")
Back to Journals » Psychology Research and Behavior Management » Volume 15
TikTok Tourette’s: Are We Witnessing a Rise in Functional Tic-Like Behavior Driven by Adolescent Social Media Use?
Authors Frey J , Black KJ , Malaty IA
Received 1 September 2022
Accepted for publication 19 November 2022
Published 5 December 2022 Volume 2022:15 Pages 3575—3585
DOI https://doi.org/10.2147/PRBM.S359977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Jessica Frey,1 Kevin J Black,2 Irene A Malaty3
1Department of Neurology, Rockefeller Neuroscience Institute, West Virginia University, Morgantown, WV, USA; 2Departments of Psychiatry, Neurology, Radiology, and Neuroscience, Washington University in St. Louis, St. Louis, MO, USA; 3Department of Neurology, Fixel Institute for Neurological Diseases, University of Florida, Gainesville, FL, USA
Correspondence: Jessica Frey, Department of Neurology, Rockefeller Neuroscience Institute, West Virginia University, 1 Medical Center Drive, Morgantown, WV, 26505, USA, Tel +1 304-298-6127, Fax +1 304 598 6442, Email [email protected]
Abstract: Perceptions of Tourette syndrome (TS) and tic disorders are often driven by social media. During the COVID-19 pandemic, social media consumption greatly increased, particularly in the adolescent population. In parallel with increased social media consumption, there has also been an increase in tic severity and functional tic-like behavior (FTLB). Given that many of the tic videos posted on social media are misleading, perpetuate false beliefs about TS, or reinforce tic-like behaviors, there is increasing concern that these videos are driving the rapid increase in FTLBs. Several studies have reviewed newly presenting cases of FTLB and have found shared characteristics, including that a higher proportion of affected individuals are female, there is a low proportion with a history of childhood or family tics, and symptom onset is typically acute and develops in the teenage years. In addition, the quality of the tics seen in association with FTLB mirrors many of the tics seen on popular social media channels, with higher rates of coprophenomena, tic attacks, and involvement of the trunk and extremities than is seen with typical tics. FTLBs are likely a specific subgroup of functional tics largely influenced by the portrayal of and growing popularity of functional tics posted on social media during the COVID-19 pandemic. However, several factors, including increased anxiety, social isolation, and social media use in general during the pandemic are likely also contributing factors to the surge of FTLBs seen recently. In this era of increased social media consumption, it will become increasingly important for clinicians to educate patients about where and how medical information is spread, to ensure the best possible diagnosis, treatment, and outcomes for patients.
Keywords: functional tics, social media, functional tic-like behavior, COVID-19 pandemic, Tourette syndrome
Introduction
Tourette’s syndrome (TS) is a neurodevelopmental disorder characterized by multiple motor tics and at least one phonic tic, typically preceded by a premonitory urge.1,2 To fulfill DSM-5 criteria, these symptoms must be present for at least one year and must be present before the age of 18.2 TS is more common in males compared to females (~4:1), and most commonly begins during childhood around ages 4–8.3 Chronic tic disorder (CTD) is diagnosed when an individual has either motor or phonic tics but not both.1 There is often a decrease in tic frequency starting around the ages of 12–17, with 75% of children having considerable tic improvement during adulthood and up to 32% having complete tic remission.4,5 However, although tics may improve during puberty, adolescents report this period of time as the most challenging from a social perspective since exclusion amongst peers due to tic symptoms often becomes more prominent.6 In addition to tics, TS is associated with comorbid symptoms such as obsessive-compulsive behavior (OCB), attention deficit hyperactivity disorder (ADHD), and mood disorders.7
Quality of life can be severely impaired in patients with TS due to tics, including difficulties with family relationships in 29%, difficulties in making friends in 27%, difficulties with socialization in 20%, and feeling self-conscious of tics in 15%.8 Beyond tics, up to 70% of individuals with TS reported non-tic-related impairments in quality of life, including difficulties in the school, home, or social environment.9 School difficulties include increased likelihood of having an individualized education plan (IEP), increased likelihood of needing to repeat a grade, and higher rates of absenteeism.10,11 One study of tic disorder impact involving 623 parents of children and 281 adults found that 35% of children and 77% of adults reported that tics interfered with achieving education commensurate with intellectual ability, and almost 20% of adult respondents reported subsequent limitation to their career paths as a result.12 These barriers result from negative stigmas surrounding TS, often due to misperceptions of TS in the larger community by teachers, peers, and parents.8 These stigmas can in turn lead to bullying and discrimination, with up to 75% of parents reporting that their child was treated differently due to their tics.11 In addition, societal stigmas often lead to self-stigmatization, along with higher rates of depression and anxiety compared to the general population.8,13 Many studies conclude that increasing education and awareness about what TS is and how it impacts an individual’s life can improve the overall well-being and quality of life for that individual.8,10,13 For example, a few studies evaluating the knowledge of teachers and children about TS revealed only a basic knowledge that was amenable to educational interventions.14,15
Since the onset of the COVID-19 pandemic, there has been a significant rise in sudden-onset, complex, and significantly disruptive tics with atypical features (described later). These presentations have been more consistent with functional neurological symptoms, which are thought to comprise a separate disorder, with characteristics distinct from typical organic tics. Sometimes referred to as functional tic-like behavior (FTLB), these tics can be seen in youth with no prior history of tics, and can also be seen to complicate the course of some youth with known tics and TS. This global phenomenon has resulted in concern that in the context of isolation and stress, attention and exposure to inaccurate portrayals of tics on social media may be fueling this notable rise.16,17 There are also concerns that these social media platforms may unintentionally increase misperceptions of TS, furthering stigma and the sequelae of living with a stigmatized disorder.16,18 Therefore, it is important not only to educate the general public about TS but also to educate individuals presenting with functional tics thought to be largely influenced by social media in order to reduce stigma, improve quality of life for those who have TS, and improve outcomes for individuals with functional tics.3
This review will evaluate the complex relationship between social media, COVID-19, and the impact each of these has on tic-related disorders.
