")
Back to Journals » Research and Reports in Urology » Volume 13
Topographic Labeling of Glans Penis and Corpus Spongiosum When Planning Surgery for Distal Hypospadias
Authors Seleim HM
Received 26 February 2021
Accepted for publication 26 March 2021
Published 12 April 2021 Volume 2021:13 Pages 167—173
DOI https://doi.org/10.2147/RRU.S308451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Supplementary Video presented by Hamed M Seleim.
Views: 429
Hamed M Seleim
Pediatric Surgery and Urology, Tanta University Hospitals, Tanta, Egypt
Correspondence: Hamed M Seleim
Pediatric Surgery and Urology, Tanta University Hospitals, Tanta, P.C.: 31527, Egypt
Tel +20 1066799775
Email [email protected]
Background: Outcomes of hypospadias surgery continually lagged behind anticipations among practitioners, prompting continuing refinement of approaches. Refinements typically involved modified surgical techniques.
Objective: Herein, the author aimed for reporting the comparative anatomical topography of distal hypospadias anomaly vs normal controls, to boost its reparative approach.
Patients and Methods: This is a prospective clinical study of distal hypospadias cases presented to the author’s facility between June 2018 and June 2020. Anatomical topography of the hypospadias penis was studied concerning the corresponding marks in another control cohort with normal penile development. Meatal marks, glans wings alignment, frenulum, and corpus spongiosum were the anatomical landmarks looked into. Operative correction of the anomaly was carried out considering these landmarks, aiming for pinpoint reassembly. The control group served to identify the normal topography.
Results: The author studied 49 cases of distal hypospadias and 10 uncircumcised boys with an otherwise normal penile anatomy. In distal hypospadias, the corpus spongiosum splayed out – at about mid-penile level – ending at a consequently splayed glans penis, rather than involving a primary glans defect. After the corpus spongiosum had been closed/zippered up, no further glans wings’ surgical dissection was deemed necessary to attain the anatomical topography identified by the control group. By the end of a median follow-up period of 14 months, no urethrocutaneous fistulae or meatal stenoses were reported, with a typical apical re-assembled meatus, glans ventrum, and frenulum.
Conclusion: Topographic mapping against control subjects revealed that the glans penis is fully developed in boys with distal hypospadias. After the spongiosal plate has been adequately zippered up, no glans wings’ surgical dissection was deemed necessary to attain the typical glanular topography identified by the control group.
Keywords: distal hypospadias, anatomical topography, meatal marks, spongioplasty, the urethral plate
Introduction
Surgery for hypospadias has been evolving since the first descriptions of this anomaly with alternating eras of technical refinement and latency in evaluation.1–5 Although the procedures became labeled “the science and art of hypospadias surgery”, the outcomes always lagged behind anticipations among routine practitioners compared with pioneers, prompting continuing refinement of approaches.6,7 Refinements typically involved improving tissue handling, boosting vascularity, the use of tension-free reconstruction, and modified surgical techniques.8,9 Herein, the author aimed for reporting the comparative anatomical topography of distal hypospadias anomaly vs normal controls, to boost its reparative surgical approach.
Patients and Methods
This is a prospective clinical study of all cases presenting to the author’s facility with distal penile hypospadias, between June 2018 and June 2020. Distal penile hypospadias is defined as a hypospadias meatus located along the distal half of penile urethra, in the absence of a significant chordee (ie, a ventral curvature of more than 30°).
The topographic anatomy of the penis in the enrolled cases was studied in comparison with parallel landmarks in another cohort with normal penile development who were subjected to circumcision or other inguinoscrotal surgeries. Previous penile surgery in either group was an exclusion factor. Meatal configuration, the ventral aspect of the glans penis, the frenulum, and the corpus spongiosum were assessed (ie, detailed description of its features). Topographic labeling of these features rather than quantitative measurements was used here because penile measures change with age.
