")
Back to Journals » International Medical Case Reports Journal » Volume 15
Tracheobronchomegaly (Mounier-Kuhn Syndrome) in a 43-Year-Old Male: A Case Report
Authors Babirye D , Walubembe J, Babirye JA, Baluku JB , Byakika-Kibwika P , Nabawanuka E
Received 12 August 2022
Accepted for publication 1 November 2022
Published 7 November 2022 Volume 2022:15 Pages 631—637
DOI https://doi.org/10.2147/IMCRJ.S386083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ronald Prineas
Deborah Babirye,1 Jonathan Walubembe,1 Juliet Allen Babirye,2 Joseph Baruch Baluku,2,3 Pauline Byakika-Kibwika,4 Eva Nabawanuka1
1Department of Radiology, Makerere University College of Health Sciences, Kampala, Uganda; 2Department of Research, Makerere University Lung Institute, Kampala, Uganda; 3Division of Pulmonology, Kiruddu National Referral Hospital, Kampala, Uganda; 4Department of Medicine, Makerere University College of Health Sciences, Kampala, Uganda
Correspondence: Deborah Babirye, Department of Radiology, Makerere University College of Health Sciences, PO Box 7072, Kampala, Uganda, Email [email protected]
Abstract: Mounier-Kuhn syndrome (MKS) or congenital tracheobronchomegaly is a rare disorder characterized by marked dilatation of the trachea and main bronchi, bronchiectasis, and recurrent respiratory tract infections. The etiology of this disorder is uncertain and the clinical presentation is variable. The diagnosis is usually made based on the characteristic computed tomography (CT) scan findings. This report describes a case of a 43-year-old man presenting with persistent cough and recurrent lower respiratory tract infections since childhood associated with copious amounts of purulent sputum, difficulty in breathing, and weight loss. In addition, he reported palpitations, dyspnea, orthopnea, abdominal and lower limb swelling. The chest X-ray showed a dilated trachea (35mm) and bronchi (26mm (right) and 27mm (left)) with cystic bronchiectasis and reticulolinear opacities predominantly involving the middle and lower lung zones. Chest CT scan confirmed the diagnosis of MKS as evidenced by dilated trachea and bronchi complicated by diverticula formation. Electrocardiogram, echocardiography and abdominal ultrasound scan showed features of right-sided heart failure secondary to pulmonary hypertension. MKS, although rare, should be considered as a possible diagnosis in patients presenting with productive chronic cough, recurrent pneumonia, or incomplete response to appropriate antibiotic therapy for pneumonia.
Keywords: Mounier-Kuhn syndrome, tracheobronchomegaly, MKS
Introduction
Mounier Kuhn syndrome or congenital tracheobronchomegaly is a rare airway disorder that causes variable dilatation of the trachea and bronchi. There are less than 400 cases reported to date,1 with only three cases described in sub-Saharan Africa to our knowledge.2–4 For unknown reasons, the disease has been found to affect males more than females with a ratio of 8:1.1 An association with smoking has been suggested, although there have been cases reported of lifetime non-smokers.5 MKS is characterized by atrophy or absence of the elastic fibers and smooth muscle tissues of the trachea and main bronchi, resulting in dilatation on inspiration with narrowing or collapse on expiration. The abnormal airway dynamics and pooling of secretions in broad outpouchings of redundant musculomembranous tissue between the cartilaginous rings predispose to the development of chronic pulmonary suppuration, bronchiectasis, emphysema, and pulmonary fibrosis.6
The cause of MKS is unknown, although cigarette smoke and pollutants may be predisposing factors by causing airway inflammation.7
The diagnosis of MKS is based on lung functional tests, bronchoscopy, and radiological imaging which confirms the diagnosis, although specific criteria are not described.1
Case Presentation
A 43-year-old male presented to the Makerere University Lung Institute in Kampala as a referral from a rural tertiary hospital in Uganda. He presented with a 30-year history of a productive cough, whose initial onset followed an episode of cough during a nationwide outbreak of whooping cough at 10 years of age. The cough had worsened over the past one year, had no diurnal variation, was wet and associated with copious amounts of purulent sputum, difficulty in breathing, chest pain and weight loss for 3 months. The chest pain was predominantly left-sided and non-radiating. There was no history of hemoptysis, nasal blockage, loss of sense of smell, fever, or night sweats. Patient reported no history of loud snoring, he had no episodes of gasping for air during sleep and no history of somnolence. He however reported palpitations, dyspnea, orthopnea, and body swelling involving the lower limbs and abdomen. On presentation, he had had several admissions because of worsening cough, and had unscheduled outpatient visits almost monthly for the cough in the past 30 years. He had been treated with intravenous and oral medications with minimal to no improvement. At 19 years of age, he was treated for clinically diagnosed pulmonary TB (no bacteriological confirmation), but with no improvement. He had no known allergies. He denied any history of cigarette smoking and alcohol use. He had no family history of similar illness. He was a farmer until 3 years prior to presentation when the symptoms limited his physical activity.