Functional Tics
Functional tics fall under the larger umbrella of functional movement disorders (FMDs), generally thought to be an external manifestation or reaction to underlying psychosocial stressors.19 Functional tics have previously been referred to as pseudo-tics, psychogenic tics, and non-organic tics; however, the etiology of these non-typical tics has still not been well established and therefore the term functional tics is most often used as convention in recent years.20
The phenomenological characteristics of tics in TS are somewhere between volitional movement and involuntary movement,21 which makes distinguishing between typical tics of TS and functional tics challenging. There have been several proposals on how best to differentiate between typical tics and FTLBs, mainly based on clinical observations and case series of patients with atypical tics. Clues to the diagnosis of functional tics include a later onset in adolescence or young adulthood as opposed to childhood, sudden onset, complex tics at onset, and association with other functional neurologic disorders such as pseudoseizures. They occur more often in females as opposed to males, with a lack of childhood or family history of tics.17,20–22 In addition, functional tics may be associated with a lack of premonitory sensation, unusual premonitory symptoms, a perception of being totally involuntary, poor response to typical tic medications, difficulty with suppression, and higher rates of suggestibility.17,20–22 Certain behaviors are more common with functional tics, such as blocking tics, speaking in accents, as well as echo-, pali-, and coprophenomena.3,23 The characteristics of the tics themselves may also have features distinctive of organic tics, such as occurring more often in the trunk and extremities as opposed to the head, face, and neck.24,25 In addition, functional coprolalia is marked by longer and more complex phrases as well as a higher number of obscene words per individual.21 The tics themselves may be more self-injurious or functionally limiting than is typically seen in TS.3,23 However, shared risk factors such as anxiety and impulsivity, as well as overlap of clinical features can make it difficult to tell typical and functional tics apart.23 This is further complicated by the fact that individuals with a typical history of TS can later develop functional tics that may co-occur with their previous tics.20,21,23,26
There may be some overlap between the pathophysiology of typical tics and functional tics. In general, the pathophysiology of typical tics has clear influence of genetic determinants and is thought to be driven by a combination of two mechanisms, including enhanced reinforcement of motor learning via abnormally enhanced dopamine pathways and disinhibition of the cortico-thalamo-cortical loops leading to motor overflow.23 Similar neural pathways have been postulated in association with functional neurologic disorders, where enhanced limbic-cortical activity may lead to reinforcement of abnormal motor patterns of movements and eventually lead to habituation of movement.23 Functional tics may additionally be modified by attention to tics, perception of whether or not movements are voluntary, skewed sense of agency over movements, and behavioral reinforcement.23 These modifiers, especially behavioral reinforcement, have become particularly relevant in the context of FTLBs seen recently. Observation of tics online via social media may lead to learning of this tic-like behavior and eventual habituation, which is discussed in more detail below.
Functional tics have been reported previously as a reaction to psychosocial stressors.27,28 However, functional tics were previously reported as relatively rare compared to other functional movement disorders (2%)20 and also rare compared to organic tics (1.9%).29,30 Explosive or acute onset of tics was previously reported to represent only 5–8% of cases of TS.24,31 Within the last several years, there has been a tremendous increase in acute-onset tics, tic attacks, and FTLBs,24,25,30,32 with at least one study reporting a tenfold increase in the prevalence of FTLBs.33 Although the rise of functional tics has been seen in a variety of distinctive geographic regions, the quality of the functional tics is similar and often exactly mimics the same symptoms posted online, leading many researchers to posit that the common thread between these individuals is the portrayal of functional tics in social media.26
Social Media and COVID-19
In response to the COVID-19 pandemic, quarantining and physical social distancing quickly became strategies to try to prevent further spread of the disease. In so doing, many individuals turned to social media to continue to feel connected to the rest of society and to cope with increasing anxiety, fear, and uncertainty for the future. One study of over 2000 adolescents found that social media was overall a constructive coping strategy during the pandemic, leading to increased happiness in individuals with anxiety and loneliness.34 While older children and adolescents used social media as a tool to become more informed about the pandemic, younger children often used social media to escape from the negativity associated with the pandemic and to seek out emotional support from others with an online presence.34,35 As reliance on and interest in using social media has grown during the pandemic, there has also been a corresponding increase in excessive social media use, leading to addictive tendencies in some cases.36 Interestingly, particular social media platforms were more likely to be associated with more addictive behaviors. For example, TikTok was found to be the most addictive social media platform amongst adolescents during the pandemic.36 This finding correlates well with the fact that TikTok also had a tremendous increase in use during the pandemic.24
Social media can be a valuable tool for disseminating information quickly, especially during a pandemic when time to publication could delay important information from becoming available to the public.37 It may also allow for a sense of connectedness in otherwise isolated individuals. However, social media is a double-edged sword in that it can cause harm either directly by spreading misleading or false claims or indirectly by overwhelming social media posts with misinformation and making accurate content more difficult to find or engage with.37 Misinformation spread via social media is not specific to TS or tics. In fact, several studies have demonstrated that information regarding COVID-19 on YouTube and TikTok is generally not useful or actually misleading.38–40 Another study evaluated information accuracy regarding ADHD, a common comorbid symptom of TS, and found that 52% of the TikTok videos about ADHD were misleading.41 Similar rates of misinformation have been reported for other medical conditions portrayed in social media such as acne and diabetes.41 Social media therefore could potentially exert a detrimental influence on healthcare outcomes, as misinformation may lead to increased healthcare anxiety surrounding various conditions or inappropriate utilization of healthcare resources, based on representations that are viewed.37,41
Portrayal of Tics in Media
Even before social media was a commonly used platform, tics and TS have been represented to the public in a variety of capacities, often through television, film, and literature. Many of these portrayals include exaggerated stereotypes and even incorrect depictions of individuals with TS. For example, characters with TS are often used as comic relief by demonstrating swearing tics or using profanity, even though the Tourette Association of America has concluded that only a small minority of patients experience coprolalia.1 Studies have reported rates of coprolalia ranging from 10% to 30% and indicate that having coprolalia leads to a much poorer quality of life as opposed to the comedic representation of coprolalia seen in the media.42–44 In addition, characters that were intended to have TS were incorrectly represented as having autism spectrum disorder instead, and interpersonal relationships with friends and family were often negatively portrayed, with increased conflict, difficulty communicating, and toxic relationship tendencies.45 Other studies have also demonstrated that although some depictions can be realistic, the vast majority of depictions of tics are stereotyped portrayals, which inadvertently worsen the stigmatization of individuals with TS.42,45–47 One study evaluating adolescents’ perceptions of peers with TS found that individuals with TS were thought to be deprived of agency and in need of assistance, leading to a “benevolence stigma” in combination with a reluctance to initiate any close or meaningful relationships with these individuals, due to fears of “social contamination.”42 This study went on to conclude that the reason for these misperceptions primarily stemmed from misrepresentations of the condition in the media, which may be the only baseline exposure non-affected individuals are aware of from which to derive their understanding of TS.42 These misrepresentations can also be seen on the internet. For example, online support groups can be an invaluable source of information and acceptance for individuals with TS, reducing social isolation and enabling accessibility when face-to-face resources may not be available or appropriate.48 However, even though these support groups typically have good intentions, users have identified tic triggers, tic suggestibility, and conflict among other users of the online support groups as negatively affecting their experience and worsening their tics.48 In some online forums, participants are encouraged to rate how severe their individual tics are and to compare to one another, leading to another layer of complexity in the psychodynamics of promoting illness or wellness. Finally, excessive engagement with tic-related content may lead to excessive focus on tics and detract from recognizing the individual as a whole person or other aspects of an individual’s identity and connectedness.