Operative correction of distal hypospadias was carried out considering the corresponding labeled landmarks, aiming for a pinpoint reassembly. The control cohort served only to identify normal topography, but not for measuring operative outcomes. The author of this report operated on the enrolled series, who were followed up after hospital discharge for at least 6 months. Outcomes evaluated included urethrocutaneous fistula, neourethral stenosis, dehiscence, or other suture line complications. Especial attention was given to assessing the configurations of the glans penis, meatus, and frenulum, after have been surgically re-assembled.
Results
During the study inclusion period, 49 cases of distal penile hypospadias and 10 uncircumcised boys were enrolled. Supplementary Video S1 comprehensibly illustrates the comparative topographic assessment of the studied cohorts and the followed spongiosal reparative approach for the hypospadias group. https://drive.google.com/file/d/1D1556lGOzkSLUx6DvlVNDsZhRB0RrL6z/view?usp=sharing
Evaluation of the Cohort with Normal Penile Development (Figure 1)
- Meatal marks. The normal glans penis is blunt with an apical sagittal slit that has a ventral extension distal to a pair of side protrusions. Thus, four points configure the orthotopic urethral meatus: a dorsal end, two side protrusions, and a ventral end. The ventral extension is located at the ventral aspect of the glans and measures up to two-thirds the distance between the dorsal end and the side protrusions.
- Ventral glans. This is the part of the glans penis located ventral to its hemispherical blunt tip. Its distal sagittal terminus is at the side protrusions of the meatus. From these protrusions, glans wings converge to meet at the ventral end of the urethral meatus, then diverge to converge with the coronal sulcus laterally.
- Frenulum. This is a web-shaped fold of the inner face of the prepuce, with a glanular and a preputial limb. Its glans limb covers the distal part of the corpus spongiosum between the divergent stubby glans wings and diminishes towards the ventral end of the meatus. Its preputial limb is the ventral midline fusion of the inner face of the prepuce, analogous to the median raphe of the outer penile skin.
- Corpus spongiosum. This comprises the ventral axis of the penis from its root in the pelvis to the ventral endpoint of the meatus, where bilateral glans wings diverge on its ventrolateral sides.
 |
Figure 1 Topographic mapping of the meatal marks and glans wings among the control cohort. The blue dotted line represents the converging alignment of the glans wings in-between the side protrusions and ventral endpoint of the meatus. The red dotted arrows represent the diverging glans wings alignments over the ventrolateral aspect of the corpus spongiosum. |
Evaluation of the Cohort with Distal Hypospadias (Figure 2)
- Corpus spongiosum. At a nearly mid-penile level, the corpus spongiosum diverged into two limbs - with an adjoining interbulbar commissure - spanning into an open glans penis where the natural ventral marks of the meatus should have been located. A sheet of hypoplastic urothelium—roofed with hypoplastic skin of the penile shaft—extended distally for varied spans beyond the bifurcation of the corpus spongiosum and gave a reference for the conventional nomenclature of distal hypospadias variants based on the hypospadias meatus location. This meatus was relatively - rather than absolutely - stenotic compared with the normal meatus and thus might have resulted in slight developmental ballooning of the unsupported V-shaped hypoplastic urothelial sheet with secondary yielding of lateralized spongiosal pillars.
- Glans penis. Though consequently splayed out secondary to splaying of the spongiosal plate, it uniformly retained all of its natural meatal marks (paired side protrusions and ventral marks), and natural glans wings recline over each ipsilateral spongiosal pillar (ie, the divergence alignment of the stubby wings over splayed out spongiosal plate).
- Bifurcation landmarks. The ventral demarcation line of the blending of ipsilateral inner- and outer face of the prepuce—predominantly on the right side—continued into the median raphe of penile skin in the territory of spongiosal bifurcation. Moreover, applying modest compression over the penile root against the pubic symphysis augmented the silhouette of the spongiosal bifurcation (Figure 3).
