")
Back to Journals » Journal of Blood Medicine » Volume 13
Thrombocytopenia Among Pregnant Women in Southwest Ethiopia: Burden, Severity, and Predictors
Authors Haile K , Kebede S, Abera T, Timerga A , Mose A
Received 10 March 2022
Accepted for publication 23 May 2022
Published 26 May 2022 Volume 2022:13 Pages 275—282
DOI https://doi.org/10.2147/JBM.S365812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Kassahun Haile,1 Solomon Kebede,1 Temesgen Abera,1 Abebe Timerga,2 Ayenew Mose3
1Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 2Department of Biomedical Science, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 3Department of Midwifery, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
Correspondence: Kassahun Haile, Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wolkite University, P.O. Box: 07, Gubre, Wolkite, Ethiopia, Tel +259-26-07-43-74, Fax +251 11 322 0041, Email [email protected]
Background: Thrombocytopenia is a worldwide public health problem in pregnant women and is associated with significant maternal–fetal complications and mortality. Determination of burden, severity, and predictors of thrombocytopenia in pregnant women is imperative to develop intervention measures to mitigate their risk and public health impact, which is not well known in Ethiopia, particularly in the selected study area. Thus, this study aimed to determine the burden, severity, and predictors of thrombocytopenia among pregnant women in Wolkite University Specialized Hospital, southwest Ethiopia.
Materials and Methods: A cross-sectional study was employed among 422 pregnant women from May to August 2021. A structured questionnaire was used to collect data on socio-demographic, reproductive, and related characteristics. Venous blood samples were collected and platelet counts were determined by Sysmex XP-300 hematology analyzer. A binary logistic regression analysis was performed using SPSS version 22 software to identify independent predictors of thrombocytopenia. The p-value < 0.05 was considered statistically significant.
Results: The overall burden of thrombocytopenia among pregnant women was 14.5% (95% CI: 11.4– 17.8). Among them, 77%, 16.4%, and 6.6% had mild, moderate, and severe thrombocytopenia, respectively. Rural residence (AOR: 2.9, 95% CI: 1.5– 5.8), increasing age (AOR: 1.9, 95% CI: 1.04– 3.44), alcohol consumption (AOR: 2.48, 95% CI: 1.3– 4.5), and HIV infection (AOR: 8.5, 95% CI: 1.9– 18.4) were independent predictors of thrombocytopenia among the pregnant women.
Conclusion: A high burden of thrombocytopenia (14.5%) was observed among the pregnant women in this study area. Rural residence, increasing age, consumption of alcohol, and HIV infection were identified as independent predictors of thrombocytopenia. The findings of this study should be taken into consideration to conduct appropriate intervention measures on identified predictors and implement routine screening of platelet count, thrombocytopenia diagnosis, and treatments to reduce the burden of morbidity and mortality among pregnant women.
Keywords: pregnant women, thrombocytopenia, predictors, Wolkite, Ethiopia
Introduction
Thrombocytopenia is a substantial hematological abnormality among pregnant women, affecting approximately 7–11% of pregnant women around the world.1,2 Developing countries share a huge burden of thrombocytopenia. A study revealed 8.4% of the overall global burden of thrombocytopenia among pregnant women; with the highest burden reported from Africa (15.3%) and the lowest from Taiwan.3
Thrombocytopenia in pregnant women was defined as a blood platelet (PLT) count below 150 ×109/L,4 and it is categorized as mild (PLT, 100–150×109/L), moderate (PLT, 50–100×109/L), and severe thrombocytopenia (PLT, <50×109/L).5 During pregnancy, thrombocytopenia might be associated with gestational conditions (it accounts for 70–80%), hypertensive disorders (15–20%), immune-mediated conditions (3–5%),6–9 chronic infections (malaria, HIV, HBV, HCV),6,10 hematological malignancy,11 folate deficiency, and adverse reaction from the drug.6,12 Furthermore, impaired platelet production or destruction, increased platelet sequestration and aggregation as well as increased platelet consumption in the peripheral tissue were the main underlying mechanisms that might contribute to the development of thrombocytopenia during pregnancy.6,7,12
