")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Thiazolidinediones are associated with a reduced risk of COPD exacerbations
Authors Rinne S, Liu C, Feemster L, Collins B, Bryson C, O'Riordan T, Au D
Received 11 February 2015
Accepted for publication 20 April 2015
Published 10 August 2015 Volume 2015:10(1) Pages 1591—1597
DOI https://doi.org/10.2147/COPD.S82643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Seppo T Rinne,1,2 Chuan-Fen Liu,3,4 Laura C Feemster,3,5 Bridget F Collins,3,5 Christopher L Bryson,3,6 Thomas G O’Riordan,7 David H Au3,4
1Department of Veterans Affairs, VA Connecticut Healthcare System, West Haven, 2Division of Pulmonary and Critical Care, Yale University, New Haven, CT, USA; 3VA Puget Sound Health Care System, Department of Veterans Affairs, 4Department of Health Services, University of Washington, 5Division of Pulmonary and Critical Care, University of Washington, 6Division of General Internal Medicine, University of Washington, 7Gilead Sciences, Inc., Seattle, WA, USA
Background: Thiazolidinediones (TZDs) are oral antihyperglycemic medications that are selective agonists to peroxisome proliferator-activated receptor gamma and have been shown to have potent anti-inflammatory effects in the lung.
Objective: The purpose of this study was to assess whether exposure to TZDs is associated with a decreased risk of chronic obstructive pulmonary disease (COPD) exacerbation.
Methods: A cohort study was performed by collecting data on all US veterans with diabetes and COPD who were prescribed oral antihyperglycemic medications during from period of October 1, 2005 to September 30, 2007. Patients who had two or more prescriptions for TZDs were compared with patients who had two or more prescriptions for an alternative oral antihyperglycemic medication. Multivariable negative binomial regression was performed with adjustment for potential confounding factors. The primary outcome was COPD exacerbations, including both inpatient and outpatient exacerbations.
Results: We identified 7,887 veterans who were exposed to TZD and 42,347 veterans who were exposed to non-TZD oral diabetes medications. COPD exacerbations occurred in 1,258 (16%) of the TZD group and 7,789 (18%) of the non-TZD group. In multivariable negative binomial regression, there was a significant reduction in the expected number of COPD exacerbations among patients who were exposed to TZDs with an incidence rate ratio of 0.86 (95% CI 0.81–0.92).
Conclusion: Exposure to TZDs was associated with a small but significant reduction in risk for COPD exacerbation among diabetic patients with COPD.
Keywords: peroxisome proliferator-activated receptors, glitazones, COPD exacerbation, inflammation, cohort study
Introduction
Recent estimates suggest that up to 10% of the world’s population has moderate-to-severe chronic obstructive pulmonary disease (COPD).1 In the US, COPD has risen to be the third leading cause of death and costs up to $38.8 billion annually in indirect and direct costs.2–4 Much of the cost of COPD is related to the burden of acute exacerbations.5
COPD exacerbations are characterized by a precipitous increase in airway inflammation, smooth muscle contraction, and mucus hypersecretion.6 A major focus of current COPD management is to prevent exacerbations by inhibiting these underlying physiological changes. This approach typically relies on treatment with long-acting bronchodilators and inhaled corticosteroids; however, these interventions are not always effective.7 One clinical trial found that despite therapy with inhaled bronchodilators (tiotropium and salmeterol) and inhaled corticosteroids (fluticasone propionate), 60% of patients with COPD had an exacerbation during the study year.8 Therefore, the major emphasis in drug development is to find novel pathways to decrease airway inflammation and prevent COPD exacerbations.9
Thiazolidinediones (TZDs) are a class of oral antihyperglycemic medications that include ciglitazone, pioglitazone, rosiglitazone, and troglitazone. A growing body of evidence demonstrates that these medications have anti-inflammatory effects through selective stimulation of peroxisome proliferator-activated receptor gamma (PPARγ).10 Activation of PPARγ inhibits the production and release of pro-inflammatory cytokines and impairs the function of immune cells.11 The anti-inflammatory effects of TZDs on human airway smooth muscle cells have been shown to be more potent than corticosteroids.12 We have previously shown that asthmatic patients who are exposed to TZDs have a decreased risk for asthma exacerbations.13 These findings could also provide a novel approach for the prevention of COPD exacerbations.9 The purpose of this study therefore was to assess whether the use of TZDs was associated with a decreased risk of COPD exacerbation and mortality.