Portrayal of Tics in Social Media
The skewed portrayal of tics in social media is not new. In fact, a study from 2012 analyzed TS portrayals on YouTube and found that although there were some accurate and positive portrayals of TS available to view, negative portrayals of TS were associated with significantly more views.47 This bias may inadvertently reinforce negative stereotypes and spread misinformation.47 As early as 2016, there were documented cases of “tic attacks”, which were thought to represent a combination of tics and non-suppressible, disabling functional movements that could last for minutes to hours and often appeared to mimic seizure-like activity.31 The authors concluded that these tic attacks likely stem from both internal and external contextual factors, including increased attentional focus on tics, a cognitive-affective feedback loop leading to increasing anxiety, and greater interoceptive awareness.31
During the pandemic, there was an increased interest in TS via social media, leading to “#tourette” being viewed nearly 5 billion times on the TikTok platform alone.3,49 Social media can, in fact, be a positive support system in which users have acknowledged that social media portrayals of tics have led to peer support and a sense of belonging.24 However, there may be unintended consequences of viewing inaccurate portrayals of tics on social media, including reinforcement of maladaptive behaviors. Unfortunately, some of the misinformation propagated via social media may be financially motivated. For example, TikTok tic influencers sell merchandise related to the content of their videos or may even be paid to make an appearance. The videos with more views tend to be the videos portraying the most frequent, extraordinary, and violent tics, even when these are inaccurate portrayals.24 These same popular videos are the ones that are most likely to generate the most income for the uploader.24
Studies have sought to determine if there is a difference in phenomenology between organic and functional tics by analyzing the most-viewed videos on various social media platforms involving tics and TS.17,24 Among 28 videos of TikTok influencers with a keyword of Tourette or tic, the average age was 19, 64% were female, 64% had tic attacks, 93% had coprolalia, and 86% had injurious behavior, features that are not consistent with the typical individual experiencing TS.24 Similarly, another study also found higher rates of coprophenomena, self-injurious behavior, and environmental influences in videos labeled as “Tourette” on social media platforms such as TikTok, but that were believed to portray FTLB.17 There are concerns from experts in the TS community that inaccurate and popular portrayals of tics such as these may actually increase stigmatization and marginalization of individuals with tics.33,50
Social Media and COVID-19: Influence on Tic-Related Disorders
The COVID-19 pandemic clearly had an impact on tics, but this impact is complex and more nuanced than was originally thought. This complex influence will be analyzed for a variety of tic-related disorders including FMDs, PANDAS/PANS, and both typical and functional tics below.
Functional Movement Disorders (FMDs)
Since the onset of COVID-19, there has been growing interest in the number of functional movement disorders that have been reported across multiple institutions. Although there was no significant worsening of symptoms in patients who have preexisting FMD, there was an increase in the number of people who newly presented to clinic with FMD during the pandemic.19,49,51 At least one study reported a 60.1% increase in new patients diagnosed with FMD between March 1, 2020 and October 30, 2020.19 The majority of these new presentations occurred in female patients (75.6%), and the most common type of functional movement disorder reported was tremor (53.3%) followed by dystonia (31.1%).19 Although functional tics have garnered quite the presence in news and media outlets, this study reported that functional tics accounted for only 8.9% of the FMDs that presented during COVID-19.19 In addition, the rate of new-onset FMD following infection with COVID-19 was low, reported to only be 3% in comparison to other movement disorders seen following infection with COVID-19.52
Although the pathophysiology of FMDs is unclear, stress does seem to play a role as a precipitating factor. In addition, altered connectivity between the limbic and motor networks as well as decreased activation of the SMA may represent neurobiological differences in individuals who develop FMDs.19 It is hypothesized that prior traumas or other psychosocial stressors reshape the connectivity of the brain to make the brain more susceptible to having an FMD.19 During a time when psychosocial stressors are high secondary to COVID-19, these risk factors could at least in part account for the increase in FMDs being seen at movement disorder clinics. The treatment for FMD remains challenging, but a combination of psychoeducation and cognitive behavioral therapy may be helpful.53 Avoiding inadvertent reinforcement of the movements and addressing comorbidities such as depression, anxiety, and insomnia can also benefit patients with FMD.54
Tic Triggers in Other Disorders
Given the longstanding controversial consideration that rare cases of immune-triggered tics may follow certain types of infections, one study sought to characterize tic and other symptom changes during the COVID-19 pandemic in individuals with a prior diagnosis of Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections or Pediatric Acute-Onset Neuropsychiatric Syndrome (PANDAS/PANS). Of note, evidence in support of a link between streptococcal infection and acute tic onset or exacerbation has been equivocal,3,55,56 and association with other non-streptococcal infections has also been postulated. Among 108 included individuals that previously met the diagnostic criteria for PANDAS/PANS,57 71% reported an increase in overall symptoms during the pandemic lockdown.58 Interestingly, tics were more commonly reported to increase (56%) than were symptoms from other domains, all of which were below 50%, although it is unclear why tics were reported to have increased more in comparison to other symptoms.58 Environmental factors were suspected to account for worsening symptoms in these individuals, with sleep disruption proposed to be a key contributor. This same study identified the following risk factors for worsening neuropsychiatric symptoms: changes in parental work routine, parental stress or anxiety transmitted to children, boredom, being quarantined to a small living space, and inadequate information related to COVID-19.58 These same risk factors have also been identified for symptom worsening in disorders other than PANDAS/PANS, including TS.18,53,55 This highlights the importance of psychosocial environment in aggravating pre-existing symptoms.
