")
Back to Journals » Biologics: Targets and Therapy » Volume 16
TNF Inhibitors Exert a “Hidden” Beneficial Effect in the Cardiovascular Lipoprotein Profile of RA Patients
Authors Calvo Alén J , Lavin-Gomez BA , Aurrecoechea E, Guerra Ruiz AR , Martínez Taboada V, Gómez Gerique J
Received 26 February 2022
Accepted for publication 14 July 2022
Published 17 October 2022 Volume 2022:16 Pages 187—197
DOI https://doi.org/10.2147/BTT.S364191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Shein-Chung Chow
Jaime Calvo Alén,1 Bernardo Alio Lavin-Gomez,2 Elena Aurrecoechea,3 Armando Raul Guerra Ruiz,2 Víctor Martínez Taboada,4 Juan Gómez Gerique2, †
1Rheumatology Department, Hospital Universitario Araba, Universidad del País Vasco, and Instituto de Investigación Biomédica BIOARABA, Vitoria, Spain; 2Clinical Biochemistry Department, Hospital Universitario Marqués de Valdecilla, Santander, Spain; 3Rheumatology Division, Hospital Universitario Sierrallana, Torrelavega, Spain; 4Rheumatology Department, Hospital Universitario Marqués de Valdecilla Universidad de Cantabria, Santander, Spain
†Juan Gómez Gerique passed away on 30 December 2015
Correspondence: Jaime Calvo Alén, Rheumatology Department, Hospital Universitario Araba, Universidad del País Vasco, C/ Francisco Leandro de Viana s/n, Vitoria, Alava, 01009, Spain, Tel +34 945007576, Email [email protected]
Purpose: A high cardiovascular risk has been described in patients with rheumatoid arthritis (RA); the effects of different biological agents have also been described in these patients. The aim of the present study is to examine the effects of tumor necrosis factor inhibitors (TNFi) in the lipoprotein profile of RA patients using a broad laboratory assessment including a large number of non-routine tests.
Patients and Methods: RA patients treated with and without TNFi (70 patients in each group) were cross-sectionally compared regarding a broad spectrum of lipoprotein parameters including serum levels of total and HDL, LDL and VLDL cholesterol triglycerides, lipoprotein A (LpA), apolipoprotein A1 (Apo A), B100 (Apo B) and paroxonase. For each lipoprotein subfraction (HDL, LDL and VLDL), we assess specific concentrations of cholesterol, triglycerides, phospholipids and proteins and total mass of each one. Additionally, HDL Apo A, LDL and VLDL Apo B concentrations and number of particles of LDL and VLDL were also determined. Exploratory univariate and multivariate analyses of the different variables were performed.
Results: Seventy patients in each subset were enrolled. Patients on treatment with TNFi showed a trend to be younger and to have a longer disease duration. Regarding the lipoprotein analyses, borderline significant higher levels of serum Apo A were detected and an independent association with lower HDL mass, LDL triglyceride, VLDL cholesterol, VLDL Apo B, VLDL mass, number of VLDL cholesterol molecules and number of particles of VLDL was clearly observed.
Conclusion: TNFi treatment was associated with beneficial atherogenic effects at the lipoprotein level especially centered in the VLDL-related parameters consistent with a reduction of the atherogenic risk.
Keywords: rheumatoid arthritis, lipoproteins, tumor necrosis factor inhibitors
Introduction
Rheumatoid arthritis (RA) is a multisystemic inflammatory condition largely characterized by its articular involvement. However, during the last several years, a large body of evidence has shown that this disease portends an increasing risk for cardiovascular complications.1,2 Patients with RA have two- or three-fold higher risk than healthy individuals of suffering a myocardial infarction and a 50% higher risk of having a stroke. These patients also have an increased cardiovascular disease (CVD) mortality with a standardized mortality ratio of 1.5 (95% CI 1.4–1.6), as has been reported in several meta-analyses and systematic reviews.3–6 Furthermore, imaging studies have shown that these patients present an accelerated rate of atherogenesis in comparison with the general population.7,8
The reasons for this increased risk of CVD in RA most probably include both traditional risk factors for CVD and disease-related features.9 Patients with RA present a higher incidence of traditional CVD risk factors including lack of exercise, obesity, diabetes and/or dyslipidemia. In fact, changes in lipid profile, indicative of higher atherogenic risk, have been described even during the preclinical phase of this disease.10 These changes might be further worsened by some treatments, particularly glucocorticoids. Furthermore, it has been described that the inflammatory and immunologic milieu of this type of disease may exert pro-atherogenic effects at the endothelial and metabolic levels.11,12
Specifically, it has been reported that a systemic inflammatory status may have a negative influence on the lipid profile of these patients that can be evident even before the clinical onset of the disease, as has been already underscored. Moreover, in RA as in other immunologically mediated systemic diseases such as systemic lupus erythematosus (SLE), it has been demonstrated that high-density lipoprotein (HDL) loses its protective characteristics against atherogenesis turning out into a pro-atherogenic phenotype.13 These lipoprotein alterations seem to be mostly mediated by some of the cytokines produced during the inflammatory state characteristic of these diseases. To this end, TNFα, which has been seen to play a central role in the pathogenesis of RA, seems to have important effects on lipid metabolism and atherogenesis.14 Furthermore, it has been reported that TNF is able to reduce the serum activity of paraoxonase 1 (PON 1) this enzyme being one of the main factors that mediates the anti-atherogenic activity of HDL.15,16 Anti-TNF therapy also has other potential positive metabolic effects on other cardiovascular risk factors as they have been proved to improve insulin sensitivity and reversed defects in the insulin signaling cascade in RA patients with active disease and high insulin resistance. However, the impact of these biochemical changes in modifying cardiovascular disease burden in active RA patients remains to be demonstrated.17
Treatment of RA has improved significantly over the last few decades, not only due to the development of highly effective targeted agents but also because of an earlier and more aggressive therapeutic approach based on a “treat to target” (T2T) approach. This stricter control of the inflammatory process should also lead to better outcomes in the disease-related CVD complications. In fact, the use of methotrexate has been associated with a decrease in CVD mortality.18
Biologic agents and specifically TNF inhibitors (TNFi) constitute a step forward in the management of this disease. Undoubtedly, they have allowed a better control of the clinical activity of the disease by using a more specific and targeted mechanism of action. Beneficial cardiovascular effects in RA have been reported with the use of TNFi,19 despite the fact that elevations of serum levels of total cholesterol and LDL have been observed in some patients. Whether this positive effect is only due to a better control of the inflammatory process or to specific beneficial actions at the metabolic level has not been totally clarified.
