")
Back to Journals » Clinical Ophthalmology » Volume 14
Topical Difluprednate for Early Corneal Graft Rejection After Penetrating Keratoplasty
Authors Said OM , Saleh MGA , Omar AF , Abdou AA , Riad Mostafa AN
Received 25 June 2020
Accepted for publication 1 September 2020
Published 27 October 2020 Volume 2020:14 Pages 3495—3498
DOI https://doi.org/10.2147/OPTH.S267888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Omar M Said,1 Mohamed GA Saleh,2 Ahmed F Omar,2,3 Ahmed A Abdou,2 Ali Natag Riad Mostafa2
1Department of Ophthalmology, Faculty of Medicine, Fayoum University, Fayoum, Egypt; 2Department of Ophthalmology, Faculty of Medicine, Assiut University, Assiut, Egypt; 3University Hospitals Eye Institute and the Department of Ophthalmology and Visual Sciences, Case Western Reserve University School of Medicine, Cleveland, OH, USA
Correspondence: Ahmed F Omar Tel +1 216 844-7230
Email [email protected]
Purpose: To evaluate the safety and efficacy of topical difluprednate ophthalmic emulsion use for prophylaxis of corneal graft rejection in patients undergoing penetrating keratoplasty.
Methods: This study reviewed the charts of patients undergoing penetrating keratoplasty who were treated with difluprednate (DP) ophthalmic emulsion postoperatively. At each follow-up visit, patients were followed for signs of graft rejection, cataract development, and intraocular pressure rise in addition to routine ocular examination.
Results: The charts of 36 patients (38 eyes) who underwent penetrating keratoplasty (PKP) (27 eyes) and PKP triple (11 eyes) were reviewed. All eyes were followed up for at least 8 months postoperatively. Five grafts developed rejection and three grafts subsequently failed. Six eyes had an increase of IOP that required use of antiglaucoma drops. Three eyes were switched from difluprednate to prednisolone acetate (PA) after persistent rise of IOP failed to respond to antiglaucoma drops. None of these cases needed glaucoma surgery. Two patients developed cataract during the follow-up period (out of 12 phakic eyes).
Conclusion: Topical difluprednate is potentially effective and safe in preventing graft rejection after penetrating keratoplasty. Larger prospective clinical trials are warranted.
Keywords: difluprednate, penetrating keratoplasty, graft rejection
Introduction
Penetrating keratoplasty (PKP) is a widely practiced procedure. Rejection of the transplanted cornea by the immune system is an important mechanism of graft failure postoperatively. Corneal graft rejection follows a sequence of immune responses that starts with the recognition of the foreign antigens of the graft by the host’s immune system, triggering the immune response cascade. This immunological process may induce damage to the grafted cornea, that could be reversed if recognized and treated early.1,2
Epithelial rejection, chronic stromal rejection, hyperacute rejection, and endothelial rejection are the different types of corneal graft rejection that might occur in isolation or in combination.
Early detection and aggressive corticosteroids therapy are the keys to successful management of corneal graft rejection. Addition of immunosuppressive to the treatment regimen helps in quick and long-term recovery.3
Topical corticosteroids are used as a routine postoperative treatment after PKP for their good ocular penetration and potent immunomodulatory action. Treatment regimen varies depending on the risk of rejection, lens status, and risk of IOP elevation. Prednisolone is the preferred treatment by most surgeons. Other commonly used preparations include dexamethasone, loteprednol, and fluorometholone.4
Difluprednate (difluoroprednisolone butyrate acetate) is a difluorinated prednisolone derivative. Originally developed for dermatologic applications, it was later formulated as a 0.05% ophthalmic emulsion that has a greater potency and superior tissue penetration than other topical ophthalmic preparations. Difluprednate has shown promising success in management of postoperative inflammation and even in cases of refractory uveitis and uveitic macular edema.5
Methods
This is a chart review of patients who underwent PKP at the departments of Ophthalmology, Assiut University hospital and Fayoum University hospital between August 2016 and April 2019.
The study was conducted according to ethical tenets of the Declaration of Helsinki and after obtaining approval of the IRB of the Faculty of Medicine, Assiut and Fayoum Universities.