Tics
Some individuals with tics may traverse the pandemic with no major changes in baseline tic severity, or even experience reduced tics during periods of less frequent social interactions. However, overall presentations to American emergency departments for tics increased substantially during the pandemic peak.59,60 The pandemic has exerted a negative influence on tics in the following three manners: worsening of tics in individuals who already have a preexisting history of tics, the acute onset of tic attacks or FTLBs, or a combination of worsening functional and typical tics in a single individual. However, because phenomenological features of TS and FTLB can overlap, distinguishing the symptoms can be difficult.17
Early in the pandemic, a study revealed that 48% of individuals with preexisting TS or CTD reported worsening of their tics and cited reasons such as increased anxiety due to fears surrounding the future, quarantining, fewer distractions, and changes in routine.61 Similarly, there was a worsening of symptoms in 67% of adolescents during the beginning of the pandemic, including more severe tics, hyperactivity, rage attacks, obsessions/compulsions, and anxiety.18
The COVID-19 pandemic was initially postulated to impact tic symptoms through a variety of avenues, including anxiety related to the pandemic, confinement/quarantine, alterations in tics specific to the pandemic, and neurotropic effects of COVID-19.55 The neurotropic effects are now thought much less likely to contribute to tic symptoms, and indirect impacts of COVID-19 are more likely to modify tic symptoms. For example, fears related to the pandemic, changes in work or financial stability, poor health of loved ones, or restricted freedom due to quarantine may contribute to anxiety that can in turn lead to worsening of tics. Indeed, one study found that in parents of children with tics, 32% had a significant reduction in income and 17% experienced unexpected unemployment in both parents.18 On the other hand, some individuals reported improvements in their tics because quarantining or virtual school removed many of the triggers that usually lead to worse tics.18 Up to 87% of children with tics have reported participating in online learning at home during the pandemic, and aside from school activities, the most popular pastimes were playing video games (69%) and interacting on social media (54%).18 Finally, pandemic-specific tics such as coughing or throat clearing may become more troubling or lead to worse stigmatization given public fears of contamination and spread of viral disease.55
In addition to alterations in tic symptoms in individuals who already carry a diagnosis of TS or CTD, there have also been reports of increasing cases of functional tics. Given the rapid onset and similarity to many tics represented in social media, it was proposed that these functional tics may be an example of a mass sociogenic illness.33 This is not the first time that tics have been “spread” by observing another individual’s behaviors. For example, there was an infamous outbreak of tic-like behavior in 19 students at Le Roy High School in 2012, sometimes referred to as “mass hysteria.”33 Due to their spread via social media, these functional tics may be a new digital equivalent termed “mass social media-induced illness” (MSMI).33 Some of the signs linking these functional tics to social media include the nearly identical replication of some tics (such as saying “beans”, or “woo hoo” or specific self-injurious or incapacitating tics similar to those seen online),62 as well as adoption of similar behaviors such as giving a name to the tic symptoms.33,50 Other indications that these functional tics may be a distinctive entity are that the tics tend to be severe enough to limit performing unpleasant tasks but abate when doing enjoyable activities, and remission of these tics was seen in some patients after a diagnosis of TS was excluded.33 Of course, it is important to remain cautious in identifying any causative forces without clear supporting evidence.63 Indeed, several studies have proposed that the functional tics seen in association with social media use are likely caused by a combination of complex factors, including predisposing factors such as pre-existing genetic risk factors for depression and anxiety, poor adaptive or coping behaviors, family and peer-related stressors, pandemic-specific impacts on mental health, social isolation, and behavioral modeling through exposure to social media.16,30,62
Regardless, several case reports, case series, and cohort studies have collectively identified over 100 patients that have been newly presented to a variety of institutions with what is believed to be FTLB (Table 1). Although the causative effect of social media has not been definitively linked to the onset of FTLBs, it is hard to ignore the similarities in pattern and behavior between the social media influencers and the patients presenting to movement disorder clinics around the world.
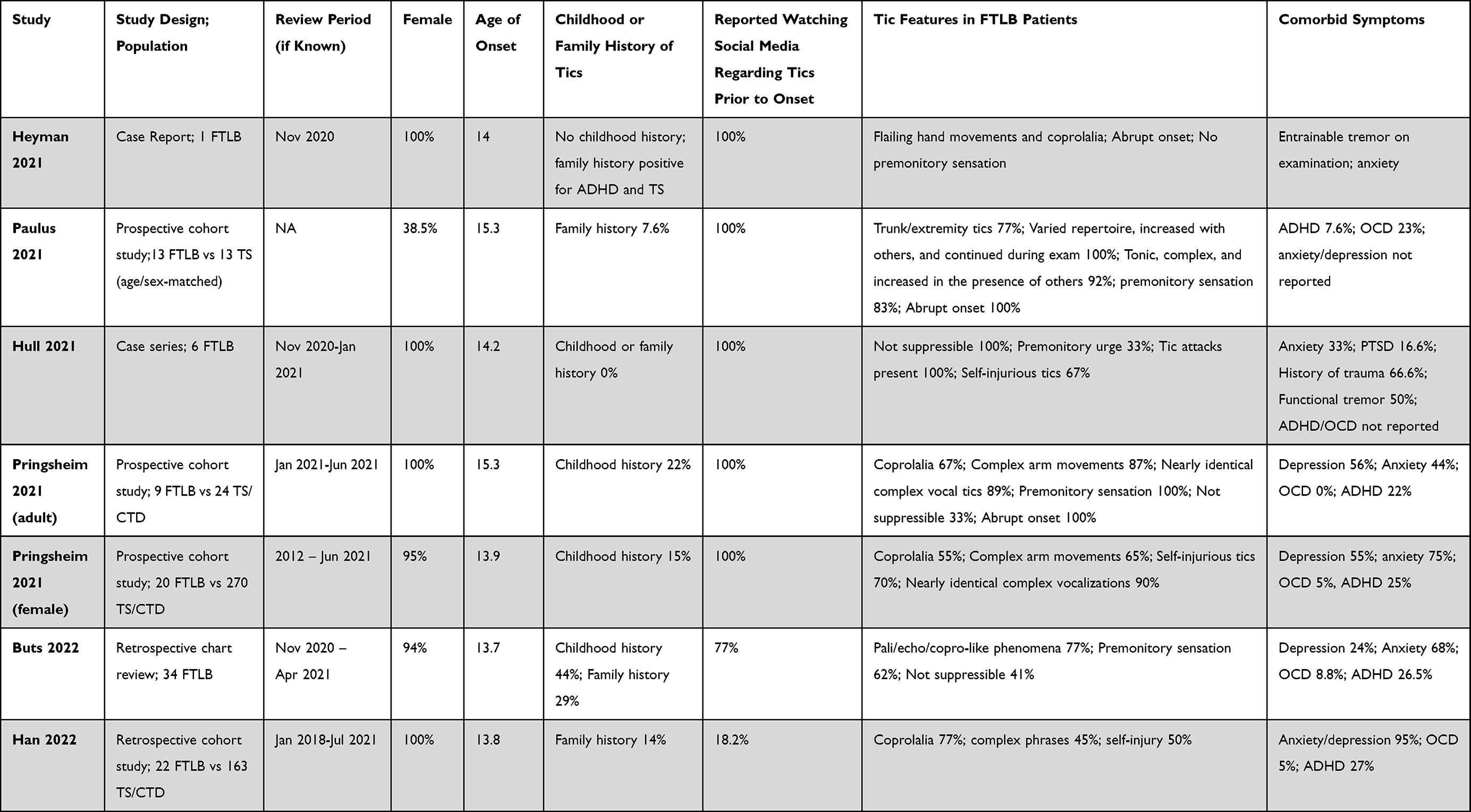 |
Table 1 Summary of Studies Evaluating FTLB Patients, Including Demographic Information, Exposure to Social Media Portrayals of Tics Prior to Onset, Tic Characteristics, and Comorbid Features |