Our objective was to perform a comprehensive and exploratory study about the potential effects of TNFi on the lipoprotein metabolism, studying a broad number of conventional and non-conventional lipoprotein parameters. Our hypothesis is that we may uncover beneficial effects that may help to explain the positive cardiovascular profile of these agents.
Methods
Study Design and Setting
Cross-sectional comparative study of patients on treatment with TNFi or only with conventional synthetic DMARDs (csDMARDs). The study was undertaken at two University hospitals (Hospital Universitario Marqués de Valdecilla and Hospital Universitario Sierrallana) of the autonomic community of Cantabria in Northern Spain, covering a total health-care area of about half a million inhabitants.
This study was approved by our regional IRB committee named: Comité de Etica e Investigación de Cantabria. All procedures of the present study were performed in agreement with the principles of the World Medical Association’s Declaration of Helsinki.
Study Population
Patients older than 18 years and fulfilling the 1987 revised ACR classification criteria for rheumatoid arthritis (RA) were eligible for the study.20 For the group treated with TNFi, eligible patients were those on treatment with TNFi for at least the preceding six months (TNFi group). As controls, a 1:1 sex and age (±5 years) matched group of patients treated only with csDMARDs was selected (csDMARD group).
General Clinical Evaluation
A review of the medical records of patients in both groups was done, and clinical, laboratory and comorbidity data were recorded. Physical and complete joint examination were performed in all participants at the outpatient clinic once; during that visit, blood tests were obtained including complete blood cell counts, biological markers of clinical activity [erythrocyte sedimentation rate (ESR) and C-Reactive protein (CRP)] and immunology tests including antinuclear antibodies (ANA), rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA). Additionally, blood samples were sent to the cardiovascular risk laboratory at the Hospital Universitario Marqués de Valdecilla, for the assessment of all the specific lipid determinations for this study (see below).
Clinical Activity and Disability Assessments
To assess clinical activity, the investigators calculated the DAS 28 (ESR) index21 at the time of the in-person clinic visit. The DAS-28 is an internationally validated and standardized index which collapses into a single number, using a mathematical formula, diverse clinical, laboratory, patient reported parameters [number of tender and swollen joints, the patient global assessment using a visual analog scale from 0 (perfect state) to 100 (the worst possible state)] and ESR; the end result is a numeric value which represents the level of clinical disease activity. This value allows classifying patients into remission (<2.6), low disease activity (≥2.6, <3.2), moderate disease activity (≥3.2, <5.1) and high disease activity (≥5.1).
Disability was assessed using the validated Spanish version of the Health Assessment Questionnaire (HAQ).22 This questionnaire evaluates the difficulties experienced in performing specific daily activities grouped into eight blocks. Each question scores range from 0–3 depending on the level of difficulty that the patient refers for performing such activity (0, no difficulty, 1 some, 2 a lot and 3, impossible to perform); the final score for each block is the worst answer. The final index score goes from 0–3, resulting from the sum of the scores of the eight blocks divided by eight.
Specific Lipid and Additional Realted Parameters
Plasma and serum samples were obtained by centrifugation at 1500 g, aliquoted, and frozen at −80°C, in less than 30 minutes after the blood had been obtained. In total serum, the following were determined: total cholesterol, triglycerides and total proteins by automatized enzymatic methods (ADVIA 2400 Clinical Chemistry System, Siemens Healthcare Diagnostics, Newark, United States), phospholipids (BEN Biochemical Enterprise, Italy) and HDL cholesterol (HDL-C) by enzymatic method after precipitation of non-HDL lipoproteins with phosphotungstic-magnesium acid of Biosystems (Barcelona, Spain) by slightly modified CHOD-PAP method, in a Dimension RXL (Siemens Healthcare Diagnostics, Germany), apolipoprotein A1 (Apo A), apolipoprotein B100 (Apo B), high sensitivity CRP (hsCRP) and Serum Amyloid A (SAA) by immunonephelometric (BNII-System, Siemens Healthcare Diagnostics, Germany), paraoxonase 1 (PON1) (Molecular Probes, UK), and activity of secretory phospholipases A2 (sPLA2) (Cayman Chemical, USA).
Separation of lipoproteins: a combined ultra-centrifugation method was used. The first centrifugation (40 minutes to 13,500 rpm, 5424 Eppendorf centrifuge) for separating chylomicrons and the second ultracentrifugation of the previous infranatant in density gradient (1006–1300 g/mL, dynamic gradient with potassium bromide (KBr)) for separating VLDL, LDL and HDL. This method consists of increasing the density of the serum above that of HDL and below that of the rest of the plasma proteins (usually at 1.24 g/mL) by adding KBr salt to the serum (387 g/L or 3.25 mol/kg). A volume of this high-density serum is placed at the bottom of an ultracentrifuge tube, and then superimpose solutions of decreasing density (ex: one volume of solution with a density of 1.21 g/mL and two volumes of 1.006 density solution). The sample was then centrifuged in Optima L-90 Beckman Coulter (23 hours to 57.000 rpm).