Thrombocytopenia is a common problem during pregnancy and is associated with several negative consequences such as excessive bleeding during or after childbirth, maternal and fetal complications,10,13 which may result in significant morbidity and mortality for both mother and fetus.3,14 Several epidemiological studies reported 19%, 15.8%, and 8.8–10.5% burden of thrombocytopenia among pregnant women in Libya,9 Uganda,15 and India,2,16,17 respectively. Furthermore, the risk of bleeding was significantly higher among severe thrombocytopenic women,15,18 which requires appropriate monitoring and management. The studies revealed 6.6%, 7%, 11.54%, and 10.3% prevalence of severe thrombocytopenia among pregnant women in Uganda,15 India,19 Hawassa,4 and Gondar,20 respectively. In addition, a high burden of severe thrombocytopenia was reported in pregnant women who had bleeding problem.4 Therefore, assessing the burden and severity of thrombocytopenia in pregnant women is important to reduce the risk of bleeding, maternal and fetal complications as well as related mortality, which is not frequently detected and appropriately described in Ethiopia. In addition, different studies suggested that evaluation of thrombocytopenia routinely by checking the platelet count and peripheral smear in early pregnancy and third trimester would aid in the early diagnosis of thrombocytopenia.3,4,8 In Ethiopia, particularly in the selected study area, complete blood counts are routinely performed for all pregnant women attending their first antenatal care (ANC); however, there is no follow-up on platelet count particularly during the third trimester, labour, and delivery until severe complications were ensured. Determining severity pattern, burden, and predictors of thrombocytopenia plays a great role in the management of thrombocytopenic women and is important to develop evidence-based intervention measures, which are not well known in this study area. Therefore, this study aimed to determine thrombocytopenia burden, severity, and predictors among pregnant women in Wolkite University Specialized Hospital, southern Ethiopia.
Materials and Methods
Study Design, Area, and Period
A cross-sectional study was employed from May to August 2021 at Wolkite University Specialized Hospital in the Gurage zone, Southern Nation Nationality and Peoples Regional State (SNNPR), Ethiopia. The hospital is located 170km far away from the capital city of Ethiopia, Addis Ababa and it provides services for more than 1.2 million inhabitants living in the Gurage zone and surrounding districts. The study was conducted among pregnant women who attended ANC clinics at Wolkite University Specialized Hospital.
Sample Size Determination and Sampling Technique
A single population proportion formula was used to determine the sample size for the study by considering a 95% level of confidence, 10% non-response rate, 5% margin of error, and 50% proportion of thrombocytopenia. Finally, we got sample sizes of 422. Accordingly, pregnant women (ages range, 15–49 years) who attended the ANC clinic during the data collection period were consecutively included in the study until attaining the final sample size. Study participants who took drugs such as heparin and non-steroidal anti-inflammatory drugs like aspirin, had bleeding manifestations, splenomegaly, and chronic disease (HCV, HBV, and hypertension) were excluded from the study after reviewing their records.
Data Collection and Analysis Method
Data on socio-demographic, reproductive, and related characteristics were collected by structured and pre-tested questionnaires through interviews by a trained midwife. Four milliliters of venous blood samples were collected in an EDTA tube and platelet counts were determined by the Sysmex XP-300 hematology analyzer. Thin blood films were prepared, air-dried, and then stained with Wright stain to examine the presence of platelet aggregation and malaria parasites. Thrombocytopenia among pregnant women was defined as a platelet count (PLT) below 150×109/L and thin blood films were checked for the presence of agglutination of the platelet. The severity of thrombocytopenia was categorized into mild (PLT, 100–150×109/L), moderate (PLT, 50–99×109/L), and severe thrombocytopenia (PLT<50×109/L).20
Data Processing and Analysis
The data were entered and analyzed using SPSS version 22 software and presented in tables using descriptive summaries. Binary logistic regression analysis was performed to determine the presence and strength of an association between the prevalence of thrombocytopenia and independent predictors. Bivariate analysis was performed for each independent predictor to select candidate predictors for multivariate analysis by considering a p-value <0.25. Multivariate analysis was used to control the effect of confounding variables and to identify significantly associated factors with the prevalence of thrombocytopenia. The 95% CI, crude odds ratio (COR), and adjusted odds ratio (AOR) were used to see the strength and directions of associations. The p-value <0.05 was considered statistically significant.
