.5 (9–36.25) day) were significantly high in MDR group as compared to the no-MDR cohort. The Hb in the MDR group was lower than that in the no-MDR group (89 (77.25–102.75) g/L vs 96 (80–115) g/L).
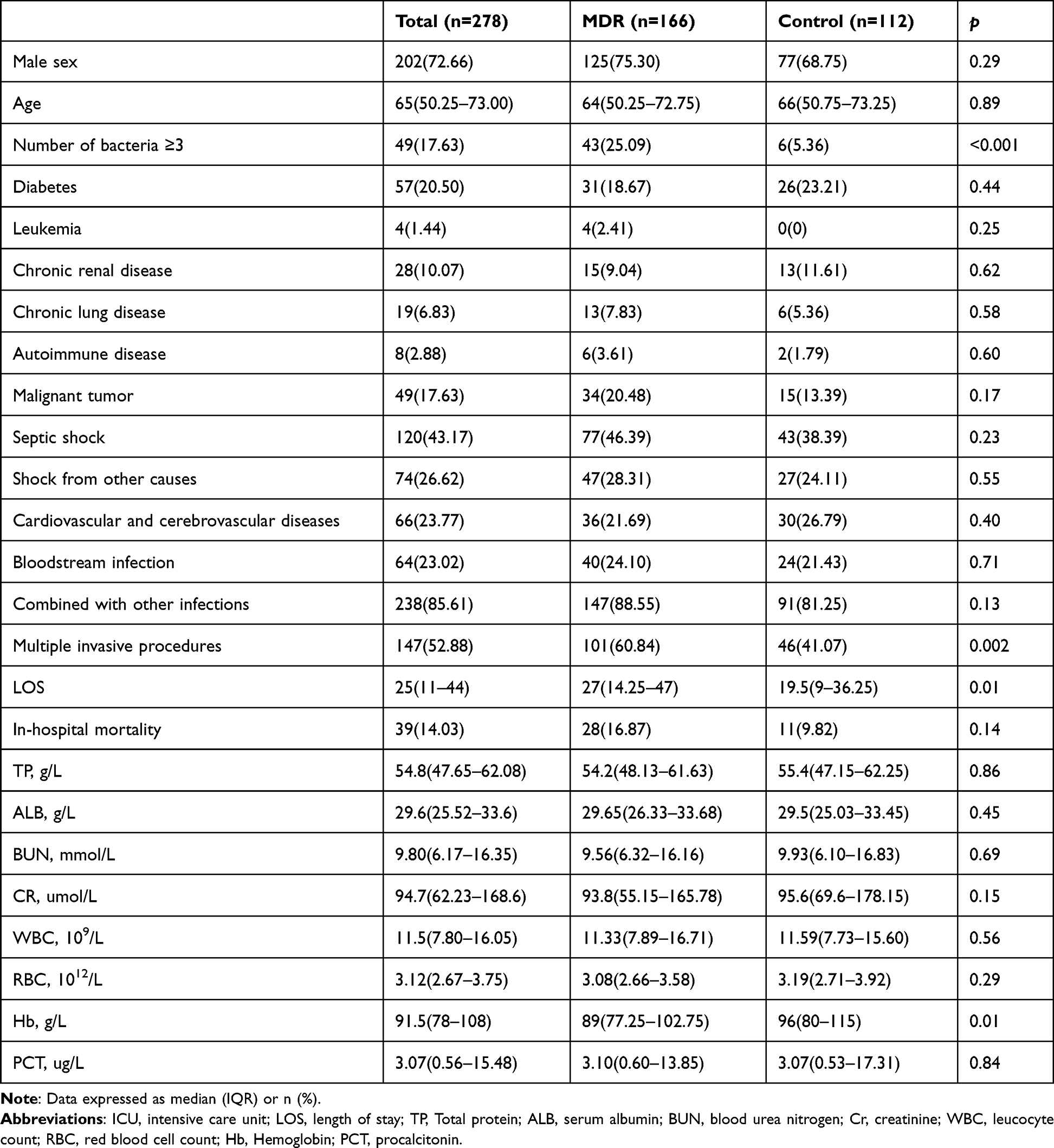 |
Table 1 Clinical and Demographic Characteristics of the ICU Patients |
Distribution Characteristics of Pathogen ICU Patients
483 strains were isolated from 278 ICU patients, with an incidence shown in Table 2. The majority were Enterobacterales species 192 (39.75%), followed by Acinetobacter spp. 68 (14.08%), Pseudomonas spp. 66 (13.66%), Staphylococcus spp. 44 (9.11%), and Enterococcus spp. 34 (7.04%). Specifically, for all pathogens, gram-negative bacteremia (GNB) accounted for 364 (75.36%). Klebsiella pneumoniae 104 (28.57%) is the main species, followed by Acinetobacter baumannii 65 (17.85%), Pseudomonas aeruginosa 59 (16.21%), and Escherichia coli 52 (14.29%).
