")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Tolerance and Efficacy of a Dermocosmetic Containing Neurosensine® in Subjects with Eyelid Eczema
Authors Tan J , Demessant A , Le Dantec G , Le Floc'h C , Kerob D
Received 11 October 2022
Accepted for publication 10 January 2023
Published 20 January 2023 Volume 2023:16 Pages 161—165
DOI https://doi.org/10.2147/CCID.S391890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anne-Claire Fougerousse
Jerry Tan,1 Ann’Laure Demessant,2 Guénaelle Le Dantec,2 Caroline Le Floc’h,2 Delphine Kerob2
1Department of Medicine and Windsor Clinical Research Inc, Western University, Windsor, ON, Canada; 2International Scientific Affairs, La Roche-Posay Laboratoire Dermatologique, Levallois-Perret, France
Correspondence: Jerry Tan, Western University, Department of Medicine and Windsor Clinical Research Inc, 300-2224 Walker Road, Windsor, ON, N8W 5L7, Canada, Tel +8615199719542, Email [email protected]
Background: Eyelid eczema (EE) is frequently observed in patients with an allergic or atopic diathesis. As for atopic eczema, restoring the skin barrier of the periocular region together with relieving clinical signs and symptoms is important in the management of EE. This study assessed the benefit and tolerance of a dedicated dermocosmetic (DC) in subjects with EE.
Materials and Methods: Open-label study in adults with EE and sensitive skin. The DC was applied twice daily for 28 days. Dermatological signs (eczema, desquamation/dryness, erythema, swelling, roughness) and symptoms (itching, prickling, heat/burning sensation, tightness) on the periorbital region, as well as ophthalmological evaluation were assessed at Day 0, 14 and 28. Subjects assessed quality of life (QOL) using DLQI, the perceived benefit and cosmetic acceptability of the DC.
Results: Overall, 41 subjects were included; 59% were women. The mean age was 52.4± 15.8 years; all subjects had periorbital sensitive skin. The DC immediately reduced the intensity of itching, prickling, heat/burning sensation and tightness. Clinical signs and symptoms had all significantly (p< 0.001) improved by Day 14 and were sustained to Day 28. The DC significantly (p< 0.001) improved the perception of irritation (73%) and swelling (66%) while soothing (59%) the periorbital skin regions at Day 28. QOL had improved at Day 28 (0.82± 1.0) compared to Day 0 (4.17± 2.23). No local adverse reactions were reported. Ophthalmological examinations paralleled the excellent dermatological tolerance of DC.
Discussion: The tested DC is highly efficacious in reducing clinical signs and symptoms of eyelid eczema and was well tolerated.
ClinicalTrials.gov Identifier: NCT05540496.
Keywords: eyelid eczema, dermocosmetic, sensitive skin, periorbital skin
Introduction
Eyelid eczema (EE) is clinically and therapeutically clearly delineated but remains a heterogeneous entity.1–3 In addition to frequent resistance to therapy and a tendency to relapse, its diagnostic is difficult and treatment challenging to dermatologists and ophthalmologists.4
Its aetiology may have different origins. It can be associated with atopic dermatitis, or due to contact dermatitis. Allergens commonly triggering eyelid eczema comprise fragrances, metals, neomycin, oleamidopropyl dimethylamine, tosylamide formaldehyde resin, benzalkonium chloride, and other preservatives.3,5 Moreover, topical ophthalmic treatments may cause EE as well.6
The tested dermocosmetic (Toleriane® Dermallergo Eye Cream, La Roche-Posay Laboratoire Dermatologique, France; hereafter DC) has been specifically developed to restore the skin barrier of the periocular region and to provide relief from signs and symptoms of EE. The DC contains niacinamide, fractions of the probiotic Sphingobioma and a soothing compound (Neurosensine®, La Roche-Posay Laboratoire Dermatologique) that acts on skin sensitivity in decreasing erythema, irritation, and pruritus, all frequently observed in periorbital eczema.7,8
This study assessed the local tolerance and efficacy of a novel DC in subjects with EE.