Results
A total of 422 pregnant women were included in this study with a response rate of 100%. The mean (±SD) age of the study participants was 29.1±5.3 years (age ranges from 18 to 40). The majority of the study participants 220 (52.1%) were aged ≤29 years and rural residents 220 (52.1%). About 176 (41.7%) were in their third trimester, 129 (30.6%) in the second trimester, and 117 (27.7%) in the first trimester. Among the study participants, about 135 (32%) were illiterate (unable to read and write), 207 (49.1%) were housewives, and 126 (29.9%) had a habit of alcohol consumption during the time of the data collection (Table 1).
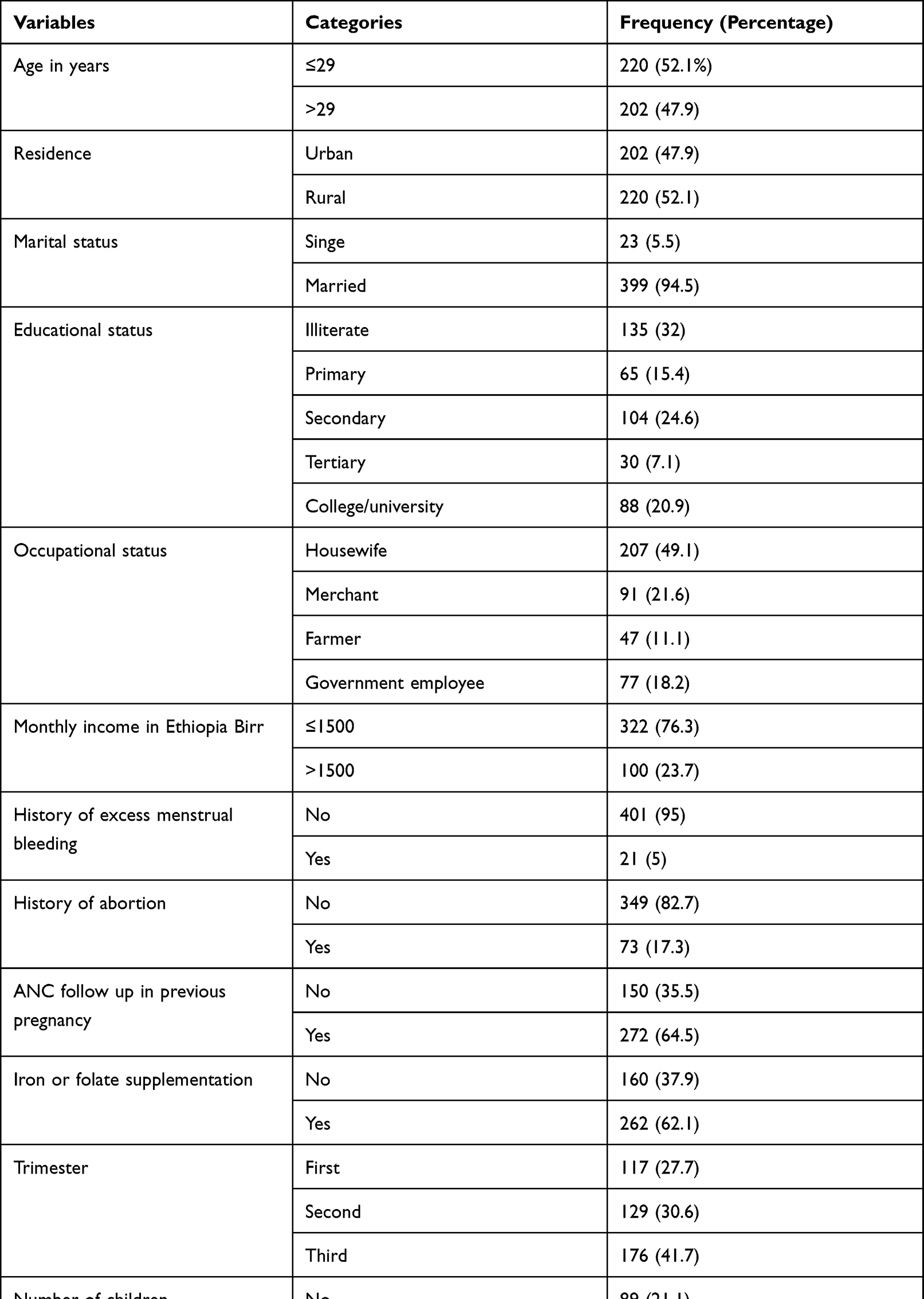 |
Table 1 Socio-Demographic, Reproductive, and Related Characteristics of Pregnant Women Attending Antenatal Care Clinics at Wolkite University Specialized Hospital, Southwest Ethiopia, May to August 2021 |
Prevalence and Severity Pattern of Thrombocytopenia Among Study Participants
The mean (±SD) of the PLT count among the study participant was 232.07±77.48×109/L. The overall prevalence of thrombocytopenia among the study participant was 61 (14.5%) with 95% CI (11.4–17.8). Among thrombocytopenic study participants, 47 (77%), 10 (16.4%), and 4 (6.6%) had mild, moderate, and severe thrombocytopenia, respectively.
Independent Predictors of Thrombocytopenia Among the Study Participants
In the bivariate analysis: being a rural dweller, increasing age, educational status, history of excess menstrual bleeding, alcohol consumption, and being HIV positive were identified as candidate predictors for multivariate analysis by considering p-value <0.25 (Table 2).
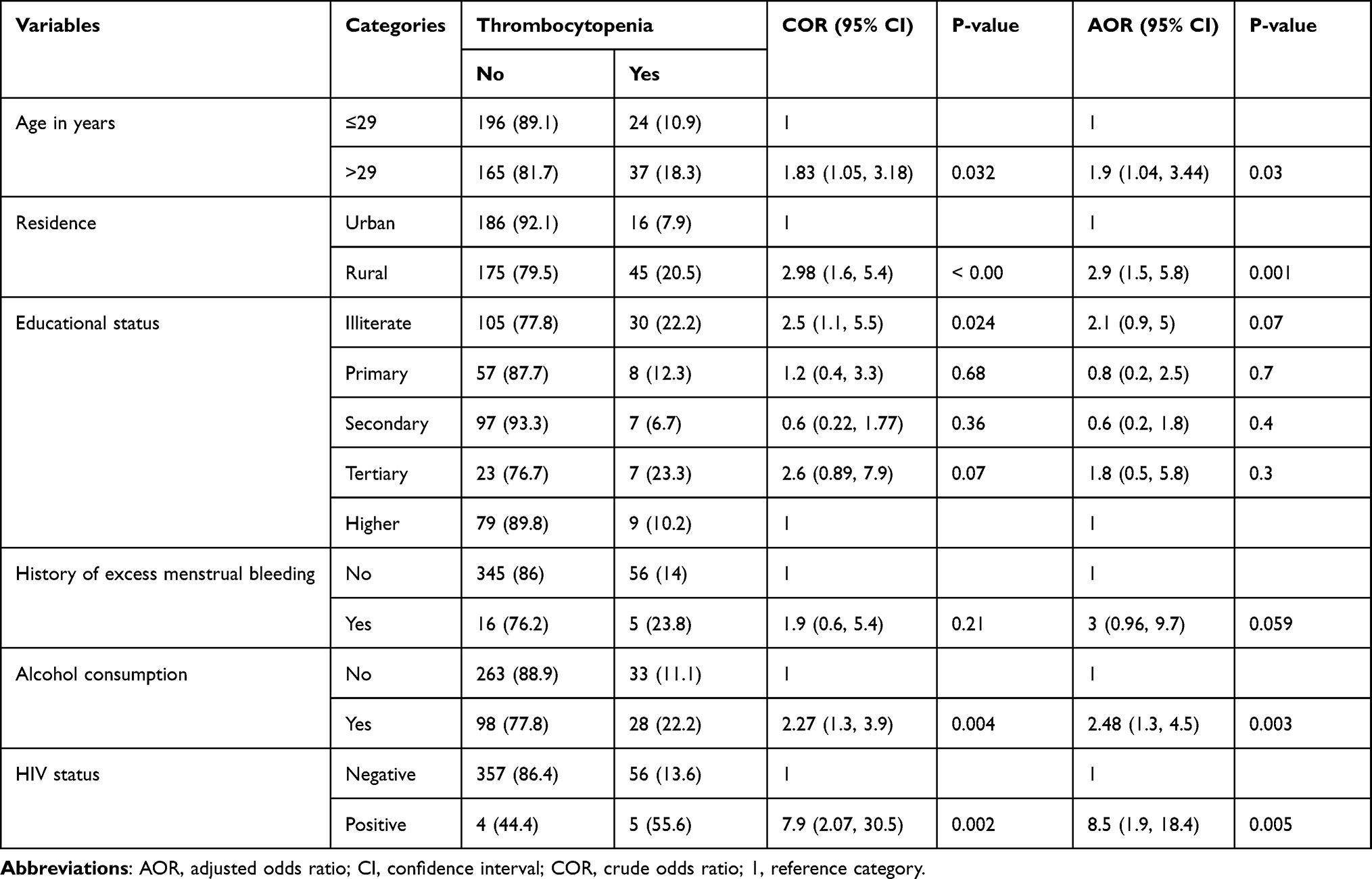 |
Table 2 Predictors Associated with Thrombocytopenia Among Study Participants, 2021 |
A multivariate binary logistic regression model was used to identify independent predictors of thrombocytopenia among study participants. A significantly high prevalence of thrombocytopenia was observed in older study participants (18.3%) as compared to younger participants (AOR: 1.9, 95% CI: 1.04–3.44, p=0.03). Rural area residents were ~3 times higher odds of thrombocytopenia as compared to urban residents. Study participants who had a habit of alcohol consumption at least once per week were 2.48 times more likely to develop thrombocytopenia than their counterparts. A higher proportion of thrombocytopenia (55.6%) was found in HIV seropositive than seronegative study participants, which was significant (AOR: 8.5, 95% CI: 1.9–18.4) (Table 2).