Charts of patients who underwent PKP and completed follow-up on scheduled visits on the first postoperative day, week 1, month 1, and monthly thereafter were reviewed.
Inclusion criteria were age above 18 years, no other ocular pathology apart from corneal pathology and cataract, and compliance with medication regimen and follow-up.
Exclusion criteria included cases of corneal regrafting, and failure to complete the follow-up visits.
Data collected included demographic data, initial diagnosis, other ocular and systemic co-morbidities, date and detailed operative notes of surgery, and postoperative follow-up notes including initial postoperative medications and complications, eg, first date of noticing early rejection signs, anterior and posterior segment examination findings and relevant investigations, if done (eg, B scan ultrasonography, corneal endothelium count and pachymetry).
IOP measurements before and after surgery at different follow-up visits were also noted. IOP was measured using Goldmann applanation tonometer. Patients were seen at day 1, day 7, and day 14 after surgery. Subsequent visits timing and frequency were determined according to the finding observed during initial follow-up. Patients were given instructions to use the postoperative medication regimen including DP eye drops 4-times daily for the first 2 weeks. Subsequently, dose was adjusted according to the observed degree of inflammation and IOP. In addition, patients received topical antibiotic eye drops (moxifloxacin). Systemic steroids were not used on a routine basis.
Data was recorded as excel spread sheets and statistical analysis was performed using SPSS program (version 21; International Business Machines Co, Armonk, NY).
Results
Baseline characteristics of the study subjects are shown in Table 1.
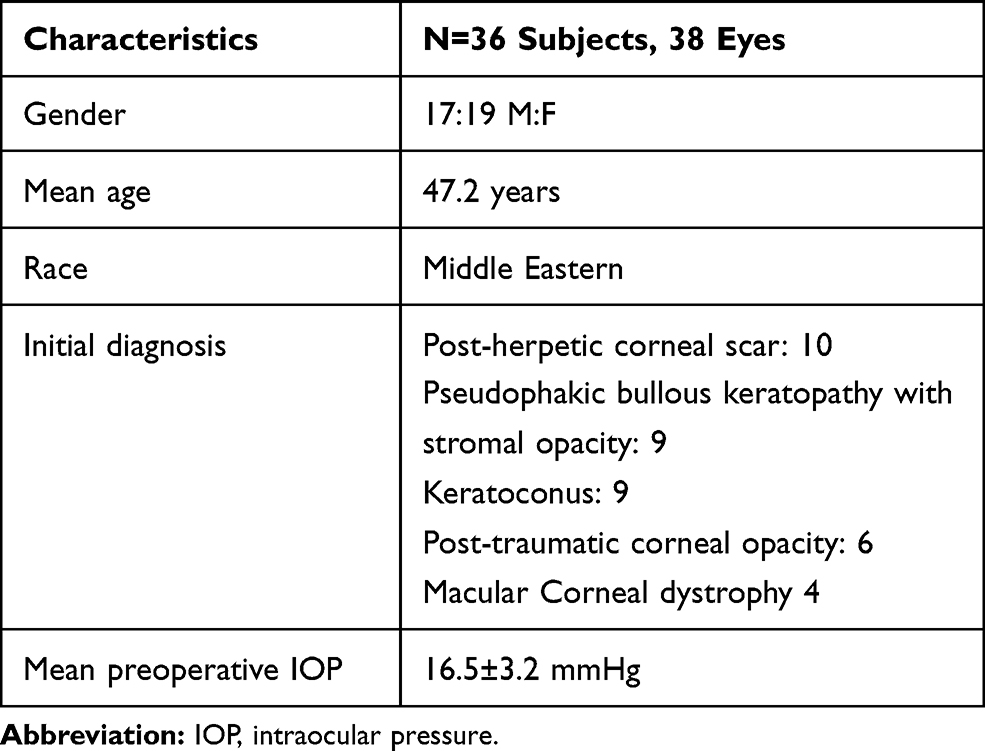 |
Table 1 Baseline Characteristics of Study Subjects |
Thirty-eight eyes from 36 patients were included in the study. Twenty-seven eyes underwent PKP, while PKP triple (PKP, cataract extraction, and intraocular lens implantation) was done for the other 11 eyes. Of the 27 eyes that underwent PKP only, 12 eyes were phakic (with clear crystalline lens). Mean follow-up duration was 326 days (range=163–496 days).