Patients and Methods
This open-label, observational and exploratory study was conducted at one investigational site at Batumi, Georgia. According to local regulatory guidelines of Georgia, this type of trial testing marketed cosmetics does not require approval from local ethics committees. However, the local ethics committee of Batumi, Georgia, was informed about this study. The study respected the principles of the Declaration of Helsinki and has received the Clinical Trial Identifier Number NCT05540496. Subjects meeting recruitment criteria were recruited at the investigational site upon invitation to participate in this study and provided written informed consent. The study was performed under ophthalmological and dermatological control in adult female or male subjects of any age with EE ground (blepharitis, epiphora, chronic whimpering/watery eyes) and sensitive skin. Sensitive skin was defined as a condition of subjective cutaneous hyper-reactivity to environmental factors or exposome.9
Dermatological signs (desquamation/dryness, eczema, erythema, palpebral swelling, roughness on a scale from 0=non to 5=very severe) and symptoms (itching, prickling, heat/burning sensation, tightness on a visual analogue scale (VAS) from 0=none to 5=very severe) in the periorbital region, ophthalmological signs and symptoms as well as tear film breakup time and colorimetric examination of the cornea and conjunctiva were assessed at Day 0, 14 and 28. Subjects’ quality of life (QoL) was assessed using DLQI, and the efficacy and cosmetic acceptability of the DC was self-assessed by patients on a scale from 0=not satisfied at all to 5=very satisfied.10
The DC was applied twice daily for 28 days. Usual skin care was allowed. The use of eye makeup, pharmacological treatments on eyelids and ophthalmological surgery was prohibited during the study.
Results
Overall, 41 subjects were included; 59% were women. The mean age was 52.4±15.8 years; all subjects had periorbital sensitive skin. A total of 37% of the subjects had mixed, 34% dry and 29% normal periorbital skin.
The DC had an immediate effect 10 minutes after the first application in reducing the intensity of itching, prickling, tightness and burning sensation with an average decrease of one point on a 5-point scale. Clinical signs (Figure 1) as evaluated by dermatologists and symptoms (Figure 2) assessed by subjects had all significantly (p<0.05) improved on Day 14 and were sustained to Day 28.
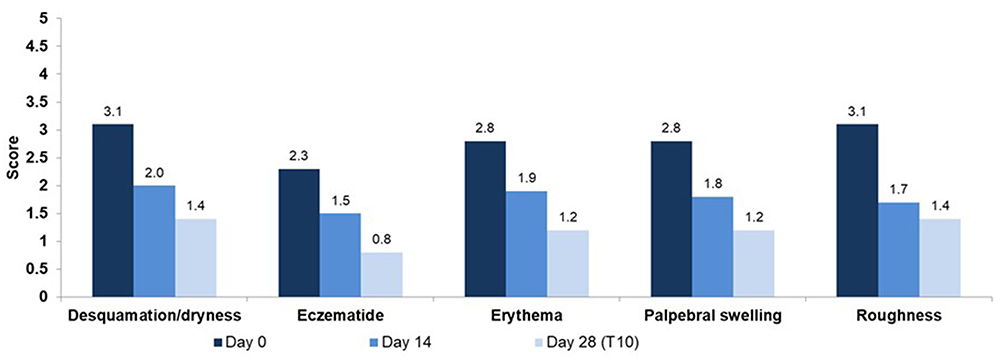 |
Figure 1 Clinical signs as assessed by the dermatologists at Day 0, Day 14, and Day 28 (T10). All clinical signs had significantly (p<0.05) improved after 14 days and 28 days of daily use. |
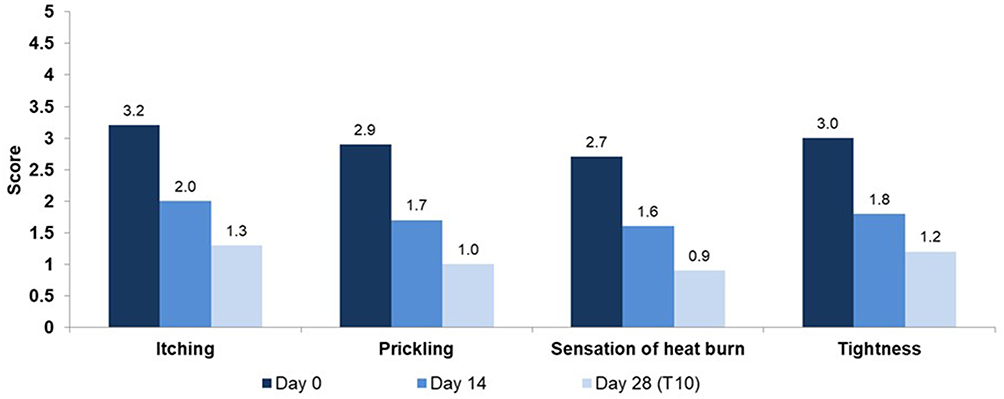 |
Figure 2 Subject reported symptoms at Day 0, Day 14, and Day 28 (T0). All subject-reported symptoms of palpebral eczema had significantly (p<0.05) improved at Day 14 and Day 28 (T10). |
At Day 28 (T10), the percentage of subjects with desquamation at Day 0 had decreased to 46%, that with eczema to 18%, that with erythema to 51%, that with palpebral swelling to 59% and that with roughness to 13%. In parallel, at Day 28, the percentage of subjects reporting itching at Day 0 decreased to 64%, that of prickling to 26%, that of heat/burn sensation to 18 and that of tightness to 23%.