Discussion
Platelet abnormality is a significant problem encountered in pregnant women and is associated with negative impacts on both women and the fetus.3,21 The present study attempted to determine thrombocytopenia burden, severity, and predictors among pregnant women at Wolkite University Specialized Hospital, southern Ethiopia. Our finding showed a 14.5% (95% CI: 11.4–17.8) burden of thrombocytopenia among pregnant women; out of them 77%, 16.4%, and 6.6% had mild, moderate, and severe thrombocytopenia, respectively. Rural residence, older age, alcohol consumption, and HIV infection were identified as independent predictors of thrombocytopenia. The burden of thrombocytopenia obtained in our study was consistent with the findings reported from Ethiopia 13.5%,4 Ghana 15.3%,11 Uganda 15.8%,25 and India 12.82%.19
Mohseni et al stated that thrombocytopenia affects around one‑tenth of pregnant women and estimated 8.4% (6.9–10.1%) global burden of thrombocytopenia.3 However, our study finding was much higher than the global estimate. These warrants need to routinely evaluate thrombocytopenia in pregnant women as well as implement appropriate intervention measures to alleviate adverse outcomes. Furthermore, our finding was higher than studies reported from different parts of Ethiopia 7.7%–10.2%20,22,23 and Iraq 8%,5 but it was lower than the study reported from India 19%.24 The variation in the burden of thrombocytopenia might be due to differences in sample size, hematology analyzer, and socio-demographic characteristics. In addition, our result revealed a huge burden of thrombocytopenia which should need extra attention to avoid the occurrence of adverse outcomes in pregnant women. Several literatures suggested that early evaluation of thrombocytopenia in pregnancy is required for optimal care of mother and the neonate as well as to achieve a favorable fetomaternal outcome.26,27
Thrombocytopenia had a significant impact on both women and fetus outcomes. David Ruiru et al25 revealed that women who had thrombocytopenia were significant immediate maternal outcomes such as placenta abruption and postpartum hemorrhage. In addition, a statistically significant association was observed between maternal thrombocytopenia and stillbirths,27 among thrombocytopenic women 3.2%, 15.8%, and 24.5% had bleeding manifestations before delivery, primary postpartum hemorrhage, and had other antepartum complications (incision site ooze, wound hematoma, episiotomy hematoma, and placental abruption), respectively.27 This implies that pregnant women should be paid more attention to thrombocytopenia to avoid the occurrence of bleeding events before or after delivery.28