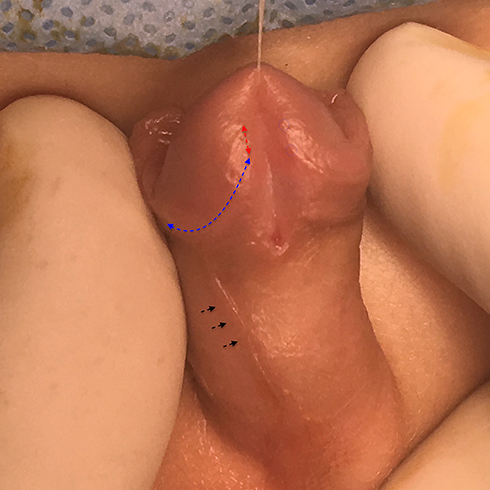 |
Figure 2 Topographic mapping of distal hypospadias case. The blue dotted circles show the retained natural meatal marks (side protrusions and ventral end-point). The red dotted line represents the proposed ventral limb of the orthotopic meatus. The blue dotted line shows the diverging alignment of the glans wings commencing at the ventral endpoint. Black arrows show the demarcation line of blending between the inner and outer face of the prepuce on the right side continuing into the median raphe of the penile skin at the territory of spongiosal bifurcation. |
 |
Figure 3 “Spongiosal plate” and “urethral plate” in distal penile hypospadias. The left photo shows the narrow glistening urothelial sheet overlying the interbulbar commissure “ie, urethral plate”. The right photo shows the augmented silhouette of the spongiosal plate from its bifurcation to its destination achieved by modest compression at the penile root. It favorably seemed not-linked to the poor condition of the “urethral plate” in both width and depth. |
Surgical Technique “Topography Guided Reassembly” (Figure 4)
With the child under general anesthesia with a caudal blockage, each was approached at lithotomy position, at the edge of the operative table A stay suture was placed at the glans tip vertically to exit at the dorsal endpoint of the meatus. Fine tipped tenotomy scissors were used for dissection, with 0.5 mm-tip bipolar forceps for hemostatic control.
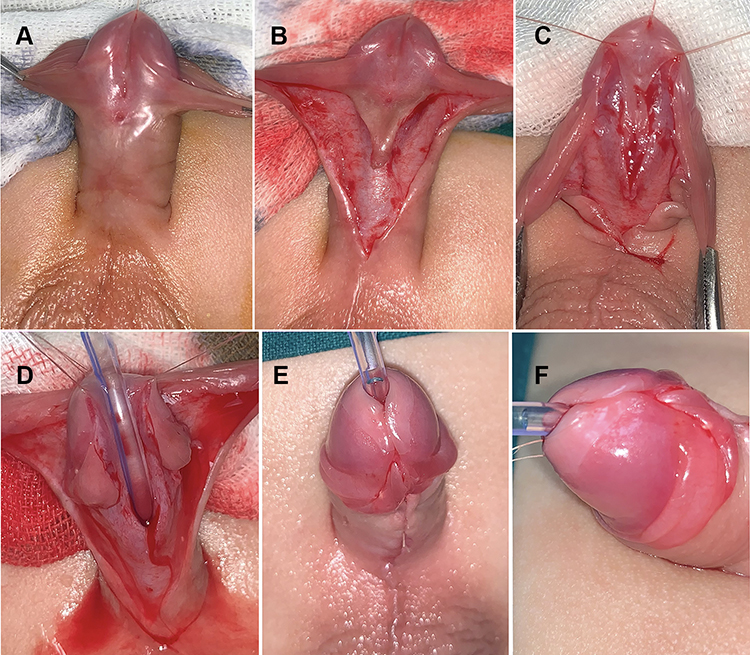 |
Figure 4 Operative technique; (A) distal penile hypospadias with a noticeable silhouette of spongiosal bifurcation, (B) median hypoplastic triangle of skin and urothelial sheet, (C) complete exposure of the edges of the spongiosal plate till the ventral meatal marks, (D) stay suture helps depict the suture line after urethral tube placement, (E) ventral glans outlook after complete spongiosal plate folding, (F) tilted view of the ventral glans shows the attainable typical topography. |
Adequate exposure of the corpus spongiosum was planned at operative dissection, from its bifurcation to its termination at the natural glanular ventral meatal marks, below the side protrusions. The ventral hypoplastic urothelial sheet was cut back from the hypospadias meatus to the spongiosal bifurcation. Three stay sutures were then used to line up the suture line: one at the spongiosal bifurcation and two where the natural ventral mark of the meatus should have been located (precisely between the converging and diverging alignments of each wing of the glans). A silicone-made urethral stent was used in the operated cases. A single-layered, interrupted, spongioplasty “zipper closure” using VicrylTM 6/0 absorbable sutures (Ethicon, Cincinnati, OH, USA) was applied for all cases. Splitting of the “urethral plate” or incorporating its sides into the suture bites was not done. After the corpus spongiosum had been closed/zippered up, no further glans wings’ surgical dissection was deemed necessary to attain the anatomical topography identified by the control group. Subdermal frenular construction (ie, glans frenulum and sub-glans mucosal collar) and penile skin closure completed the procedure. Dressings were taken off at the time of catheter removal; 5 days post-repair.
Outcomes of the Proposed Reparative Approach