According to the subjects, the DC significantly improved (p<0.05) the perception of irritation (73%) and swelling (66%) and had soothed (59%) the periorbital skin regions at Day 28 (Figure 3).
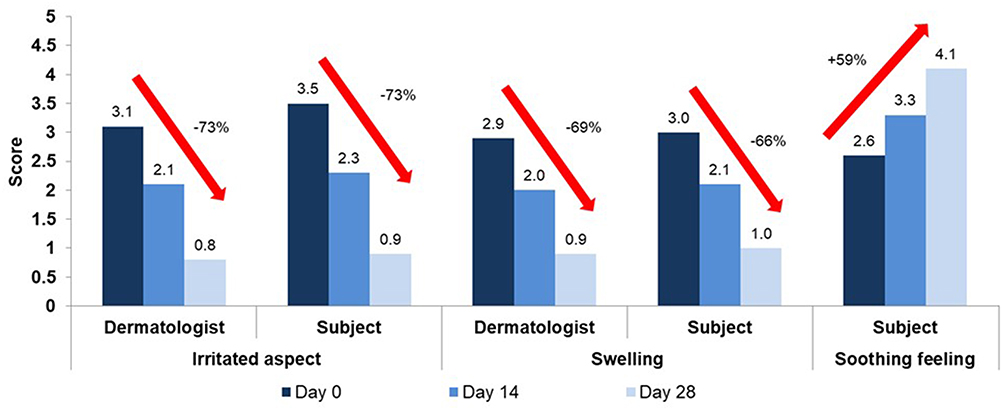 |
Figure 3 Perception of the irritated, swelling, and soothed aspect of the eye contours at Day 0, Day 14 and Day 28. The eye contour had significantly (p<0.0001) improved according to the dermatologists and the subjects. Moreover, subjects reported a significantly (p<0.0001) improved soothed eye contour. |
QOL had strongly improved at Day 28 (0.82±1.0) compared to Day 0 (4.17±2.23).
No local adverse reactions considered related to the DC were reported. Ophthalmological examinations paralleled the excellent dermatological tolerance of the DC with no ophthalmological side effects.
Discussion
Results from the present study show that the tested DC reduces clinical signs and symptoms of EE.
For both dermatologists and patients, the irritated aspect and swelling of the eye contours had significantly (p<0.0001) reduced after 14 days while the soothing feeling of the eye contours had strongly increased.
The periorbital skin is particularly sensitive and thus requires specific attention. Inappropriate cosmetic products, fragrances containing allergens may worsen EE leading to a painful and difficult to treat condition.11–13 Topical corticosteroids are the mainstay for treatment of eczema. However, when used frequently or for longer periods, corticosteroids may induce local skin or even ocular adverse events.14 For these reasons, the use of specifically developed periorbital dermocosmetics that maintain or restore the natural skin barrier while also reducing potentially present clinical signs or symptoms of EE is interesting either as a monotherapy or as an adjunct to topical drugs to maintain their benefit.15,16 These products must present with specific qualities, should not contain any known allergens, must be very well tolerated and not cause any side effects which may further alter the damaged skin barrier.
The presently tested DC was beneficial and did not cause any dermatological or ophthalmological side effects and thus meeting all requirements for a periorbital DC.
Moreover, subjects easily accepted the product and were pleased with its use, texture and benefit resulting a remarkable improvement in their quality of life. These observations should not be neglected as compliance of use goes along with an increased benefit resulting in an improved quality of life.
While this exploratory study was not double-blinded and conducted in a small number of subjects, it nevertheless confirms that a specifically developed DC provides a substantial benefit in EE, thus potentially limiting the use of pharmacological active treatments such as topical corticosteroids over a prolonged period. Additionally, we acknowledge that 18% of the participants were not completely cleared from their periorbital eczema at the end of study period and may require pharmacological treatment.