Those presenting with FTLB share similar characteristics across reports: tic onset tends to be sudden and in teenage years, the majority are female, and few have a history of childhood or family tics. Tic characteristics are also strikingly similar: acute onset of complex movements predominately involving the trunk and extremities rather than the more usual tic onset with simple tics evolving over time to more complex and without the usual rostro-caudal evolution. In addition, there were high percentages of self-injurious behavior, coprophenomena, tic attacks, comorbid FMDs, and comorbid depression or anxiety.25,30,32,62,64–66 A high percentage of patients with FTLB were first seen in the emergency department due to the acuity and severity of their initial presentation.64 While there are several features that distinguish FTLBs from typical tics, there are also features that may or may not be present in either manifestation of tics, and may not necessarily help to differentiate between them. Specifically, suppressibility, premonitory urges, and comorbid symptoms such as anxiety could be seen in either population.25,62,64,65 In general, there were higher rates of anxiety and depression, lower rates of ADHD and OCD, and a lack of agency over movements was more often reported in patients with FTLBs compared to patients with typical tics.30,62,65 The demographic and clinical features of these patients are consistent with the videos posted in social media portraying FTLB.17,24 In addition, these features are also consistent with prior descriptions that have sought to differentiate functional tics from TS.20–22 Finally, many patients reported watching social media tic-related videos prior to their presentation to a movement disorder clinic with FTLB, although duration of exposure to this social media content was not documented in most studies.25,30,32,62,64,65
A 6-month follow-up of the patients with FTLB in the studies by Howlett et al found that there was an average decrease in the Yale Global Tic Severity Scale (YGTSS) of 31.9 and 19.6 points in adolescents and adults, respectively, which suggests that adolescents may have a better prognosis than adults, or at least respond more quickly.67 The most effective treatment approaches for achieving reduction in functional tic symptoms are still being investigated. To date, there are no randomized controlled studies dedicated to treatments specifically for functional tics. Some studies observed improvement in functional tics when treating underlying comorbidities such as anxiety and depression.67 In general, pharmacologic therapies used for the treatment of typical tics (ie alpha-2-adrenergic agonists, antipsychotics, etc.) have not been as effective for functional tics, and lack of response to pharmacotherapy may actually be an indicator of functional disease,23 although formal studies assessing the efficacy of pharmacologic therapy for functional tics have not yet been performed. Motor retraining aiming to reestablish normal movement patterns through physical and occupational therapy may be helpful for functional tics.24 Cognitive behavioral therapy (CBT) is a type of behavior modification that has been effectively used to improve symptoms of other functional neurologic disorders68 and may therefore also be helpful for functional tics. CBT works by teaching patients competing or distracting maneuvers to refocus attention away from the abnormal movements.23,68 An alternative behavioral modification approach, called comprehensive behavioral intervention for tics (CBIT), combines habit reversal therapy, relaxation training, and psychoeducation to help identify tic triggers or reinforcers and to redirect abnormal movements into a competing, voluntary action. CBIT is an efficacious treatment for typical tics, and while there may be some role for CBIT in the treatment of functional tics, studies have not yet directly assessed CBIT for functional tics. In addition, since exposure to functional tics via social media may lead to inadvertent behavioral reinforcement of such tics, exposure reduction should be considered by limiting social media with misleading content. Educating the patient and family about appropriate, valid, and reliable resources is one of the first steps to reducing exposure to misleading social media content. Other mechanisms of reducing exposure to misinformation have been proposed including redesigning social media search algorithms so that credible sources of information are elevated to the top, tagging content that is evidenced based versus not evidence based, using systematic surveillance to detect spread of misinformation, and training clinicians how to help patients identify reliable sources of information.69 Finally, educating the patient and family members about functional tics is extremely important for fostering acceptance of the diagnosis and working toward symptom and quality of life improvement.62 Similarly, educating the public about functional diagnoses such as FTLB will help to reduce the stigma that comes with both FMDs and TS.