Physical Examination
On physical examination, he was sick-looking, severely wasted (37kgs body weight, height -160.5cm, BMI-14.4 kilogram per meters2; Figure 1A). He had proptosis grade 3 digital clubbing (Figure 1B), central and peripheral cyanosis and pretibial oedema (Figure 1C). He was afebrile (temperature 36.9°Celsius). He had no pallor, jaundice, lymphadenopathy or signs of dehydration.
 |
Figure 1 General physical examination findings in a man with Mounier Kuhn Syndrome: (A) shows wasting and mild abdominal distension due to ascites, (B) shows grade 3 digital clubbing, (C) shows pitting oedema after removing stockings. |
On respiratory system examination, he had mild respiratory distress with a respiratory rate of 32 breaths per minute (tachypneic). His SPO2 was 99% on room air. He had no chest deformities or asymmetry. The trachea was centrally placed. There was equal air entry bilaterally with bilateral widespread loud harsh breath sounds, bilateral crepitations and rhonchi. In cardiovascular examination, he had a thin volume pulse with a tachycardia of 108 beats/minute. The blood pressure was normal (92/70mmHg). The apex beat was in the 5th intercostal space, mid-clavicular line. The heart sounds I and II were heard, with a 3rd heart sound (a gallop rhythm) and a loud second heart sound