In all the obtained lipoprotein subfractions we measured cholesterol, triglycerides, phospholipids, proteins (colorimetric assay, Coomassie brilliant blue - CBB R250, Sigma, USA) and potassium concentration. The mean density of each subfraction was calculated through the concentration of potassium used for the formation of the gradient with potassium bromide (KBr) previously mentioned. In addition, in the HDL subfraction the concentration of specific proteins such as ApoA1, SAA and PON 1 was measured. In all the subfractions the final volume was corrected to be referred to its specific concentration in whole serum (measured volume through the weight/ density rate and referred to the initial used serum volume).
The number of VLDL and LDL particles was estimated from Apo B determination by their equimolar presence (1 particle of Apo B in each one of these two fractions). The number of cholesterol and triglyceride molecules per particle was estimated from the determination of cholesterol and triglycerides for each fraction. Total mass of each lipoprotein was calculated by adding the estimated masses for each fraction of cholesterol, triglycerides, phospholipids and proteins.
Statistical Methods
Our initial sample size estimation was to include at least 70 patients per group. There is not much information in the literature regarding data explored in our study but according to some studies which have examined some of these parameters,13 to detect the expected differences in them with a level of two tailed significance of 5% and a power of 80%, and assuming similarity between the standard deviations of the groups to be compared, forty patients, at least, would have been necessary for each group. Anticipating 20% losses, we finally decided that the number of patients aforementioned by group would be sufficient to carry out the study.
Standard descriptive parameters were used for showing salient characteristics of the patients. For univariate analysis, Chi-square for categorical variables and Student’s t-tests for continuous variables were applied. In the case that the distribution of the continuous variable was not normal the non-parametric test of Mann–Whitney’s U-test was utilized.
Variables of interest found to differ significantly between both subsets of patients were further analyzed. In order to control potential confounding factors, multivariate linear regression models were built. In all the cases, all the variables found to be significant in the univariate analysis as well as those thought to be clinically relevant were entered in the different multivariate models using a manual backward variable selection strategy according to the level of significance of each variable to select the most parsimonious and biological consistent models.
SPSS software V.23 (IBM SPSS Statistics Armonk, NY, USA) was used for all statistical analyses.
Results
General Findings