Conclusion
To summarize, the FTLBs that have been observed during the pandemic may be a distinct subtype of functional tics strongly influenced by portrayals in social media. Tic characteristics such as higher rates of coprophenomena, predominant arm and trunk involvement, intense and potentially self-injurious movements, and complex vocalizations along with distinctly later onset may flag the need to consider FTLB. A greater representation of females among those affected, association with other functional neurologic disorders, and lack of prior history of childhood tics can be helpful in distinguishing FTLB, but must be considered together with clinical features and overall clinical presentation. Importantly, clinicians should remain diagnostically cautious since FTLB and organic tics can coexist in a single individual.
While there are many factors that have likely contributed to the increase in FTLB seen during the pandemic, there is no question that social media is one of these factors given the rapid rise across geographic and cultural borders and striking similarities between the tics on social media and the FTLB seen in clinic.30,49,62,64,66 In a somewhat ironic cycle, the influence of social media on tics has gained popularity in news and media outlets, spreading the popularity of these videos to even wider audiences. However, the relationship between these social media posts and the onset of new FTLB is much more complex than a straightforward cause-and-effect relationship. Other factors such as social isolation during the pandemic, increased rates of social media use during the pandemic, increased rates of depression and anxiety, and instability as a direct or indirect result of the pandemic also likely contribute to the rising rates of FTLB that have been documented during the pandemic.
Given this era of increased social media consumption and reliance on virtual technology to communicate remotely, the rise of FTLB is unlikely to be the only mass sociogenic illness spread. Indeed, it will be important for clinicians to remain vigilant about where and how medical information is consumed and to properly educate patients regarding medical diagnoses and treatments. Recognizing FTLB as a separate entity is important for many reasons, including treatment for the functional symptoms, avoiding unnecessary hospitalizations, minimizing unnecessary diagnostic tests, and allocating appropriate resources and treatments for patients. The more that clinicians are able to identify risk factors for and make accurate diagnoses of FTLB, the more that patients will be able to receive proper treatment and care and ultimately achieve a better quality of life.
Disclosure
Dr Jessica Frey reports grants from the Tourette Association of America, outside the submitted work. Dr Kevin J Black reports personal fees from SK Life Science, Inc., Medscape, Mededicus, and Huntington Study Group; grants from Emalex Biosciences, outside the submitted work; and he is also an invited member of a working group on functional tic-like behavior convened by the Tourette Association of America. Dr Irene A Malaty participated in research funded by Teva/Nuvelution, outside the submitted work; and she serves on the medical advisory board of the Tourette Association of America (uncompensated). The authors report no other conflicts of interest in this work.
References
1. Robertson MM, Eapen V, Singer HS, et al. Gilles de la Tourette syndrome. Nat Rev Dis Primers. 2017;3(1):16097. doi:10.1038/nrdp.2016.97
2. Novotny M, Valis M, Klimova B. Tourette syndrome: a mini-review. Front Neurol. 2018;9:139. doi:10.3389/fneur.2018.00139
3. McGuire JF, Bennett SM, Conelea CA, et al. Distinguishing and managing acute-onset complex tic-like behaviors in adolescence. J Am Acad Child Adolesc Psychiatry. 2021;60(12):1445–1447. doi:10.1016/j.jaac.2021.07.823
4. Casagrande SCB, Cury RG, Alho EJL, Fonoff ET. Deep brain stimulation in Tourette’s syndrome: evidence to date. Neuropsychiatr Dis Treat. 2019;15:1061–1075. doi:10.2147/NDT.S139368
5. Leckman JF, Zhang H, Vitale A, et al. Course of tic severity in Tourette syndrome: the first two decades. Pediatrics. 1998;102(1 Pt 1):14–19. doi:10.1542/peds.102.1.14
6. Sukhodolsky DG, Woods DW, Piacentini J, et al. Moderators and predictors of response to behavior therapy for tics in Tourette syndrome. Neurology. 2017;88(11):1029–1036. doi:10.1212/WNL.0000000000003710
7. Xu W, Zhang C, Deeb W, et al. Deep brain stimulation for Tourette’s syndrome. Transl Neurodegener. 2020;9:4. doi:10.1186/s40035-020-0183-7
8. Eapen V, Cavanna AE, Robertson MM. Comorbidities, social impact, and quality of life in Tourette Syndrome. Front Psychiatry. 2016;7:97. doi:10.3389/fpsyt.2016.00097
9. Storch EA, Lack CW, Simons LE, Goodman WK, Murphy TK, Geffken GR. A measure of functional impairment in youth with Tourette’s syndrome. J Pediatr Psychol. 2007;32(8):950–959. doi:10.1093/jpepsy/jsm034
10. Claussen AH, Bitsko RH, Holbrook JR, Bloomfield J, Giordano K. Impact of Tourette Syndrome on school measures in a nationally representative sample. J Dev Behav Pediatr. 2018;39(4):335–342. doi:10.1097/DBP.0000000000000550
11. Conelea CA, Woods DW, Zinner SH, et al. Exploring the impact of chronic tic disorders on youth: results from the Tourette Syndrome impact survey. Child Psychiatry Hum Dev. 2011;42(2):219–242. doi:10.1007/s10578-010-0211-4
12. Malaty I, Shineman D, Himle M. Tourette Syndrome has substantial impact in childhood and adulthood as well. J Dev Behav Pediatr. 2019;40(6):468–469. doi:10.1097/DBP.0000000000000699
13. Malli MA, Forrester-Jones R, Murphy G. Stigma in youth with Tourette’s syndrome: a systematic review and synthesis. Eur Child Adolesc Psychiatry. 2016;25(2):127–139. doi:10.1007/s00787-015-0761-x
14. Holtz KD, Tessman GK. Evaluation of a peer-focused intervention to increase knowledge and foster positive attitudes toward children with Tourette Syndrome. J Dev Phys Disabil. 2007;19(6):531–542. doi:10.1007/s10882-007-9042-z
15. White SW, Sukhodolsky DG, Rains AL, Foster D, McGuire JF, Scahill L. Elementary school teachers’ knowledge of Tourette syndrome, obsessive-compulsive disorder, & attention-deficit/hyperactivity disorder: effects of teacher training. J Dev Phys Disabil. 2011;23(1):5–14. doi:10.1007/s10882-010-9209-x