Methods
Design
We performed a cohort study on US veterans receiving medical care at Veterans Affairs (VA) medical facilities during October 1, 2005–September 30, 2007 (2006 and 2007 fiscal years). All baseline characteristics and underlying diagnoses were identified in the 2006 fiscal year, and outcomes were compared in the 2007 fiscal year. Data were collected from electronic medical records of all diabetic VA service users. COPD exacerbations were compared between patients who were prescribed TZDs and those who were prescribed non-TZD oral antihyperglycemic medications. The study was approved by the institutional review board at the VA Puget Sound Health Care System.
Study cohort
Patients were included in the study if they had two or more ICD-9 diagnoses of diabetes (250.xx, 357.2, 362.0–362.02, or 366.41), received at least two ≥30-day prescriptions for an oral antihyperglycemic medication, and had a coexisting diagnosis of COPD identified in the baseline year (fiscal year 2006). Patients with COPD were identified using previously verified diagnostic criteria with ICD-9 codes (491, 492, 493.2, or 496).14 Patients were excluded from the study if they only received one prescription for TZDs in the baseline year to clearly delineate TZD from non-TZD exposures. Because patients who have bronchodilator-responsive COPD are often also classified as asthmatics, we did not exclude patients who had a concurrent diagnosis of asthma in this analysis.15 We performed a separate analysis excluding patients with asthma, and our results were similar.
Exposure to TZDs was defined as having filled two or more TZD prescriptions. During the study period, the vast majority of prescriptions for TZDs (97.1%) were rosiglitazone, which was a part of the pharmacy formulary for the VA. Only 2.9% of prescriptions had pioglitazone. Patients who were prescribed TZDs could also have been prescribed additional antihyperglycemic medications. The reference comparison was having filled two or more prescriptions for a non-TZD oral antihyperglycemic medication, including sulfonylureas (62.6% of study patients) and/or metformin (54.8% of study patients). We intentionally separated the exposure in the baseline year from the outcome in the follow-up year to avoid an immortal time bias.16
Covariates included patient demographics (age, sex, marital status, race), access to VA care (free care, distance to VA), health care utilization (number of primary care visits), and comorbidities (asthma, atrial fibrillation/flutter, congestive heart failure, ischemic heart disease, alcohol use, drug abuse, schizophrenia, and depression). The severity of diabetes was measured by the Diabetes Severity Index score, a composite measure of hemoglobin A1c and end organ damage.17 Overall patient health care burden was further evaluated using Diagnostic Cost Group scores.18 The number of COPD exacerbations and prescriptions for respiratory medications during the baseline year was also documented.
Study outcomes
The primary outcome was COPD exacerbation, defined as either inpatient or outpatient exacerbation, during the follow-up year (October 1, 2006–September 31, 2007). Inpatient COPD exacerbations included a primary ICD-9 discharge diagnosis of COPD (491, 492, 493.2, or 496), or a primary discharge diagnosis of acute respiratory failure and a secondary discharge diagnosis of COPD (518.8). Outpatient COPD exacerbations included a primary clinic diagnosis of COPD accompanied by a prescription for oral steroids or an appropriate antibiotic within 2 days of the visit. A secondary outcome was all-cause mortality, which was assessed by using vital status from the VA Information Resource Center.19
Statistical analysis
All statistical analyses were performed using Stata 11.2.20 Negative binomial regression analysis was used to assess the risk of COPD exacerbation. Results were reported as incidence rate ratios (IRRs), which were derived by dividing the expected number of exacerbations among the TZD group by the expected number of exacerbations among the non-TZD group. It was decided a priori to perform two multivariable models, one that did not control for exacerbations and respiratory medications in the baseline year (Model 1) and one that does control for them (Model 2). We performed these two models because it was unclear whether differences in these factors were a disease-modifying effect of TZDs in the baseline year or reflected the underlying severity of COPD. We repeated the analysis with proportional hazards models to evaluate the time to exacerbation, and the results were similar (results not shown).
A sensitivity analysis was done to evaluate only those patients who were adherent to diabetic therapy. To do this, medication possession ratios were created using Recomp scores for the 6 months prior to the study (which also incorporated a run-in period to account for previously dispensed medications).21 Recomp scores are a composite algorithm with a range between 0 and 1 representing the proportion of days in which a drug is available. Adherence was defined as a Recomp score of 0.8 or greater. Lastly, we used logistic regression to assess the risk of mortality with exposure to TZDs.