We enrolled seventy patients in each treatment group. In Table 1 the demographics and salient clinical and therapeutic characteristics of both treatment groups are shown. The total population represents the typical RA cohort with higher female representation and with percentages of positivity for RF and ACPA between 60–70% (61.2 and 70.5% respectively), without significant inter-subset differences in all these figures. Mean age at diagnosis and disease duration were 51.1±13.1 years and 99.8±76.8 months for the entire cohort. Patients in the TNFi subgroup had a trend towards being younger (49.0±12.5 vs 53.2±13.3 years; p=0.058) and a significant longer disease duration (117.5±77.3 vs 81.6±72.1 months; p=0.005). No relevant differences were found between the two subgroups of patients regarding the comorbidities recorded in the study.
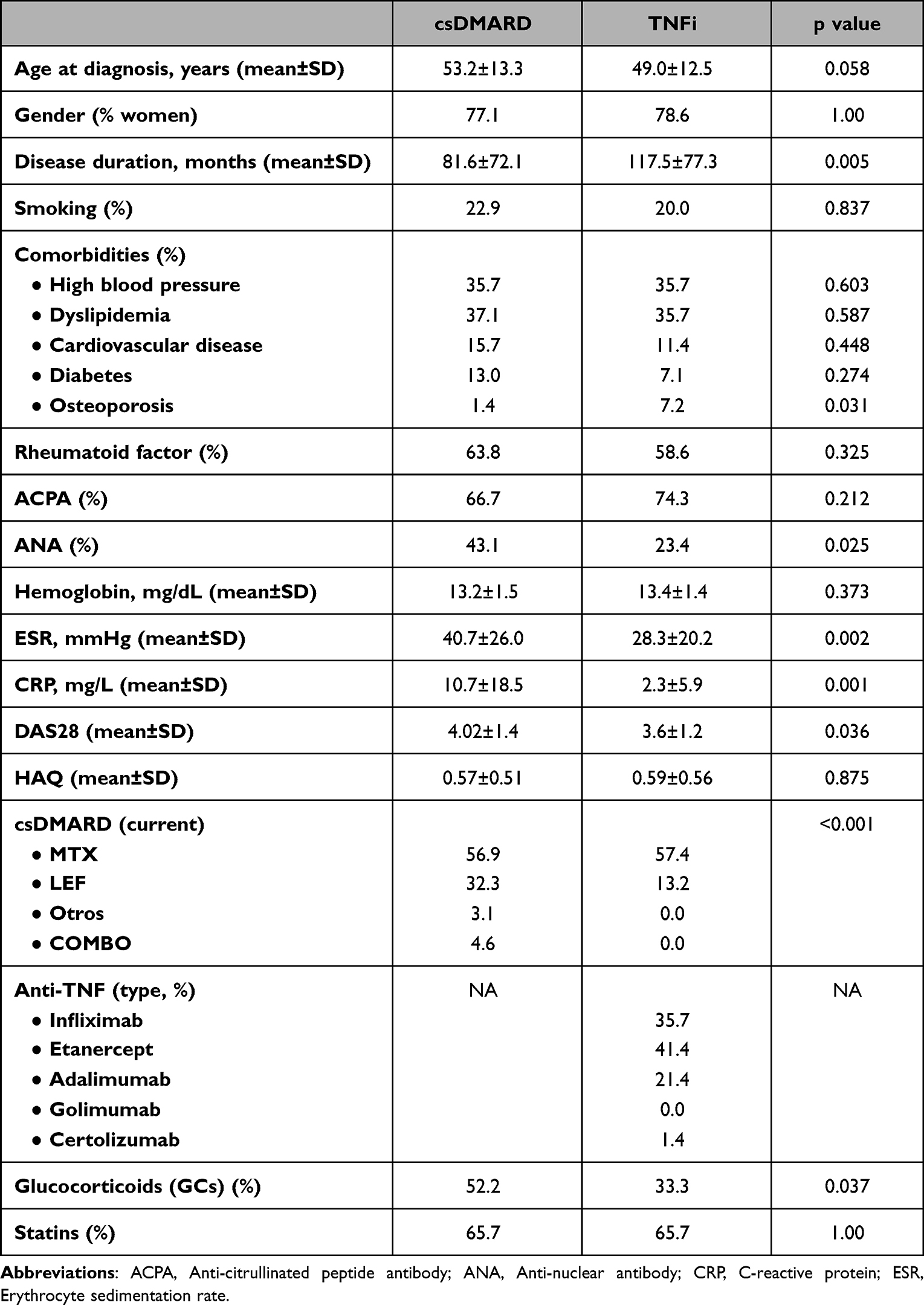 |
Table 1 General Characteristics |
With respect to the clinical status of the patients, biological and composite indices showed that patients in the csDMARD subgroup presented higher disease activity with higher ESR (40.7±26.0 vs 28.3±4; p=0.025), CRP (10.7±18.5 vs 2.3±5.9; p=0.001) and DAS 28 (4.0±1.4 vs 3.6±1.2; p=0.036) values. Conversely, the level of functional impairment as assessed by the HAQ was similar in both subsets of patients.
Finally, with respect to treatment the large majority of patients were still on csDMARDs, mostly using methotrexate. A larger percentage of patients on TNFi therapy were off any type of csDMARD (29.4 vs 3.1%; p<0.001).
Lipoprotein Profile Comparisons: Univariate Analyses
A detailed description of the univariate comparisons for all the parameters examined is given in Table 2. No differences between both groups of patients were observed in the standard lipid profile (concentrations of total cholesterol, HDL and LDL-Cholesterol and triglycerides). We did not find either differences in the serum total concentrations of Lipoprotein (a) [Lp (a)] or Apo B but a borderline significant difference with a higher value of Apo A in the TNFi subset was observed (169.8±29.3 vs 160.2±28.2; p=0.052).
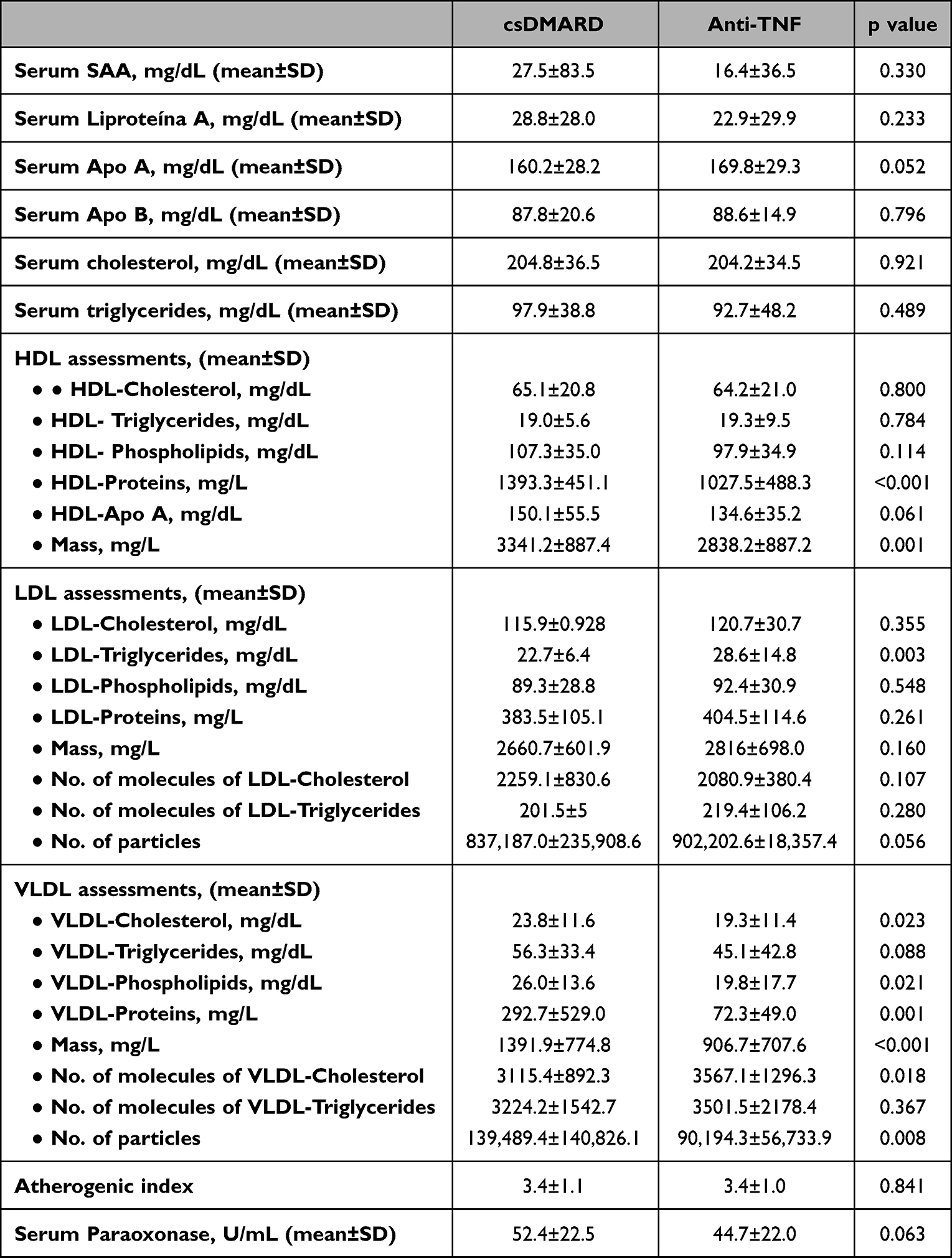 |
Table 2 Univariate Analyses |
Regarding the specific assessments of each lipoprotein we find the following results. In HDL, no differences were observed in the composition of the different lipid constituents (cholesterol, triglycerides and phospholipids). On the contrary, a decrease in the protein concentration was present in the TNFi subgroup (1027.5±488.3 vs 1393.3±451.1; p<0.001). Likewise, a lower HDL mass was recorded among patients in the TNFi vs the comparison groups (2838.2±887.2 vs 3341.2±887.4; p=0.001). On the other hand, no significant differences were found in any parameter related to LDL with the exception of triglyceride subfraction concentration (22.7 to 28.6; p=0.003). Finally, the most noticeable findings were seen in relation with the VLDL particle. Patients treated with TNFi showed lower levels of cholesterol, phospholipids and proteins including Apo B, a decrease in VLDL total mass as well as in the number of particles of VLDL.