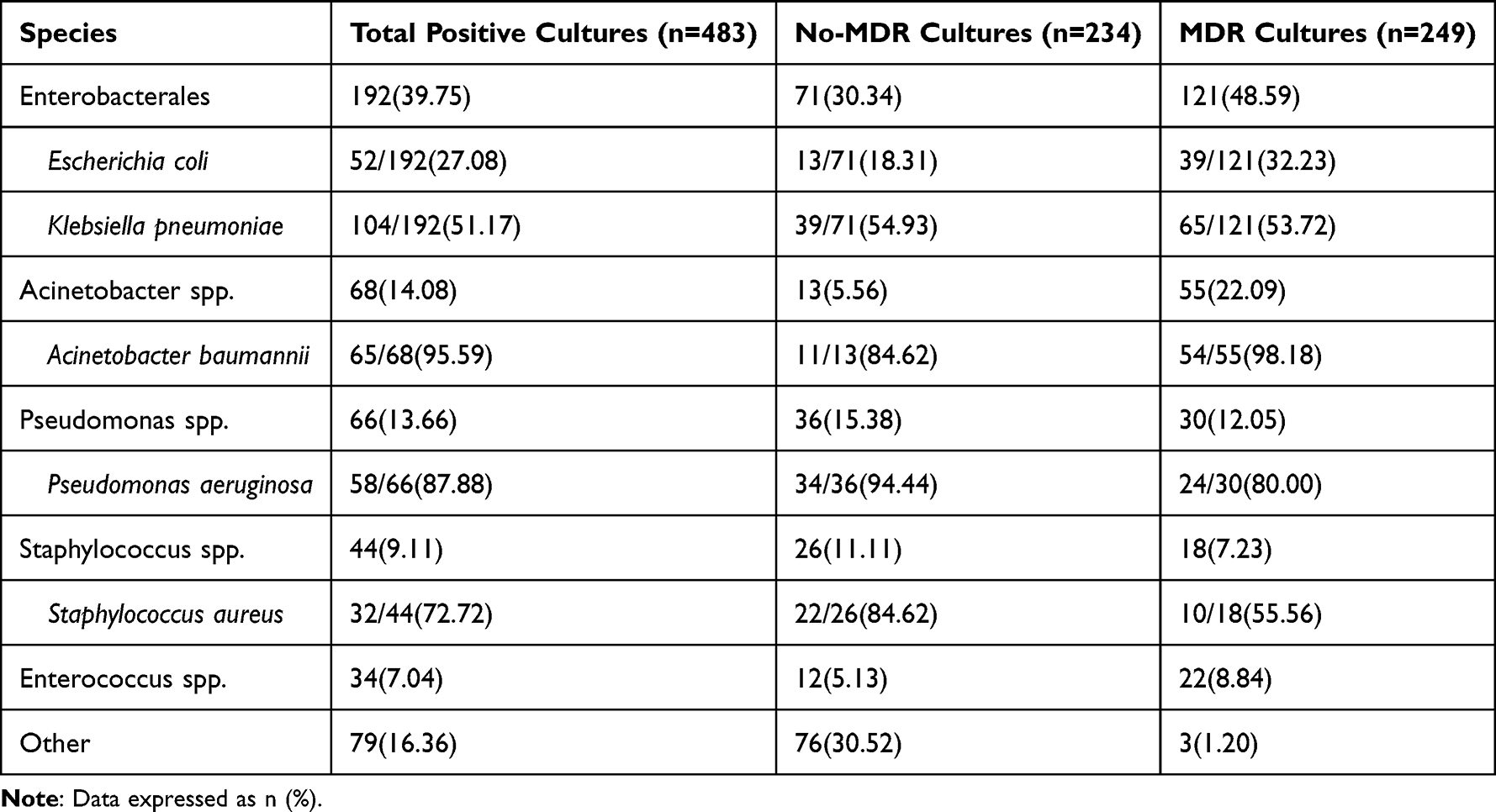 |
Table 2 Distribution of Main Pathogenic Bacteria in ICU Patients |
Prevalence of MDR Bacteria
A summary of total positive cultures and patients with positive cultures is presented in Table 3. Of the 483 positive cultures from 278 patients, 249 (51.55%) had at least one MDR pathogen, including XDR 77 (30.92%) and PDR 39 (15.66%), respectively. In addition, MRSA, ESBL, CRE, Carbapenem-resistant Pseudomonas aeruginosa (CRPA), Carbapenem-resistant Acinetobacter baumannii (CRAB), and VRE isolated from all positive cultures were 7 (1.45%), 93 (19.25%), 54 (11.18%), 15 (3.11%), 51 (10.56) and 0 (0%). Among 278 patients, 166 (59.71%) had at least one MDR pathogen. Of the 166 patients, XDR 47 (28.31%) and PDR 38 (22.89%) pathogens grew, respectively. The pathogens of MRSA 6 (2.16%), ESBL 89 (32.01%), CRE 53 (19.06%), CRPA15 (5.40%), CRAB51 (18.35%), and VRE 0 (0%) were found in all patients.