Based on the platelet count in the current study, 77%, 16.4%, and 6.6% of pregnant women had mild, moderate, and severe thrombocytopenia, respectively. Our finding was comparable with studies reported from Ethiopia,20 Ghana,11 Uganda,15 and India.24 The consequences of thrombocytopenia in pregnancy are mostly benign, but moderate-to-severe thrombocytopenia was associated with adverse obstetric and perinatal outcomes.29 A study reported that moderate-to-severe thrombocytopenic women were at a greater risk of cesarean section, antepartum hemorrhage, postpartum hemorrhage, wound hematoma, intrauterine fetal death, preterm delivery, and intrauterine growth restriction as compared with mild thrombocytopenic pregnant women.29 Therefore, it requires careful surveillance of these high-risk women for earlier detection and treatment of complications to decelerate the fetomaternal morbidity.26,30
Several studies revealed that platelet count was significantly affected by different socio-demographic factors.20,31 Rural residence was significantly associated with thrombocytopenia in the current study. This was in line with the studies reported from different parts of the world.20 The possible reasons might be a lack of information on the causes and prevention mechanism of thrombocytopenia.
Different literatures reported that platelet count is inversely associated with age.32–34 Older age (age>29 years) was significantly associated with thrombocytopenia. Older study participants had nearly 2 times higher odds of thrombocytopenia than younger age groups. This finding was in agreement with studies reported from different countries.9,15 The probable reason for the associations might be due to stem cell reserves. The studies revealed that older individuals had a lower stem cell reserve compared to younger subjects,35 and platelet hyperactivity is increased as age increase.31–33,35
HIV infection is associated with several hematological abnormalities. The current study revealed that there is a statistically significant association between thrombocytopenia and HIV infection. HIV-infected participants were approximately 9 times more likely to develop thrombocytopenia compared to their non-infected counterparts. Our finding was in agreement with a previous study conducted in Kampala, western Uganda.15 The possible explanations that justify the associations might be due to decreased production,36 reduced life span, increased peripheral sequestration of platelet as well as production of abnormal and dysfunctional megakaryocytes, and peripheral destruction of platelets due to cross-reactivity with HIV antibodies.34,36,37