Multivariate Analyses
We built different multivariate models for all the variables that had shown statistically significant inter group differences and with relevant biological meaning for the objective of the study, entering in each case all the possible confounding variables to explore the independent association with the utilization of TNFi including age and disease duration which have been shown to be different between the two patient groups. As can be observed in Table 3, such independent association was corroborated in all cases, regardless of the fact that different additional variables had also an independent association with the dependent variable in some of the cases. Specifically, to note that in the majority of VLDL parameters including decrease in cholesterol, Apo B, total mass and number of particle levels, in addition with the treatment with TNFi the use of statins showed an independent effect as well.
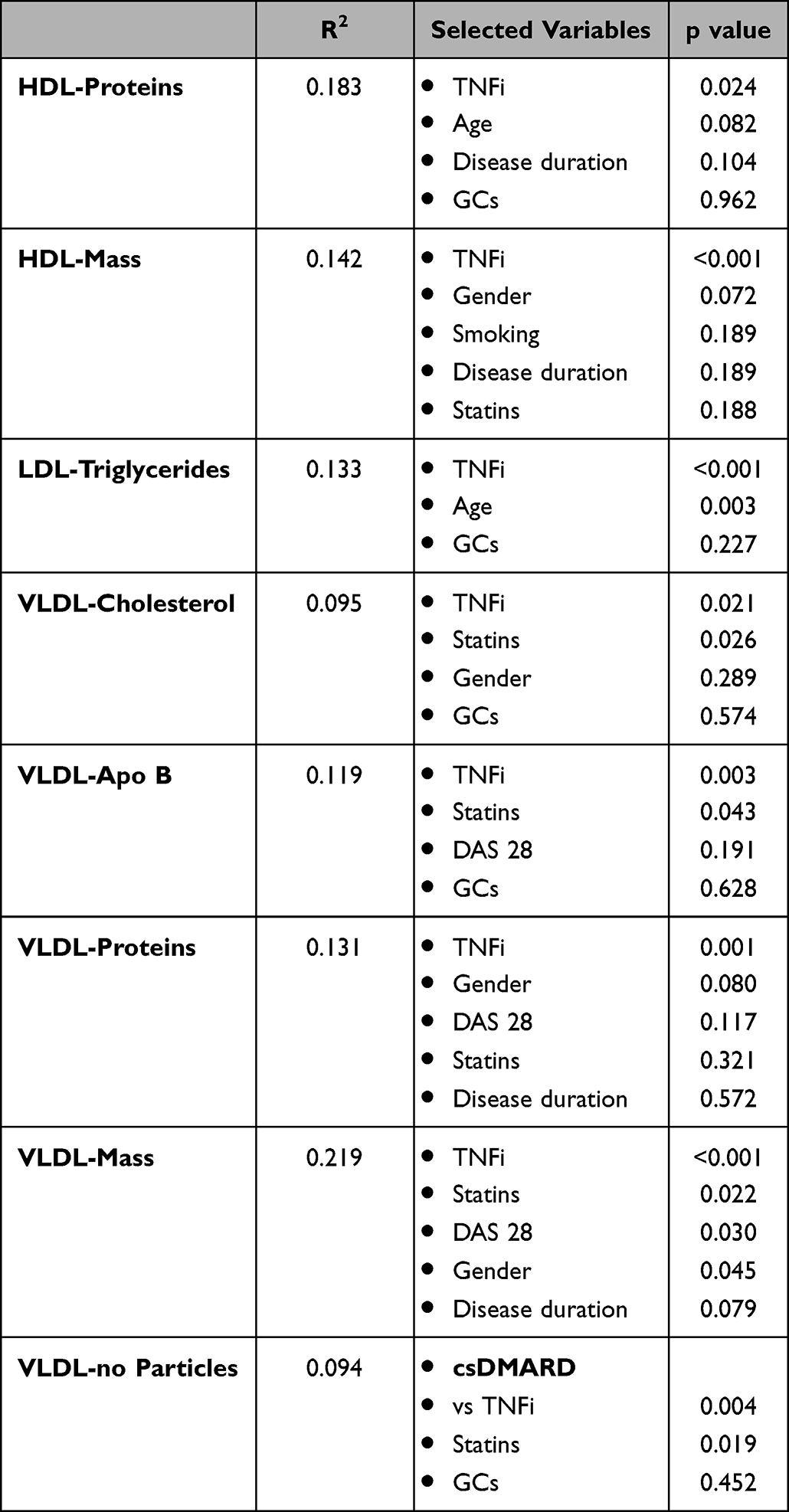 |
Table 3 Multivariate Analyses (Selected Models) |
Discussion
Our results show that TNFi produce a net beneficial effect in the lipoprotein profile of RA patients which may lead to a lower atherosclerotic risk. However, this biochemical effect is generally overlooked given that their effects seem to be centered in several aspects related with VLDL particles which are not routinely determined.