in the pulmonary area (loud P2). On abdominal examination, he had mild abdominal distension, shifting dullness (indicative of moderate ascites), and a tender hepatomegaly of 8 cm below the coastal margin with a positive hepatojugular reflux.
Diagnostic Work Up
The diagnostic work up is summarized in Table 1. Serum creatinine, urea, electrolytes, liver enzymes, bilirubin were all normal. Spirometry evaluation was attempted but he had very poor respiratory effort to complement the examination.
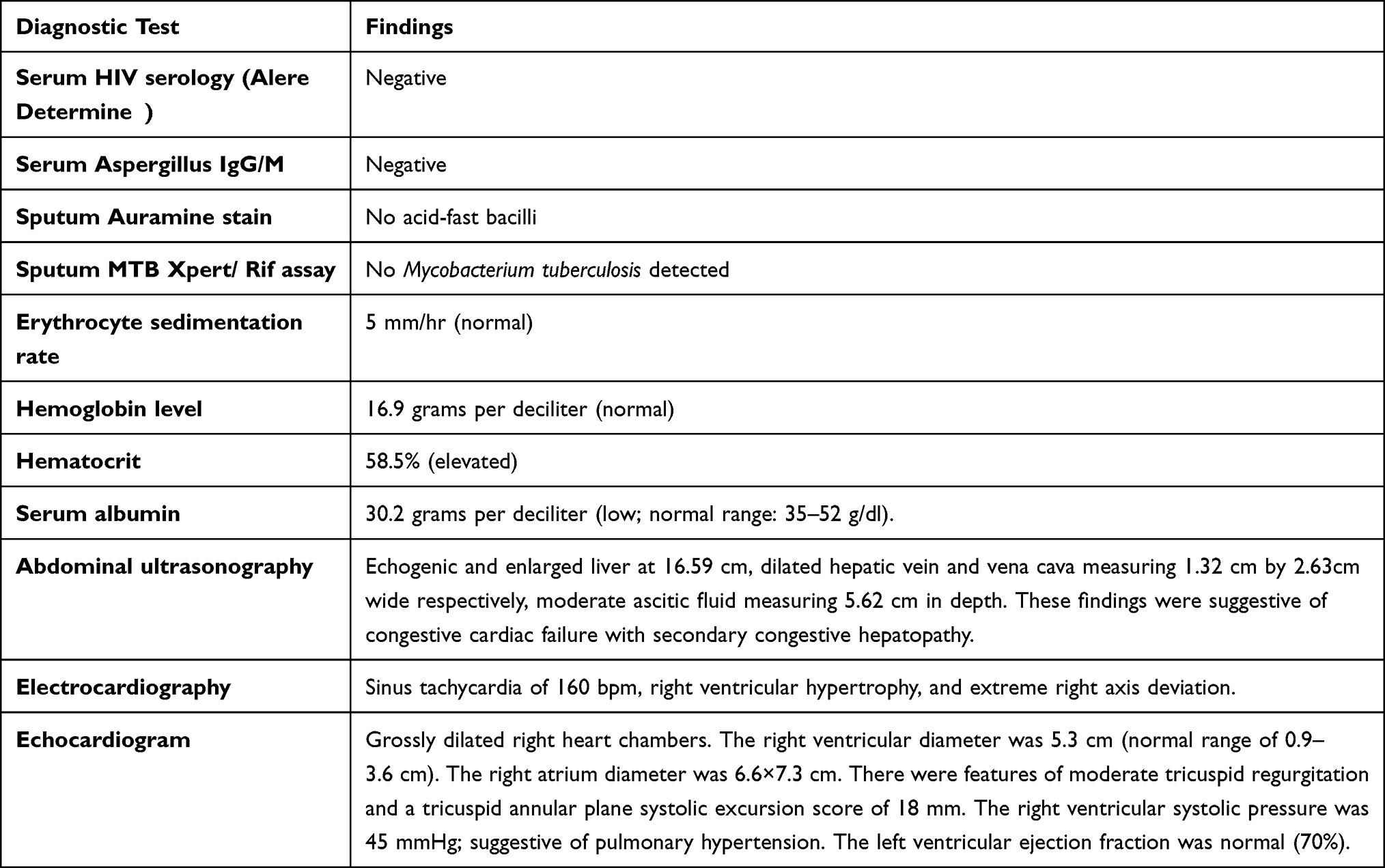 |
Table 1 Diagnostic Work Up in a Man with Mounier Kuhn Syndrome |
Radiological Imaging
The chest X-ray showed dilated trachea and principal bronchi with diffuse reticulolinear and ring-like opacities involving mainly the mid and lower lung zones bilaterally. Figure 2 shows the chest X-ray. A sequential high resolution computed tomography (HRCT) scan was performed using a 128-slice multidetector CT scanner. The study was performed in full inspiration with a scan time of five seconds. The scan time was short enough to enable the patient hold his breath throughout the scanning period and this avoided motion artifacts. An expiratory scan would have complemented the findings; however, this was not performed. Figures 3–5show the High-resolution chest computed tomography (HRCT).