Results
We evaluated 51,216 diabetic veterans who had two or more prescriptions for an oral hypoglycemic agent and a diagnosis of COPD (Figure 1). After excluding patients who received only one prescription for TZDs, we identified 7,887 patients who were exposed to TZDs and 42,347 who were exposed to non-TZD oral diabetes therapy.
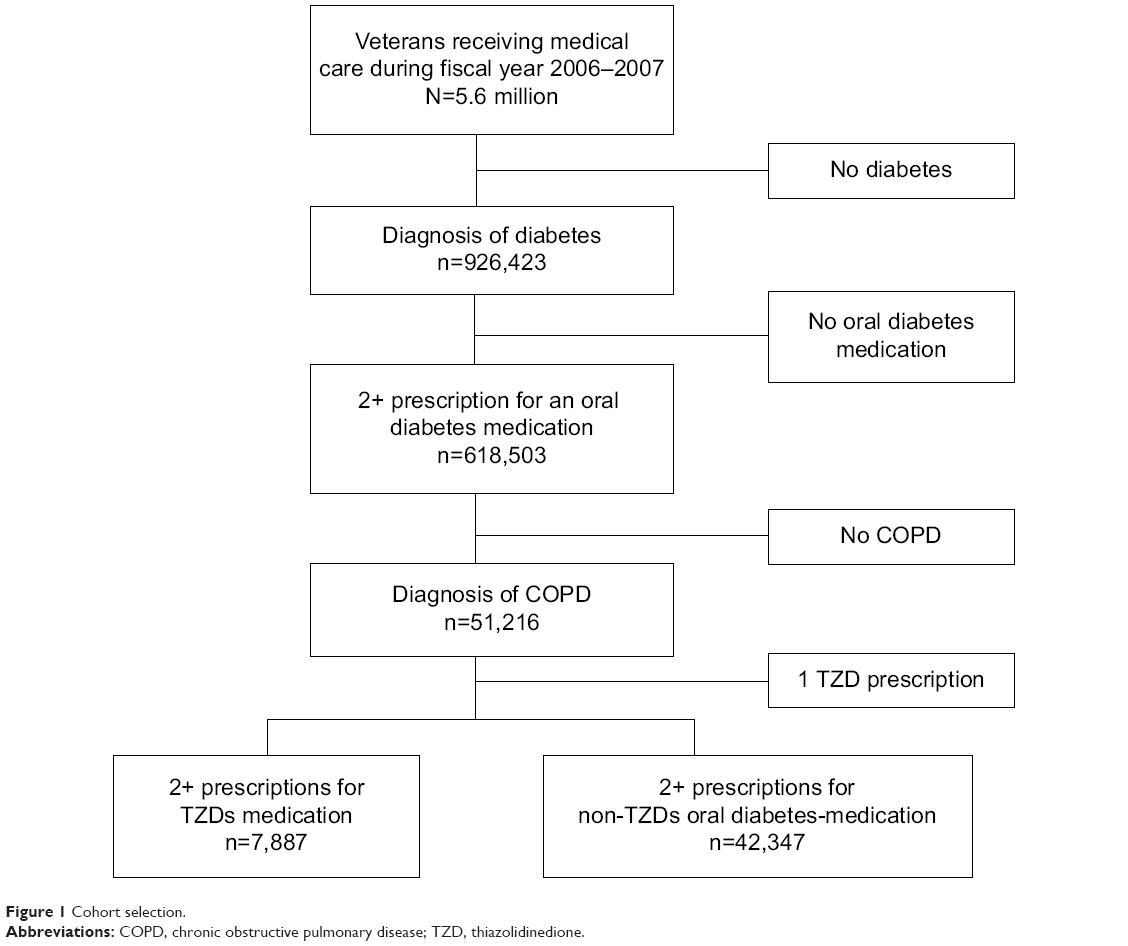 | Figure 1 Cohort selection. |
As seen in Table 1, patients exposed to TZDs were younger, more likely to be married, and less likely to be white. Diabetes Severity Index scores and Diagnostic Cost Group scores were higher among patients who were exposed to TZDs. Comorbidities also differed between the two groups. Patients who were exposed to TZDs had a lower prevalence of heart failure, atrial fibrillation, alcohol abuse, drug abuse, and schizophrenia, but had a higher prevalence of ischemic heart disease. In addition, patients exposed to TZDs had fewer prescriptions for respiratory medications, including short-acting beta agonists, long-acting beta agonists, inhaled corticosteroids, and nebulized bronchodilators. They also had fewer COPD exacerbations during the baseline year.