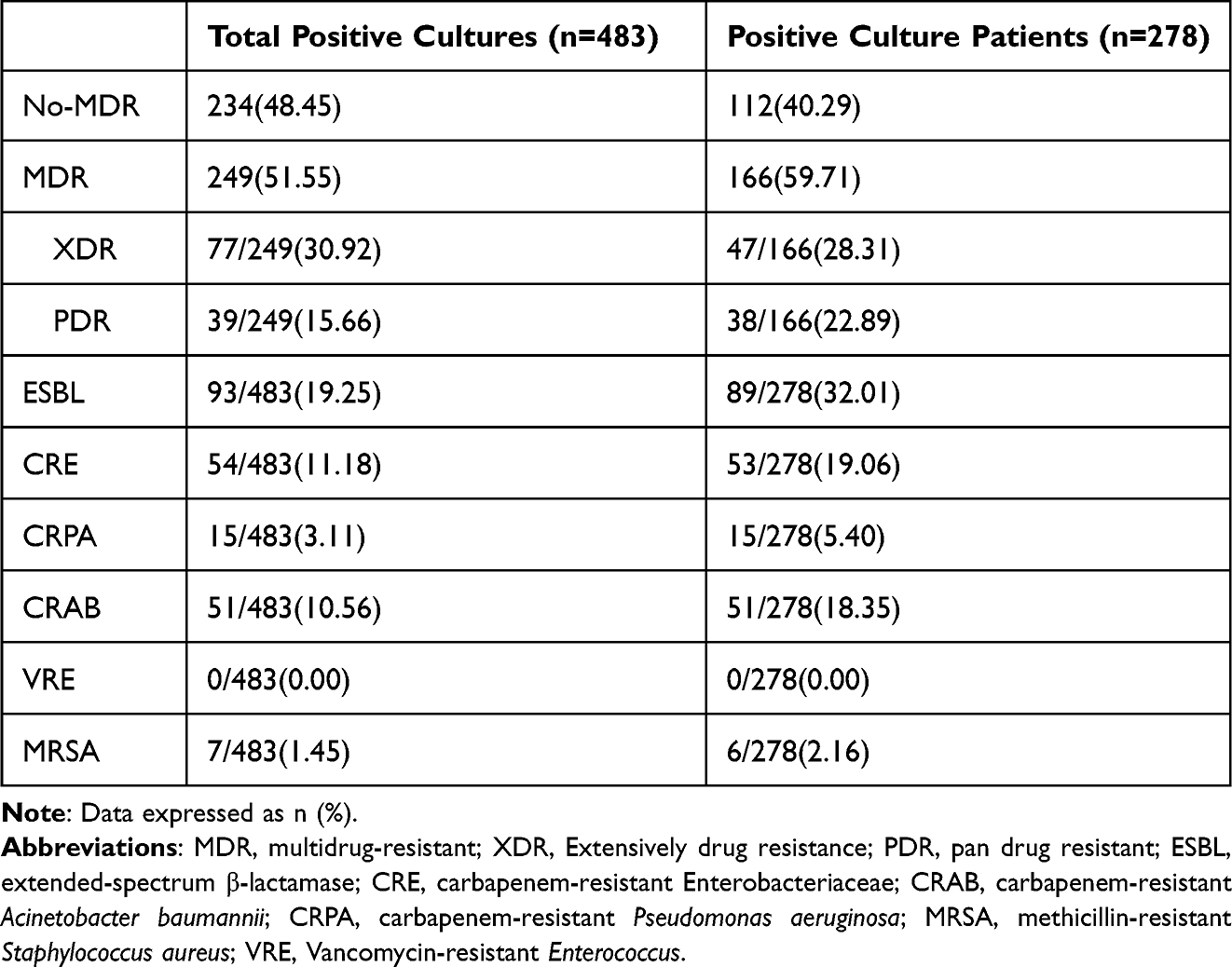 |
Table 3 The Incidence of MDR Pathogens in ICU Patients |
Presentation of a Prediction Model for Patients with MDR
Potential predictors with a P-value < 0.3 in the univariate logistic regression analysis were included in multivariate analyses (Figure 1A). The multivariate analysis revealed that the variable associated with MDR pathogens were (Figure 1B): number of bacteria (OR 2.91, 95% CI 1.97–4.29, P < 0.001), multiple invasive procedures (OR 2.23, 95% CI 1.37–3.63, P = 0.001), length of stay (OR 1.01, 95% CI 1.00–1.02, P = 0.007), Hb (OR 0.99, 95% CI 0.98–1.00, P = 0.01). And then, we construct a nomogram based on the above independent factors to predict the probability of the occurrence of MDR infection in ICU patients. (Figure 2A). Immediately, the ROC curve was drawn to validate the predictive accuracy of the nomogram (Figure 2B). The ROC results had areas under the curve of 0.75 (95% CI: 0.70–0.81), indicating good discrimination. Additionally, Figure 2C shows the decision curve for the nomogram. The nomogram-based decisions demonstrated superior net benefit, indicating the clinical utility of our nomogram.