During the study period, 49 boys with distal hypospadias were enrolled. The hypospadias meatus was coronal/sub-coronal in 18 boys, distal penile in 25 boys, and mid–penile in 6 boys. The mean age at correction was 1.08±0.365 (SD). The operative time was 65–90 min (mean 76 min). The early postoperative period was uneventful apart from infection and partial dehiscence of ventral skin closure in one case (Figure 5). Two other cases presented with minute urethrocutaneous fistula that healed spontaneously within 2–4 weeks, after 1–3 sets of outpatient clinic neourethral metal calibration with topical steroid ointment. After a median follow-up period of 14.2 months, no urethrocutaneous fistulae or meatal stenoses were reported.
 |
Figure 5 Early postoperative skin infection and partial dehiscence. |
Discussion
Tubularization of the urethral plate has constituted the standard surgical approach for treating distal hypospadias; either by incorporating the plate in the reconstruction of a fully epithelialized neourethra (after has been boosted with local skin flaps or grafts) or by relying solely on the plate for the reconstruction of an incompletely epithelialized neourethra, hoping for secondary healing with minimal scarring.10,11
Mobilization of the wings of the glans and closure over the tubularized plate, or even tunneling the glans to incorporate a reconstructed neourethral flap, has been considered another constituent of successful hypospadias repair. This notion might have emerged from the assumption that the distal part of the urethra - within the glans - originates during embryogenesis from canalization of a solid ectodermal ingrowth.12 This misconception might have been based on the anatomical illustrations13 depicting the glans penis as the distal continuation of the corpus spongiosum. However, there is now evidence that the entire male urethra, including its glanular part, is developed by dorsal growth of the urethral plate into the genital tubercle with a ventral fusion of the urethral folds in a proximal to distal sequence (a closing zipper); progressing to the glans tip.14,15 Moreover, the presence of a fully developed glans penis in the presented series with hypospadias emphasizes the lack of reliability of such anatomical depictions.
Surgical dissection within the glans tissue at the surgery for hypospadias has led to frequent glans scarring, meatal problems, or glans tissue loss, necessitating complex reconstructive surgeries. It has been proven that the glans epithelium demonstrated the Koebner phenomenon in response to surgical trauma, ending up with lichen sclerosus (also termed balanitis xerotica obliterans).16 Such clinical and anatomical insights into the hypospadias anomaly helped clarify its comprehension.
According to the presenting author’s belief, other than being attached to the splayed out spongiosal plate, the ontogenesis of the glans penis is not related to that of the corpus spongiosum, as the case with the female glans clitoridis. Both glandes are not the distal continuation of the corpus spongiosum as has been shown (incorrectly) in anatomical illustrations. Apart from being laid open as a consequence of the bifurcation of the corpus spongiosum, the glans penis in the presented series retained all the topographic features of a normal one: meatal marks and the convergence-divergence alignment of the stubby wings.