The VLDL particles are produced by the liver and are triglyceride rich. They contain various apolipoproteins and Apo B-100 is the core structural protein; each VLDL particle contains one Apo B-100 molecule. These nascent VLDL are in charge of transporting these lipids from the liver to the peripheral tissues where the tryglycerides undergo lipolysis.23,24 The nascent VLDL particles do not portend a high atherogenic risk since they have a low content of cholesterol and a larger molecular size than other lipoproteins, which makes it difficult for these molecules to go through the endothelial cell barrier into the arterial walls. At the peripheral level, the triglyceride depletion of VLDL produces remnant VLDL molecules of smaller size and enriched in cholesterol. Some of these particles are transformed into the LDL by the action of enzymes such as hepatic lipase (HL) which totally depletes them from triglycerides and cholesteryl ester transfer protein (CEPT) that allows them to capture esterified cholesterol molecules.25,26 On the other hand, part of the remnant VLDL remain in the circulation becoming highly atherogenic particles. A body of evidence exists pointing out an important role of triglyceride-rich lipoproteins, and especially VLDL in cardiovascular risk.27,28 Moreover, some recent studies have shown that this subfraction of lipoprotein is especially relevant for the cardiovascular risk in those individuals with LDL level below 130 mg/dl, which is part of remnant cardiovascular risk.29
According to the data from our study, RA patients on TNFi therapy present lower levels of atherogenic VLDL related parameters including the concentration of total VLDL-cholesterol, VLDL-proteins and specifically VLDL-Apo B, total VLDL mass, number of cholesterol molecules per VLDL particle and number of VLDL particles. Besides, regarding the last-mentioned parameter, it has been underscored that the number of particles is a more accurate measurement than the cholesterol lipoprotein concentration to assess the cardiovascular risk. A higher number of particles is usually associated with a smaller molecular size and the smaller the lipoproteins are the more atherogenic they become.30
Regarding the rest of the main lipoproteins, our study showed less pronounced effects. HDL is a lipoprotein which consists of a core of hydrophobic lipids, including cholesteryl esters and triglycerides, and a surface monolayer containing phospholipids, free cholesterol, and apolipoproteins.31 Apo A is, largely, the most abundant protein, representing 70% of the total. In addition, HDL contain the enzyme PON 1 that is responsible for the antioxidant properties of the HDL. Thus, this lipoprotein exerts anti-inflammatory and athero-protective effects in healthy individuals due to its capacity to remove the excess cholesterol from macrophages of the arterial wall as well as preventing LDL particles from being oxidized.32 However, in several chronic inflammatory conditions such as RA, HDL may turn into a dysfunctional state losing these protective functions and shifting to a more proinflammatory phenotype.13 In these situations, it has been observed that Apo A is displaced by SAA, that is elevated in chronic inflammatory states, and at the same time is largely oxidized, whereas there is also a decrease of PON activity. All these changes lead to a minor cholesterol efflux activity and a lower anti-oxidative capacity.33,34 We did not assess functional HDL activity in our study and therefore we cannot assert whether TNFi help to reverse the potential proinflammatory phenotype of HDL. Nevertheless, we did not observe major changes in the HDL composition. Our results only showed a significant decrease in HDL mass mainly due to a decrease in the protein content. We may speculate that this protein depletion might be due to a decrease in the HDL-SAA concentration given that we did not see significant differences in the HDL-Apo A levels (the other preponderant protein). Moreover, we observed that TNFi is associated with a borderline significant increase in the Apo A serum levels along with a non-significant trend (by parametric analysis) towards lower serum levels of SAA; in fact when a non-parametric analysis such as Mann–Whitney’s U-test was performed, given the distribution skewness of this variable, the difference of serum SAA became significant (p=0.001; data not shown). On the other hand, we did not observe differences in the serum concentration of PON (data not shown), although no anti-oxidative capacity specific tests were performed.
As has been stated, LDL particles are produced from the VLDL. They are rich in cholesterol and Apo B is their main protein35 and carry the highest risk for atherosclerosis. These particles form a relatively heterogeneous population of lipoproteins with different sizes and density, with those that are smaller and denser being more atherogenic. According our results, the only relevant change observed in the TNFi subset of patients in the LDL composition was a significant increase of triglycerides. Although the triglyceride enrichment of these particle might be associated with less penetration and deposit of particles under endothelium, and consequently a decrease in the cardiovascular risk, this fact has not yet clearly established.36 We did also observe a non-significant increase in the number of particles in patients treated with TNFi, which is difficult to interpret at this moment.