In conclusion, the tested DC is beneficial in the clinical management of eyelid eczema.
Data Sharing Statement
Jerry Tan, the corresponding author will share upon reasonable request for 1 year after publication of this manuscript the study protocol and all data collected and statistically analysed and in relationship with this study, except deidentified participant data.
Ethical Statement
According to local regulatory guidelines, this type of trial testing marketed cosmetics does not require approval from local ethics committees. However, the local ethics committee of Batumi, Georgia, was informed about this study and subjects provided written informed consent prior to participation. The study complied with the principles of the Declaration of Helsinki.
Acknowledgments
The authors acknowledge the investigators Tamar Aroshidze and Nino Tsikvadze, the project manager Meryem Nili – Dermtech and the writing support of Karl Patrick Göritz, SMWS, France.
Disclosure
AD, GLD, ClF and DK are employees of La Roche-Posay Laboratoire Dermatologique. JT reports personal fees from La Roche-Posay Laboratoire Dermatologique, Laboratoire Vichy and CeraVe, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Feser A, Mahler V. Periorbital dermatitis: causes, differential diagnoses and therapy. J Dtsch Dermatol Ges. 2010;8(3):159–166.
2. Wolf R, Orion E, Tüzün Y. Periorbital (eyelid) dermatides. Clin Dermatol. 2014;32(1):131–140. doi:10.1016/j.clindermatol.2013.05.035
3. Zirwas MJ. Contact dermatitis to cosmetics. Clin Rev Allergy Immunol. 2019;56(1):119–128. doi:10.1007/s12016-018-8717-9
4. Wollenberg A, Kerschenlohr K, Pavicic T, Messmer EM. Diagnostik und Therapie des Lidekzems: eine interdisziplinäre Herausforderung [Diagnosis and treatment of eyelid eczema. An interdisciplinary challenge]. Hautarzt. 2004;55(7):677–87; quiz 88. German. doi:10.1007/s00105-004-0759-7
5. Amin KA, Belsito DV. The aetiology of eyelid dermatitis: a 10-year retrospective analysis. Contact Dermatitis. 2006;55(5):280–285. doi:10.1111/j.1600-0536.2006.00927.x
6. Gilissen L, De Decker L, Hulshagen T, Goossens A. Allergic contact dermatitis caused by topical ophthalmic medications: keep an eye on it! Contact Dermatitis. 2019;80(5):291–297. doi:10.1111/cod.13209
7. Boo YC. Mechanistic basis and clinical evidence for the applications of nicotinamide (Niacinamide) to control skin aging and pigmentation. Antioxidants. 2021;10(8):1315. doi:10.3390/antiox10081315
8. Ferreira MS, Sousa Lobo JM, Almeida IF. Sensitive skin: active ingredients on the spotlight. Int J Cosmet Sci. 2022;44(1):56–73. doi:10.1111/ics.12754
9. Berardesca E, Farage M, Maibach H. Sensitive skin: an overview. Int J Cosmet Sci. 2013;35(1):2–8. doi:10.1111/j.1468-2494.2012.00754.x
10. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
11. Worm M, Sterry W. Periorbitale Kontaktekzeme [Periorbital contact eczema]. Klin Monbl Augenheilkd. 2005;222(11):853–855. German. doi:10.1055/s-2005-858796
12. Feser A, Plaza T, Vogelgsang L, Mahler V. Periorbital dermatitis-a recalcitrant disease: causes and differential diagnoses. Br J Dermatol. 2008;159(4):858–863. doi:10.1111/j.1365-2133.2008.08790.x
13. Scheinman PL. Allergic contact dermatitis to fragrance: a review. Am J Contact Dermat. 1996;7(2):65–76.
14. Beltrani VS, Barsanti FA, Bielory L. Effects of glucocorticosteroids on the skin and eye. Immunol Allergy Clin North Am. 2005;25(3):557–580. doi:10.1016/j.iac.2005.05.006
15. Seite S, Flores GE, Henley JB, et al. Microbiome of affected and unaffected skin of patients with atopic dermatitis before and after emollient treatment. J Drugs Dermatol. 2014;13(11):1365–1372.
16. Seite S, Bieber T. Barrier function and microbiotic dysbiosis in atopic dermatitis. Clin Cosmet Investig Dermatol. 2015;8:479–483. doi:10.2147/CCID.S91521
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.