The presenting author argues that an interrupted mesenchymal spongiosal folding and ventral fusion is the key cause of distal hypospadias. Hence, fixing such a problem should rely on spongioplasty. The quality of endodermal urothelium overlying the interbulbar commissure “the urethral plate”—in terms of both width and depth—should not be the prime surgeon’s concern when planning surgical management, fortunately, the robust “spongiosal plate” should. The rationale behind incising the ventral hypoplastic urothelial sheet back to the point of spongiosal bifurcation was to optimize tuning with the fully developed proximal penile urethra. Such anatomical matching matters in terms of assuring a steady urinary stream in the reassembled distal penile urethra and apical meatus.
The anatomical landmarks of the external urethral meatus—namely the dorsal and ventral endpoints—have been addressed in former reports relating to boys with distal hypospadias.17,18 The divergence of corpus spongiosum is a well–described anatomic feature of the anomaly, further.9,15,19–21 Herein, the presenting author analyzed the topographic mapping of the meatal marks with the layout of the bifurcated spongiosal plate, the alignment of the splayed-out glans wings, and the natural marks of the prepuce. Study results revealed that the robust “spongiosal plate” is favorably not relevant to the characteristics of the glistening urothelial coverage of its interbulbar commissure “urethral plate” (Figure 3). Such a deliberate topographic analysis of every single component of the anomaly has guided to put forward a seemingly simple, yet comprehensive, reconstructive approach.
The enrolled series was managed in the light of the aforementioned concerns, anticipating possible endoluminal urothelial “creeping” within the newly folded spongiosal plate. The case with post-operative ventral skin dehiscence could have arisen from mingling the hypoplastic skin triangle covering the bifurcation territory into the suture line, an issue that was addressed later in this work. None of the approached cases presented with glans dehiscence; suturing of a robust spongiosal plate with preserved integrity (absence of mid-line or side incisions of the spongiosal plate solidity) and intimate relationship with its overlying stubby wings could have been a plausible explanation.
Study Limitations
Apparent limitations of the current study are the small series, single surgeon outcomes, and short-term evaluation.
Conclusions
Topographic mapping against control subjects revealed that the glans penis is fully developed in boys with distal hypospadias. The corpus spongiosum splayed out at a mid-penile level, ending into a consequently splayed glans penis, rather than having a primary glans defect. After the spongiosal plate has been adequately zippered up, no glans wings’ surgical dissection was deemed necessary to attain the aimed normal glanular topography identified by the control group. Nevertheless, further extended comparative studies are needed to verify the long-term outcomes of the proposed approach.
Research Ethics Committee Approval
FWA00022834 - IRP0010038 - Approval code: 34193/10/20.
Ethical Considerations
The protocol for the research project has been approved by Ethics Committee of the institution within which the work was undertaken and it conforms to the provisions of the Declaration of Helsinki in 1995 (as revised in Edinburgh 2000). Informed parental consent was obtained for all participants in this research. Privacy and confidentiality of data were granted.
Disclosure
The author of this report has no conflict of interest or financial ties to disclose.
References
1. Snodgrass W. Tubularized incised plate urethroplasty for distal hypospadias. J Urol. 1994;151:464–465. doi:10.1016/S0022-5347(17)34991-1
2. Asopa HS, Elhence IP, Atri SP, et al. One stage correction of penile hypospadias using a foreskin tube: a preliminary report. Int Surg. 1971;55:435–440.
3. Duckett JW. Transverse preputial island flap technique for repair of severe hypospadias. Urol Clin North Am. 1980;7:423–430.