Finally, we measured serum levels of Lp (a), another cholesterol rich and atherogenic lipoprotein, but no significant differences were found. Lp (a) serum levels are genetically determined and minor changes are expected through an individual’s lifetime, except for acute inflammatory states. Treatment with statins does not modify circulating levels of Lp(a), and only recently some data have been published notifying a decrease in Lp(a) concentration in patients treated with PCSK9 inhibitors. Our results suggest that treatment with TNFi, despite their effect on the inflammatory state, do not seem to alter Lpa levels.37
We recognize that our study has several limitations derived from its cross-sectional design. However, we have tried to overcome in part such problems using multivariable models to adjust for potential confounders such as demographic factors, disease activity, or the use of statins, for example. We cannot rule out the potential metabolic effects of csDMARDs in our patients. However, methotrexate was by far, the most used csDMARD and it was equally used in both patient subsets. The only differences found were with the use of leflunomide, which was more frequently taken by the controls, but this variable did not show any effect in the multivariate analysis. The limited sample size may also pose some concerns, especially when multiple comparisons are performed. Again, we think that the use of multivariate models may circumvent this issue in some way. Finally, as has been mentioned, functional analysis of HDL oxidative capacity is lacking but we focus our study on an in-depth analysis of the composition and structure of the main lipoprotein using determinations that to our knowledge have not been previously reported in these types of patients.
In conclusion, we are reporting that in RA patients, treatment with TNFi produce beneficial effects at the lipoprotein level and from an atherogenic point of view with triglycerides enrichment of the LDL particles and, mainly, smaller remnant atherogenic risk with lower VLDL-cholesterol, VLDL-Apo B, total VLDL mass, number of cholesterol molecules per VLDL particle and number of VLDL particles. All this positive effect remains hidden using conventional lipid determinations and may provide some mechanistic explanations for the cardioprotective effects that these agents have shown in clinical registries.
Data Sharing Statement
Any material or additional data are available by request to the corresponding author.
Ethics Approval
As stated in the manuscript our study was approved by our regional IRB committee named: Comité de Etica e Investigación de Cantabria. All procedures of the present study were performed in agreement with the principles of the World Medical Association’s Declaration of Helsinki.
Consent to Participate
All the participants in the present study signed the corresponding informed consent.
Author Contributions
All the authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas as well as everyone drafted or written, or substantially revised or critically reviewed the article. All of them agreed on the journal to which the article will be submitted and reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Finally, all authors agree to take responsibility and be accountable for the contents of the article.
Funding
This study was carried out with the support of Instituto de Salud Carlos III (ISCIII) (grant number PI0810119).
Disclosure
Dr Víctor Martínez Taboada reports Lectures from Abbvie, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Blum A, Adawi M. Rheumatoid arthritis (RA) and cardiovascular disease. Autoimmun Rev. 2019;18(7):679–690. doi:10.1016/j.autrev.2019.05.005
2. Ward MM. Recent improvements in survival in patients with rheumatoid arthritis: better outcomes or different study designs? Arthritis Rheum. 2001;44(6):1467–1469. doi:10.1002/1529-0131(200106)44:6<1467::AID-ART243>3.0.CO;2-6
3. Avina-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59(12):1690–1697. doi:10.1002/art.24092
4. Avina-Zubieta JA, Thomas J, Sadatsafavi M, Lehman AJ, Lacaille D. Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies. Ann Rheum Dis. 2012;71(9):1524–1529. doi:10.1136/annrheumdis-2011-200726
5. Levy L, Fautrel B, Barnetche T, Schaeverbeke T. Incidence and risk of fatal myocardial infarction and stroke events in rheumatoid arthritis patients. A systematic review of the literature. Clin Exp Rheumatol. 2008;26(4):673–679.
6. Meune C, Touze E, Trinquart L, Allanore Y. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology. 2009;48(10):1309–1313. doi:10.1093/rheumatology/kep252
7. Gonzalez-Gay MA, Gonzalez-Juanatey C, Martin J. Rheumatoid arthritis: a disease associated with accelerated atherogenesis. Semin Arthritis Rheum. 2005;35(1):8–17. doi:10.1016/j.semarthrit.2005.03.004
8. Corrales A, Gonzalez-Juanatey C, Peiro ME, Blanco R, Llorca J, Gonzalez-Gay MA. Carotid ultrasound is useful for the cardiovascular risk stratification of patients with rheumatoid arthritis: results of a population-based study. Ann Rheum Dis. 2014;73(4):722–727. doi:10.1136/annrheumdis-2012-203101
9. Liao KP, Solomon DH. Traditional cardiovascular risk factors, inflammation and cardiovascular risk in rheumatoid arthritis. Rheumatology. 2013;52(1):45–52. doi:10.1093/rheumatology/kes243
10. van Halm VP, Nielen MM, Nurmohamed MT, et al. Lipids and inflammation: serial measurements of the lipid profile of blood donors who later developed rheumatoid arthritis. Ann Rheum Dis. 2007;66(2):184–188. doi:10.1136/ard.2006.051672
11. Bartoloni E, Alunno A, Bistoni O, Gerli R. How early is the atherosclerotic risk in rheumatoid arthritis? Autoimmun Rev. 2010;9(10):701–707. doi:10.1016/j.autrev.2010.06.001