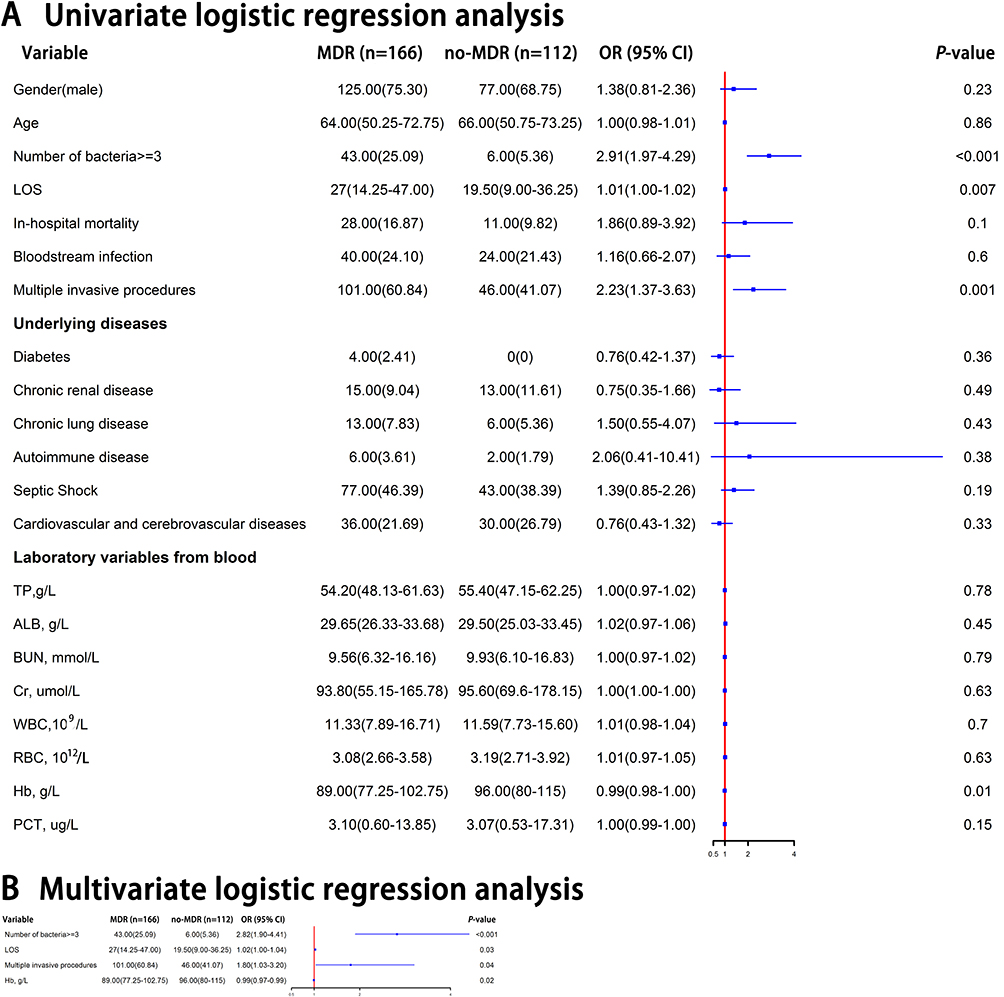 |
Figure 1 Forest plot of predictive factors for MDR infection in ICU patients. (A) Univariate logistic regression analysis of the risk factors for MDR infection in ICU patients; (B) multivariate logistic regression analysis of independent predictors of MDR infection. Abbreviations: CI, confidence interval; ICU, intensive care unit; OR, odds ratio; LOS, length of stay; TP, total protein; ALB, serum albumin; BUN, blood urea nitrogen; Cr, creatinine; WBC, leucocyte count; RBC, red blood cell count; Hb, Hemoglobin; PCT, procalcitonin. |
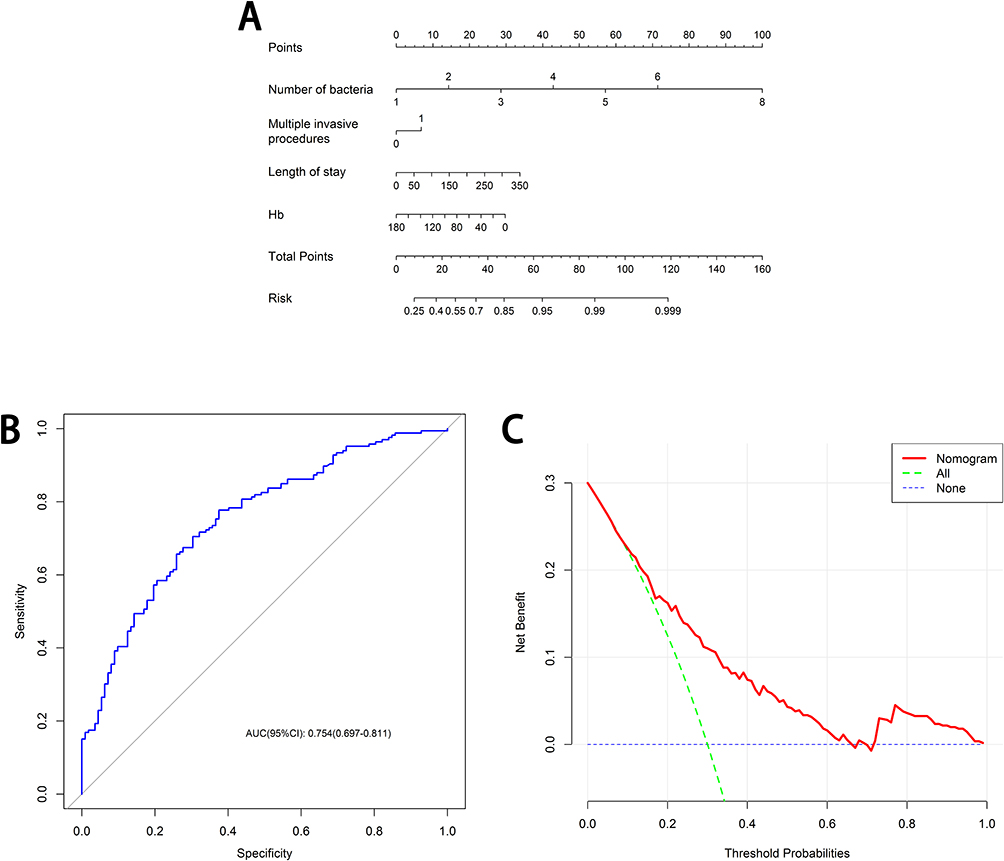 |
Figure 2 (A) The nomogram to predict the occurrence of MDR infection in ICU patients. This nomogram provides a method to predict the probability of occurrence of MDR infection based on the number of bacteria, multiple invasive procedures, length of stay, and Hb. (B) The receiver operating characteristic curves for the nomogram. (C) Decision curves for the overall incidence of MDR infection based on the nomogram. The green dotted line: predicts the net benefit for all patients; the blue dotted line: predicts the net benefit of no patient; Red line: net benefit to patients as predicted by nomogram. Abbreviation: Hb, Hemoglobin. |
Predictors of In-Hospital Mortality in Patients with MDR Pathogens
We performed Cox regression analyses in MDR patients to identify independent in-hospital mortality of risk factors associated with MDR pathogens. The results showed that XDR (HR, 2.60; 95% CI: 1.08–6.25; P = 0.03) and TP (HR, 0.95; 95% CI: 0.91–0.99; P = 0.03) were the independent factors for fatal outcomes (Figure 3). In addition, the KM curves were plotted to confirm that infection with XDR (P =0.02) or PDR (P =0.02) has a higher risk of mortality (Figure 4).