4. Koyanagi T, Nonomura K, Yamashita T, et al. One-stage repair of hypospadias: is there no simple method universally applicable to all types of hypospadias? J Urol. 1994;152:1232–1237. doi:10.1016/S0022-5347(17)32556-9
5. Bracka A. A versatile two-stage hypospadias repair. Br J Plast Surg. 1995;48:345–352. doi:10.1016/S0007-1226(95)90023-3
6. Braga LH, Pippi Salle JL, Lorenzo AJ, et al. Comparative analysis of tubularized incised plate versus onlay island flap urethroplasty for penoscrotal hypospadias. J Urol. 2007;178:1451–1457. doi:10.1016/j.juro.2007.05.170
7. Eliçevik M, Tireli G, Demirali O, et al. Tubularized incised plate urethroplasty for hypospadias reoperations in 100 patients. Int Urol Nephrol. 2007;39:823–827. doi:10.1007/s11255-006-9145-y
8. Kureel SN, Gupta A, Sunil K, et al. Surgical anatomy of the penis in hypospadias: magnetic resonance imaging study of the tissue planes, vessels, and collaterals. J Urol. 2015;85:1173–1178. doi:10.1016/j.urology.2015.02.017
9. Yerkes EB, Adams MC, Miller DA, et al. Y-to-I wrap: use of the distal spongiosum for hypospadias repair. J Urol. 2000;163:1536–1538. doi:10.1016/S0022-5347(05)67673-2
10. Hadidi AT. History of hypospadias: lost in translation. J Ped Surg. 2017;52:211–217. doi:10.1016/j.jpedsurg.2016.11.004
11. Seleim HM, El Sheemy MS, Abdalazeem Y, et al. Comprehensive evaluation of grafting the preservable narrow plates with consideration of native plate width at primary hypospadias surgery. J Ped Urol. 2019;15:345–351. doi:10.1016/j.jpurol.2019.05.002
12. van der Werff JF, Nievelstein RA, Brands E, et al. Normal development of the male anterior urethra. Teratology. 2000;61:172–183. doi:10.1002/(SICI)1096-9926(200003)61:3<172::AID-TERA4>3.0.CO;2-B
13. Moore K, Agur A, Dalley A. Clinically Oriented Anatomy, 8th Ed, Pelvis and Perineum. Baltimore, MD: Lippincott Williams and Wilkins; 2018:646–655.
14. Baskin LS, Ebbers MB. Hypospadias: anatomy, etiology, and technique. J Ped Surg. 2006;41:463–472. doi:10.1016/j.jpedsurg.2005.11.059
15. Ramazan K, Zeynep K. Embryology of corpus spongiosum and glans penis in hypospadias. Plast Reconstr Surg. 2000;105(2):813. doi:10.1097/00006534-200002000-00081
16. Bunker CB, Shim TN. Male genital lichen sclerosus. Indian J Dermatol. 2015;60:111–117. doi:10.4103/0019-5154.152501
17. Hutton KA, Babu R. Normal anatomy of the external urethral meatus in boys: implications for hypospadias repair. BJU Int. 2007;100:161–163. doi:10.1111/j.1464-410X.2007.06798.x
18. Babu R. Glans meatus proportion in hypospadias versus normal: does marking reference points impact outcome? J Pediatr Urol. 2014;10:459–462. doi:10.1016/j.jpurol.2013.11.008
19. Bao X, Huang Y, Lyu Y, et al. A histomorphological study of the divergent corpus spongiosum surrounding the urethral plate in hypospadias. Urology. 2020;144:188–193. doi:10.1016/j.urology.2020.04.139
20. Horton CE, Sadove RC, Devine CJ. Reconstruction of male genital defects: congenital. In: McCarthy JG, editor. Plastic Surgery. Vol. 6. Philadelphia: Saunders; 1990:4153.
21. Zhang B, Bi YL, Ruan SS. Application and efficacy of reconstructing forked corpus spongiosum in distal/midshaft hypospadias repair. Asian J Androl. 2021;23:47–51. doi:10.4103/aja.aja_42_20
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.