 | Table 1 Baseline characteristics of TZD and non-TZD patients |
COPD exacerbations
There were 1,258 patients who were exposed to TZDs and had a COPD exacerbation during the study (16% of the TZD group). In contrast, 7,789 patients exposed to non-TZD oral diabetes therapy had an exacerbation (18% of the non-TZD group). The unadjusted IRR for any COPD exacerbation was 0.77 (95% CI 0.73–0.83), which indicates that the expected number of COPD exacerbations was 23% lower among the TZD group than the non-TZD group (Table 2). This benefit of TZD exposure remained statistically significant even after controlling for potential confounding factors, including baseline exacerbations and prescriptions for respiratory medications. In the multivariable model that included baseline exacerbations and respiratory medications (Model 2), the IRR for any COPD exacerbation was 0.85 (95% CI 0.80–0.91), while the model excluding these factors (Model 1) yielded an IRR of 0.77 (95% CI 0.72–0.82).
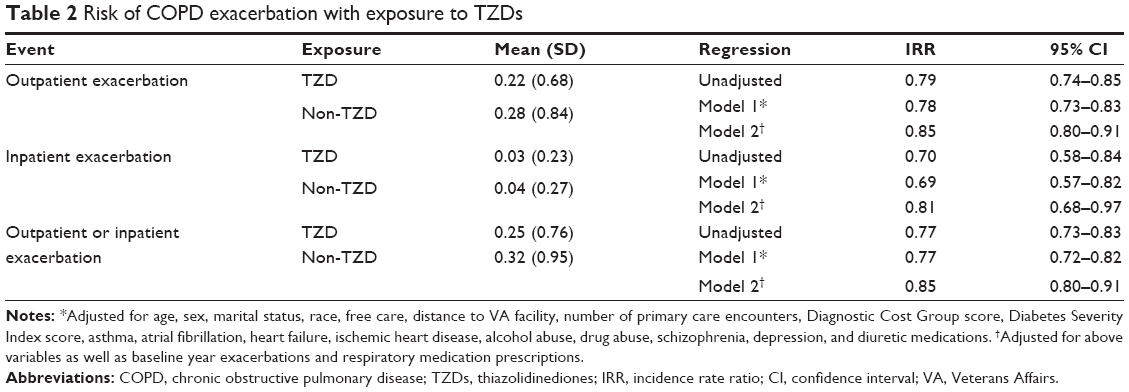 | Table 2 Risk of COPD exacerbation with exposure to TZDs |
Similar results were found in the sensitivity analysis, evaluating only patients who were adherent to therapy (Recomp scores greater than or equal to 0.8). There were 5,644 patients (71.5%) who were adherent to TZDs and 32,970 patients (77.9%) who were adherent to non-TZD diabetic medications. Unadjusted IRR for TZD exposure in this sensitivity analysis was 0.79 (95% CI 0.73–0.86), and after controlling for potential confounders (including respiratory medications and baseline exacerbations), the IRR was 0.88 (95% CI 0.82–0.95).
Mortality
In unadjusted analysis, there was a significant decrease in all-cause mortality among patients who were prescribed TZDs (OR =0.90, 95% CI 0.81–0.99); however, in multivariable analyses, there were no significant differences between the two groups (OR =0.90, 95% CI 0.81–1.00) (Table 3).
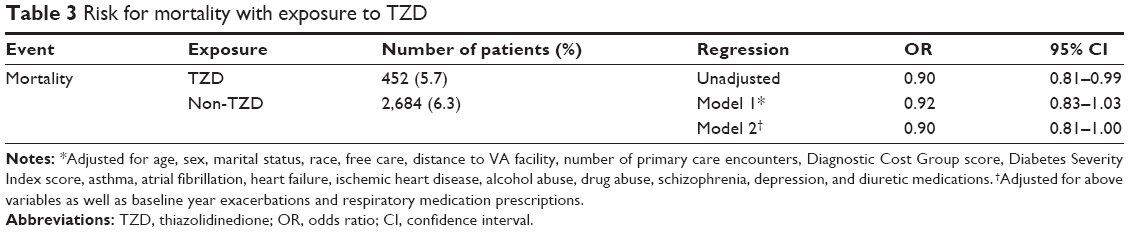 | Table 3 Risk for mortality with exposure to TZD |
Discussion
We found a small, but significant reduction in COPD exacerbations among diabetic patients who were exposed to TZDs. There was no difference in mortality between COPD exposed and unexposed patients. Although these data are observational in nature, our results suggest a potential benefit of TZDs among patients with diabetes and COPD.