16. Nilles C, Pringsheim TM, Martino D. The recent surge of functional movement disorders: social distress or greater awareness? Curr Opin Neurol. 2022;35(4):485–493. doi:10.1097/WCO.0000000000001074
17. Zea Vera A, Bruce A, Garris J, et al. The phenomenology of tics and tic-like behavior in TikTok. Pediatr Neurol. 2022;130:14–20. doi:10.1016/j.pediatrneurol.2022.02.003
18. Conte G, Baglioni V, Valente F, Chiarotti F, Cardona F. Adverse mental health impact of the COVID-19 lockdown in individuals with Tourette Syndrome in Italy: an online survey. Front Psychiatry. 2020;11:583744. doi:10.3389/fpsyt.2020.583744
19. Hull M, Parnes M, Jankovic J. Increased incidence of functional (psychogenic) movement disorders in children and adults amid the COVID-19 pandemic: a cross-sectional study. Neurol Clin Pract. 2021;11(5):e686–e690. doi:10.1212/CPJ.0000000000001082
20. Demartini B, Ricciardi L, Parees I, Ganos C, Bhatia KP, Edwards MJ. A positive diagnosis of functional (psychogenic) tics. Eur J Neurol. 2015;22(3):527–e536. doi:10.1111/ene.12609
21. Ganos C, Edwards MJ, Müller-Vahl K. ”I swear it is Tourette’s!”: on functional coprolalia and other tic-like vocalizations. Psychiatry Res. 2016;246:821–826. doi:10.1016/j.psychres.2016.10.021
22. Baizabal-Carvallo JF, Jankovic J. The clinical features of psychogenic movement disorders resembling tics. J Neurol Neurosurg Psychiatry. 2014;85(5):573–575. doi:10.1136/jnnp-2013-305594
23. Ganos C, Martino D, Espay AJ, Lang AE, Bhatia KP, Edwards MJ. Tics and functional tic-like movements: can we tell them apart? Neurology. 2019;93(17):750–758. doi:10.1212/WNL.0000000000008372
24. Olvera C, Stebbins GT, Goetz CG, Kompoliti K. TikTok tics: a pandemic within a pandemic. Mov Disord Clin Pract. 2021;8(8):1200–1205. doi:10.1002/mdc3.13316
25. Hull M, Parnes M. Tics and TikTok: functional tics spread through social media. Mov Disord Clin Pract. 2021;8(8):1248–1252. doi:10.1002/mdc3.13267
26. Ganos C. Tics and tic-like phenomena-old questions on a grand new scale invited editorial on TikTok and tics. Mov Disord Clin Pract. 2021;8(8):1198–1199.
27. Kurlan R, Deeley C, Como PG. Psychogenic movement disorder (pseudo-tics) in a patient with Tourette’s syndrome. J Neuropsychiatry Clin Neurosci. 1992;4(3):347–348.
28. Dooley JM, Stokes A, Gordon KE. Pseudo-tics in Tourette syndrome. J Child Neurol. 1994;9(1):50–51. doi:10.1177/088307389400900112
29. Janik P, Milanowski L, Szejko N. Tiki psychogenne: charakterystyka kliniczna i częstośćwystępowania [Psychogenic tics: clinical characteristics and prevalence]. Psychiatr Pol. 2014;48(4):835–845. Polish.
30. Pringsheim T, Ganos C, McGuire JF, et al. Rapid onset functional tic-like behaviors in young females during the COVID-19 pandemic. Mov Disord. 2021;36(12):2707–2713. doi:10.1002/mds.28778
31. Robinson S, Hedderly T. Novel psychological formulation and treatment of “tic attacks” in Tourette Syndrome. Front Pediatr. 2016;4:46. doi:10.3389/fped.2016.00046
32. Heyman I, Liang H, Hedderly T. COVID-19 related increase in childhood tics and tic-like attacks. Arch Dis Child. 2021;106(5):420–421. doi:10.1136/archdischild-2021-321748
33. Müller-Vahl KR, Pisarenko A, Jakubovski E, Fremer C. Stop that! It’s not Tourette’s but a new type of mass sociogenic illness. Brain. 2022;145(2):476–480. doi:10.1093/brain/awab316
34. Cauberghe V, Van Wesenbeeck I, De Jans S, Hudders L, Ponnet K. How adolescents use social media to cope with feelings of loneliness and anxiety during COVID-19 lockdown. Cyberpsychol Behav Soc Netw. 2021;24(4):250–257. doi:10.1089/cyber.2020.0478
35. Cauberghe V, De Jans S, Hudders L, Vanwesenbeeck I. Children’s resilience during Covid-19 confinement. A child’s perspective-which general and media coping strategies are useful? J Community Psychol. 2022;50(3):1503–1520. doi:10.1002/jcop.22729
36. Marengo D, Angelo Fabris M, Longobardi C, Settanni M. Smartphone and social media use contributed to individual tendencies towards social media addiction in Italian adolescents during the COVID-19 pandemic. Addict Behav. 2022;126:107204. doi:10.1016/j.addbeh.2021.107204
37. Topf JM, Williams PN. COVID-19, social media, and the role of the public physician. Blood Purif. 2021;50(4–5):595–601. doi:10.1159/000512707
38. Basch CH, Hillyer GC, Jaime C. COVID-19 on TikTok: harnessing an emerging social media platform to convey important public health messages. Int J Adolesc Med Health. 2020. doi:10.1515/ijamh-2020-0111
39. Li HO, Bailey A, Huynh D, Chan J. YouTube as a source of information on COVID-19: a pandemic of misinformation? BMJ Glob Health. 2020;5(5):e002604. doi:10.1136/bmjgh-2020-002604
40. D’Souza RS, D’Souza S, Strand N, Anderson A, Vogt MNP, Olatoye O. YouTube as a source of medical information on the novel coronavirus 2019 disease (COVID-19) pandemic. Glob Public Health. 2020;15(7):935–942. doi:10.1080/17441692.2020.1761426
41. Yeung A, Ng E, Abi-Jaoude E. TikTok and attention-deficit/hyperactivity disorder: a cross-sectional study of social media content quality. Can J Psychiatry. 2022;7067437221082854. doi:10.1177/07067437221082854
42. Malli MA, Forrester-Jones R. “I’m not being rude, I’d want somebody normal”: adolescents’ perception of their peers with Tourette’s Syndrome: an exploratory study. J Dev Phys Disabil. 2017;29(2):279–305. doi:10.1007/s10882-016-9524-y
43. Eddy CM, Cavanna AE. ‘It’s a curse!’: coprolalia in Tourette syndrome. Eur J Neurol. 2013;20(11):1467–1470. doi:10.1111/ene.12207
44. Freeman RD, Zinner SH, Müller-Vahl KR, et al. Coprophenomena in Tourette syndrome. Dev Med Child Neurol. 2009;51(3):218–227. doi:10.1111/j.1469-8749.2008.03135.x
45. Calder-Sprackman S, Sutherland S, Doja A. The portrayal of Tourette Syndrome in film and television. Can J Neurol Sci. 2014;41(2):226–232. doi:10.1017/S0317167100016620
46. Collado-Vázquez S, Carrillo JM. Los tics y el síndrome de Tourette en la literatura, el cine y la televisión [Tics and Tourette syndrome in literature, cinema and television]. Rev Neurol. 2013;57(3):123–133. Spanish.