12. Liao KP, Solomon DH. Mechanistic insights into the link between inflammation and cardiovascular disease: rheumatoid arthritis as a human model of inflammation. Circ Cardiovasc Imaging. 2014;7(4):575–577. doi:10.1161/CIRCIMAGING.114.002235
13. McMahon M, Grossman J, FitzGerald J, et al. Proinflammatory high-density lipoprotein as a biomarker for atherosclerosis in patients with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Rheum. 2006;54(8):2541–2549. doi:10.1002/art.21976
14. Dixon WG, Symmons DP. What effects might anti-TNFalpha treatment be expected to have on cardiovascular morbidity and mortality in rheumatoid arthritis? A review of the role of TNFalpha in cardiovascular pathophysiology. Ann Rheum Dis. 2007;66(9):1132–1136. doi:10.1136/ard.2006.063867
15. Feingold KR, Memon RA, Moser AH, Grunfeld C. Paraoxonase activity in the serum and hepatic mRNA levels decrease during the acute phase response. Atherosclerosis. 1998;139(2):307–315. doi:10.1016/S0021-9150(98)00084-7
16. Kumon Y, Suehiro T, Ikeda Y, Hashimoto K. Human paraoxonase-1 gene expression by HepG2 cells is downregulated by interleukin-1beta and tumor necrosis factor-alpha, but is upregulated by interleukin-6. Life Sci. 2003;73(22):2807–2815. doi:10.1016/S0024-3205(03)00704-5
17. Stagakis I, Bertsias G, Karvounaris S, et al. Anti-tumor necrosis factor therapy improves insulin resistance, beta cell function and insulin signaling in active rheumatoid arthritis patients with high insulin resistance. Arthritis Res Ther. 2012;14(3):R141. doi:10.1186/ar3874
18. Choi HK, Hernan MA, Seeger JD, Robins JM, Wolfe F. Methotrexate and mortality in patients with rheumatoid arthritis: a prospective study. Lancet. 2002;359(9313):1173–1177. doi:10.1016/S0140-6736(02)08213-2
19. Low AS, Symmons DP, Lunt M, et al. Relationship between exposure to tumour necrosis factor inhibitor therapy and incidence and severity of myocardial infarction in patients with rheumatoid arthritis. Ann Rheum Dis. 2017;76(4):654–660. doi:10.1136/annrheumdis-2016-209784
20. Arnett FC, Edworthy SM, Bloch DA, et al. The The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–324. doi:10.1002/art.1780310302
21. Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38(1):44–48. doi:10.1002/art.1780380107
22. Pincus T, Summey JA, Soraci SA, Wallston KA, Hummon NP. Assessment of patient satisfaction in activities of daily living using a modified Stanford Health Assessment Questionnaire. Arthritis Rheum. 1983;26(11):1346–1353. doi:10.1002/art.1780261107
23. Tiwari S, Siddiqi SA. Intracellular trafficking and secretion of VLDL. Arterioscler Thromb Vasc Biol. 2012;32(5):1079–1086. doi:10.1161/ATVBAHA.111.241471
24. Choi SH, Ginsberg HN. Increased very low density lipoprotein (VLDL) secretion, hepatic steatosis, and insulin resistance. Trends Endocrinol Metab. 2011;22(9):353–363. doi:10.1016/j.tem.2011.04.007
25. Kita T, Brown MS, Bilheimer DW, Goldstein JL. Bilheimer DW and Goldstein JL. Delayed clearance of very low density and intermediate density lipoproteins with enhanced conversion to low density lipoprotein in WHHL rabbits. Proc Natl Acad Sci U S A. 1982;79(18):5693–5697. doi:10.1073/pnas.79.18.5693
26. Fitzgerald ML, Mujawar Z, Tamehiro N. ABC transporters, atherosclerosis and inflammation. Atherosclerosis. 2010;211(2):361–370. doi:10.1016/j.atherosclerosis.2010.01.011
27. Nordestgaard BG. Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: new Insights From Epidemiology, Genetics, and Biology. Circ Res. 2016;118(4):547–563. doi:10.1161/CIRCRESAHA.115.306249
28. Budoff M. Triglycerides and triglyceride-rich lipoproteins in the causal pathway of cardiovascular disease. Am J Cardiol. 2016;118(1):138–145. doi:10.1016/j.amjcard.2016.04.004
29. Lawler PR, Akinkuolie AO, Chu AY, et al. Atherogenic lipoprotein determinants of cardiovascular disease and residual risk among individuals with low low-density lipoprotein cholesterol. J Am Heart Assoc. 2017;6. doi:10.1161/JAHA.117.005549
30. Cromwell W, Otvos J. low-density lipoprotein particle number and risk for cardiovascular disease. Curr Atheroscler Rp. 2004;6(5):381–387. doi:10.1007/s11883-004-0050-5
31. Kontush A, Lindahl M, Lhomme M, Calabresi L, Chapman MJ, Davidson WS. Structure of HDL: particle subclasses and molecular components. Handb Exp Pharmacol. 2015;224:3–51. doi:10.1007/978-3-319-09665-0_1
32. Kim SY, Yu M, Morin EE, Kang J, Kaplan MJ, Schwendeman A. High-density lipoprotein in lupus: disease biomarkers and potential therapeutic strategy. Arthritis Rheumatol. 2020;72(1):20–30. doi:10.1002/art.41059
33. Kakkar VV, Rao VS, Kakkar VV. Friend turns foe: transformation of anti-inflammatory HDL to proinflammatory HDL during acute-phase response. Cholesterol. 2011;2011:274629. doi:10.1155/2011/274629
34. Gaal K, Tarr T, Lorincz H, et al. High-density lipopoprotein antioxidant capacity, subpopulation distribution and paraoxonase-1 activity in patients with systemic lupus erythematosus. Lipids Health Dis. 2016;15:60. doi:10.1186/s12944-016-0229-0
35. National Cholesterol Education Program Expert Panel on Detection E, Treatment of High Blood Cholesterol in A. Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143–3421. doi:10.1161/circ.106.25.3143
36. Boren J, Chapman MJ, Krauss RM, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2020;41(24):2313–2330. doi:10.1093/eurheartj/ehz962
37. Rehberger Likozar A, Zavrtanik M, Sebestjen M. Lipoprotein(a) in atherosclerosis: from pathophysiology to clinical relevance and treatment options. Ann Med. 2020;52(5):162177–162186. doi:10.1080/07853890.2020.1775287
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.