The reduced risk for COPD exacerbations that we observed with TZDs is similar to what has been reported for other COPD medications, including inhaled corticosteroids and long-acting bronchodilators, although the absolute risk difference that we observed was small.22–24 Given the high prevalence of COPD and substantial morbidity related to COPD exacerbations, even a small risk reduction in exacerbation could have important contributions to COPD therapy. While many patients in our study were already on COPD therapy, taking TZDs was associated with a further reduction in risk for COPD exacerbation. Further studies, including randomized controlled trials, are needed to examine the exact impact of TZDs on COPD exacerbations and determine their clinical utility.
TZDs are selective agonists to PPARγ, a ligand-activated transcription factor that belongs to the steroid receptor superfamily.25 Though the clinical utility of TZDs was initially focused on adipose and glucose regulation, they are also involved in a variety of biological pathways, including cellular proliferation, metabolism, and inflammation.26 In the lungs, PPARγ is found in airway epithelium, submucosa, and airway smooth muscle.27 PPARγ activation inhibits the production and release of proinflammatory cytokines from macrophages and airway epithelial cells.28,29 TZDs also have anti-inflammatory properties that extend beyond the PPARγ pathway.30 In a study on human airway smooth muscle cells, TZDs inhibited inflammatory cytokine release more effectively than corticosteroids.12 Recent clinical trials of asthmatic patients demonstrate a consistent benefit of TZDs on pulmonary function and response to allergen challenge.31,32 We have also demonstrated a significant reduction in asthma exacerbations among patients who are exposed to TZDs.13 These findings open the door for possible therapy in other inflammatory respiratory conditions, including COPD.9
While there is biological plausibility for how the anti-inflammatory effects of TZDs could lead to fewer COPD exacerbations, non-biological mechanisms could also have influenced the outcome. It is notable that the two groups that we studied differed at baseline. We controlled for a broad range of potential confounding factors, including demographics, health care utilization, comorbidities, baseline exacerbations, and respiratory medications. Unmeasured confounding variables could have impacted the results. Obese patients are more likely to have severe diabetes and require more intensive antihyperglycemic therapy. Among patients with COPD, obesity is also associated with less severe disease and improved mortality.33 This could have created an indication bias for less severe COPD patients being exposed to TZDs. We were unable to control for body mass index in our study and could not evaluate this relationship closer. Patients who were prescribed TZDs may have also had better access to health care or other behaviors that could be associated with reduced COPD exacerbations. We attempted to control for access to care and frequency of primary care visits, although additional variables related to health behavior could have influenced our findings.
Concerns have been raised about the safety of TZDs. TZDs increase fluid retention by acting on PPARγ receptors in the distal collecting tubule of the kidney.34 Among patients who have underlying cardiac disease, TZDs can exacerbate heart failure.35 In addition, rosiglitazone has been associated with an increased risk for myocardial infarction.36 Owing to the small number of new starters of TZDs, we were unable to assess the adverse effects among patients who recently started TZDs. Clinicians may have avoided starting TZDs in patients who had a history of heart disease, and patients with heart failure may not have tolerated being on TZDs. This potential selection bias limits our ability to effectively assess the safety of TZDs in all patients with COPD. Any potential benefit of TZDs for patients with COPD would have to be weighed against the adverse effects of the medication.