Graft rejection occurred in five eyes, and three of those eyes developed subsequent graft failure. Graft rejection was defined as an endothelial rejection line present in a graft that was previously clear or when there was inflammation (stromal infiltrate, keratic precipitates, cells in the anterior chamber, or ciliary injection) without an endothelial rejection line.
Graft failure was defined as non-resolving corneal edema (corneal edema persisting after antirejection treatment), loss of central graft clarity sufficient to compromise vision, or the need for a re-graft. The average timing of graft rejection was 8 months, while three of these grafts failed.
Six eyes developed IOP elevation (16%), defined as IOP above 21 mmHg or a rise of 10 mmHg or more from baseline (IOP before surgery), for which they were treated by topical IOP lowering medications (beta blockers and topical carbonic anhydrase inhibitors); none needed surgery to lower IOP. Three of those patients were shifted to prednisolone acetate to control IOP.
Two patients developed cataract during the follow-up period, out of 12 phakic eyes.
Discussion
Worldwide, corneal transplantation is one of the most commonly performed transplantation procedures. The graft survival rate diminishes with time after surgery. Immune rejection accounts for more than 50% of graft failure cases.
Treatment with topical corticosteroids after keratoplasty has been the mainstay treatment to minimize postoperative inflammatory reaction.6
In June 2008 difluprednate ophthalmic emulsion 0.05% (Durezol™; Sirion Therapeutics, Tampa, FL) was approved by the US Food and Drug Administration (FDA) for the treatment of inflammation and pain associated with ocular surgery – the first strong ophthalmic steroid approved by the FDA since 1973.5
In the present study, we showed that difluprednate (DP) was able to control inflammation in patients who showed signs of early graft rejection. Traditionally, topical PA 1% is the drug of choice for prevention and treatment of corneal graft rejection.7 For high risk grafts, surgeons tend to increase the frequency and extend the duration of prednisolone use. A useful advantage of DP is the requirement of less frequent dosing due to higher potency and also it does not need to be shaken before use (because it is an emulsion rather than a suspension), thus improving patient’s compliance.8
Surgeons’ preference regarding choice of steroid type and regimen used after PKP depends on the risk of graft rejection. For low risk grafts, surgeons use loteprednol, dexamethasone, or prednisolone. For high risk grafts, some surgeons increase the intensity and duration of treatment and rarely use loteprednol.4 Since its introduction, the use of DP after PKP, on an anecdotal base, is on the rise.9
Our series is, to our knowledge, the first to describe results of DP use after PKP.
A Multicenter Randomized Controlled Fellow Eye Trial showed that DP was superior to PA in multiple end points after cataract surgery. The authors reported better UCVA and BCVA at 1 day after cataract surgery, reduced macular swelling at 2 and 4 weeks after surgery, and reduced endothelial cell loss at 4 weeks after surgery in eyes treated with DP. Those results are mostly attributed to the greater anti-inflammatory potency of DP compared to prednisolone acetate (PA)5.
In a series by Pedersen et al,10 15% of the PK-treated eyes and 4% of the DSAEK-treated eyes experienced rejection. Graft failure occurred in 8% of the PK-treated eyes and in 7% of the DSAEK-treated eyes.
Also, the rate of IOP rise was 16% and all of those cases were controlled by IOP lowering eye drops (beta blockers and topical carbonic anhydrase inhibitors). None of those eventually required filtration surgery. The incidence of a significant postoperative IOP rise in eyes treated with DP varies significantly in different series. Donnenfeld et al5 reported an incidence of 3–6%. On the other hand, Jeng et al11 reported a much higher likelihood of IOP rise with DP use (35%) following vitreoretinal surgery. Those variations might be explained by the different nature of the surgical procedure involved and the variable pathology already present in those eyes and partly by ethnic differences among different study populations.
In our study two eyes receiving topical DP developed a posterior subcapsular cataract, out of 12 phakic eyes (16.7%).