 |
Figure 2 Chest x-ray images AP (A) and lateral (B), showing the dilated trachea (block arrow) and right principal bronchus (notched arrow) with diffuse reticulolinear opacities and cystic bronchiectasis of the lower lung zones. |
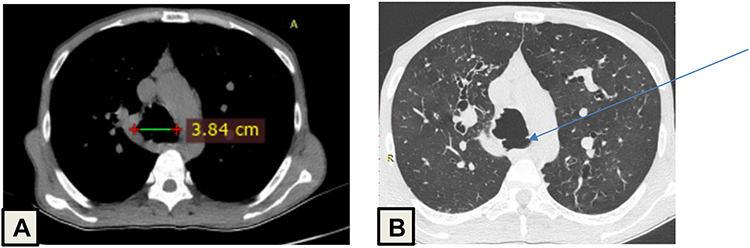 |
Figure 3 Axial CT images (A) is soft tissue window demonstrating a dilated trachea (measurement calipers) and (B) is a lung window demonstrating a tracheal diverticulum (arrow). |
 |
Figure 4 Coronal CT scans, lung window: (A) demonstrates the grossly dilated and tortuous principal bronchi (measurement calipers), Right bronchus measures 4.25cm and left bronchus measures 3.81cm; (B) demonstrates cystic and varicose bronchiectasis. |
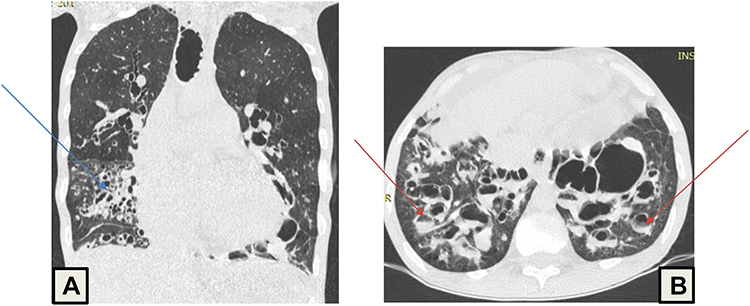 |
Figure 5 CT images lung window: (A) demonstrating ground glass opacities and bronchiectasis in the right middle lobe (blue arrow) and (B) demonstrating mucus filled bronchi with air fluid levels (orange arrows). |
Diagnosis and Treatment
In this patient, a diagnosis was made of tracheobronchomegaly (Mounier Kuhn syndrome), complicated with pulmonary hypertension, and right-sided heart failure. Differential diagnoses of cystic fibrosis and bronchiectasis were considered. The patient was initiated on oral prednisolone 20 mg (short-course), oral furosemide 40 mg, rhinathiol syrup, oral azithromycin (empirically for suspected lung infection), megestrol (for cachexia), and low-dose oral morphine (for the dyspnea), inhaled corticosteroid/long-acting beta agonist, inhaled tiotropium, and chest physiotherapy. Two months later, the patient reported improvement. The sputum volume was much less, had less exercise intolerance and had gained 3 kgs. He was also linked to the palliative care team to offer home-based palliative care in addition to the long-term therapies above. He was also scheduled for monthly reviews at the Makerere University Lung Institute. However, he passed away from home in the fourth month of follow-up from a lung infection that was managed at a peripheral rural health facility.
Discussion
Mounier Kuhn syndrome is a rare condition characterized by marked tracheobronchial dilatation with trachea measuring more than 30mm and bronchi measuring more than 24 and 23 mm for right and left, respectively.7 The etiology is unknown but thought to have familial susceptibility and inheritance through autosomal recessive mechanisms. Histological findings of MKS reveal atrophy or absence of the elastic tissue and smooth muscles of the trachea and bronchi leading to dilatation with formation of diverticula.7,8 Patients are usually diagnosed in the 3rd or 4th decade of life despite a long history of respiratory symptoms.6 This is because the symptoms are usually nonspecific. The patient presented in this case was diagnosed at the age of 43 years after a 30-year history of respiratory symptoms.
The clinical presentation varies widely, ranging from asymptomatic disease with preserved lung functions to recurrent chest infections, wheezing, exertional dyspnea progressing to severe respiratory failure and death.9,10 In developing countries some patients have received therapy for tuberculosis even without evidence of the presence of tuberculosis bacteria.11 TB treatment before diagnosis of MKS was seen in this case and is reported in two other cases reported by Shahin in Zambia and Mkandawire in Namibia.2,3 This patient also presented with symptoms like palpitations, dyspnea, orthopnea, abdominal swelling and pedal edema. These were suggestive of right-sided heart failure secondary to pulmonary hypertension. There are no case reports in the literature showing this association. However, in this case, the complications could have been brought about by the delayed diagnosis and improper initial management of MKS.
Although many studies have documented an association of MKS with smoking, this patient had no history of smoking, although there could have been exposure to pollutants as the family mainly uses charcoal and firewood for cooking. The history of a cough during nationwide outbreak of whooping cough in this case raises the possibility of an infectious agent as a trigger for the subsequent airway damage.