This study had a number of additional limitations. Though it would be ideal to study patients who are newly started on TZDs, there were insufficient numbers of new starters in our cohort to do this analysis. Because of the observational design, no cause and effect inferences can be made. Although we attempted to control for a broad range of potential confounding factors, unmeasured variables that differed between the two groups could have impacted the outcome. While we used a validated approach to identify patients with COPD, we did not have spirometric confirmation of COPD and we were also not able to control patients’ physiologic severity.37 We also did not have access to information on smoking status or oxygen use. We did collect other important measures of COPD severity, including previous COPD exacerbations and prescriptions for respiratory medications, but it was unclear whether fewer baseline exacerbations and respiratory medications among the TZD group indicated less severe COPD at baseline or were related to the disease-modifying effects of TZDs during the baseline year. We presented our data with and without controlling for these measures, and there was no change in our interpretation of the results. Controlling for prior exacerbations and baseline respiratory medications may still not fully control for differences in baseline disease severity. Despite the limitations of our study, we analyzed one of the largest sample sizes of COPD patients who were taking TZDs in the US and were able to control for a wide variety of potential confounders.
Conclusion
In summary, these findings suggest that TZDs could provide a new pathway for the prevention of COPD exacerbations. We saw a significant reduction in exacerbations among diabetic patients with COPD who were exposed to TZDs. Randomized controlled trials would be needed to further evaluate the benefit of TZDs among patients with COPD and to assess appropriate dosing and frequency of therapy. With a growing burden of COPD on patients and health care systems throughout the world, TZDs may provide a novel approach for COPD management.
Acknowledgments
Research funding for this project was from a VA HSR&D grant (IIR 07-068-2) along with funding from Gilead Sciences Inc. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government. Dr Feemster is supported by the NIH NHLBI (K23 HL111116).
Disclosure
Gillead Sciences LLC funded the analysis through monies paid to the author’s institution. Dr. O’Riordan is an employee of Gilead Sciences. The authors report no other conflicts of interest in this work.
References
Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. | ||
Minino AM, Murphy SL, Xu J, Kochanek KD. Deaths: final data for 2008. Natl Vital Stat Rep. 2011;59(10):1–126. | ||
Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397–412. | ||
Foster TS, Miller JD, Marton JP, Caloyeras JP, Russell MW, Menzin J. Assessment of the economic burden of COPD in the U.S.: a review and synthesis of the literature. COPD. 2006;3(4):211–218. | ||
Toy EL, Gallagher KF, Stanley EL, Swensen AR, Duh MS. The economic impact of exacerbations of chronic obstructive pulmonary disease and exacerbation definition: a review. COPD. 2010;7(3):214–228. | ||
Papi A, Luppi F, Franco F, Fabbri LM. Pathophysiology of exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(3):245–251. | ||
Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. | ||
Aaron SD, Vandemheen KL, Fergusson D, et al; Canadian Thoracic Society/Canadian Respiratory Clinical Research Consortium. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2007;146(8):545–555. | ||
Remels AH, Gosker HR, Schrauwen P, Langen RC, Schols AM. Peroxisome proliferator-activated receptors: a therapeutic target in COPD? Eur Respir J. 2008;31(3):502–508. | ||
Spiegelman BM. PPAR-gamma: adipogenic regulator and thiazolidinedione receptor. Diabetes. 1998;47(4):507–514. | ||
Spears M, McSharry C, Thomson NC. Peroxisome proliferator-activated receptor-gamma agonists as potential anti-inflammatory agents in asthma and chronic obstructive pulmonary disease. Clin Exp Allergy. 2006;36(12):1494–1504. | ||
Patel HJ, Belvisi MG, Bishop-Bailey D, Yacoub MH, Mitchell JA. Activation of peroxisome proliferator-activated receptors in human airway smooth muscle cells has a superior anti-inflammatory profile to corticosteroids: relevance for chronic obstructive pulmonary disease therapy. J Immunol. 2003;170(5):2663–2669. | ||
Rinne ST, Feemster LC, Collins BF, et al. Thiazolidinediones and the risk of asthma exacerbation among patients with diabetes: a cohort study. Allergy Asthma Clin Immunol. 2014;10(1):34. | ||