Topical corticosteroid treatment following PKP is one of the factors that might contribute to lens opacification. A study on patients who had PKP reported that 45 (24.45%) developed cataract. Most cataracts (n=31) developed within the first year of surgery.12
The association between cataract development and use of topical PA was studied more than the association with DP. Topical PA was shown to be significantly associated with development of cataract in children with chronic uveitis due to juvenile idiopathic arthritis in a dose dependent manner.13 Data regarding the risk of cataract development associated with DP use is sparse in the literature. Most papers reported the use of DP after cataract surgery. However, because DP is more potent than PA and its penetration into the AC is greater, it is prudent that it might be more cataractogenic than PA at least theoretically.
In conclusion, topical DP is shown to be non-inferior to conventionally used PA regarding effectiveness and safety for preventing graft rejection after penetrating keratoplasty.
Larger controlled clinical trials with a longer follow-up duration are warranted in the future to further refine the evidence of difluprednate use after PKP.
Ethical Consideration
All patient data accessed complied with relevant data protection and privacy regulations.
The abstract of this paper was presented at the ASCRS annual meeting, May 2019, as a conference talk with interim findings.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Panda A, Vanathi M, Kumar A, Dash Y, Priya S. Corneal graft rejection. Surv Ophthalmol. 2007;52(4):375–396. doi:10.1016/j.survophthal.2007.04.008
2. Coster DJ, Williams KA. The impact of corneal allograft rejection on the long-term outcome of corneal transplantation. Am J Ophthalmol. 2005;140(6):1112–1122. doi:10.1016/j.ajo.2005.07.024
3. Alldredge OC, Krachmer JH. Clinical types of corneal transplant rejection: their manifestations, frequency, preoperative correlates, and treatment. Arch Ophthalmol. 1981;99(4):599–604. doi:10.1001/archopht.1981.03930010599002
4. Randleman JB, Stulting RD. Prevention and treatment of corneal graft rejection: current practice patterns (2004). Cornea. 2006;25(3):286–290
5. Donnenfeld ED, Holland EJ, Solomon KD, et al. A multicenter randomized controlled fellow eye trial of pulse-dosed difluprednate 0.05% versus prednisolone acetate 1% in cataract surgery. Am J Ophthalmol. 2011;152(4):609–17.e1. doi:10.1016/j.ajo.2011.03.018
6. Ross AH, Jones MN, Nguyen DQ, et al. Long-term topical steroid treatment after penetrating keratoplasty in patients with pseudophakic bullous keratopathy. Ophthalmology. 2009;116(12):2369–2372. doi:10.1016/j.ophtha.2009.06.006
7. Tabbara KF. Pharmacologic strategies in the prevention and treatment of corneal transplant rejection. Int Ophthalmol. 2008;28(3):223–232. doi:10.1007/s10792-007-9100-7
8. Stringer W, Bryant R. Dose uniformity of topical corticosteroid preparations: difluprednate ophthalmic emulsion 0.05% versus branded and generic prednisolone acetate ophthalmic suspension 1%. Clin Ophthalmol. 2010;4:1119. doi:10.2147/OPTH.S12441
9. Jamal KN, Callanan DG. The role of difluprednate ophthalmic emulsion in clinical practice. Clin Ophthalmol. 2009;3:381–390.
10. Pedersen IB, Ivarsen A, Hjortdal J. Graft rejection and failure following endothelial keratoplasty (DSAEK) and penetrating keratoplasty for secondary endothelial failure. Acta Ophthalmol. 2015;93(2):172–177. doi:10.1111/aos.12518
11 Jeng KW, Fine HF, Wheatley HM, Roth D, Connors DB, Prenner JL. Incidence of steroid-induced ocular hypertension after vitreoretinal surgery with difluprednate versus prednisolone acetate. Retina (Philadelphia, Pa). 2014;34(10):1990–1996. doi:10.1097/IAE.0000000000000215
12. Rathi VM, Krishnamachary M, Gupta S. Cataract formation after penetrating keratoplasty. J Cataract Refract Surg. 1997;23(4):562–564. doi:10.1016/S0886-3350(97)80214-3
13. Thorne JE, Woreta FA, Dunn JP, et al. Risk of cataract development among children with juvenile idiopathic arthritis-related uveitis treated with topical corticosteroids.. Ophthalmology. 2020;127(4):S21–S26. doi:10.1016/j.ophtha.2020.01.036
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.