Our finding revealed a significantly higher proportion of thrombocytopenia among alcohol-consuming study participants. This might be due to the adverse effects of alcohol on platelet production and functions; it results in suppression of platelet production and impaired function.38,39
Limitation of the Study
The result of our study should be interpreted in light of the following limitations; causal links between thrombocytopenia and independent predictors were not established due to the cross-sectional nature of the study design and intestinal parasites were not detected due to logistic constraints. Data on alcohol consumption with regard to type, amount, and duration was not collected.
Conclusion
A high prevalence of thrombocytopenia (14.5%) was observed among the pregnant women in this study area. Rural residence, older age, alcohol consumption, and HIV infection were identified as independent predictors of thrombocytopenia among pregnant women. The finding of this study should be taken into consideration to conduct appropriate intervention measures on identified predictors and implement routine screening of platelet count, treatments, and prevention of thrombocytopenia to reduce the burden of mortality and complications among pregnant women.
Data Sharing Statement
The original data for this study are available from the corresponding author on a reasonable request.
Ethical Consideration
Ethical clearance was obtained from Wolkite University Ethical Review Committee. Permission was obtained from hospital administration before commencing the study. Written informed consent was obtained from each study participant after describing the objective and procedures of the study. Every response of the participants was kept confidential and their result was also communicated to their respective physician for proper management and further investigation. The study was carried out in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to acknowledge our study participants for their willingness to provide all relevant information. We are grateful to the Wolkite University Specialized Hospital staff and data collectors for their support during the data collection.