 |
Figure 3 Forest plot of predictors of in-hospital mortality in patients with MDR pathogens. (A) Univariate Cox regression analysis of the risk factors of in-hospital mortality in patients with MDR pathogens. (B) Multivariate logistic regression analysis of independent predictors of in-hospital mortality in patients with MDR pathogens. Abbreviations: CI, confidence interval; ICU, intensive care unit; HR, hazard ratio; XDR, extensively drug-resistance; PDR, pan drug-resistant; TP, total protein; ALB, serum albumin; BUN, blood urea nitrogen; Cr, creatinine; WBC, leucocyte count; RBC, red blood cell count; Hb, Hemoglobin; PCT, procalcitonin. |
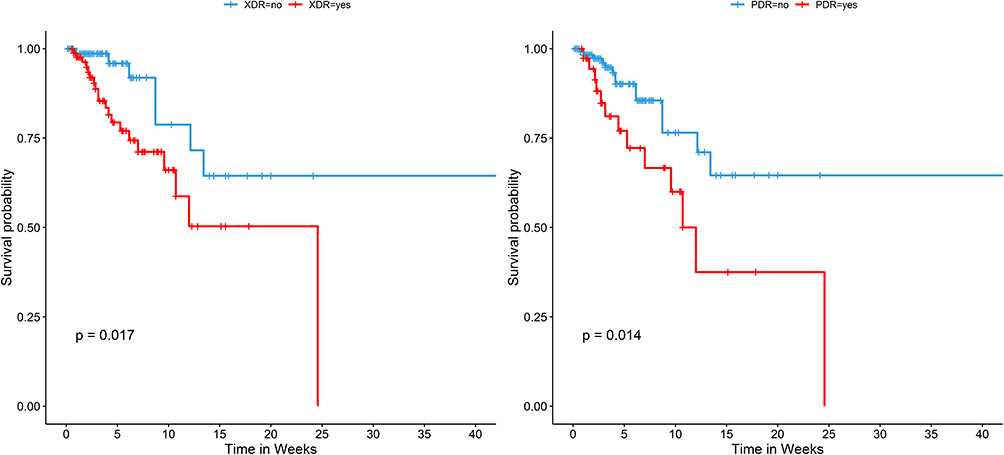 |
Figure 4 Kaplan–Meier survival curves estimate the mortality among patients with XDR or PDR. Abbreviations: XDR, Extensively drug-resistance; PDR, pan drug-resistant. |
Discussion
MDR has emerged as one of the most serious threats, particularly in the ICU of the hospital. An estimated 4.95 million deaths were associated with MDR infections globally in 2019, including 1.27 million deaths directly attributable to drug resistance.19 Despite the importance of epidemiology and the generation of large amounts of clinical data, patterns of MDR vary geographically, with different pathogens and pathogen-drug combinations predominant in different regions. Additionally, the evidence supporting the management of MDR infection remains patchy. To improve the effectiveness of empirical and targeted therapy, we evaluated local prevailing pathogens in ICU patients, assessment of risk factors for MDR microorganisms, and established a nomogram for predicting MDR infection.
In this retrospective, 278 patients were enrolled, including 166 patients with MDR and 112 with no MDR. We identified that number of bacteria, multiple invasive procedures, LOS, and Hb were associated with MDR pathogens. Thus, a nomogram with 4 independent predictors was constructed to predict the probability of the occurrence of MDR infection in ICU patients. A significant advantage of our nomogram is that all parameters are available from laboratory data or routine examinations. Further, the nomogram is a simple and practical clinical system. As long as the results of the correlation factors are entered into the nomogram, the corresponding results are easily obtained. Thus, our nomogram could help clinicians quickly identify high-risk patients and make management decisions. The area under the ROC curve was 0.75, which displayed good discrimination ability for predicting MDR pathogens. Additionally, the nomogram-based decision curve demonstrated superior net benefit, indicating the clinical utility of our nomogram.
A recent study reported that male sex, CRP levels, and Pitt scores were independent predictors of MDR organism colonization or infection in ICU patients.20 The nomogram established in the present study incorporated four factors, number of bacteria, multiple invasive procedures, LOS, and Hb. Many previous studies showed prolonged hospital length of stay was a possible risk factor for MDR.21–23 Similarly, invasive procedures were also confirmed as an independent risk factor in some studies including our study.24–28 Compared with previous assessments, we also found some novel risk factors, including multiple bacterial infections and low Hb. Infection with MDR organisms causes significant mortality in hospitalized patients.27 As expected, XDR and TP were found to be independent predictors of in-hospital mortality. The KM curve further confirms that infection with XDR (P =0.02) or PDR (P =0.02) has a higher risk of in-hospital mortality, in line with previous research.29–31
Another main objective of this study was to evaluate the incidence of MDR organism infections in ICU patients. Strikingly, in our study, the incidence of MDR organisms accounted for 59.71% of patients, quite higher than the global prevalence of infections sustained by MDR organisms.28 The incidence of XDR and PDR pathogens was 28.31% and 22.89%, respectively, far higher than previously reported.26 Significant differences in bacterial distribution and types across geographic regions. Wang20 showed that Acinetobacter baumannii (n = 62, 30.0%) was the most common gram-negative bacteria in the ICU, while the main pathogen in our study was Klebsiella pneumoniae. At this point, monitoring the demographics, prevalence trends, and transmission of patients with MDR infection can help control these infections and improve patient outcomes. Efforts should be made to limit the spread of multidrug-resistant bacteria, especially multidrug-resistant Klebsiella pneumoniae in our region.