The diagnosis of MKS is based on lung function tests, bronchoscopy, and radiological imaging which confirms the diagnosis.7,12 Bronchoscopy shows proximal airway dilation, tracheal and bronchial diverticula and retained secretion. Lung function tests using spirometry reveals an obstructive pattern which supplements the diagnosis.13 In this patient, bronchoscopy was not performed due to hypercapnia and the high risk of acute respiratory failure. Spirometry was attempted but stopped due to poor respiratory effort. Radiological imaging with chest x ray and computed tomography (CT) scan confirms the diagnosis of MKS by demonstrating the abnormally large trachea and bronchi at times with associated complications of diverticula, bronchiectasis, and infections as was seen in this case. In adults, the CT diagnostic criteria are tracheal diameters > 30mm, main bronchi diameters of >24mm and 23 mm for right and left, respectively.6,14 The patient presented in this case, had a trachea measuring 38.4mm with the right and left main bronchi measuring 42.5mm and 38.1mm respectively. A thin slice, volumetric MDCT paired inspiratory and expiratory protocol or dynamic MDCT during full respiratory cycle allows exquisite visualization of the airways and contribute to the accurate evaluation of abnormalities in the lung parenchyma and airways.15 Inspiratory phase demonstrates the maximum diameter of the airway with significant collapse on expiratory phase which confirms the diagnosis of MKS. In this case, however, a sequential HRCT was used with only the inspiratory phase obtained. Although we were able to get diagnostic information, this would have been boosted further if the right protocol had been applied. Reconstructive methods including multiplanar imaging and virtual bronchoscopy have made a significant impact on diagnosis and management of patients.15
MKS has been associated with other connective tissue diseases like Marfan syndrome, Ehlers–Danlos syndrome, ankylosing spondylitis and rheumatoid arthritis,16–18 the patient presented in this case had no features to suggest any of the above connective tissue disorders. Unfortunately, we were unable to perform genetic tests that would have helped us to exclude these differentials due to the limited access of these tests in our setting. The cause of proptosis in this case was not apparent. Moreover, there were no symptoms to suggest Grave’s disease.
The treatment of MKS is mainly supportive and asymptomatic patients require no specific treatments. In symptomatic patients, therapy is limited to chest physiotherapy for clearing secretion and antibiotic use in case of an infectious cause of the exacerbation.7 Tracheal stenting may be helpful in severe cases, although surgery is rarely performed because of the diffuse nature of the disease.13 Cessation of smoking and minimizing exposure to industrial and occupational irritants and pollutants is likely to be beneficial. The role of pulmonary rehabilitation is unclear in MKS. The patient in this case was managed for both the respiratory and cardiac symptoms using the medications elaborated in the case presentation. In the recent review, there was some improvement in both the cardiorespiratory symptoms and the nutrition status. The patient was also counseled regarding prognosis of his medical condition and linked to home-based palliative care services. A month later the patient was reported to have developed a severe lung infection which was managed from a peripheral health facility. Unfortunately, the patient succumbed to the infection while at home.
Limitations
We were unable to perform genetic tests for connective tissue diseases and the sweat chloride test to exclude other possible causes of tracheobronchomegaly like Marfan’s syndrome and cystic fibrosis. However, there was no family history to suggest cystic fibrosis and the physical examination was not suggestive of a connective tissue disease. The patient was unable to tolerate spirometry and hence lung function tests could not be performed. Moreover, the hypercapnia (deduced from cyanosis) and the high risk for acute respiratory failure precluded us from performing bronchoscopy. Furthermore, there was a limitation in the CT scan protocol used in which a sequential HRCT was used with only the inspiratory phase of the scan obtained.
Conclusion
Mounier Kuhn syndrome is a rare disease affecting the large airways. Presentation may be asymptomatic or present with clinical manifestations ranging from minimal symptoms with preserved lung function to severe respiratory failure. The radiological findings of Mounier Kuhn syndrome include tracheal and bronchial dilatations with diameters greater than 30mm, 20mm (right) and 18mm (left), respectively, on inspiratory phase with significant tracheal collapse on expiratory phase. MKS, although rare, should be considered as a possible diagnosis in patients presenting with productive chronic cough, recurrent pneumonia, or incomplete response to appropriate antibiotic therapy for pneumonia. Evaluation using the recent state-of-the-art MDCT protocol should be done for a more accurate diagnosis.
Data Sharing Statement
All data are provided in this manuscript.