Author Contributions
All authors made substantial contributions to the conception and study design, data collection, or analysis and interpretation of data; took part in drafting the manuscript and revising it critically for important intellectual content; agreed to submit it to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declared that they have no competing interests in this work.
References
1. Barsode S, Tarlekar V, Shora M, Mehendale S. Clinical profile of thrombocytopenia in pregnancy. Indian Journal Obs Gynecol Res. 2019;6(2):192–195. doi:10.18231/j.ijogr.2019.044
2. Chandil N, Luthra S, Dwivedi AD, Singh A. Prevalence of thrombocytopenia during pregnancy, and its effect on pregnancy and perinatal outcome. Int J Clin Obstet Gynaecol. 2020;4(2):60–62. doi:10.33545/gynae.2020.v4.i2a.503
3. Mohseni M, Asgarlou Z, Azami-Aghdash S, Gareh Sheyklo S, Tavananezhad NMA. The global prevalence of thrombocytopenia among pregnant women: a systematic review and meta-analysis. Nurs Midwifery Stud. 2019;8:57–63.
4. Belayneh F, G/Mariam A, Solomon F, et al. Prevalence of thrombocytopenia, and associated factors among pregnant women attending antenatal care at Hawass. J Harmon Res Med Heal Sci. 2015;2(4):175–182.
5. Shamoon R, Muhammed NJM. Prevalence and etiological classification of thrombo- cytopenia among a group of pregnant women in Erbil city, Iraq. Turk J Hematol. 2009;26:123–128.
6. Marin A, Colibaba S, Cimpoca B, Peltecu G, Maria A. Thrombocytopenia in pregnancy. MEDICA. 2016;11(1):55–60.
7. Levy JA, Murphy LD. Thrombocytopenia in pregnancy. J Am Board Fam Pr. 2002;15(4):290–297.
8. Begam A, Tl S, Nambisan B, Kp V. Risk factors of thrombocytopenia in pregnancy. Int J Reprod Contracept Obs Gynecol. 2017;6(2):700–706. doi:10.18203/2320-1770.ijrcog20170408
9. Elgodwi S. Prevalence of thrombocytopenia among pregnant women in the Tripoli region, Libya. J Med App Sci. 2020;3(3):83.
10. Elvedi-gasparovic V, Beljan P, Gveric-ahmetasevic S, Schuster S, Skrablin S. Fetal-maternal complications and their association with gestational thrombocytopenia. Ginekol Pol. 2016;87(6):454–459. doi:10.5603/GP.2016.0025
11. Olayemi E, William F, Ariyibi EK, Kolawole TF, Ogunleye AI. Gestational thrombocytopenia among pregnant Ghanaian women. Pan Afr Med J. 2012;12:2–7.
12. Paidas MJ, Hossain N. Hematologic changes in pregnancy. Hemost Thromb Obstetrics Gynecol. 2011;3:1–11.
13. Strong J. Bleeding disorders in pregnancy. Curr Obstet Gynaecol. 2003;13:1–6. doi:10.1054/cuog.2003.0300
14. Bioomenthai D, Simrose R. Thrombocytopaenia in pregnancy: when to intervene. J Soe Obs Gynecol. 2000;22(1):37–45.
15. Ruiru D, Byonanuwe S, Oguttu BE, et al. Severity patterns and determinants of thrombocytopenia among women delivering at Kampala International University Teaching Hospital, Western Uganda. Med J Obs Gynecol. 2021;9(1):1–4.
16. Nisha S, Amita D, Uma S, Tripathi AK, Pushplata S. Prevalence and characterization of thrombocytopenia in pregnancy in Indian women. Indian J Hematol Blood Transfus. 2012;28:77–81. doi:10.1007/s12288-011-0107-x
17. Arora M, Goyal L, Khutan H. Prevalence of thrombocytopenia during pregnancy & its effect on pregnancy & neonatal outcome. Ann Int Med Dent Res. 2017;3:3–5.