In conclusion, the number of bacteria, multiple invasive procedures, LOS, and Hb were the independent predictors associated with MDR pathogens. The nomogram to Predict the probability of MDR infection was constructed based on the risk factors, and it showed good discrimination ability and clinical utility. Thus, our nomogram is available for clinicians to identify patients at high risk for MDR infection. Future prospective studies should be conducted to verify the predictive value of the model. Besides, we also identify XDR and TP were the independent risk factors for in-hospital mortality among ICU patients with MDR infection. The KM curve further confirms that infection with XDR or PDR has a higher risk of in-hospital mortality. Our study also describes the current prevalence of MDR strains in the ICU. The regional estimates may be useful to adjust local responses and provide data to support future comprehensive assessments. Identifying risk factors and taking appropriate measures against them or microbiological screening of patients can reduce MDR infection.32 It also reported that additional infection control nurse positions could significantly reduce MDR transmission.33 In addition, reducing the use of invasive devices, hand hygiene, and antimicrobial management remains the optimal treatment strategy for managing MDR.27 All in all, the principles of infection prevention and control remain the foundation of widespread infection prevention and the cornerstone of curbing the spread of drug resistance.34,35 Additionally, given the limited options available for treating bacterial infections with MDR, new antibiotics should be developed.
Abbreviations
MDR, multidrug-resistant; XDR, Extensively drug resistance; PDR, pan drug resistant; ESBL, extended-spectrum β-lactamase; CRE, carbapenem-resistant Enterobacterales; CRAB, carbapenem-resistant Acinetobacter baumannii; CRPA, carbapenem-resistant Pseudomonas aeruginosa; MRSA, methicillin-resistant Staphylococcus aureus; VRE, Vancomycin-resistant Enterococcus; ICU, intensive care unit; LOS, length of stay; TP, Total protein; ALB, serum albumin; BUN, blood urea nitrogen; Cr, creatinine; WBC, leucocyte count; RBC, red blood cell count; Hb, Hemoglobin; PCT, procalcitonin.
Data Sharing Statement
Due to the principles of medical research ethics and confidentiality, the clinical data are not publicly available. However, in addition to personal private information, other research data may also be obtained from the corresponding authors with the consent of the ethics committee.
Ethics Statement
The studies involving human participants were reviewed and approved by the southern medical university (The first people’s hospital of Shunde) of the Ethics Committee. Written informed consent to participate in this study was provided by the patients. This study complies with the Declaration of Helsinki.
Acknowledgment
The authors would like to thank everyone who contributed to this research.
Funding
This work was funded by 2019 the Science and Technology Innovation Project from Foshan, Guangdong (1920001000706 to C. WU).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chacko B, Thomas K, David T, Paul H, Jeyaseelan L, Peter JV. Attributable cost of a nosocomial infection in the intensive care unit: a prospective cohort study. World J Crit Care Med. 2017;6(1):79–84. doi:10.5492/wjccm.v6.i1.79
2. Bergmann JN, Killen-Cade RR, Parish LA, Albrecht MT, Wolfe DN. Partnering on Vaccines to Counter Multi-Drug Resistant Threats: Workshop Proceedings, Biomedical Advanced Research and Development Authority. Taylor & Francis; 2022.
3. Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309–318.
4. Bloom G, Merrett GB, Wilkinson A, Lin V, Paulin S. Antimicrobial resistance and universal health coverage. BMJ Glob Health. 2017;2(4):e000518.
5. World Health Organization. Global antimicrobial resistance and use surveillance system (GLASS) report: 2021; 2021.
6. Han Y, Zhang J, Zhang HZ, Zhang XY, Wang YM. Multidrug-resistant organisms in intensive care units and logistic analysis of risk factors. World J Clin Cases. 2022;10(6):1795–1805.
7. Hu F, Zhu D, Wang F, Wang M. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(suppl_2):S128–s34.
8. Hanberger H, Arman D, Gill H, et al. Surveillance of microbial resistance in European intensive care units: a first report from the Care-ICU programme for improved infection control. Intensive Care Med. 2009;35(1):91–100.
9. Luna CM, Rodriguez-Noriega E, Bavestrello L, Guzmán-Blanco M. Gram-negative infections in adult intensive care units of latin america and the Caribbean. Crit Care Res Pract. 2014;2014:480463.