Cooke CR, Joo MJ, Anderson SM, et al. The validity of using ICD-9 codes and pharmacy records to identify patients with chronic obstructive pulmonary disease. BMC Health Serv Res. 2011;11:37. | ||
Zeki AA, Schivo M, Chan A, Albertson TE, Louie S. The asthma-COPD overlap syndrome: a common clinical problem in the elderly. J Allergy (Cairo). 2011;2011:861926. | ||
Suissa S. Immortal time bias in pharmaco-epidemiology. Am J Epidemiol. 2008;167(4):492–499. | ||
Joish VN, Malone DC, Wendel C, Draugalis JR, Mohler MJ. Development and validation of a diabetes mellitus severity index: a risk-adjustment tool for predicting health care resource use and costs. Pharmacotherapy. 2005;25(5):676–684. | ||
Ash AS, Ellis RP, Pope GC, et al. Using diagnoses to describe populations and predict costs. Health Care Financ Rev. 2000;21(3):7–28. | ||
Dendale P, De Keulenaer G, Troisfontaines P, et al. Effect of a telemonitoring-facilitated collaboration between general practitioner and heart failure clinic on mortality and rehospitalization rates in severe heart failure: the TEMA-HF 1 (TElemonitoring in the MAnagement of Heart Failure) study. Eur J Heart Fail. 2012;14(3):333–340. | ||
StataCorp. Stata Statistical Software: Release 11.2. College Station, TX: StataCorp LP; 2012. | ||
Bryson CL, Au DH, Young B, McDonell MB, Fihn SD. A refill adherence algorithm for multiple short intervals to estimate refill compliance (ReComp). Med Care. 2007;45(6):497–504. | ||
Sin DD, McAlister FA, Man SF, Anthonisen NR. Contemporary management of chronic obstructive pulmonary disease: scientific review. JAMA. 2003;290(17):2301–2312. | ||
Thompson AB, Mueller MB, Heires AJ, et al. Aerosolized beclomethasone in chronic bronchitis. Improved pulmonary function and diminished airway inflammation. Am Rev Respir Dis. 1992;146(2):389–395. | ||
Agarwal R, Aggarwal AN, Gupta D, Jindal SK. Inhaled corticosteroids vs placebo for preventing COPD exacerbations: a systematic review and metaregression of randomized controlled trials. Chest. 2010;137(2):318–325. | ||
Evans RM. The steroid and thyroid hormone receptor superfamily. Science. 1988;240(4854):889–895. | ||
Blanquart C, Barbier O, Fruchart JC, Staels B, Glineur C. Peroxisome proliferator-activated receptors: regulation of transcriptional activities and roles in inflammation. J Steroid Biochem Mol Biol. 2003;85(2–5):267–273. | ||
Braissant O, Foufelle F, Scotto C, Dauca M, Wahli W. Differential expression of peroxisome proliferator-activated receptors (PPARs): tissue distribution of PPAR-alpha, -beta, and -gamma in the adult rat. Endocrinology. 1996;137(1):354–366. | ||
Jiang C, Ting AT, Seed B. PPAR-gamma agonists inhibit production of monocyte inflammatory cytokines. Nature. 1998;391(6662):82–86. | ||
Wang AC, Dai X, Luu B, Conrad DJ. Peroxisome proliferator-activated receptor-gamma regulates airway epithelial cell activation. Am J Respir Cell Mol Biol. 2001;24(6):688–693. | ||
Zhu M, Flynt L, Ghosh S, et al. Anti-inflammatory effects of thiazolidinediones in human airway smooth muscle cells. Am J Respir Cell Mol Biol. 2011;45(1):111–119. | ||
Richards DB, Bareille P, Lindo EL, Quinn D, Farrow SN. Treatment with a peroxisomal proliferator activated receptor gamma agonist has a modest effect in the allergen challenge model in asthma: a randomised controlled trial. Respir Med. 2010;104(5):668–674. | ||
Spears M, Donnelly I, Jolly L, et al. Bronchodilatory effect of the PPAR-gamma agonist rosiglitazone in smokers with asthma. Clin Pharmacol Ther. 2009;86(1):49–53. | ||
Cao C, Wang R, Wang J, Bunjhoo H, Xu Y, Xiong W. Body mass index and mortality in chronic obstructive pulmonary disease: a meta-analysis. PLoS One. 2012;7(8):e43892. | ||
Guan Y, Hao C, Cha DR, et al. Thiazolidinediones expand body fluid volume through PPARgamma stimulation of ENaC-mediated renal salt absorption. Nat Med. 2005;11(8):861–866. | ||
Nesto RW, Bell D, Bonow RO, et al. Thiazolidinedione use, fluid retention, and congestive heart failure: a consensus statement from the American Heart Association and American Diabetes Association. October 7, 2003. Circulation. 2003;108(23):2941–2948. | ||
Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007;356(24):2457–2471. | ||
Drummond MB, Hansel NN, Connett JE, Scanlon PD, Tashkin DP, Wise RA. Spirometric predictors of lung function decline and mortality in early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185(12):1301–1306. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.