18. Adams TM, Allaf MB, Vintzileos AM. Maternal thrombocytopenia in pregnancy: diagnosis and management. Clin Lab Med. 2013;33:327–341. doi:10.1016/j.cll.2013.01.002
19. Vijay Zutshi NG, Renu Arora SD, Arora R, Dhanker S. Prevalence of gestational thrombocytopenia and its effect on maternal and fetal outcome. Iraqi J Hematol. 2019;8(1):21–24. doi:10.4103/ijh.ijh_17_18
20. Asrie F, Enawgaw B, Getaneh Z. Prevalence of thrombocytopenia among pregnant women attending antenatal care service at Gondar University Teaching Hospital in 2014, Northwest Ethiopia. J Blood Med. 2017;8:61–66. doi:10.2147/JBM.S136152
21. Zahida PB, Uzma Perveen AS. Thrombocytopenia in pregnancy: an Observational Study. Pak J Med Res. 2013;52(3):67–70.
22. Gebreweld A, Bekele D, Tesgaye A. Hematological profile of pregnant women at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. BMC Hematol. 2018;18(1):1–7.
23. Shitie D, Zewde T, Molla Y. Anemia and other hematological profiles of pregnant women attending antenatal care in Debre Berhan Referral Hospital, North Shoa. BMC Res Notes. 2018;11(1):1–7.
24. Madhuri K, Movva N. Prevalence of maternal thrombocytopenia and anemia in pregnant woman-an institutional experience. Int J Gynaecol. 2022;21(2):43–46.
25. Ruiru D, Nzabandora E, Ssebuufu R, Byonanuwe S. Immediate maternal complications associated with thrombocytopenia among women delivering at a tertiary hospital in southwestern Uganda. Int J Reprod Contracept Obs Gynecol. 2021;10(2):448–451. doi:10.18203/2320-1770.ijrcog20210291
26. Mangla A, Hamad H. Thrombocytopenia Pregnancy. StatPearls Publishing LLC.; 2019.
27. Gaba N, Gaba S. Etiology and fetomaternal outcomes of thrombocytopenia during pregnancy. Perinatology. 2020;21(2):45–49.
28. Xia ZL, Dong N, Xia YR, Li A, Mei LX, Yang N. Platelet counts during pregnancy in Chinese women. JLab Med. 2020;44(5):313–317.
29. Khadra M, Fram K. Thrombocytopenia in pregnancy; prevalence, causes, and fetomaternal outcome. Clin Exp Obs Gynecol. 2020;7(2):0–5.
30. Nigam A, Nigam A, Agarwal K, Agarwal K. Fetomaternal outcome in pregnancy with severe thrombocytopenia. Eur Rev Med Pharmacol Sci. 2012;16(11):1563–1566.
31. Biino G, Santimone I, Minelli C, et al. Age-and Sex-Related Variations in Platelet count in Italy. PLoS One. 2013;8(1):1–7. doi:10.1371/journal.pone.0054289
32. Zhang J, Li M, He Y. Large population study for age- and gender-related variations of platelet indices in Southwest China healthy adults. Hematol Transfus Int J. 2015;1(4):108–114.
33. Balduini CL, Noris P. Platelet count and aging. Haematologica. 2014;99(6):953–955. doi:10.3324/haematol.2014.106260
34. Littleton N. Thrombocytopenia in HIV. CME. 2007;25(6):272–275.
35. Le BJ, Lordkipanidzé M, Sæland C, Eftestøl T, Larsen AI. Platelet function in aging. Front Cardiovasc Med. 2019;6:1–8. doi:10.3389/fcvm.2019.00001
36. Mehta PS. Hematologic manifestations of HIV/AIDS. Med Update. 2014;9:484–490.
37. Miguez-Burbano MJ, Jackson J
38. Sammaiah P, Prasad R, Shekhar VC. Study of haematological manifestations, among alcoholics in Tertiary Care Hospital. Int J Sci Study. 2018;6(3):135–140.
39. Ballard H. Hematological complications of alcoholism. Alcohol Heal Res World. 1997;21(1):42–52.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.