10. Shi J, Sun T, Cui Y, et al. Multidrug resistant and extensively drug resistant Acinetobacter baumannii hospital infection associated with high mortality: a retrospective study in the pediatric intensive care unit. BMC Infect Dis. 2020;20(1):597. doi:10.1186/s12879-020-05321-y
11. De Waele JJ, Boelens J, Leroux-Roels I. Multidrug-resistant bacteria in ICU: fact or myth. Curr Opin Anaesthesiol. 2020;33(2):156–161. doi:10.1097/ACO.0000000000000830
12. Blot S, Antonelli M, Arvaniti K, et al. Epidemiology of intra-abdominal infection and sepsis in critically ill patients: “AbSeS”, a multinational observational cohort study and ESICM trials group project. Intensive Care Med. 2019;45(12):1703–1717. doi:10.1007/s00134-019-05819-3
13. Masters BR. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Graefes Arch Clin Exp Ophthalmol. 2016;254(11):2285–2287. doi:10.1007/s00417-015-2950-1
14. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
15. Gilbert DN. The Sanford guide to antimicrobial therapy 2011. Antimicrob Ther. 2011;2011:4–62.
16. Siegel JD, Rhinehart E, Jackson M, Chiarello L. Management of multidrug-resistant organisms in health care settings, 2006. Am J Infect Control. 2007;35(10 Suppl 2):S165–93. doi:10.1016/j.ajic.2007.10.006
17. Rawat D, Nair D. Extended-spectrum β-lactamases in Gram Negative Bacteria. J Glob Infect Dis. 2010;2(3):263–274. doi:10.4103/0974-777X.68531
18. Laboratory C, Institute S. Performance Standards for Antimicrobial Susceptibility Testing. PA: Clinical Laboratory and Standards Institute Wayne; 2019.
19. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
20. Wang L, Huang X, Zhou J, et al. Predicting the occurrence of multidrug-resistant organism colonization or infection in ICU patients: development and validation of a novel multivariate prediction model. Antimicrob Resist Infect Control. 2020;9(1):66. doi:10.1186/s13756-020-00726-5
21. Zaragoza R, Vidal-Cortés P, Aguilar G, et al. Update of the treatment of nosocomial pneumonia in the ICU. Crit Care. 2020;24(1):383. doi:10.1186/s13054-020-03091-2
22. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT. Eur Respir J. 2017;50:3.
23. Burillo A, Muñoz P, Bouza E. Risk stratification for multidrug-resistant Gram-negative infections in ICU patients. Curr Opin Infect Dis. 2019;32(6):626–637. doi:10.1097/QCO.0000000000000599
24. Vasudevan A, Mukhopadhyay A, Li J, Yuen EG, Tambyah PA. A prediction tool for nosocomial multi-drug Resistant Gram-Negative Bacilli infections in critically ill patients - prospective observational study. BMC Infect Dis. 2014;14:615. doi:10.1186/s12879-014-0615-z
25. Sonti R, Conroy ME, Welt EM, Hu Y, Luta G, Jamieson DB. Modeling risk for developing drug resistant bacterial infections in an MDR-naive critically ill population. Ther Adv Infect Dis. 2017;4(4):95–103. doi:10.1177/2049936117715403
26. Cucci M, Wooten C, Fowler M, Mallat A, Hieb N, Mullen C. Incidence and risk factors associated with multi-drug-resistant pathogens in a critically ill trauma population: a retrospective cohort study. Surg Infect. 2020;21(1):15–22. doi:10.1089/sur.2019.031
27. Strich JR, Palmore TN. Preventing transmission of multidrug-resistant pathogens in the intensive care unit. Infect Dis Clin North Am. 2017;31(3):535–550. doi:10.1016/j.idc.2017.05.010
28. Piano S, Singh V, Caraceni P, et al. Epidemiology and effects of bacterial infections in patients with cirrhosis worldwide. Gastroenterology. 2019;156(5):1368–80.e10.
29. Roberts RR, Hota B, Ahmad I, et al. Hospital and societal costs of antimicrobial-resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship. Clin Infect Dis. 2009;49(8):1175–1184.
30. Mathers AJ, Cox HL, Kitchel B, et al. Molecular dissection of an outbreak of carbapenem-resistant Enterobacteriaceae reveals intergenus KPC carbapenemase transmission through a promiscuous plasmid. mBio. 2011;2(6):e00204–11.
31. Snitkin ES, Zelazny AM, Thomas PJ, et al. Tracking a hospital outbreak of carbapenem-resistant Klebsiella pneumoniae with whole-genome sequencing. Sci Transl Med. 2012;4(148):148.
32. Wang Z, Xia Z. What we can do? The risk factors for multi-drug resistant infection in pediatric intensive care unit (PICU): a case-control study. Ital J Pediatr. 2020;46(1):17.
33. Xu W, He L, Liu C, et al. The effect of infection control nurses on the occurrence of pseudomonas aeruginosa healthcare-acquired infection and multidrug-resistant strains in critically-ill children. PLoS One. 2015;10(12):e0143692.
34. Silva AC, Nogueira PJ, Paiva J-A. Determinants of antimicrobial resistance among the different European countries: more than human and animal antimicrobial consumption. Antibiotics. 2021;10(7):834.
35. Tacconelli E, Pezzani MD. Public health burden of antimicrobial resistance in Europe. Lancet Infect Dis. 2019;19(1):4–6.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.