47. Fat MJ, Sell E, Barrowman N, Doja A. Public perception of Tourette syndrome on YouTube. J Child Neurol. 2012;27(8):1011–1016. doi:10.1177/0883073811432294
48. Perkins V, Coulson NS, Davies EB. Using online support communities for Tourette Syndrome and tic disorders: online survey of users’ experiences. J Med Internet Res. 2020;22(11):e18099. doi:10.2196/18099
49. Martindale JM, Mink JW. The rise of functional tic-like behaviors: what do the COVID-19 pandemic and social media have to do with it? A narrative review. Front Pediatr. 2022;10. doi:10.3389/fped.2022.863919
50. Müller-Vahl KR, Pisarenko A, Jakubovski E, Fremer C. Reply: a call for caution: ‘stop that’ sentiments threaten tic research, healthcare and advocacy progress. Brain. 2022;145(4):e21–e23. doi:10.1093/brain/awac029
51. Sandri A, Di Vico IA, Riello M, Marotta A, Tinazzi M. The impact of recurrent Covid-19 waves on patients with functional movement disorders: a follow-up study. Clin Park Relat Disord. 2022;6:100139. doi:10.1016/j.prdoa.2022.100139
52. Brandão PRP, Grippe TC, Pereira DA, Munhoz RP, Cardoso F. New-onset movement disorders associated with COVID-19. Tremor Other Hyperkinet Mov. 2021;11:26. doi:10.5334/tohm.595
53. Schneider SA, Hennig A, Martino D. Relationship between COVID-19 and movement disorders: a narrative review. Eur J Neurol. 2022;29(4):1243–1253. doi:10.1111/ene.15217
54. Malaty I, Anderson S, Bennett S, et al. Diagnosis and management of functional tic-like phenomena. J Clin Med. 2022;11(21):6470
55. Robertson MM, Eapen V, Rizzo R, Stern JS, Hartmann A. Gilles de la Tourette Syndrome: advice in the times of COVID-19. F1000Res. 2020;9:257. doi:10.12688/f1000research.23275.1
56. Schrag AE, Martino D, Wang H, et al. Lack of association of Group A Streptococcal infections and onset of tics: European multicenter tics in children study. Neurology. 2022;98(11):e1175–e1183. doi:10.1212/WNL.0000000000013298
57. Snider LA, Swedo SE. PANDAS: current status and directions for research. Mol Psychiatry. 2004;9(10):900–907. doi:10.1038/sj.mp.4001542
58. Guido CA, Loffredo L, Zicari AM, et al. The impact of the COVID-19 epidemic during the lockdown on children with the Pediatric Acute-Onset Neuropsychiatric Syndrome (PANDAS/PANS): the importance of environmental factors on clinical conditions. Front Neurol. 2021;12:702356. doi:10.3389/fneur.2021.702356
59. Anderson KN, Radhakrishnan L, Lane RI, et al. Changes and inequities in adult mental health-related emergency department visits during the COVID-19 pandemic in the US. JAMA Psychiatry. 2022;79(5):475–485. doi:10.1001/jamapsychiatry.2022.0164
60. Radhakrishnan L, Leeb RT, Bitsko RH, et al. Pediatric emergency department visits associated with mental health conditions before and during the COVID-19 pandemic - United States, January 2019-January 2022. MMWR Morb Mortal Wkly Rep. 2022;71(8):319–324. doi:10.15585/mmwr.mm7108e2
61. Mataix-Cols D, Ringberg H, Fernández de la Cruz L. Perceived worsening of tics in adult patients with Tourette Syndrome after the COVID-19 outbreak. Mov Disord Clin Pract. 2020;7(6):725–726. doi:10.1002/mdc3.13004
62. Pringsheim T, Martino D. Rapid onset of functional tic-like behaviours in young adults during the COVID-19 pandemic. Eur J Neurol. 2021;28(11):3805–3808. doi:10.1111/ene.15034
63. Conelea CA, Bervoets J, Bethan Davies E, et al. A call for caution: ‘stop that’ sentiments threaten tic research, healthcare and advocacy. Brain. 2022;145(4):e18–e20. doi:10.1093/brain/awac028
64. Buts S, Duncan M, Owen T, et al. Paediatric tic-like presentations during the COVID-19 pandemic. Arch Dis Child. 2022;107(3):e17. doi:10.1136/archdischild-2021-323002
65. Paulus T, Bäumer T, Verrel J, et al. Pandemic tic-like behaviors following social media consumption. Mov Disord. 2021;36(12):2932–2935. doi:10.1002/mds.28800
66. Han VX, Kozlowska K, Kothur K, et al. Rapid onset functional tic-like behaviours in children and adolescents during COVID-19: clinical features, assessment and biopsychosocial treatment approach. J Paediatr Child Health. 2022;58(7):1181–1187. doi:10.1111/jpc.15932
67. Howlett M, Martino D, Nilles C, Pringsheim T. Prognosis of rapid onset functional tic-like behaviors: prospective follow-up over 6 months. Brain Behav. 2022;12(6):e2606. doi:10.1002/brb3.2606
68. Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor disorders: a consensus recommendation. J Neurol Neurosurg Psychiatry. 2015;86(10):1113–1119. doi:10.1136/jnnp-2014-309255
69. Khullar D. Social media and medical misinformation: confronting new variants of an old problem. JAMA. 2022;328(14):1393–1394. doi:10.1001/jama.2022.17191
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.