Consent to Publish
The patient provided written informed consent for publication of personal information and images.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krustins E. M ounier‐K uhn syndrome: a systematic analysis of 128 cases published within last 25 years. Clin Respir J. 2016;10(1):3–10. doi:10.1111/crj.12192
2. Shahin S, Hoffman T, van Es W, Grutters J, Mateyo K. Congenital tracheobronchomegaly (Mounier-Kuhn syndrome) in a 28-year-old Zambian male: a case report. Pan Afr Med J. 2021;40:153.
3. Mkandawire MJ, Muramira NM, Mraba N. A curious case of cough: Mounier-Kuhn syndrome in a Namibian female patient. Pan Afr Med J. 2020;36(1). doi:10.11604/pamj.2020.36.56.23375
4. Bass E. Tracheobronchomegaly: the Mounier-Kuhn syndrome. South Afr Med J. 1974;48(8):1718–1720.
5. Woodring JH, Howard RS, Rehm SR. Congenital tracheobronchomegaly (Mounier-Kuhn syndrome): a report of 10 cases and review of the literature. J Thorac Imaging. 1991;6(2):1–10. doi:10.1097/00005382-199104000-00003
6. Menon B, Aggarwal B, Iqbal A. Mounier-Kuhn syndrome: report of 8 cases of tracheobronchomegaly with associated complications. South Med J. 2008;101(1):83–87. doi:10.1097/SMJ.0b013e31815d4259
7. Krustins E, Kravale Z, Buls A. Mounier-Kuhn syndrome or congenital tracheobronchomegaly: a literature review. Respir Med. 2013;107(12):1822–1828. doi:10.1016/j.rmed.2013.08.042
8. Katz I, Levine M, Herman P. Tracheobronchiomegaly. The Mounier-Kuhn syndrome. Am J Roentgenol Radium Ther Nucl Med. 1962;88:1084–1094.
9. Odell DD, Shah A, Gangadharan SP, et al. Airway stenting and tracheobronchoplasty improve respiratory symptoms in Mounier-Kuhn syndrome. Chest. 2011;140(4):867–873. doi:10.1378/chest.10-2010
10. Benesch M, Eber E, Pfleger A, Zach M. Recurrent lower respiratory tract infections in a 14‐year‐old boy with tracheobronchomegaly (Mounier‐Kuhn syndrome). Pediatr Pulmonol. 2000;29(6):476–479. doi:10.1002/(SICI)1099-0496(200006)29:6<476::AID-PPUL10>3.0.CO;2-R
11. Sundaram P, Joshi J. Tracheobronchomegaly associated tracheomalacia: analysis by sleep study. Indian J Chest Dis Allied Sci. 2004;46(1):47–50.
12. Sarper A, Oz N, Demircan A, Isin E. Mounier-Kuhn syndrome: case report. Turk J Thorac Cardiovasc Surg. 2002;10(2):116–117.
13. Ghanei M, Peyman M, Aslani J, Zamel N. Mounier-Kuhn syndrome: a rare cause of severe bronchial dilatation with normal pulmonary function test: a case report. Respir Med. 2007;101(8):1836–1839. doi:10.1016/j.rmed.2007.02.005
14. Dunne MG, Reiner B. CT features of tracheobronchomegaly. J Comput Assist Tomogr. 1988;12(3):388–391. doi:10.1097/00004728-198805010-00004
15. Mansour HH. Role of volumetric chest high-resolution CT in the diagnosis of Mounier-Kuhn syndrome. Clin Cases Med. 2021;1(2):1009.
16. Ayres J, Pope F, Reidy J, Clark T. Abnormalities of the lungs and thoracic cage in the Ehlers-Danlos syndrome. Thorax. 1985;40(4):300–305. doi:10.1136/thx.40.4.300
17. Celenk C, Celenk P, Selcuk M, Özyazici B, Kuru Ö. Tracheomegaly in association with rheumatoid arthritis. Eur Radiol. 2000;10(11):1792–1794. doi:10.1007/s003300000451
18. Fenlon H, Casserly I, Sant S, Breatnach E. Plain radiographs and thoracic high-resolution CT in patients with ankylosing spondylitis. AJR Am J Roentgenol. 1997;168(4):1067–1072. doi:10.2214/ajr.168.4.9124117
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.